Back to Journals » International Medical Case Reports Journal » Volume 18
A Traumatic and Infected Left Ventricular Pseudoaneurysm 2 years After the Explantation of a Bridge-to-Recovery Left Ventricular Assist Device
Authors Aziz U ![]() , Strachinaru M
, Strachinaru M
Received 30 January 2025
Accepted for publication 28 June 2025
Published 10 July 2025 Volume 2025:18 Pages 883—886
DOI https://doi.org/10.2147/IMCRJ.S517668
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Vinay Kumar
Usama Aziz, Mihai Strachinaru
Cardiology Department – Erasme Hospital (Université Libre de Bruxelles), Brussels, Belgium
Correspondence: Usama Aziz, Cardiology Department, Erasme Hospital (Université Libre de Bruxelles), Route de Lennik 808, Brussels, Belgium, 1070, Email [email protected]
Abstract: Left ventricular assist devices (LVADs) have become an important modality of treatment in advanced heart failure, serving sometimes as a bridge to recovery. A subject in his 30s with alcohol-induced dilated cardiomyopathy underwent LVAD implantation following severe cardiac dysfunction. After six years, a sufficient myocardial recovery led to successful LVAD explantation. 2 years post-explant, the patient continued high-risk lifestyle behaviors (like smoking and drinking alcohol) and eventually developed a left thoracic pseudoaneurysm due to a fall with left chest trauma. Surgical repair revealed infection, treated with targeted antibiotics. This case shows a rare echocardiographic presentation and underscores the complexities of LVAD explantation, particularly in patients continuing high-risk lifestyle behaviors. To our knowledge, an infected left ventricular pseudoaneurysm complicating LVAD explantation has not previously been reported. Thus, its management and long-term outcomes could not be assessed using evidence-based guidelines.
Keywords: left ventricular assist device, explantation, complication, pseudoaneurysm
Case
A male patient in his 30s (Body-Mass index: 19.61) with alcohol-induced dilated cardiomyopathy and a history of heavy alcohol consumption and smoking underwent left ventricular assist device (LVAD) implantation after failing optimal medical therapy. Despite recommendations to cease alcohol and smoking, the patient continued both habits, albeit with drastic reduction in alcohol intake. Following 6 years of LVAD support, sufficient myocardial recovery was observed.
After medical-surgical consultation, LVAD explantation was proposed to the patient on condition that the patient permanently stops his alcohol and smoking habits. The patient agreed and the device was explanted successfully. Initial recovery post-explantation appeared promising despite a small ventricular septal defect (VSD) and apical akinesia. However, the patient stopped attending follow-up appointments and he was lost to care for extended periods.
Two years later, he presented with a pulsatile mass after a thoracic injury two weeks ago by falling and hitting the left side of his chest on the armrest of a chair. An echocardiography was done and the mass was diagnosed as a left ventricular pseudoaneurysm originating at the LVAD explantation site through a fistula in the myocardial scar (Figures 1 and 2). Surgical exploration revealed infection with Staphylococcus species, necessitating staged repair and prolonged antibiotic therapy. Despite challenges in care continuity and persistent high-risk lifestyle behaviors, the patient regained functional independence, albeit with a mid-range reduced left ventricular ejection fraction (LVEF) (Figure 3) and a persistent small VSD.
