Back to Journals » Research and Reports in Urology » Volume 15
A Triplicated Bladder with Diphallia; Rare Variant of Duplicate Exstrophy
Authors Gebreselassie HA, Godu BG ![]() , Assefa HG, Erge MG
, Assefa HG, Erge MG ![]()
Received 18 November 2022
Accepted for publication 28 February 2023
Published 3 March 2023 Volume 2023:15 Pages 109—112
DOI https://doi.org/10.2147/RRU.S397296
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Panagiotis J Vlachostergios
Hana Abebe Gebreselassie, Binyam Gebremedihin Godu, Hiwote Girma Assefa, Maru Gama Erge
St. Paul’s Hospital Millennium Medical College, Department of Surgery, Pediatrics Surgery Unit, Addis Ababa, Ethiopia
Correspondence: Hana Abebe Gebreselassie, St. Paul’s Hospital Millennium Medical College, Department of Surgery, Pediatrics Surgery Unit, Addis Ababa, Ethiopia, Tel +251 913 766 868, Email [email protected]
Background: Exstrophy variants are well described urologic anomalies. They are characterized by atypical anatomical and physical findings than those found in patients with classic bladder exstrophy and epispadias malformation. The combination of these anomalies with duplicated phallus is a rare occurrence. Here we present a neonate with a rare form of exstrophy variant associated with penile duplication.
Case Summary: One day old male neonate who was born at term was admitted to our neonatal intensive care unit. He had lower abdominal wall defect and open bladder plate with no visible ureteric orifices. There were two completely separate phalluses with penopubic epispadias and urethral orifices draining urine. Both testes were descended. Abdominopelvic ultrasound showed normal upper urinary tract. He was prepared and operated with intra operative finding of complete bladder duplication in the sagittal plane and each bladder has its own ureter. The open bladder plate which had no connection with both ureters and urethras was excised. The pubic symphysis was approximated without osteotomy and abdominal wall was closed. He was immobilized with mummy wrap. He had uneventful post-operative course and was discharged on the 7th post-operative day. He was evaluated on the 3rd month post operatively and he was thriving well with no complications.
Conclusion: The occurrence of a triplicated bladder along with diphallia is an exceptionally rare urologic anomaly. As a number of variations are possible in this spectrum, the management of neonates with this anomaly should be individualized.
Keywords: bladder duplication, exstrophy variant, diphallia, duplicate exstrophy
Introduction
Exstrophy variants are rare subsets of an infrequent urologic malformation which is bladder Exstrophy Epispadias complex. Classic bladder Exstrophy has an incidence of 1 in 40,000 to 50,000 live births and exstrophy variants occur 10 times less frequently than this figure making their incidence 2 per one million live births.1,2
Although a spectrum of disorders exists in these variants, they share the musculoskeletal defect of wide pubic diastasis and divergent rectus abdominis muscles. According to Marshal and et al the well-known exstrophy variants include superior vesical fissure, pseudo-exstrophy, duplicate exstrophy and superior vesical fistula.3 Other variants like covered exstrophy and inferior vesical fissure have been described then after showing the complexity of these malformations.4
The occurrence of this rare anomaly in combination with another unusual urologic malformation namely diphallia is an exceptional phenomenon. To our knowledge, this is the first report of such combination of complex urologic malformations.
Case Summary
One-day old male neonate who was born at term with a birth weight of 3000 grams was admitted to our neonatal intensive care unit. Upon examination, he was stable and active. He has no dysmorphic features. Chest and cardiac examination was unremarkable. On abdominal examination, he had infra umbilical midline abdominal wall defect with visible open bladder plate with no visible ureteric orifices. Pubic diastasis was 4 centimeters. There were two completely separate phalluses with epispadias and patent urethral orifices draining urine. Both testes were descended. No other skeletal deformity was noted (Figure 1). The anus was normally located and patent. The sacrum was also well noted upon palpation.
