Back to Journals » Therapeutics and Clinical Risk Management » Volume 14
A vascular access and midlines program can decrease hospital-acquired central line-associated bloodstream infections and cost to a community-based hospital
Authors Pathak R ![]() , Gangina S
, Gangina S ![]() , Jairam F, Hinton K
, Jairam F, Hinton K
Received 20 April 2018
Accepted for publication 22 June 2018
Published 21 August 2018 Volume 2018:14 Pages 1453—1456
DOI https://doi.org/10.2147/TCRM.S171748
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Garry Walsh
Rahul Pathak, Sumalatha Gangina, Falina Jairam, Kimberly Hinton
University of Central Florida School of Medicine and Heart of Florida Regional Medical Center, Davenport, FL, USA
Background: We propose that substituting central lines with midlines can help reduce the total number of central line catheter-days as well as central line-associated bloodstream infections (CLABSIs), thereby reducing the associated costs and the resulting increased length of stay. A midline or vascular access program in a community hospital can bring about these positive changes.
Objectives: Our objective is to evaluate whether the institution of a midline program for vascular access at a community hospital can reduce the number of central line catheter-days and the associated CLABSI rate, incidence, and cost.
Materials and methods: We collected data on the number of central line catheter-days per year starting from 2012. We also collected data on the total number of patient-days during this period and the number of CLABSIs. We started Centers for Disease Control and Prevention (CDC)-based recommendations to help decrease CLABSIs in June 2014; this included the use of the central venous catheters (CVC) insertion bundles and CVC maintenance bundle. Chlorhexidine baths were also given to all patients with central lines. In June 2015, we started a midline program and tracked data till June 2017. We then compared the infection rates during these periods.
Results: We conclude that instituting CDC recommendations to decrease CLABSIs did bring down the CLABSI rate; this decrease was not statistically significant. However, the addition of the midline program to replace central lines whenever possible, combined with universal CDC recommendations, did result in a significant decrease in both the number of central line days per patient-day and the CLABSI rate.
Conclusion: We recommend hospitals to develop a midline program to help reduce the use of central line catheters when possible to reduce the total number of catheter-days and the CLABSI rate associated with them.
Keywords: central line-associated bloodstream infections, midline, venous access, hospital-acquired infections, hospital length of stay, quality of care
Introduction
Central venous catheters are the most common source of hospital-acquired bloodstream infections in the US. Each infection has an estimated additional cost of $25,000/- per episode.1 There are up to 250,000 episodes reported in the US per year, each episode increasing the cost and duration of the hospital stay.2 The Centers for Disease Control and Prevention (CDC) has released many guidelines to help prevent and reduce catheter-related bloodstream infections, and this has helped bring down the rate of infections significantly.3,4 However, the number of central venous catheter-days remains close to 15 million catheter-days per year.5 The CDC reports a 50% decrease in central line-associated bloodstream infection (CLABSI) rate from 2008 to 2014 and a 9% decrease between 2013 and 2014. The CDC introduced general guidelines to decrease and prevent CLABSI in 2009 (hospital acquired infections data reports on CDC website). Nevertheless, about 30,100 CLABSIs still occur in the intensive care units and wards of US acute care facilities each year.6
In addition to bloodstream infection, central lines are also associated with significant complications including bleeding, pneumothorax, and arrhythmias.7
Midline catheters are intravenous (IV) devices placed in deep peripheral veins (eg, basilic, brachial, cephalic) usually under ultrasound guidance. They are between 3 and 10 inches in length (8–25 cm), and their tips reside distal to the axillary vein.8,9 These catheters are termed “midlines” because they are longer than peripheral IV catheters, which are generally 1–3 inches long, and shorter than peripherally inserted central catheters (PICCs), which extend into the vena cava. Several studies have demonstrated that central line use can be decreased by the use of midline catheters.10–13 Two studies recently showed that the use of central venous catheters was decreased by 80%–85% in an emergency department setting over the span of 5 years by using midlines instead.11,13 Another study recently demonstrated a decrease in the rate of CLABSI by introducing a midline program in a ventilator unit.12
In a recent 2-year study, the rate of bacteremia in midline catheters was reported to be 0.3%.14 We wanted to study whether introducing a midline program can help bring the rate and incidence of CLABSI down in a small community hospital.
Materials and methods
This was a retrospective review of the data collected over the past 5 years from our infection control department. This study was determined to be a non-human subjects research, and a waiver for informed consent was granted by the University of Central Florida institutional review board. There were no patient identifiers used in this data for our study. We collected data on the number of central line catheter-days per year starting from 2012. We also collected data on the total number of patient days during this period and the number of CLABSI.