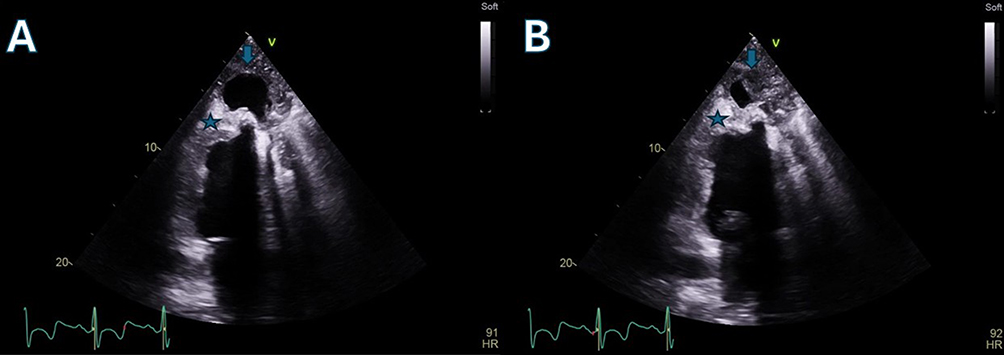 |
Figure 1 (A) end-systolic phase and (B) (end-diastolic phase) depict an apical two-chamber echocardiographic view showing the apical pseudoaneurysm (arrow). In the apical region of the left ventricle, the hyperechoic area (star) represents a rigid zone corresponding to the scar and patch following LVAD explantation. The pseudoaneurysm is pulsatile. The parietal pericardium is difficult to visualise and appears to be absent in the apical region. Consequently, the pseudoaneurysm is contained by adhesions to the fascia of the soft tissues of the thoracic wall. |
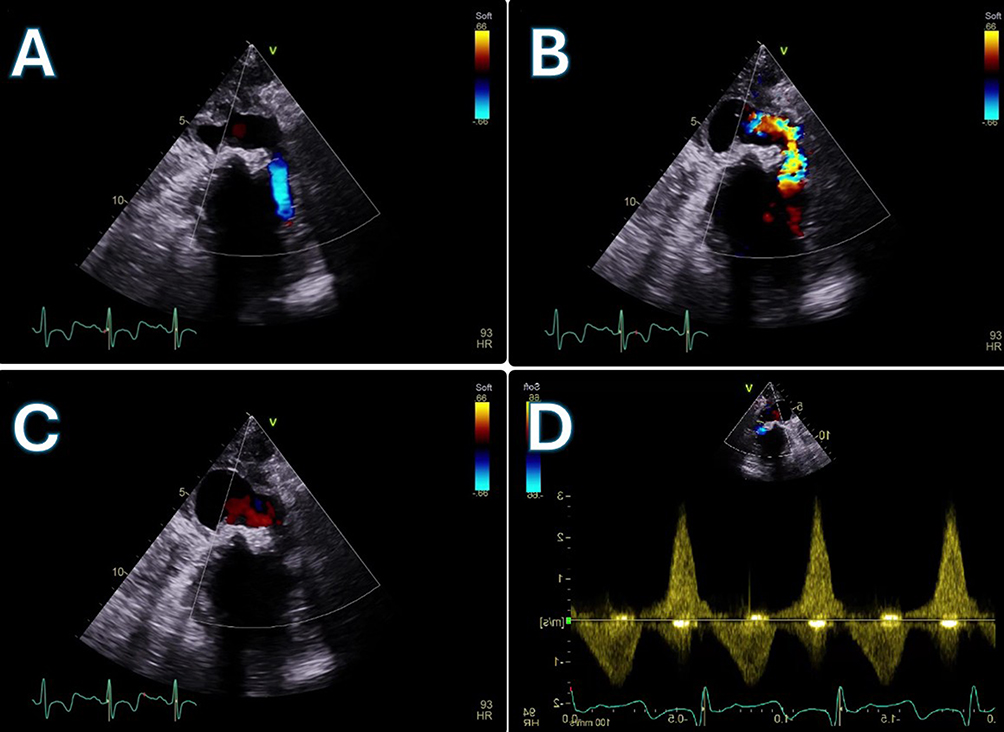 |
Figure 2 (A) end-diastolic, (B) (mid-systolic), and (C) (end-systolic) demonstrate blood flow using colour Doppler in a slightly modified three-chamber echocardiographic view. There is a continuity defect between the myocardium and the patch/scar at the anterolateral wall of the left ventricle, located at the junction of the middle and apical thirds. The pseudoaneurysm is supplied by this fistula and is contained by the soft tissues of the thoracic wall. The neck of the pseudoaneurysm is located at the level of the intercostal space. (D) shows both systolic and diastolic flow through the fistula. |
 |
Figure 3 (A) (end-diastolic and (B) end-systolic) shows the patient’s heart after surgical treatment of the pseudoaneurysm. |
Discussion
Management of advanced heart failure (HF) is particularly challenging. While patients with HF optimised with guideline‐directed medical therapy often demonstrate improved survival and reduced hospitalisation rates, approximately 5% of patients progress to develop advanced HF. Heart transplantation is an effective solution in such cases but is often not feasible due to the limited availability of donor organs.1,2
To address this gap, left ventricular assist devices (LVADs) have become a crucial modality in the treatment of end-stage HF, serving as a bridge to transplantation, bridge to candidacy, destination therapy, or even a bridge to recovery. It is estimated that in approximately 1–2% of cases, sufficient myocardial recovery occurs to allow for LVAD explantation.3 Other studies suggest that LVAD explantation occurs in even fewer cases, with estimates below 1%. For LVAD explantation to be feasible, myocardial recovery at the structural, molecular, and haemodynamic levels is necessary to ensure sustained recovery post‐LVAD.2
The mechanisms of myocardial recovery are complex and the subject of extensive study. It has been proposed that myocardial recovery can occur through LVAD therapy, which provides mechanical unloading of the left ventricle. Several mechanisms have been suggested, including restoration of the physiological structure of the extracellular matrix and protein changes, alongside histological evidence of decreased cellular hypertrophy and apoptosis.4
While not all cases of HF are reversible, patients with reversible causes of cardiomyopathy—such as tachycardia‐induced, peripartum, Takotsubo, alcohol-induced, and chemotherapy‐induced cardiomyopathy—may have a higher likelihood of sufficient improvement in cardiac function to allow for LVAD explantation.2
In our case study, the patient had alcohol-induced dilated cardiomyopathy and appeared to be a good candidate for LVAD explantation. Indeed, independent predictive factors for myocardial recovery have been established, including age <50 years, non-ischaemic cardiomyopathy, duration from cardiac diagnosis <2 years, absence of an implantable cardiac defibrillator, creatinine ≤1.2 mg/dL, and left ventricular end-diastolic diameter (LVEDD) <6.5 cm.2 Our patient met four of these six criteria.
