Back to Journals » International Journal of Women's Health » Volume 18
Acceptability of Modified Early Obstetric Warning Systems Among Midwives in Malawi; An Exploratory Qualitative Study
Authors Mndolo NCM ![]() , Baluwa MA, Yeboa NK
, Baluwa MA, Yeboa NK ![]() , Kazembe A, Chirwa E
, Kazembe A, Chirwa E
Received 27 February 2026
Accepted for publication 9 June 2026
Published 18 June 2026 Volume 2026:18 605608
DOI https://doi.org/10.2147/IJWH.S605608
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Matteo Frigerio
Neggie Chinyanga Mkundika Mndolo,1,2 Masumbuko Albert Baluwa,1,3 Naomi Kyeremaa Yeboa,1 Abigail Kazembe,1 Ellen Chirwa1
1School of Maternal Neonatal and Reproductive Health, Kamuzu University of Health Sciences, Blantyre, Malawi; 2Department of Midwifery, Malawi College of Health Sciences, Lilongwe, Malawi; 3Department of Nursing and Midwifery, Mzuzu University, Mzuzu, Malawi
Correspondence: Neggie Chinyanga Mkundika Mndolo, School of Maternal Neonatal and Reproductive Health, Kamuzu University of Health Sciences, P/Bag 360, Blantyre, Malawi, Email [email protected]
Background: The Modified Early Obstetric Warning systems (MEOWS) has received global endorsement as a key strategy for reducing maternal mortality over the past decade. However, evidence on MEOWS acceptability among midwives in sub-Saharan Africa, including Malawi, remains limited. Understanding how potential users perceive a newly introduced intervention is required to assess acceptability prior to implementation.
Purpose: To explore the acceptability of MEOWS among midwives using Sekhon’s Theoretical Framework of Acceptability.
Methods: We conducted an exploratory qualitative study between June and August 2025. Using purposive sampling, midwives across practicing, supervisory and policy making levels from Bwaila Hospital and Kamuzu Central Hospital were recruited for in-depth interviews. Data were analyzed using a deductive thematic approach with a priori coding guided by Sekhon et al’s Theoretical Framework of Acceptability (TFA).
Results: Thirty participants were interviewed. MEOWS was found acceptable across the seven domains of Sekhon et al’s TFA. Participants reported that MEOWS could guide clinical judgement and ease the workload. However, inadequate stationery and equipment were identified as key sources of burden that may threaten sustained use.
Conclusion: This study demonstrated that MEOWS was broadly acceptable among the various levels of midwives. The study identified inadequate stationery and equipment as potential barriers. Addressing these challenges may sustain MEOWS adaptation and implementation,enable early identification of maternal critical illness and reduction of maternal deaths.
Keywords: MEOWS, acceptability, midwives, maternal mortality, Malawi, implementation
Introduction
The recent trends in maternal morbidity and mortality have declined globally from 529 per 100,000 live births in 2000 to 223/100,000 live births in 2020.1 Evidence-based strategies are being implemented globally to address the high mortality rate.2,3 Sixty percent of maternal deaths have been identified as preventable, with delays in diagnosis and timely intervention recognized as key factors, necessitating the early identification of those at risk of developing maternal critical illnesses.4
While patient screening platforms in health facilities have undergone innovation over the past years, many low-income countries, including Malawi, rely on non-invasive low-cost means for continuous physiologic observation.5 Changes in the acceptable physiological parameters precede complications during pregnancy and the postpartum period.6
Recently, comorbidity-based screening tools have been developed and validated to assist in the early recognition of maternal clinical instability which may predict ICU admission.7 The Confidential Enquiry into the Maternal and Child Health (CEMACH) report in the United Kingdom recommended the use of the MEOWS tool to improve the early identification and management of pregnant women at risk of developing critical illness.8 MEOWS is a risk-stratified scoring system that measures a patient’s comorbidity burden through vital signs and other clinical observations to predict and forecast the severity of maternal morbidity and mortality.9 A trigger is defined a single markedly abnormal physiological parameter in the red zone or two mildly abnormal physiological parameters in the yellow zone.10 Abnormal parameters are classified as mildly or markedly abnormal. The implementation of MEOWS has been extensively recommended to enhance the rapid recognition and management of women at risk of developing maternal critical illness.11–14
With a mortality ratio of 381/100000 live births in 2020, Malawi is still far from achieving the Sustainable Development Goal target 3.1 of <70 deaths per 100000 live births by 2030.15 There is an urgent need for the implementation of warning systems to enable early detection and prompt management of women at risk of developing maternal critical illnesses. While MEOWS has been highly recommended, evidence on MEOWS’ acceptability across the practicing, supervisory and policy midwifery levels, particularly in low income countries remains limited. This study addresses that gap by assessing the acceptability of MEOWS in a Malawian context using the Theoretical Framework of Acceptability (TFA). The framework provides a coherent structure for assessing user acceptability before, during and after the introduction of an intervention. For this study we assessed prospective acceptability of MEOWS which may identify modifiable barriers early, inform adaptation and implementation planning for maternal critical care and support the reduction of maternal mortality in Malawi.
