Back to Journals » Pragmatic and Observational Research » Volume 8
Abortion, an increasing public health concern in Ecuador, a 10-year population-based analysis
Authors Ortiz-Prado E ![]() , Simbaña K
, Simbaña K ![]() , Gómez L
, Gómez L ![]() , Stewart-Ibarra AM, Scott L, Cevallos-Sierra G
, Stewart-Ibarra AM, Scott L, Cevallos-Sierra G
Received 5 December 2016
Accepted for publication 8 March 2017
Published 13 July 2017 Volume 2017:8 Pages 129—135
DOI https://doi.org/10.2147/POR.S129464
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor David Price
Video abstract presented by Esteban Ortiz-Prado
Views: 698
Esteban Ortiz-Prado,1–4 Katherine Simbaña,5,6 Lenin Gómez,5,6 Anna M Stewart-Ibarra,4,7 Lisa Scott,8 Gabriel Cevallos-Sierra9
1OneHealth Research Group, Faculty of Medicine, Universidad De Las Americas, Quito, Ecuador; 2Department of Cellular Biology, Physiology and Immunology, Institute of Biomedicine, Universitat de Barcelona, Spain; 3Department of Physiology, Faculty of Medicine “Eugenio Espejo”, Universidad Tecnologica Equinoccial, Quito, Ecuador; 4Department of Medicine, College of Medicine, 5Center for Global Health and Translational Science, Upstate Medical University, State University of New York, Syracuse, NY, USA; 6Faculty of Medical Science, School of Medicine, Universidad Central del Ecuador, 7Prometeo Program, SENESCYT, Quito, Ecuador; 8Graduate College of Biomedical Sciences, Western University of Health Sciences, Lebanon, OR, USA; 9School of Public Health, University of Heidelberg, Heidelberg, Germany
Objectives: To describe the epidemiology of abortion in Ecuador from 2004 to 2014 and compare the prevalence between the public and the private health care systems.
Methods: This is a cross-sectional analysis of the overall mortality and morbidity rate due to abortion in Ecuador, based on public health records and other government databases.
Results: From 2004 to 2014, a total of 431,614 spontaneous abortions, miscarriage and other types of abortions were registered in Ecuador. The average annual rate of abortion was 115 per 1,000 live births. The maternal mortality rate was found to be 43 per 100,000 live births.
Conclusions: Abortion is a significant and wide-ranging problem in Ecuador. The study supports the perception that in spite of legal restrictions to abortion in Ecuador, women are still terminating pregnancies when they feel they need to do so. The public health system reported >84% of the national overall prevalence.
Keywords: clandestine abortion, private vs public health system, misoprostol, therapeutic abortion, metrotexate, misoprostol
Introduction
Every minute there are on average 255 births worldwide1 from around 210 million pregnancies annually. Eighty million of those pregnancies are unplanned or unwanted and 1 in 2 of these are terminated before birth, representing more than 41 million abortions a year.2–5 About 47,000 women die every year due to complications from unsafe abortions, 86% of which occur in developing countries.6–8 Unsafe and clandestine abortions represent a great risk for women and therefore are an urgent public health matter.