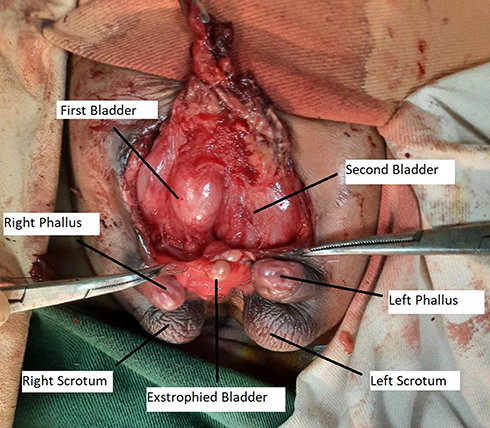 |
Figure 1 Intraoperative picture revealing a triplicated bladder with diphallia. |
Abdominopelvic ultrasound showed normal upper urinary tract. Echocardiography and other blood work ups were unremarkable. After completing investigations, the neonate was taken to the operation theater and explored. As the open bladder plate was being mobilized, it was noted that it had no connection with the ureters and also the urethras. Hence, it was excised. After excising the dry bladder plate, it was found that there was a complete bladder duplication on the sagittal plane. Each bladder was well formed and drain the ipsilateral kidney and was connected to the ipsilateral urethra. The presence of prostatic tissue and the number of corporal bodies in each phallus were not appreciated intra operatively since these structures were located deep in the pelvis. With these findings, no further urologic reconstruction was done.
The pubic symphysis was approximated with a suture without osteotomy. Abdominal wall was closed with mild tension after mobilizing the fascia on both sides. The neonate was immobilized with mummy wrap. He had uneventful post-operative course and was discharged on the 7th post-operative day. Biopsy confirmed that the excised tissue is a bladder. Subsequently, the patient was evaluated 3 months after surgery and he was noted to have smooth post-operative course with no complications.
Discussion
Bladder exstrophy is believed to occur earlier in gestation before the end of the 8th week of gestation as a result of inadequate migration of mesodermal cells in the caudal part of the abdomen. In addition, the timing of rupture of the cloacal membrane is believed to determine the extent of the lower abdominal defect and also the type of the anomaly in this spectrum of malformations. If rupture of the cloacal membrane happens prior to its fusion with the urorectal septum, cloacal exstrophy happens whereas if its rupture occurs after its fusion with this septum, classic bladder exstrophy results.5
As to the embryogenesis of exstrophy variants, due to the variability of the defects and the concomitant anomalies whose embryological origin cannot adequately be explained by the mechanisms mentioned above, further discovery is needed to fully understand the embryologic errors that result in the formation of these complex malformations.6
Exstrophy variants are characterized by atypical anatomical and physical findings than those found in patients with classic bladder exstrophy and epispadias malformation despite sharing the typical musculoskeletal defects of pubic separation and rectus diastasis. Marshal and his colloquies classified exstrophy variants into the following categories: superior vesical fissure, pseudo-exstrophy, duplicate exstrophy, superior vesical fistula.3 After their publication, other variants including covered exstrophy and inferior vesical fissure have been described revealing the complex nature of these malformations.4
Fewer than 30 cases of duplicate exstrophy have been reported so far.7 Benjamin and et al reported their experience on 25 patients with exstrophy variants at their center. They described two types of duplicate exstrophy: anterior- posterior and side by side duplication. Our patient had side by side duplication of the bladder.6 We did not find any report describing duplication of the bladder in the sagittal plane along with a third bladder with features of exstrophy making our case unique.
Bladder duplication and diphallia are also rare occurrences by themselves. Approximately 70 cases of bladder duplication have been reported till date while the reported incidence of diphallia is 1 per 5 to 6 million live births.8–12 Even though the association of bladder duplication with diphallia has been described in few case reports so far, the occurrence of both of these anomalies in concurrence with a third bladder with features of exstrophy makes our case exceptional.13–15
In our patient, since each duplicated bladder had its own ureters and urethra and the exstrophied bladder was dry, simple excision of the bladder plate and abdominal wall closure was done. This approach is favored as per the recommendations of Benjamin and et al.6 The surgical management of the diphallia was left to be done at a later age.