Materials and Methods
Study Design, Sampling and Setting
This was an exploratory qualitative study that explored the prospective acceptability of the MEOWS among midwives. The study recruited 30 participants from Kamuzu Central Hospital (KCH) and Bwaila Hospital in the Lilongwe District. One prospective participant declined to be interviewed because of time constraints. KCH and Bwaila Hospital were chosen because they are the largest public referral facilities for maternity cases in Malawi. Purposive sampling was used to enrol study participants. The eligible participants were nursing and midwifery officers, registered midwives, nursing and midwifery technicians, who had worked in the maternity unit for a minimum of three months and had a minimum of one year of clinical experience. We included frontline, supervisory and policy making midwifery staff to triangulate data across clinical, management and policy levels. In purposive sampling, certain types of participants who share important perspectives on the subject under investigation are deliberately sampled.16 Sampling continued until saturation was achieved. Midwives who had worked in the maternity unit for a minimum of three months were included in the study. Midwives with less than three months’ experience in the maternity unit were excluded.
Data Collection
Data collection was done between June and August 2025. One researcher conducted the in-depth face-to-face interviews to ensure consistency in probing, rapport building and application of the interview guide. To mitigate the potential interviewer variability the interview guide was piloted and reviewed by the experienced researchers. Reflexive memos were kept for the interviews. Regular peer debriefing sessions were held with co -researchers to ensure credibility. Data were collected in a private room within the maternity unit. The interview guide was informed by Sekhon’s theoretical framework of acceptability, piloted and reviewed by experienced researchers. Minor refinements were made for clarity. The interviews were conducted in English, audio recorded, and transcribed verbatim. Unique identification numbers were assigned to the participants.
To ensure the trustworthiness of the qualitative data, the credibility, transferability, dependability, and confirmability stipulated by Lincoln and Guba’s criteria17 were followed. In-the-moment member checking was done by asking the participants for immediate elaboration and clarification. Peer debriefing with research supervisors and experts was conducted to enhance the trustworthiness and rigor of the study. Thick descriptions of the study findings were provided to ensure transferability. Peer debriefing was done to check for consistency and interpretive bias.
Data Analysis
Thematic analysis was conducted following Braun and Clarke’s six-step framework.18 The researcher familiarised herself with the data, where an overview of the data was done prior to analysis of individual items through transcribing audio, reading texts, and note taking. The collected data were categorised into predetermined themes derived from the seven constructs of Sekhon’s Theoretical Framework of acceptability; Affective Attitude, Burden, Ethicality, Intervention Coherence, Opportunity Costs, Perceived Effectiveness and self Efficacy19 The manuscript was produced, and the thematic analysis was reported. A priori codebook was developed from the seven TFA constructs.19 There were no data segments requiring categorisation outside the coding matrix, suggesting the theoretical adequacy of TFA in this context. Regular discussions were held with research team to review the coded extracts and the application of the codebook to ensure consistency. Reflexive memos were regularly kept for bias identification and methodological transparency. Data were manually analysed.
Ethical Approval
This study was conducted in accordance with the Declaration of Helsinki principles.20 Study approval was granted by the College of Medicine Research and Ethics Committee (COMREC) (Reference: P.04/25-1489). Institutional approval was obtained from Kamuzu Central Hospital and the Director of Health and Social Services for Lilongwe District. Written informed consent which included permission to publish anonymised responses and direct quotes was obtained from all study participants.