Studies have shown that banning elective termination of pregnancy is associated with an increase in clandestine abortion practices and associated medical complications that arise when abortions are performed under unsafe conditions.6,9 In some South American countries, such as Ecuador, Peru and Colombia, elective abortion is criminalized under most circumstances.10,11 However, there are a few Latin American countries and territories, such as Puerto Rico, Cuba, Uruguay and Mexico, where there are legal grounds that allow women to terminate unwanted pregnancies.12,13 In South America, the rates of unsafe abortion are one of the highest in the world.14
Restrictive laws for abortion and clandestine and unsafe practices to terminate pregnancy become even more relevant in the current Zika virus outbreak. Zika virus has been linked to severe neurological malformations in babies born from infected mothers. This has increased the demand for pregnancy termination in Latin American countries.15–17 Clandestine and unsafe abortions are more common in poor and very young women who lack access to medical services and, unfortunately, these women are also the ones who might be most affected by the Zika outbreak.14,15
Ecuador has prohibited any form of induced abortion since 1837, when the first Penal Code of Conduct was published.18 This code stated that abortions could not be requested by women for any economic, social or personal reason. Furthermore, abortions were considered illegal regardless of fetal wellbeing.19 In January 2014, the Penal Code of Conduct was ratified and therapeutic abortion was approved under specific circumstances that were limited to mentally ill or incompetent women who had been raped or cases where the woman’s physical or mental health was in direct danger as a result of the pregnancy itself.19,20
A study published in 1990 by The Bull Institute shows that there was a notable increase in the overall rate of abortions in Ecuador from 1964 to 1988.21 However, the lack of data from that period makes it difficult to ascertain whether the increase was due to an incremental rise in the number of miscarriages or induced abortions, or simply to an improvement in data collection. The study identified social determinants that were linked to abortion. It showed that most unwanted pregnancies occurred in the rural, mountainous regions of Ecuador, typically within low-income families.22 The validity of these findings is difficult to prove, due to widespread underreporting of intentionally induced abortions, most likely due to the legal consequences previously described.4,6,23
Although there are legal constraints that limit access to abortion services in Ecuador, access to some drugs such as misoprostol, an off-label abortive pill, is possible. Misoprostol is a prostaglandin E1 analog with regulatory approval in Ecuador to treat gastroduodenal ulcers but can also be used to induce abortion, either as oral pills or by vaginal placement.24 Misoprostol and its off-label indications as an abortive pill works when taken before the 63rd day of gestation, having a reported success rate for pregnancy termination higher than 90% if done within this time frame.24–29
The aim of this study is to describe the epidemiology of abortion in Ecuador from 2004 to 2014 as well as to describe its current trends. At the same time, we compared the prevalence of abortion between the public and private health care systems in Ecuador. Finally, we report the current trends in misoprostol marketing in the country in order to find if there is any correlation between the annual misoprostol consumption and the annual abortion rate.
Methods
National, provincial and regional data were analyzed from the Ministry of Public Health’s national databases of Vital Statistics Deaths and Births Databases from 2004 to 2014, Hospital Discharges Database from 2004 to 2014 and the Population Census of the National Institute of Census and Statistics (INEC) from 2010. Data includes annual hospital cases, mortality, and number of live births. Demographic characteristics of women including age, province of residency and type of establishment were analyzed. The number of units of off-label abortive drugs sold was obtained from local purchase of medications retrieved from government pharmaceutical company Enfarma EP, up to 2015.
We used the following terms to retrieve the information corresponding to the International Classification of Diseases 10th revision (ICD-10): Medically Justified abortion (ICD O04), spontaneous abortion (ICD O03) and other pregnancies that resulted in abortion (ICD O00-O02, O05-O08).
The data used is public, anonymized, thus the local regulatory agency does not require an IRB approval or ethics review.
We performed a Pearson correlation in order to find if there is any correlation between the use of the misoprostol off-label abortive pill with the rate of abortion in Ecuador, assuming the distribution of abortion rate and of misoprostol were both normally distributed. The raw data was analyzed, saved and managed within the Microsoft Excel™ software and episheet stat open source statistical software was used for descriptive and frequency analyses. References citation and retrieval were managed by Zotero Open Source Software version 4.0.11. Spatial analysis was performed using QGIS 2.8.
Results
Prevalence of abortion in Ecuador
Between 2004 and 2014, a total of 431,614 miscarriages and abortions that met any of the ICD-10 abortion classifications (spontaneous abortion, justified medical abortion or other pregnancies that ended in abortion) were reported in Ecuador within the national Hospital Discharges Database (Table 1).
 | Table 1 Distribution of abortions in Ecuador from 2004 to 2014 according to ICD category Abbreviation: ICD-10, International Classification of Diseases 10th revision. |
The number of annual spontaneous and induced abortion registrations combined ranged from 33,132 in 2004 (108/1,000) to over 40,256 (124/1,000) in 2013 and decreased to 35,711 (112/1,000) in 2014 when the abortion ban was ratified.