We started CDC-based recommendations to help decrease CLABSI in June 2014; this included the use of the central venous catheters (CVC) insertion bundles and CVC maintenance bundle. Chlorhexidine baths were also given to all patients with a central line.
We started a midline program in June 2015. With the introduction of this program, we replaced central lines in the hospital whenever possible by midlines. We had a vascular access team available to do this. All emergency central lines and central lines placed for total parental nutrition and ionotropic medications were replaced when possible by midlines. Central lines placed for difficult IV access were replaced by midlines. We then compared the bloodstream infection rate from these periods. We excluded infections in central line ports for chemotherapy and infections in hemodialysis catheters, as these cannot be replaced by midlines. Various data including the organism cultured, and the location in the hospital where the central line was placed, were also accumulated.
The number of catheter-days for any calendar year was determined by the sum total number of central line catheters in the hospital each day for that calendar year. Thus, the annual CLABSI rate is reported as the total number of CLABSI/total number of catheter-days×1,000 for each calendar year.
The data from 2012 and 2013 were compared to 2014 after the institution of CDC recommendations for CVC maintenance bundle. Then, the data from 2012 and 2013 were compared to 2015 onward – the period wherein we instituted the combined use of CVC maintenance bundle and the midline protocol.
For our statistical analysis, we used the data analysis firm called Instat Services Inc. (San Diego, CA, USA). They compared the rates of infections using the Fisher’s exact test to compare different interventions.
Results
When we introduced the universal CVC bundle recommended by the CDC, the CLABSI rate decreased, but not significantly (P=0.5768). However, the addition of midline program to replace central lines reduced the CLABSI rate significantly as compared to the use of CVC bundle alone (Table 1). Moreover, the combination of the CVC bundle plus the midline program was very significant in terms of CLABSI reduction when compared with the previous period during which there were no measures in place (P=0.003 and P=0.0113, respectively).
 | Table 1 Data broken up into periods when CDC guidelines were implemented alone and when CDC guidelines were implemented along with the midline program |
The total number of catheter-days also fell significantly (Table 2), and the catheter-days per patient-day had a significant drop as well (P<0.001).
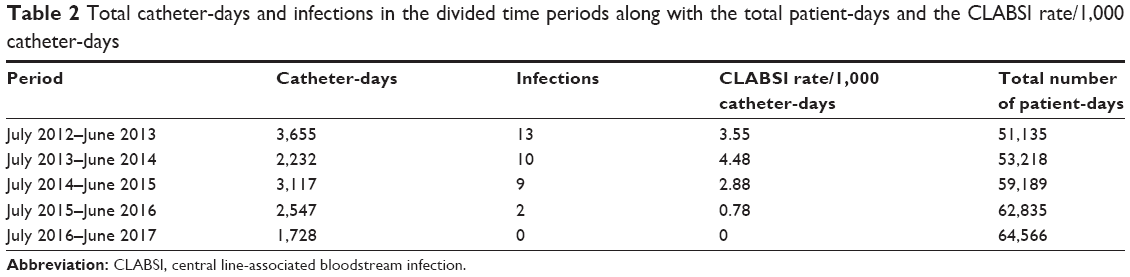 | Table 2 Total catheter-days and infections in the divided time periods along with the total patient-days and the CLABSI rate/1,000 catheter-days |
Fisher’s exact test was used to calculate significance (analysis provided by Instat Services Inc.).
Discussion
Central lines are necessary and help in improving the management of patients. When needed for the delivery of vesicant medications, inotropic medications, and management of intensive care unit patients, there are few options besides large-bore central line access. However, with the associated complications and CLABSIs, we should try other alternatives as well. Midlines are an excellent mode of venous access that, like central lines, can deliver large-volume fluids and can be placed for up to 4 weeks at a time.9,10,12 With a bloodstream infection rate of only 0.3%, they are much safer and less complicated than central lines.14
Midline catheters are peripheral IV access devices between 3 and 10 inches in length (8–25 cm). These catheters are generally placed under ultrasound guidance in proximal veins such as the brachial or cephalic with the tip distal to the axillary vein.12 Newer midlines made of novel co-polymers and treated for reduced biofilm formation are safer than the older ones and cause less thrombophlebitis. Midlines can easily be inserted by a trained vascular access nurse instead of a physician, unlike central lines. We do not need X-rays to confirm the position, as we do for central lines. It is an easy procedure and takes only a few months to set up a vascular access team with the experience to place midlines and PICC lines. Some hospitals already have special nurses trained to insert PICC lines; to teach them midline insertion takes very little time.