Regarding outcomes following successful LVAD explantation, there are few studies, but those available reports encouraging survival rates ranging from 78.3% to 100%, albeit with varying rates of HF recurrence.3 Complications have been reported, including infection or thromboembolic events, often related to retained device material or the use of occlusive plugs. Other complications, such as HF recurrence and the need for LVAD reimplantation, have also been documented.2
To our knowledge, an infected left ventricular pseudoaneurysm complicating LVAD explantation has not previously been reported. Thus, there are no standardized treatment guidelines and its management and long-term outcomes could not be assessed using evidence-based guidelines. Some case reports have described apical left ventricular false aneurysms following transapical transcatheter aortic valve implantation5 or myocardial infarction.6
As left ventricular pseudoaneurysms are rare, knowledge of their natural history is limited. Left ventricular free wall rupture is a recognised complication of acute myocardial infarction, although previous cardiac surgery is a significant risk factor. Without surgical repair, affected patients have a high mortality rate, although isolated cases of prolonged survival in patients with left ventricular pseudoaneurysms have been reported.7
In conclusion, this case underscores the potential for myocardial recovery post-LVAD explantation while highlighting the risk of rare complications such as pseudoaneurysms. Given the lack of established management guidelines, further research is needed to determine optimal treatment strategies and long-term outcomes.
Abbreviations
HF, Heart failure; LVAD, Left ventricular assist device; LVEF, Left ventricular ejection fraction; OMT, Optimal medical therapy; VSD, Ventricular septal defect.
Patient Consent and Institution Approval
Patient provided written informed consent for his case details to be published. The cardiology imaging department of the Erasme Hospital (Université Libre de Bruxelles) has given its consent for the publication of the case.
Disclosure Statement
The authors report no conflicts of interest in this work.
Funding
There is no funding to report.
References
1. Al Hazzouri A, Attieh P, Sleiman C, Hamdan R, Ghadieh HE, Harbieh B. Left ventricular assist device in advanced refractory heart failure: a comprehensive review of patient selection, surgical approaches. Complications Future Perspectives Diagnostics. 14(22):2480.
2. Hamad EA, Byku M, Larson SB, Billia F. LVAD therapy as a catalyst to heart failure remission and myocardial recovery. Clin Cardiol. 2023;46(10):1154–1162. doi:10.1002/clc.24094
3. Antonides CFJ, Schoenrath F, Tmmh DB, et al. Outcomes of patients after successful left ventricular assist device explantation: a EUROMACS study. ESC Heart Fail. 2020;7(3):1085–1094. doi:10.1002/ehf2.12629
4. Chrysakis N, Xanthopoulos A, Magouliotis D, et al. Myocardial Recovery. Diagnostics. 13;8:1504.
5. Maillet JM, Sableyrolles JL, Guyon P, Bonnet N. Apical left ventricular false aneurysm after transapical transcatheter aortic valve implantation. Interact Cardiovasc Thorac Surg. 2014;18(1):137–138.
6. Csapo K, Voith L, Szuk T, Edes I, Kereiakes DJ.Postinfarction Left Ventricular Pseudoaneurysm Clin Cardiol. 1997;20(10):898–903.
7. Fok M, Bashir M, Hammoud I, et al. An apical left ventricular aneurysm rupture presenting as left breast mass 11 years after surgical repair. Ann R Coll Surg Engl. 2014;96(7):e6–7. doi:10.1308/003588414X13946184900561
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.