Back to Journals » Research and Reports in Urology » Volume 15
A Unique Case of Inflatable Penile Prosthesis (IPP) Implantation and Mesh Phalloplasty in a Patient Born with Congenital Fusiform Megalourethra
Authors Berrettini A, Paraboschi I, Di Grazia M, Gnech M, Mantica G, Minoli DG, De Marco EA, Manzoni G, Capece M, Palmieri A, Ralph D, Mirone V
Received 14 September 2022
Accepted for publication 8 February 2023
Published 15 February 2023 Volume 2023:15 Pages 85—89
DOI https://doi.org/10.2147/RRU.S387042
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Panagiotis J Vlachostergios
Alfredo Berrettini,1 Irene Paraboschi,1 Massimo Di Grazia,1 Michele Gnech,1 Guglielmo Mantica,2 Dario Guido Minoli,1 Erika Adalgisa De Marco,1 Gianantonio Manzoni,1 Marco Capece,3 Alessandro Palmieri,3 David Ralph,3 Vincenzo Mirone3
1Department of Pediatric Urology, Fondazione IRCCS Ca’ Granda Ospedale Maggiore Policlinico, Milano, Italy; 2Department of Urology, IRCCS Ospedale Policlinico San Martino, Genova, Italy; 3Department of Urology, Azienda Ospedaliera Universitaria “Federico II”, Napoli, Italy
Correspondence: Irene Paraboschi, Department of Pediatric Urology, Fondazione IRCCS Ca’ Granda Ospedale Maggiore Policlinico, Via Francesco Sforza 35, Milano, Italy, Tel +393313229495, Email [email protected]
Abstract: We present the first case of a patient born with congenital fusiform megalourethra who underwent the successful placement of an inflatable penile prosthesis (IPP) and mesh phalloplasty due to primary erectile dysfunction (ED). After an extensive psychosexual assessment and a preoperative MRI scan, an IPP was successfully implanted. The procedure was carried out through a penoscrotal approach, which offered excellent exposure to the crura and the proximal ends of the corpora cavernosa. Following the incision and the dilatation of both corpora cavernosa, the penile cylinders were inserted and a mesh phalloplasty was performed, to replace the erectile tissues lacking in the distal corpora cavernosa. After reservoir and pump placement, the device was tested, and no mechanical issues were recorded. The postoperative course was uneventful, and, at the 2-year follow-up, the patient reported highly satisfactory results, with valid functional erections.
Keywords: congenital fusiform megalourethra, inflatable penile prosthesis, phalloplasty, erectile dysfunction
Introduction
Congenital megalourethra is an extremely rare congenital anomaly of the male anterior urethra and erectile tissues, characterized by an enlargement of the pendulous urethra with no evidence of mechanical distal obstruction.1 Two main varieties have been described: the scaphoid type, caused by poor development of the corpus spongiosum, and the fusiform type, caused by a deficiency of the corpus spongiosum and hypoplastic corpora cavernosa.2
Congenital megalourethra is known to be associated with other anomalies of the genitourinary tract, being renal hypodysplasia, hydronephrosis, hydroureter, and vesicoureteral reflux (VUR) extremely common in these children.3
Due to the poor development of the erectile tissues of the penis, a functional urinary obstruction is usually seen at birth.4 Therefore, these children usually require planned urethroplasties or urinary diversion, depending on the child’s overall health status and the severity of the hypoplasia of the corpus spongiosum.1,5 Moreover, the commonly associated kidney anomalies usually required a close and regular follow-up with periodic renal function tests and imaging studies.
Although the prevalence of erectile dysfunction (ED) in this cohort of patients remains unknown, its occurrence at puberty needs to be assessed to prevent psychosocial maladjustment and psychiatric disorders.
This report illustrated the first case of a patient born with congenital fusiform megalourethra who underwent the successful implantation of an inflatable penile prosthesis (IPP) and mesh phalloplasty to achieve and maintain valid functional erections.
Case Report
A 20-year-old boy born with congenital fusiform megalourethra was referred to our department complaining of primary ED.
Antenatally, a massive bilateral hydronephrosis and renal hypodysplasia were detected ultrasonographically, while, at birth, the diagnosis of congenital megalourethra was made.