Results
Participants Characteristics
The sample of 30 midwives included 80% female (n=24) and 20% male (n= 6) participated in this study. The midwives’ cadres included Nurse Midwife Technicians, Registered Nurse Midwives, and Nursing/Midwifery Officers. The participants’ ages ranged from 23–50 years (Table 1).
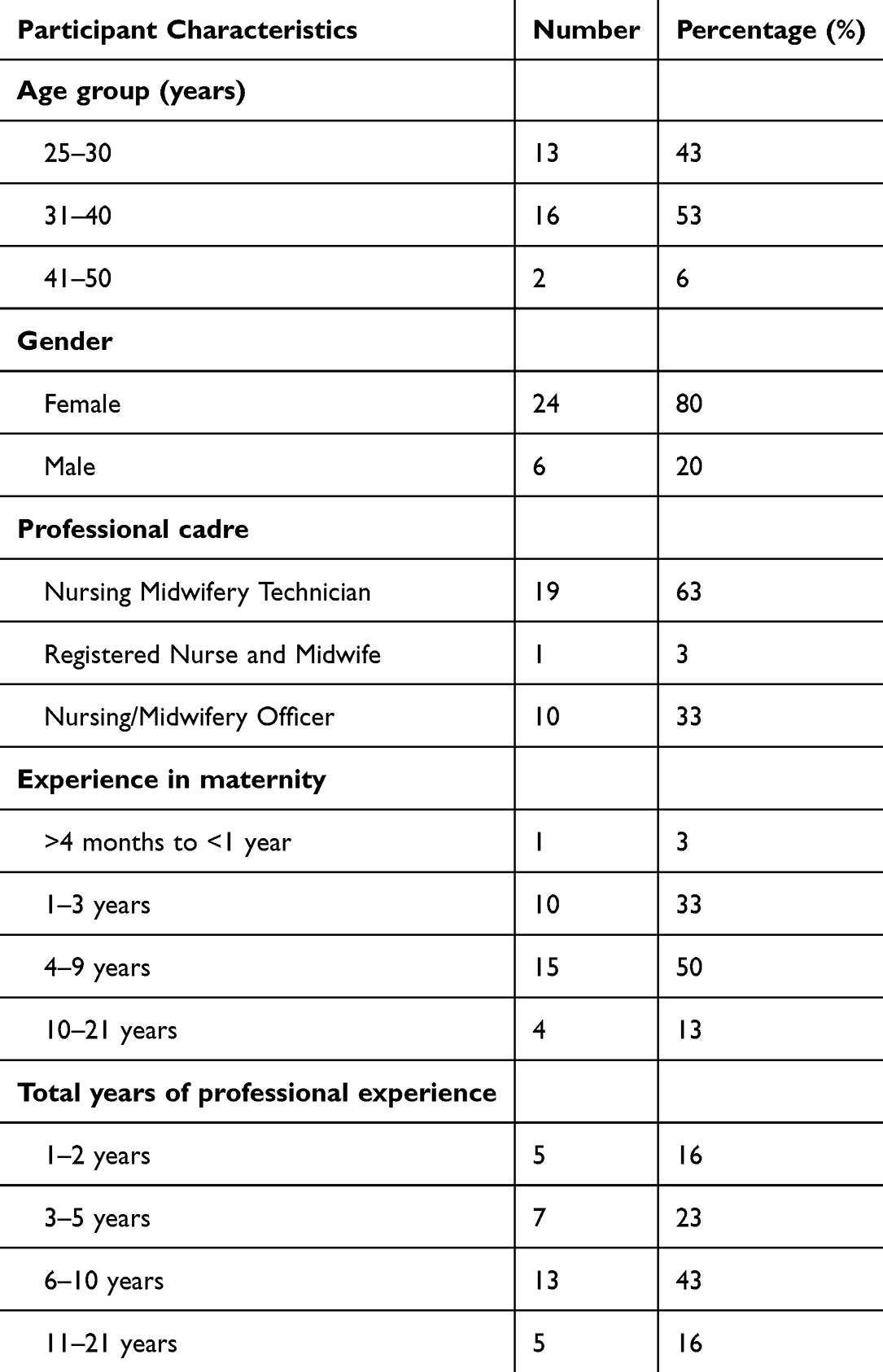 |
Table 1 Demographic Characteristics of Participants |
Affective Attitude
Affective attitude explores an individual’s feelings about an intervention.19 In this study, affective attitudes were explored by asking about the midwives’ feelings towards the introduction of the use of MEOWS at their facility. Midwives across all levels displayed a positive attitude towards introducing the MEOWS describing the MEOWS as a helpful guide that improved the quality of care.