Regarding the future management plan of this infant, we do not expect major concerns on urinary continence as the bladder neck is located deep in the pelvis. In addition, it was noted that the neonate urinates in intervals and stays dry in between. Our plan is to follow his urinary voiding pattern and to send for Magnetic Resonance Urography to have a better characterization of the lower urinary tract and the genitalia. The specific surgical approach for the diphallia will be decided after doing imaging and characterizing the number and level of development of the corpora in each phallus. Either excision or reconstruction of the corporal tissue with or without urethral reconstruction will be done based on imaging findings.
In summary, our case presents a unique constellation of rare urologic malformations namely triplicated bladders with diphallia. This case is another good example showing the complex nature of exstrophy variants in the spectrum of bladder exstrophy and epispadias malformations.
Consent for Publication
Consent for publication was taken from parents of the neonate and can be accessed from the corresponding author upon request. Institutional approval was not required to publish the case details as no personal identifiers were included and there was no other issue requiring ethical clearance.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Nelson CP, Dunn RL, Wei JT. Contemporary epidemiology of bladder exstrophy in the United States. J Urol. 2005;173:1728e31. doi:10.1097/01.ju.0000154821.21521.9b
2. Valioulis I, Levard G, Lottmann H, Hameury F, Cendron J. A rare complex bladder exstrophy variant. BJU Int. 2000;86:398. doi:10.1046/j.1464-410X.2000.00729.x
3. Marshall VF, Muecke EC. Variations in exstrophy of the bladder. J Urol. 1962;88:766–796. doi:10.1016/S0022-5347(17)64883-3
4. Gupta DK, Charles AR, Srinivas M. Exstrophy variants: should they be considered malformation complexes separate from classic exstrophy. Eur J Pediat Surg. 2003;13:377–382.
5. Hall SA, Roni Manyevitch PK, Mistry WW, Gearhart JP. New insights on the basic science of bladder exstrophy-epispadias complex. Urology. 2021;147:256–263. doi:10.1016/j.urology.2020.10.004
6. Benjamin H, Lowentritt P, Van Zijl S, et al. Gearhart; variants of the exstrophy complex: a single institution experience. J Urol. 2005;173:1732–1737. doi:10.1097/01.ju.0000154353.03056.5c
7. Bouhafs A, Azzouzi DE, Halim Y, Arifi M, Belkacem R, Barahioui M. Duplicate bladder exstrophy: a unique variant. J Pediatric Urol. 2006;2:483–485. doi:10.1016/j.jpurol.2005.08.003
8. Delconta M, Guglielmettia LC, Rajbhandari N, Walker J, Wilcox D, Raphael N. Bladder duplication - A case series. Urology. 2021;149:199–205.
9. Coker AM, Allshouse MJ, Koyle MA. Complete duplication of bladder and urethra in a sagittal plane in a male infant: case report and literature review. J Pediatric Urol. 2008;4:255–259. doi:10.1016/j.jpurol.2008.02.001
10. Acimi S. Complete diphallia. Scand J Urol Nephrol. 2008;42:389–391. doi:10.1080/00365590701877507
11. Elsawy M, Salle JLP, Abdulsalam M, Alsaid AN. Penile duplication: is it necessary to excise one of the penises? J Pediatric Urol. 2012;8:434–436. doi:10.1016/j.jpurol.2011.09.006
12. Kendrick DJ, Kimble RM. Diphallia: literature review and proposed surgical classification system. ANZ J Surg. 2022;92:2053–2065. doi:10.1111/ans.17846
13. Khorramirouz R, Bagheri A, Kajbafzadeh A-M. Unusual variant of coronal bladder duplication associated with glans Diphallia: a case report and review of the literature. Case Reports Urol. 2015;4. doi:10.1155/2015/909102
14. Debra Dunn RG. Diphallia, double bladder, and two hemiscrotums: a case report. AORN J. 2019;109(6):729–740.
15. Rock SD, Gearhart JP. Complete lower urinary tract duplication with true diphallia presenting as a rare covered exstrophy variant. J Urol. 1997;167:1907–1908. doi:10.1016/S0022-5347(01)64899-7
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.