Due to functional urinary obstruction, he required a perineal urethrostomy at 6 months of age, which allowed him to completely empty his bladder. Moreover, he developed an early presenting end-stage renal disease (ESRD), which required renal replacement therapy from the age of 1 year.
Regarding his psychosexual functioning and adjustment, he complained of primary ED resistant to phosphodiesterase-5 inhibitors.
An MRI scan of his penis and pelvic floor was therefore requested, which showed a severe hypoplasia of the corpus spongiosum and a distal deficiency of both corpora cavernosa and confirmed the diagnosis of congenital fusiform megalourethra (Figure 1).
 |
Figure 1 Preoperative MRI scan of the penis and pelvic floor. Sagittal (A) and axial (B and C) images showed severe hypoplasia of the corpus spongiosum and distal deficiency of both corpora cavernosa. The prostate gland was small and almost difficult to identify. These findings were compatible with the diagnosis of the fusiform variety of congenital megalourethra. |
Following an extensive psychosexual assessment, he was finally considered eligible for genital surgery. In particular, his motivations and expectations were discussed together with the risk of intra- and postoperative complications, and an informed consent form was completed and signed.
Considering the young patient’s age and the advantages of more natural erections and better cosmetic outcomes,6 a three-component IPP was chosen (Titan® One-Touch Release, Coloplast Ltd®, Peterborough, Cambs, United Kingdom).
Surgical Technique
Surgery was performed using the penoscrotal approach, which has been described to afford excellent exposure of the crura and proximal corpora cavernosa, prevent pump migration and provide good cosmetic outcomes.7,8
In detail, a 4-cm transverse perineal incision was made 2 cm below the penoscrotal junction, a bilateral corporotomy was performed and a dilatation of both corpora cavernosa was accomplished up to three-quarters of the penile shaft. In accordance with the preoperative MRI findings, the erectile tissues of the corpora cavernosa extended 10 cm proximally and 18 cm distally to the corporotomy, ending at three-quarters of the penile shaft. Therefore, a controlled perforation of the distal parts of the corpora cavernosa and a dilatation up to the glans were required to add 5 more centimeters to the penile length.
A 22-cm Titan® One-Touch Release IPP (Coloplast Ltd, Peterborough, Cambs, United Kingdom) was then prepared using 1-cm rear tip extenders.
Moreover, considering the lack of erectile tissue in the distal corpora cavernosa, their partial reconstruction was deemed necessary using a Ultrapro® Macroporous Partially Absorbable Mesh (Ethicon US LLC) shaped as a 6-cm rounded cap and secured at the tip of the cylinders. Finally, the penile cylinders were inserted into the penis and the corpora cavernosa were sutured with absorbable stitches (Figure 2).
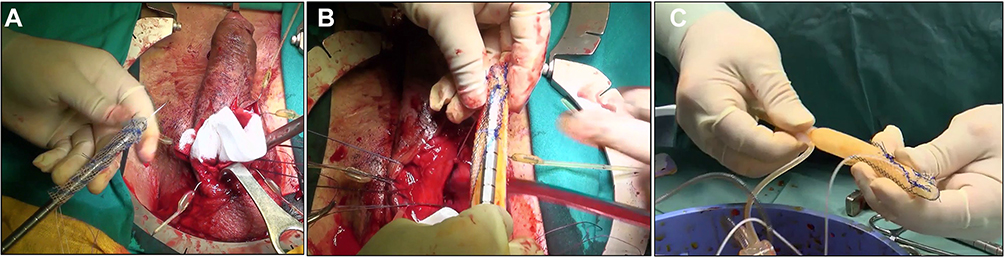 |
Figure 2 Intraoperative images showing the configuration of the inflatable penile prosthesis (IPP). Due to the lack of erectile tissue in the distal corpora cavernosa, an Ultrapro® Macroporous Partially Absorbable Mesh (Ethicon US LLC) shaped as a 6-cm rounded cap was shaped (A) and secured at the tip of the cylinders of the IPP (B and C). |
The reservoir was placed in the retropubic space while the pump was implanted in the right subdartos pouch. The device was tested to exclude any mechanical damage and was left partially inflated to minimize the formation of postoperative hematomas (Figure 3).
 |
Figure 3 Postoperative pictures documenting valid penile erections. Highly satisfactory results were documented at the end of the surgical procedure (A) and at the 2-year follow-up (B and C). A maximally turgid state was achieved by inflating the three-piece IPP using the scrotal pump placed in the right subdartos pouch. |
No intraoperative complications were reported and the postoperative course was uneventful. The device was completely deflated on POD7 and the patient was taught how to use it properly 4 weeks after surgery, gradually gaining confidence with both the inflation and the deflation of the device. At the last 2-year follow-up, the patient reported highly satisfactory results, being able to achieve and maintain valid functional erections.