I would be happy and would receive it if it can be introduced in this institution because it will help to improve the care to the patients. Participant 1
Furthermore, midwives felt that the tool was a helpful guide that would ease their work.
I feel that the tool can be helpful because it is user-friendly in terms of its design. Participant 16.
I feel that it (the MEOWS tool) will make our work easier. Participant 4.
Leaders and policymakers felt that MEOWS would ease their work and its use would be a justification for lobbying for adequate midwifery staff.
As a midwife in- charge MEOWS would make my work easier because having that system would justify calling for extra staff thereby maximizing care. Participant 11
Burden
The construct examines the extent of effort perceived by an individual to participate in an intervention.19 This study assessed the perceived effort by allowing participants to describe what would make the use of MEOWS easy or difficult for screening maternal critical illnesses.
It can make my work difficult when resources are lacking. Sometimes we do not have enough stationery. Participant 12.
Front-line midwives felt that frequent, monitoring required more midwives and resources.
However, the challenge is that if there are no resources, I will fail to use this Modified Early Obstetric Warning System. When the ward is very busy, it can be a challenge to do every day. However, with time, I think we will get used to it, and it will be better for us. Participant 19.
Ethicality
Ethicality considers the extent to which an individual feels that an intervention aligns with their personal values.19 Participants’ views were explored to determine how the use of MEOWS fits their individual values. A common view across the midwifery levels was that the MEOWS ensured the early identification of warning signs and prevented harm to both the mother and baby.
What I value most is seeing a patient come to this hospital alive and leave alive. Participant 10.
Sometimes, it becomes difficult to recognise the danger signs in women. This tool will help determine whether the patient is going into a critical state or not, and implement the specific care needed. Therefore, this will help to have a live baby and a live mother who, at the end of the day, will both go home healthy. So it will help me to realize my values. Participant 16.
Intervention Coherence
The construct evaluates the extent to which an individual understands how the intervention works.19 Participants across the levels demonstrated their understanding of the MEOWS by describing how the MEOWS is used.
This tool is in three categories, whereby we have the normal zone, the yellow zone and the red zone. So the normal zone is for those patients who have their parameters falling within normal ranges. For the yellow zone, at least two abnormal parameters. The red zone is for patients whose parameters are exceedingly higher than those in the yellow zone. Therefore, if one has at least a single parameter in the red zone, that will be categorized as having triggered. Participant 8.
Leaders and policy makers considered induction of new staff and students to MEOWS as a central approach for building intervention coherence.
Incorprate the use of MEOWS in the induction programme for new midwives and students. Participant 12.
Opportunity Cost
Opportunity cost considers the degree to which benefits, values, or profits must be given up when an individual engages in an intervention.19 Across all midwifery levels, the availability of resources and time were perceived as justified investments which must be made when the MEOWS is followed.
Sometimes you remember that you are supposed to do this, but do not have the resources to assess the patient. In addition, due to staff shortages, staff sometimes decide to take shortcuts and not do the right thing, even though we know it. Because maybe there are many patients, I do not think that you can have time to assess the patient so that you can check all the parameters needed on that patient. Participant 13.
However, Perspective of leaders and policy makers diverged based on their perception time. While some leaders regarded time as an investment to be given up, others considered time as a gain.
using MEOWS ideally, should help in timely patient intervention and ensuring that they get the maximum care they can get Participant 11
Although the costs of using MEOWS were identified, the benefits outweighed the costs.
This will benefit our profession as some parameters are missed unknowingly. This means that the patient will be assisted appropriately. It would also be a good thing for the midwives because sometimes you feel bad when something happens to a mother knowing that you could have done something. This would also help us reduce maternal deaths in our setting. Therefore, it would be beneficial to us. So, it is good and needs to be introduced here in our setting. Participant 13.