Studies have already shown that starting a midline program can decrease the overall number of central lines inserted in a hospital emergency room.10–13 The greatest number of infections associated with central lines are from those inserted in emergency situations where standard precautions may not be possible. Other studies have shown that a midline program can reduce the overall number of catheter-days and CLABSI rate in a ventilator unit.
Our study shows that midlines can decrease the overall incidence of CLABSIs in a community hospital after a midline program is initiated.
It saves the cost in a number of ways:
- Inserted by a nurse rather than a physician.
- No post-insertion X-ray needed to confirm position.
- Decreases the incidence of CLABSI and the associated costs to the hospital.
- Patients who require to be discharged with IV medications can go home or to the nursing home with a midline.
- No complications such as bleeding, pneumothorax, or cardiac arrhythmias.
- The chance of getting a deep vein thrombosis is <2% as opposed to 1%–38.5% with a PICC line.14,15
Setting up a midline program will also help other nursing units when there is difficulty in IV access. Midlines will eliminate the need for central lines for conditions such as long-term venous access, difficult venous access, irritable medication infusions, and large volume infusions. More recently invented midlines boast a near-zero bloodstream infection rate with proper insertion techniques.
Conclusion
The setting up of a vascular access program in a hospital where midlines are used to replace central lines when feasible significantly decreases the number of catheter-days within the hospital and also significantly reduces the rate of CLABSI alone or in combination with universal CDC recommendations, including CVC bundle. We recommend hospitals to develop a midline program to help reduce the use of central line catheters when possible. This will help to reduce the total number of catheter-days and the infection rate associated with them.
Disclosure
The authors report no conflicts of interest in this work.
References
Pittet D, Tarara D, Wenzel RP. Nosocomial bloodstream infection in critically ill patients. Excess length of stay, extra costs, and attributable mortality. JAMA. 1994;271(20):1598–1601. | ||
Haddadin Y, Regunath H. Central line associated blood stream infections (CLABSI). StatPearls. Epub 2017 Mar 28. | ||
O’Grady NP, Alexander M, Burns LA, et al. Guidelines for the prevention of intravascular catheter-related infections. Clin Infect Dis. 2011;52(9):e162–e193. | ||
O’Grady NP, Alexander M, Burns LA, et al. Summary of recommendations: guidelines for the prevention of intravascular catheter-related infections. Clin Infect Dis. 2011;52(9):1087–1099. | ||
Mcgee DC, Gould MK. Preventing complications of central venous catheterization. N Engl J Med. 2003;348(12):1123–1133. | ||
Bell T, O’Grady NP. Prevention of central line-associated bloodstream infections. Infect Dis Clin North Am. 2017;31(3):551–559. | ||
Kornbau C, Lee KC, Hughes GD, Firstenberg MS. Central line complications. Int J Crit Illn Inj Sci. 2015;5(3):170–178. | ||
O’Grady NP, Chertow DS. Managing bloodstream infections in patients who have short-term central venous catheters. Cleve Clin J Med. 2011;78(1):10–17. | ||
Deutsch GB, Sathyanarayana SA, Singh N, Nicastro J. Ultrasound-guided placement of midline catheters in the surgical intensive care unit: a cost-effective proposal for timely central line removal. J Surg Res. 2014;191(1):1–5. | ||
Shokoohi H, Boniface K, Mccarthy M, et al. Ultrasound-guided peripheral intravenous access program is associated with a marked reduction in central venous catheter use in noncritically ill emergency department patients. Ann Emerg Med. 2013;61(2):198–203. | ||
Schoenfeld E, Shokoohi H, Boniface K. Ultrasound-guided peripheral intravenous access in the emergency department: patient-centered survey. West J Emerg Med. 2011;12(4):475–477. | ||
Pathak R, Patel A, Enuh H, Adekunle O, Shrisgantharajah V, Diaz K. The incidence of central line-associated bacteremia after the introduction of midline catheters in a ventilator unit population. Infect Dis Clin Pract (Baltim Md). 2015;23(3):131–134. | ||
Au AK, Rotte MJ, Grzybowski RJ, et al. Decrease in central venous catheter placement due to use of ultrasound guidance for peripheral intravenous catheters. Am J Emerg Med. 2012;30(9):1950–1954. | ||
Goetz AM, Miller J, Wagener MM, Muder RR. Complications related to intravenous midline catheter usage. A 2-year study. J Intraven Nurs. 1998;21(2):76–80. | ||
Cummings M, Hearse N, Mccutcheon H, Deuter K. Improving antibiotic treatment outcomes through the implementation of a midline: piloting a change in practice for cystic fibrosis patients. J Vasc Nurs. 2011;29(1):11–15. |
 © 2018 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2018 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.