Discussion
Congenital urological anomalies significantly contribute to the estimated rate of male sexual dysfunctions, which accounts for 31% of men aged 18–59 years.9,10 Amongst them, cryptorchidism, myelodysplasia, hypospadias, and penile curvature are the most frequently occurring, followed by posterior urethral valves, prune belly syndrome, epispadias-exstrophy complex, and congenital megalourethra.10
Being extremely rare (with less than 100 cases reported in the scientific literature),3 congenital megalourethra is a very challenging clinical condition. Not only patients are faced with issues related to the early surgical reconstruction of the urethra, but also with lifelong problems related to their sexual and reproductive functions.
Due to the congenital maldevelopment of the erectile tissues of the penis, different degrees of ED should be expected in these patients.11 Particularly, an imbalance between the length of the corpora cavernosa and the penile shaft may contribute to worsening the erectile function and adding complexity to the surgical treatment.
Therefore, at puberty, regular assessments of their sexual behaviors and psychosexual functioning are mandatory to prevent possible psychosocial maladjustment and psychiatric disorders. Low levels of genital touching and initiating sexual contact, depression, poor body concept, withdrawal, and anxiety are all elements that deserve to be appropriately assessed during periodic psychosexual counseling. The occurrence of ED needs to be early recognized and managed, and in patients experiencing this symptom, treatment options (including pharmacological therapies and surgical strategies) need to be discussed carefully.
In this regard, IPP is currently recognized as the most effective option to obtain a valid erectile function in those patients in whom the first-line pharmacological approach is contraindicated or ineffective.10
Here, we report the first case of a 20-year-old boy born with congenital fusiform megalourethra who required the placement of an IPP and a partial corpora reconstruction to treat his primary ED.
A three-component IPP was chosen (Titan® One-Touch Release, Coloplast Ltd, Peterborough, Cambs, United Kingdom) being these devices very sophisticated tools which offer several advantages over semirigid and two-piece prostheses.6,12–14 They are softer when deflated, provide better cosmetic results, and ensure more natural erections. Their disadvantages are related to the possible malfunction of their three components (penile prosthesis, reservoir, and pump) and tubing system and the need for a more complex surgical technique to implant them.6,12–14 Even if surgical outcomes are usually successful, several complications may occur, including infections, erosions, mechanical failures, and bladder or urethral injuries. Therefore, their implantation must be considered a delicate and complex surgery, especially when a congenital malformation of the genitourinary tract is the underlying condition.
Moreover, in this case, the lack of erectile tissue in the distal corpora cavernosa required their partial reconstruction using a partially absorbable mesh, which was shaped as a 6-cm rounded cap and secured at the tip of the cylinders.
In the scientific literature, several other authors have reported the use of meshes during IPP positioning and reconstructive phalloplasty. They have been adopted for increasing the prosthesis diameter,15 preventing device erosion during corporal reconstruction,16 or reinforcing the glans penis in case of distal penile prosthesis extrusion.17
Although the population of patients affected by congenital megalourethra is too few to provide definitive conclusions, our case illustrates that the penoscrotal implantation of an IPP and mesh phalloplasty can provide highly satisfactory results in the hands of experienced surgeons.
However, a careful patient selection should be always performed prior to surgery and patients’ complaining symptoms, motivations, and expectations need to be properly assessed to maximize surgical outcomes.
Since these devices have currently reached high levels of mechanical reliability and safety and the technology underlying penile prosthesis development is in constant evolution, the sexual function and satisfaction of patients born with congenital megalourethra are expected to significantly improve in the years to come.
Conclusion
Excellent sexual function and satisfaction can be achieved in patients born with congenital megalourethra experiencing primary ED. Improvements in the understanding of the pathophysiology of this congenital anomaly and advances in its surgical treatments hold promise for children born with this congenital defect.
Consent Statement
Written informed consent for publication was obtained from the patient, who consented to the publication of the case details and accompanying images.