From 2004 to 2014, there was an annual average of 39,236 abortions, and 2011 reported the highest number ever recorded, reaching more than 42,500 abortions countrywide.
There is an inter-annual variability in registered abortion rates. The average rate of abortions during the evaluated period (2004 to 2014) was 115 per 1,000 live births (Figure 1). The rate of abortions per 1,000 women aged 15–44 was 7.86 in 2004 and 13.43 in 2010. From 2004 to 2014, 189 abortion-related deaths were reported to the Ministry of Health (Table 2), resulting in a maternal mortality rate of 44 per 100,000 registered abortions.
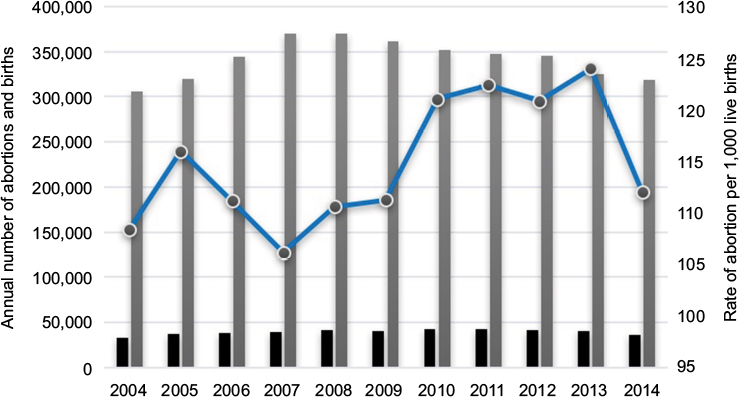 | Figure 1 Annual number of abortions and births in Ecuador from 2004 to 2014. Notes: Left axis represents the number of abortions (black bars) and births (grey bars). Right axis represents the annual abortion rates per 1,000 live births (blue line). |
 | Table 2 Number of recorded deaths related to abortion in Ecuador from 2004 to 2014 Notes: *Other pregnancies that ended in abortion. |
Geographical distribution of abortion in Ecuador
During the evaluated period (2004 to 2014), we found that all the provinces in Ecuador reported a considerably high number of abortions in absolute numbers and abortions to birth ratios. A significant geographic difference in the number of abortions is reported countrywide. When all the data from the last 11 years were plotted, we found the highest numbers to be reported in the biggest and most populated province. Guayas reported a total number of 696,038 abortions in the last 11 years, followed by Pichincha (487,344) Manabí (266,348) Los Ríos (154,487) and Azuay (130,358) (Figure 2).
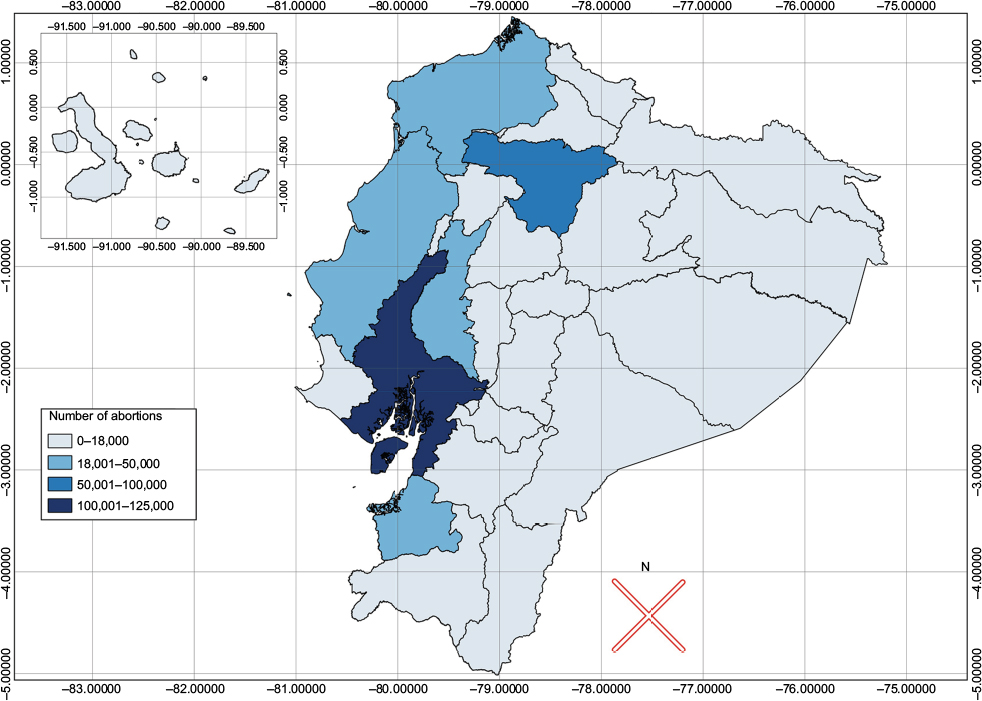 | Figure 2 Number of abortions from 2004 to 2014 per province in Ecuador. Note: The insert is a zoomed image of the Galapagos Islands, an archipelago located 200,000 miles off the coast of Ecuador with an estimated population of 25,000 people. |