Perceived Effectiveness
Perceived effectiveness assesses the degree to which an intervention is perceived to likely achieve its intended purpose.19 Participants perceived that the use of MEOWS is more likely to contribute positively to the screening of maternal critical illness. The MEOWS was rated highly across the midwifery levels.
I can give it a 100% because it contains all the vital signs that you can use to assess the patient and the well-being of the mother… All the vital signs are included. Therefore, you will be able to assess whether the patient is ill. Participant 21.
I think we are going to prevent maternal deaths because there will be early identification and management. Therefore, it will have a positive impact on healthcare. Participant 6.
Furthermore, leaders and policy makers felt that using MEOWS would facilitate prompt decision-making and guide the next steps of care.
The midwife can make a decision easily, whether to consult a senior or not. Participant 17.
Self-Efficacy
Self-efficacy describes an individual’s confidence in their ability to perform a behavior as demanded by a particular intervention.19 Participants across the levels demonstrated confidence in MEOWS, citing the clear demarcation of parameter findings into zones according to severity.
Since it is used to detect early obstetric warning signs, it would be very easy for me because I would just be following the vital components which I am supposed to assess on the mothers. Very easy because everything is well explained. Participant 2
So by just looking at it, after doing the vital signs, I will know this woman is falling under the normal zone, or the yellow zone or the red zone. Participant 7
Discussion
Using the TFA, this study explored MEOWS acceptability across frontline, leaders and policy making midwives in two busy hospitals of Malawi. The study findings demonstrate convergent and divergent views across participants and the TFA constructs. The system was generally endorsed for its perceived simplicity, effectiveness, and alignment with professional values for midwives.
A convergent perception emerged across levels of midwives. Frontline cadres demonstrated that MEOWS would ease their work. This positive effective attitude mirrors findings from studies on acceptability of screening tools done in Uganda21,22 and Ethiopia,23 where health-care providers endorsed the tools for being easy to use. Cross level convergence on affective attitude may facilitate MEOWS adoption through clinical utility for front-line midwives’ positives and leadership support and policy advocacy for leaders and policy-makers in Malawi.
The study highlighted stationery and basic resource scarcity as a possible challenge that could limit MEOWS’ implementation. The reported perception of the stationery and resource burden by front-line midwives, leaders and policy makers reflects a cross level convergence that is necessary for bridging the policy practice gap. In similar studies on acceptability of a new health care interventions stationery challenges were documented24–26 The studies identified lack of budget for stationery and equipment. Involvement of midwifery leaders and policy makers is an important consideration for ensuring sustainability of MEOWS implementation. For the system to be successful, participants highly recommended institutional support.
In line with previous studies that applied Sekhon’s acceptability framework to assess the acceptability of a healthcare intervention, the study findings demonstrated a positive attitude towards the use of MEOWS among midwives.27,28 The study suggests that the use of MEOWS would provide a clear direction for the management of maternal conditions and early identification of maternal critical illness.
Participants believed that MEOWS aligned with their individual and professional values and ensured that patients received the right care. These study findings reflect a seamless fit with the core values of midwives, which contribute to the best possible maternal and foetal outcomes.29
The participants demonstrated strong intervention coherence. They had a clear understanding of the MEOWS and clearly articulated the triage guidance using the three MEOWS categories and triggers (two findings in the yellow zone and one in the red zone).
Strengths and Limitations
The use of in-depth interviews and the theoretical framework of acceptability provided rich data that helped in understanding the midwives’ perceptions of the use of MEOWS. Additionally, purposive sampling enabled the selection of participants who were likely to provide rich data on the acceptability of the MEOWS tool. This study assessed the prospective acceptability of MEOWS using a small sample. This approach is prone to limited generalisability.
Conclusion
This study offers novel evidence of MEOWS acceptability among Malawian midwives, with participants highlighting its potential to support early recognition of maternal deterioration and prevent maternal critical illness. However, acceptability was limited by shortage of resources including stationery which increased opportunity costs for frontline midwives. While leaders perceived low advocacy burden, institutional limitation may affect implementation. Prior to MEOWS implementation, facilities must address the perceived resource gaps to ensure sustainability. Outcome studies are needed to evaluate MEOWS impact on maternal Health outcomes in Malawi. These findings underscore the need for implementation preparedness as a prerequisite for sustainable MEOWS adoption in Malawi.