Acknowledgments
This work was supported by the “Associazione per il Bambino Nefropatico ABN Onlus”, 20122, Via Commenda 16, Milan, Italy and by the “Centro di riferimento per le malformazioni congenite del rene e delle vie urinarie: prevenzione e cura del danno renale dal feto al bambino Sergio Bonelli”. This study was funded by the “Italian Ministry of Health – Fondazione IRCCS Cà Granda Ospedale Maggiore Policlinico, Milano”.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Stephens D, Fortune DW. Pathogenesis of megalourethra. J Urol. 1993;149(6):1512–1516. doi:10.1016/S0022-5347(17)36431-5
2. Dorairajan T. Defects of spongy tissue and congenital diverticula of the penile urethra. ANZ J Surg. 1963;32(3):209–214. doi:10.1111/j.1445-2197.1963.tb03031.x
3. Prakash S, Kumar V, Babu R, Mohan C. Isolated megalourethra: a rare case report and review of literature. J Indian Assoc Pediatr Surg. 2014;19(3):178. doi:10.4103/0971-9261.136481
4. Hakimi T. Congenital megalourethra. Annals Med Surg. 2022;84:104926. doi:10.1016/j.amsu.2022.104926
5. Wakhlu AK, Wakhlu A, Tandon RK, Kureel SN. Congenital megalourethra. J Pediatr Surg. 1996;31(3):441–443. doi:10.1016/S0022-3468(96)90758-7
6. Bettocchi C, Palumbo F, Spilotros M, et al. Penile prostheses. Ther Adv Urol. 2010;2(1):35–40. doi:10.1177/1756287209359174
7. Gupta NK, Ring J, Trost L, Wilson SK, Köhler TS. The penoscrotal surgical approach for inflatable penile prosthesis placement. Transl Androl Urol. 2017;6(4):628–638. doi:10.21037/tau.2017.07.32
8. Henry GD, Mahle P, Caso J, Eisenhart E, Carrion R, Kramer A. Surgical techniques in penoscrotal implantation of an inflatable penile prosthesis: a guide to increasing patient satisfaction and surgeon ease. Sex Med Rev. 2015;3(1):36–47. doi:10.1002/smrj.39
9. Laumann EO, Paik A, Rosen RC. Sexual dysfunction in the United States: prevalence and predictors. JAMA. 1999;281(6):537. doi:10.1001/jama.281.6.537
10. Taran I, Hartke DM, Palmer JS. Congenital genitourinary anomalies and sexual function. Int J Impot Res. 2007;19(2):115–118. doi:10.1038/sj.ijir.3901482
11. Pallas R, Palaniappan B, Brown G. Megalourethra as a rare cause for erectile dysfunction. Radiol Case Rep. 2015;10(2):1072. doi:10.2484/rcr.v10i2.1072
12. Lindeborg L, Fode M, Fahrenkrug L, Sønksen J. Satisfaction and complications with the Titan® one-touch release penile implant. Scand J Urol. 2014;48(1):105–109. doi:10.3109/21681805.2013.808695
13. Ohl DA, Brock G, Ralph D, et al. Prospective evaluation of patient satisfaction, and surgeon and patient trainer assessment of the Coloplast titan one touch release three‐piece inflatable penile prosthesis. J Sex Med. 2012;9(9):2467–2474. doi:10.1111/j.1743-6109.2012.02819.x
14. Shaw T, Garber BB. Coloplast titan inflatable penile prosthesis with one‐touch release pump: review of 100 cases and comparison with genesis pump. J Sex Med. 2011;8(1):310–314. doi:10.1111/j.1743-6109.2010.02064.x
15. Ghattas O, Doheim M, Kotb H, Burnett A. Modified malleable prosthesis with a fixed mesh: case series for the Ghattas technique. Asian J Androl. 2022;24(2):167. doi:10.4103/aja.aja_55_21
16. Lee WG, Venturino L, Ralph D. V07-07 Corporal reconstruction using lightweight mesh during penile prosthetic surgery. J Urol. 2021;206(Supplement3). doi:10.1097/JU.0000000000002034.07
17. Carson CC, Noh CH. Distal penile prosthesis extrusion: treatment with distal corporoplasty or Gortex windsock reinforcement. Int J Impot Res. 2002;14(2):81–84. doi:10.1038/sj.ijir.3900829
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.