When we compared the number of abortions with the number of births per province, we found that other provinces were at the top of the list. The highest abortion ratios by the number of births was found in Pastaza, a province with a ratio of 186/1,000 births, followed by Pichincha (174/1,000), Guayas (166/1,000), Galapagos Islands (165/1,000), and Esmeraldas with (164/1,000), (Figure 3).
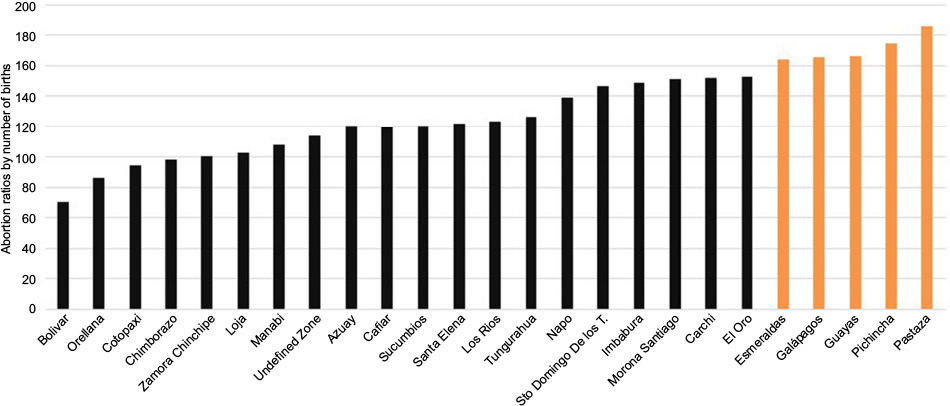 | Figure 3 Overall accumulated abortion ratio by number of births among the provinces of Ecuador from 2004 to 2014. Note: The top 5 provinces are colored in orange bars. |
Private versus public health system
The results show that 84.3% of abortions were managed within the public health system, while 15.7% occurred within all the clinics and hospitals from the private for-profit and non-profit subsystems. The majority of cases that were reported within the public health system came from hospitals of the Ministry of Public Health (88%), while the rest were seen among hospitals from the Army, Police, some Universities, local governments and other charitable centers (12%). Women who received medical attention within the private health care system were distributed among the private for-profit (87%) and non-profit private centers (13%).
Misoprostol consumption in Ecuador
According to the annual government expenditure on drugs and the private pharmaceutical consumption given by Enfarma EP database, during the last 9 years, misoprostol sold an average of 70,000 tablets per year. We performed a Pearson correlation to find if there is any correlation between the use of this off-label abortive pill with the rate of abortion in Ecuador. The results show that a weak trend may be indicated between abortion rates and units of misoprostol sold in Ecuador (r=0.63, p=0.069); however, these results were not statistically significant as we set the p-value at p<0.05 (Figure 4).