Data Sharing Statement
Data is available upon reasonable request from the corresponding author.
Acknowledgments
The authors acknowledge all the participating midwives for their contribution to this study, Dr Patrick Mapulanga for the technical assistance during the write up of this paper.
Author Contributions
All authors made a significant contribution to the work reported. This included conception, study design, execution, acquisition of data, analysis and interpretation of data; took part in drafting, revising or critically reviewing the article; gave the final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agreed to be accountable for all aspects of the work.
Funding
The authors did not receive funding for this study.
Disclosure
The authors declare that they have no conflicts of interest in this work.
References
1. World Health Organization. Trends in maternal mortality 2000 to 2020: estimates by WHO, UNICEF, UNFPA, world bank group and UNDESA/population division. World Health Organization; 2023. Available from: https://apps.who.int/iris/bitstream/handle/10665/372247/9789240069251-eng.pdf.
2. Jacob A. Mind the gap: analyzing the impact of data gap in Millennium Development Goals’(MDGs) indicators on the progress toward MDGs. World Dev. 2017;93:260–8. doi:10.1016/j.worlddev.2016.12.016
3. Kilemi B. Threats related to maternal mortality in Kenya: a systematic review. Br J Multidiscip Adv Stud. 2023;4(1):129–148. doi:10.37745/bjmas.2022.0110
4. Padilla CR, Shamshirsaz A. Critical care in obstetrics. Best Pract Res Clin Anaesthesiol. 2022;36(1):209–225. doi:10.1016/j.bpa.2022.02.001
5. Ryu D, Kim DH, Price JT, et al. Comprehensive pregnancy monitoring with a network of wireless, soft, and flexible sensors in high-and low-resource health settings. Proc Natl Acad Sci U S A. 2021;118(20):e2100466118. doi:10.1073/pnas.2100466118
6. Kuate Defo A, Daskalopoulou SS. Alterations in vessel hemodynamics across uncomplicated pregnancy. Am J Hypertens. 2023;36(4):183–191. doi:10.1093/ajh/hpac132
7. Shields A, De Assis V, Halscott T. Top 10 pearls for the recognition, evaluation, and management of maternal sepsis. Obstet Gynecol. 2021;138(2):289–304. doi:10.1097/AOG.0000000000004471
8. Singh A, Guleria K, Vaid NB, Jain S. Evaluation of maternal early obstetric warning system (MEOWS chart) as a predictor of obstetric morbidity: a prospective observational study. Eur J Obstet Gynecol Reprod Biol. 2016;207:11–17. doi:10.1016/j.ejogrb.2016.09.014
9. Kaur J, Thompson C, McLeod S, Varner C. Application of the Modified Early Obstetrical Warning System (MEOWS) in postpartum patients in the emergency department. Can J Emerg Med. 2023;25(6):481–488. doi:10.1007/s43678-023-00500-7
10. Singhal S, Acharya N, Madaan S, Mohammad S, Acharya S. Use of the modified early obstetric warning system chart as a predictor of peri-partum obstetric morbidity in a rural teaching institute: a two-year cross-sectional study. J Family Med Primary Care. 2022;11(12):7644–7651. doi:10.4103/jfmpc.jfmpc_320_22
11. Hannola K, Hoppu S, Mennander S, Huhtala H, Laivuori H, Tihtonen K. Obstetric early warning system to predict maternal morbidity of pre-eclampsia, postpartum hemorrhage and infection after birth in high-risk women: a prospective cohort study. Midwifery. 2021;99:103015. doi:10.1016/j.midw.2021.103015
12. Hedriana HL, Wiesner S, Downs BG, Pelletreau B, Shields LE. Baseline assessment of a hospital-specific early warning trigger system for reducing maternal morbidity. Int J Gynaecol Obstet. 2016;132(3):337–341. doi:10.1016/j.ijgo.2015.07.036
13. Pandya ST, Mangalampally K. Critical care in obstetrics. Indian J Anaesth. 2018;62(9):724–733. doi:10.4103/ija.IJA_577_18
14. Zuckerwise LC, Lipkind HS. Maternal early warning systems—towards reducing preventable maternal mortality and severe maternal morbidity through improved clinical surveillance and responsiveness. Semin Perinatol. 2017;41(3):161–165. doi:10.1053/j.semperi.2017.03.005
15. Gondwe MJ, Mndala L, Kondoni C, et al. Ending preventable maternal deaths in Malawi: the stakeholders consensus approach to identify maternal health needs priorities. BMC Health Serv Res. 2025;25(1):357. doi:10.1186/s12913-025-12120-x
16. Akkaş H, Meydan CH. Sampling methods in qualitative sampling in multicultural settings. In: Principles of Conducting Qualitative Research in Multicultural Settings. IGI Global Scientific Publishing; 2024:33–56. doi:10.4018/979-8-3693-3306-8.ch003
17. Lincoln YS. Naturalistic Inquiry. Vol. 289. Sage; 1985.
18. Braun V, Clarke V. Using thematic analysis in psychology. Qual Res Psychol. 2006;3(2):77–101. doi:10.1191/1478088706qp063oa
19. Sekhon M, Cartwright M, Francis JJ. Acceptability of health care interventions: a theoretical framework and proposed research agenda. Br J Health Psychol. 2018;23(3):519–531. doi:10.1111/bjhp.12295
20. Shrestha B, Dunn L. The declaration of Helsinki on medical research involving human subjects: a review of seventh revision. J Nepal Health Res Counc. 2019;17(04):548–552. doi:10.33314/jnhrc.v17i4.2443
21. Mugyenyi GR, Byamugisha JK, Tumuhimbise W, Atukunda EC, Fajardo YT. Customization and acceptability of the WHO labor care guide to improve labor monitoring among health workers in Uganda. An iterative development, mixed method study. PLOS Glob Public Health. 2024;4(5):e0002780. doi:10.1371/journal.pgph.0002780
22. Musaba MW, Nantale R, Wandabwa JN, et al. Acceptability of the Moyo device for intrapartum fetal heart rate monitoring at a referral hospital in Uganda: a qualitative study. BMC Pregnancy Childbirth. 2025;25(1):658. doi:10.1186/s12884-025-07521-x
23. Tilahun KN, Adem JB, Atinafu WT, Walle AD, Mengestie ND, Birhanu AY. Intention to use mobile-based partograph and its predictors among obstetric health care providers working at public referral hospitals in the oromia region of Ethiopia in 2022: cross-sectional questionnaire study. Online J Public Health Inform. 2024;16:e51601. doi:10.2196/51601
24. Koech A, Musitia PM, Mwashigadi GM, et al. Acceptability and feasibility of a low-cost device for gestational age assessment in a low-resource setting: qualitative study. JMIR Hum Factors. 2022;9(4):e34823. doi:10.2196/34823
25. Malel ZJ, Wapary E, Lueth GD, et al. Feasibility of labor care guide (LCG) implementation in South Sudan, creating recommendations from evaluating the LCG use in health facilities. Study and recommendations by the Association of Gynecologists and Obstetricians of South Sudan (AGOSS). Int J Gynaecol Obstet. 2026. doi:10.1002/ijgo.15782
26. Godfrey MR, Atukunda EC, Tumuhimbise W, Farjardo YF, Byamugisha J. Exploring potential opportunities and strategies of using the labour care guide to improve labour monitoring and health outcomes among health care providers in Uganda: a qualitative study. BMC Pregnancy Childbirth. 2025;25(1):1272. doi:10.1186/s12884-025-08199-x
27. Samuelsson M, Möllerberg ML, Neziraj M. The Swedish theoretical framework of acceptability questionnaire: translation, cross-cultural adaptation, and descriptive pilot study evaluation. BMC Health Serv Res. 2025;25(1):684. doi:10.1186/s12913-025-12855-x
28. Timm L, Annerstedt KS, Ahlgren JÁ, et al. Application of the theoretical framework of acceptability to assess a telephone-facilitated health coaching intervention for the prevention and management of type 2 diabetes. PLoS One. 2022;17(10):e0275576. doi:10.1371/journal.pone.0275576
29. Baldwin A, Capper T, Harvey C, Willis E, Ferguson B, Browning N. Promoting nurses’ and midwives’ ethical responsibilities towards vulnerable people: an alignment of research and clinical practice. J Nurs Manag. 2022;30(7):2442–2447. doi:10.1111/jonm.13783
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.