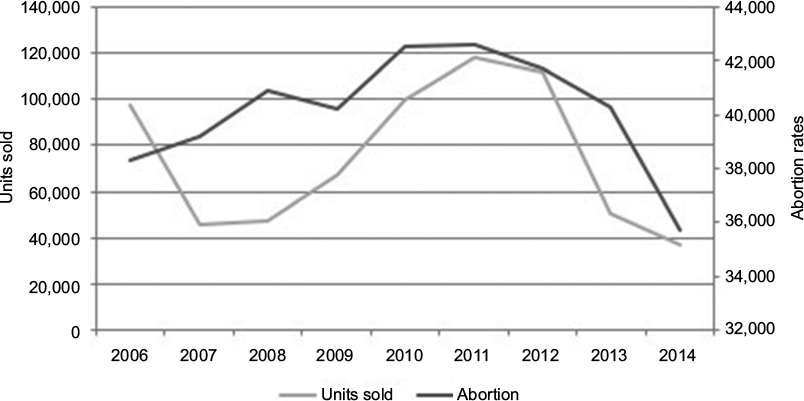 | Figure 4 Overall accumulated abortion rates and units of misoprostol sold from 2004 to 2014. Note: Correlation coefficient =0.63, p=0.069. |
Discussion
Although abortion rates in women of childbearing age have shown an important reduction in the last two decades, the data in developing countries is not always available.30 In countries with similar socioeconomic situation, abortion rates per every 1,000 births average 34 to 45 abortions per 1,000 women of childbearing age.31 Understanding abortion rates and demographic distribution among women in South America and Ecuador is important in order to establish the basis of the problem, to provoke further research, and also to encourage deeper analysis with the objective of providing good evidence to support policy making. Our findings are an important part of demonstrating the basis of abortion in Ecuador.
In Ecuador this preventable condition and its impact on women’s wellbeing and the entire health system, including the economic impact of the disability-adjusted life year and the related quality-adjusted life year measurements have not being evaluated yet; however, authorities are concerned with the increasingly higher numbers being reported to the national database.32 According to the data collected, women undergoing a medically justified abortion (ICD O04), spontaneous abortion (ICD O03) and other types of pregnancies that resulted in abortion (ICD O00-O02, O05-O08) are seeking medical care within the public health system rather than the private system 333,963 (84%) vs 61,940 (16%). This might indicate that poorer women with less education and poorer access to health care are the ones seeking medical attention if an abortion is inevitable.33
Due to the lack of data, the causes of differences in abortion ratios by province have not been studied yet; however, cultural, educational and better health care systems might be related to the higher number of abortions among the most populated provinces.34 When we compared the number of abortions with the number of children born each year, we observed that Pastaza, one of the least populated provinces with high cultural diversity, reported more abortions than any other provinces with numbers totaling 186/1,000 births. This trend might support the fact that some places with lower education levels and poorer access to health care infrastructure have higher rates of abortion among their women, forcing them to travel long distances in many cases to obtain the procedure.35,36
Although we are unable to distinguish between arbitrarily induced or self-induced abortions and miscarriages in this study, the data support evidence from prior studies that some women in Ecuador are intentionally terminating their pregnancies despite the ban on abortions.21,23,34 Interestingly, during the analyses, we found that abortion rates had declined in 2014. This behavior might correspond to the fact that during 2014 the new Organic Penal Code was approved, which punished abortion with up to 2 years of jail time either to the health care provider or to the woman who was aborting.19 In our experience, and partially supported by our results, abortion is intentionally induced in many women countrywide.21 We suspect that this is often accomplished through the use of misoprostol to induce cervix dilation.37–39
Despite the fact that the use of these medications for the purpose of causing abortions is not indicated for those without a physician’s prescription, more than 75% of drugs that require a prescription in Ecuador are sold without one.40 Thus, obtaining misoprostol, might not be that difficult.41,42 Other medications that are widely used as abortive pills (eg, mifepristone) are not publicly available in Ecuador.
The wide availability of potential medicines that can cause abortion allows women to affect the course of their pregnancies without proper medical assistance or counseling.
We believe clandestine abortions are often documented as “spontaneous” or “medically justified abortions”.14,43 Doctors are prohibited from performing any procedure that is intended to terminate unwanted pregnancy.19 However, when women arrive at the emergency room (ER) with vaginal bleeding (presumably due to self-induced cervix dilation with misoprostol), documentation of the ER service automatically changes to “spontaneous abortion” or “medically justified abortion”. Thus, causality is extremely difficult to demonstrate.25,44
Once the discussion focuses on rights, evidence, and figures, politicians will understand that women who want to abort will do so, regardless of where or with whom they do it.45
Despite the results, we experienced important limitations that were out of our control, including the information available that did not allow for differentiation between self-induced abortions and miscarriages. Additionally, we do not have any information about a number of unreported instrumental or procedural abortions that occur in clandestine facilities or those that occurred at home after self-administration of abortive pills and did not cause significant complications.46
Conclusion
In Ecuador, abortion is a public health concern, affecting more than 39,000 women every year. Since abortion is a highly controversial subject, and due to many sociocultural factors that influence public perception of the procedure, self-induced abortions might be very difficult to demonstrate and quantify in this study.
On the other hand, since demonstrating the presence of clandestine abortions is complicated, the relationship between misoprostol/abortion rates might offer some clue regarding the presence of this health problem, although this issue needs to be investigated thoroughly due to the severe health risks that these drugs pose to women terminating pregnancies.
The study supports the perception that in spite of legal restrictions to abortion in Ecuador, women are still terminating pregnancies when they feel they need to do so. Experience from developed countries shows that legal and open access pregnancy termination services reduce mortality related to abortion and its complications. Abortion restrictions in Ecuador have not reduced the practice of clandestine or unconventional pregnancy terminations. Although more study is required, it would be wise to encourage discussion within the public policy sector regarding access to medically controlled termination of pregnancies in order to reduce any more unnecessary deaths in women.
Disclosure
The authors report no conflicts of interest in this work.
References
The World Bank. Population, total; 2014. Available from: http://data.worldbank.org/indicator/SP.POP.TOTL#. Accessed November 20, 2014. | ||
World Health Organization, Geneva. Estrategia de salud reproductiva. [Reproductive health strategy]. Available from: http://apps.who.int/iris/bitstream/10665/69040/1/WHO_RHR_04.8_spa.pdf. Accessed December 1, 2016. | ||
Pazol K, Zane SB, Parker WY, et al. Abortion surveillance–United States, 2008. MMWR Surveill Summ. 2011;60(15):1–41. | ||
Goldman L, García S, Díaz J, Yam E. Brazilian obstetrician-gynecologists and abortion: a survey of knowledge, opinions and practices. Reprod Health. 2005;2:10. | ||
Sedgh G, Singh S, Hussain R. Intended and unintended pregnancies worldwide in 2012 and recent trends. Stud Fam Plann. 2014;45(3):301–314. | ||
Faúndes A, Hardy E. Illegal abortion: consequences for women’s health and the health care system. Int J Gynecol Obstet. 1997;58(1):77–83. | ||
Ahman E, Shah I. Unsafe abortion: worldwide estimates for 2000. Reprod Health Matters. 2002;10(19):13–17. | ||
WHO, others. Safe Abortion: Technical and Policy Guidance for Health Systems. Geneva: WHO; 2012. Abailable from: http://apps.who.int/iris/bitstream/10665/70914/1/9789241548434_eng.pdf. Accessed January 1, 2017. | ||
Finer L, Fine JB. Abortion law around the world: progress and pushback. Am J Public Health. 2013;103(4):585–589. | ||
Dador Tozzini MJ. El aborto terapéutico en el Perú; 2012. [Therapeutic abortion in Peru]. Available from: http://www.clacaidigital.info:8080/xmlui/handle/123456789/483. Accessed September 29, 2015. | ||
Guzmán JM, Contreras JM, Hakkert R. La situación actual del embarazo y el aborto en la adolescencia en América Latina y el Caribe. [Current situation of pregnancy and abortion among adolescents in Latin American and the carribean]. Burak SD Adolesc Juv En América Lat Costa Rica LUR. 2001:391–424. | ||
Becker D, Díaz Olavarrieta C. Decriminalization of abortion in Mexico City: the effects on women’s reproductive rights. Am J Public Health. 2013;103(4):590–593. | ||
Vazquez V, Camargo AM, Acosta M, Alonso V, Luna F. Reproductive pattern of Cuban women living in the municipality of plaza de la revolución, Havana, Cuba. J Biosoc Sci. 2015;47(04):493–504. | ||
Grimes DA, Benson J, Singh S, et al. Unsafe abortion: the preventable pandemic. Lancet. 2006;368(9550):1908–1919. | ||
Aiken AR, Scott JG, Gomperts R, Trussell J, Worrell M, Aiken CE. Requests for abortion in Latin America Related to Concern about Zika Virus Exposure. N Engl J Med. 2016;375(4):396–398. | ||
Hodge JG, Corbett A, Repka A, Judd PJ. Zika virus and global implications for reproductive health reforms. Disaster Med Public Health Prep. 2016;10(5):713–715. | ||
Miller M. Infected with Dogma: How South America’s Response to the Zika Virus Fails Women. Humanist. 2016;76(2):9. | ||
Starkoff PC. Despenalización del aborto y nuevo proyecto constitucional: un tema polémico. [Decriminalization of abortion and the new constitutional project: A polemic issue]. Íconos-Rev Cienc Soc. 2013;(32):19–23. | ||
Asamblea Nacional. Nuevo Codigo Penal Ecuatoriano. [Integral organic criminal code]. 2014. Available from: http://www.justicia.gob.ec/wp-content/uploads/2014/05/c%C3%B3digo_org%C3%A1nico_integral_penal_-_coip_ed._sdn-mjdhc.pdf. Accessed December 1, 2016. | ||
Asamblea Nacional. Constitucion Ecuatoriana del 2008. [Constitution of the Republic of Ecuador 2008]. Available from: http://www.oas.org/juridico/pdfs/mesicic4_ecu_const.pdf. Accessed December 1, 2016. | ||
Fassin D. EL ABORTO EN EL ECUADOR (1964-1988) Propuesta para una lectura de las estadísticas hospitalarias. [Proposal for a correct interpretation of hospitalization statistics]. Bull Inst Fr Andin. 1990;19(1):215–231. | ||
Eggleston E. Causas determinantes de embarazos no planeados en el Ecuador. [Determinants causes of unplanned pregnancies in Ecuador]. Perspect Int En Planif Fam. 1999:2–8. | ||
Lafaurie MM, Grossman D, Troncoso E, et al. El aborto con medicamentos en América Latina. Las experiencias de las mujeres en México, Colombia, Ecuador y Perú. [Medical Abortion in Latin America. The experiences of women in Mexico, Colombia, Ecuador and Peru]. Popul Counc Gynuity Health Proj. 2005. http://www.clacaidigital.info:8080/xmlui/handle/123456789/50. Accessed November 13, 2014. | ||
MacDonald K, Norman WV, Popescu O. New anomalies due to methotrexate and misoprostol exposure in early pregnancy. Int J Gynaecol Obstet. 2013;122(3):267–268. | ||
Manouana M, Kadhel P, Koffi A, Janky E. [Illegal abortion with misoprostol in Guadeloupe]. J Gynécologie Obstétrique Biol Reprod. 2013;42(2):137–142. French. | ||
Kulier R, Kapp N, Gülmezoglu AM, Hofmeyr GJ, Cheng L, Campana A. Medical methods for first trimester abortion. Cochrane Database Syst Rev. 2011;(11):CD002855. | ||
Wiebe ER. Methotrexate with or without misoprostol to terminate pregnancies with no gestational sac visible by ultrasound. Int J Gynaecol Obstet Off Organ Int Fed Gynaecol Obstet. 2009;107(1):64–65. | ||
Dunn S, Panjwani D, Gupta M, Meaney C, Morgan R, Feuerstein E. Comparison of remote and in-clinic follow-up after methotrexate/misoprostol abortion. Contraception. 2015;92(3):220–226. | ||
Roudsari FV, Ayati S, Shakeri MT. Efficacy of combination therapy with methotrexate and misoprostol in termination of pregnancy in the first trimester. Iran J Med Sci. 2015;34(2):116–120. | ||
Chandra-Mouli V, Camacho AV, Michaud PA. WHO guidelines on preventing early pregnancy and poor reproductive outcomes among adolescents in developing countries. J Adolesc Health. 2013;52(5):517–522. | ||
Singh S, Wulf D. Estimated levels of induced abortion in six Latin American countries. Int Fam Plan Perspect. 1994;20(1):4–13. | ||
Instituto Ecuatoriano de Estadisticas y Censos. Ecuador en Cifras. Anuario de Estadisticas Hospitalarias: Camas y Egresos 2014. [Ecuador in numbers. Hospital statitics, discharges and morbility, 2014]. 2014. Available from: www.inec.gob.ec. Accessed December 1, 2016. | ||
Ortiz-Prado E, Ponce J, Cornejo-Leon F, et al. Analysis of health and drug access associated with the purchasing power of the ecuadorian population. Glob J Health Sci. 2016;9(1):201. | ||
Dzuba IG, Winikoff B, Peña M. Medical abortion: A path to safe, high-quality abortion care in Latin America and the Caribbean. Eur J Contracept Reprod Health Care. 2013;18(6):441–450. | ||
Fotso JC, Ezeh A, Madise N, Ziraba A, Ogollah R. What does access to maternal care mean among the urban poor? factors associated with use of appropriate maternal health services in the slum settlements of Nairobi, Kenya. Matern Child Health J. 2009;13(1):130–137. | ||
Essendi H, Mills S, Fotso JC. Barriers to formal emergency obstetric care services’ utilization. J Urban Health. 2011;88(2):356–369. | ||
Costa SH, Vessey MP. Misoprostol and illegal abortion in Rio de Janeiro, Brazil. Lancet. 1993;341(8855):1258–1261. | ||
Khoo CL, Meskhi A, Harris CP. Fatal Clostridium septicum following medical termination of pregnancy. J Obstet Gynaecol. 2013;33(5):530–537. | ||
Cittadini F, Loyola G, Caradonna L, Minelli N, Rossi R. A case of toxic shock due to clandestine abortion by misoprostol self-administration. J Forensic Sci. 2014;59(6):1662–1664. | ||
Ortiz-Prado E, Galarza C, Cornejo León F, Ponce J. Acceso a medicamentos y situación del mercado farmacéutico en Ecuador [Access to drugs and the situation of the pharmaceutical market in Ecuador]. Rev Panam Salud Pública. 2014;36(1):57–62. Spanish. | ||
Kourilovitch M, Galarza-Maldonado C, Ortiz-Prado E. Diagnosis and classification of rheumatoid arthritis. J Autoimmun. 2014;48–49:26–30. | ||
Anand BS, Graham DY. Ulcer and gastritis. Endoscopy. 1999;31(2):215–225. | ||
Sedgh G, Henshaw S, Singh S, Ahman E, Shah IH. Induced abortion: estimated rates and trends worldwide. Lancet. 2007;370(9595):1338–1345. | ||
Allen R, O’Brien BM. Uses of misoprostol in obstetrics and gynecology. Rev Obstet Gynecol. 2009;2(3):159–168. | ||
Paxman JM, Rizo A, Brown L, Benson J. The clandestine epidemic: the practice of unsafe abortion in Latin America. Stud Fam Plann. 1993;24(4):205–226. | ||
Kopp Kallner H, Fiala C, Stephansson O, Gemzell-Danielsson K. Home self-administration of vaginal misoprostol for medical abortion at 50-63 days compared with gestation of below 50 days. Hum Reprod Oxf Engl. 2010;25(5):1153–1157. |
 © 2017 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2017 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.