Back to Journals » International Journal of Women's Health » Volume 18
A Systematic Concept Analysis of Psychological Birth Trauma in Couples
Received 25 February 2026
Accepted for publication 6 May 2026
Published 20 May 2026 Volume 2026:18 598308
DOI https://doi.org/10.2147/IJWH.S598308
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Matteo Frigerio
Yang Shen,1 Ruolin Qiu,1,2 Qian Sun1
1School of Public Health and Nursing, Hangzhou Normal University, Zhejiang, Hangzhou, 310000, People’s Republic of China; 2Zhejiang Philosophy and Social Science Laboratory for Research in Early Development and Childcare, Hangzhou Normal University, Zhejiang, Hangzhou, 310000, People’s Republic of China
Correspondence: Ruolin Qiu, Email [email protected]
Aim: To explore the concepts and connotations of psychological birth trauma at the psychological level and to provide a reference for clinical practice.
Design: Concept analysis.
Data Sources: A systematic literature search on psychological birth trauma published between May 2021 and March 2024 in CNKI, VIP, Wanfang Database, Web of Science, PubMed, Embase, Scopus, CINAHL, PsycINFO.
Methods: Walker and Avant’s concept analysis method. The authors followed the PRISMA checklist.
Results: A total of 28 papers were included, summarizing the defining attributes of psychological birth trauma as the subjective feelings of the women and their partners, the appearance of avoidance behavior, throughout labor and until the postpartum period; the antecedents include self-factors, obstetric factors, medical related factors, and interpersonal factors; consequences include mental health, family relationships, and plans for another pregnancy.
Conclusion: This concept analysis provides a theoretical basis for subsequent in-depth research, demonstrating that birth and related events not only triggered psychological burdens for women but also caused negative emotional experiences for partners. By offering a more complete conceptualization, it helps healthcare personnel better identify psychological birth trauma in couples. Furthermore, psychological birth trauma is a multidimensional phenomenon that requires comprehensive strategies involving social support systems, mental health services, and medical systems to help couples cope with the trauma and promote their mental health and family harmony.
Keywords: psychological birth trauma, couple, concept analysis
Introduction
Birth is an important experience of a woman at the childbearing age, and the process is accompanied by dramatic physiological changes and complex psychological feelings.1 Birth is usually regarded as a pleasant event, while some women take it for a negative one.2 In recent years, the global fertility rate has declined,3 and especially in China, the fertility rate is relatively low in the global rankings. With full implementation of the three-child policy in 2021 throughout China, followed by the increasing proportion of high-risk pregnancies, the maternal physical and mental health issues are of great concern.4
Psychological birth trauma is one of the major problems faced by pregnant women, and studies have shown that at least 10% of all women experience trauma during childbirth.5 Research on the maternal mental health is gradually increasing in past years, focusing on women’s postnatal secondary mental health problems such as post-traumatic stress disorder (PTSD).5–8 There is a difference between psychological birth trauma and postpartum PTSD according to the statistics, in other words, the prevalence of psychological birth trauma ranges from 9% to 68.6% in different countries or regions,9–11 but only 1% to 6% of women who experience trauma develop postpartum PTSD.12 However, there is much more research literature on PTSD than psychological birth trauma. The concept of psychological birth trauma is often blurred, and the phenomenon of mixing with PTSD is common. However, a clear distinction between the two has important clinical and research implications. PTSD requires meeting specific diagnostic criteria. It involves exposure to a traumatic event involving actual or threatened death, serious injury, or sexual violence, along with the presence of a specific cluster of symptoms. These symptoms must persist for at least one month and cause significant impairment in social, occupational, or other important areas of functioning.13 Psychological birth trauma is more associated with negative experiences during childbirth, such as extreme reactions to pain, feelings of loss of control, and dissatisfaction with medical interventions.11,12 These situations, while not necessarily meeting the diagnostic criteria for PTSD, can still have a profound impact on physical and mental health.
PTSD is a long-term psychological disorder caused by individuals who experience, witness, or learn of life-threatening, physical integrity, or major shock events.6 Compared to PTSD that may emphasize personal influences, the impact of psychological birth trauma is multifaceted. Beck et al14 used the term “ripple effect” to describe the impact, emphasizing that psychological birth trauma not only affects the mother herself, but also spreads like ripples on the water surface. The psychological birth trauma gradually could separate and influence the mother–child relationship, the relationship between the husband and the wife, the harmony of the family, and the wider society.
After initial searching, it was showed that studies related to psychological birth trauma were mainly focused on exploring its causes and effects, and most of the research types were qualitative, and there was scarce literature discussing the concept of psychological birth trauma.15 Moreover, the existed concept focused on women’s all respects but ignored the psychological experience of men in traumatic childbirth experiences. However, childbirth is an event that occurs in the family and is a process that couples experience together. Researches have shown that men’s exposure to traumatic childbirth experiences can result in fear,16–20 guilt,16,20 feelings of helplessness20–22 and feeling marginalized by healthcare personnel,16–18,21 and that some men even perceive the experience as causing ongoing pain.23 A study looking at the impact of traumatic birth experiences on men found that17 males wanted the same counseling support as females after a traumatic birth experience. This suggests that men’s traumatic experiences and needs during birth should also be noticed. Thus, a couple-based perspective is necessary to fully understand and address psychological birth trauma.
At present, academic experts have not yet reached a consensus on the concept of psychological birth trauma, and the ambiguity of the concept is likely to cause cognitive bias and hinder the development of clinical care and academic research. Therefore, this study aims to adopt concept analysis method24 to comprehensively analyze the concept of psychological birth trauma, as well as clarify its attributes and causal relationships, to provide a reference for the development of appropriate measurement tools and intervention studies on psychological birth trauma in the future.
Data Sources
Search Strategy
A comprehensive and systematic search was conducted for databases such as CNKI, VIP, Wanfang Database, Web of Science, PubMed, Embase, Scopus, CINAHL, PsycINFO, with a retrieval timeframe from May 2021 to March 2024. The search terms are shown in Table 1. The search strategy built is described in Table 2 Search strategy. Inclusion criteria: 1) articles in English or Chinese; 2) Women with vaginal birth; 3) psychological birth trauma of the women or spouses during/after labor; 4) research or review articles. Exclusion criteria: 1) only exploring physiological trauma; 2) only describing the relevant scales; 3) only exploring the trauma of healthcare workers; 4) animal experiments; 5) full text not available.
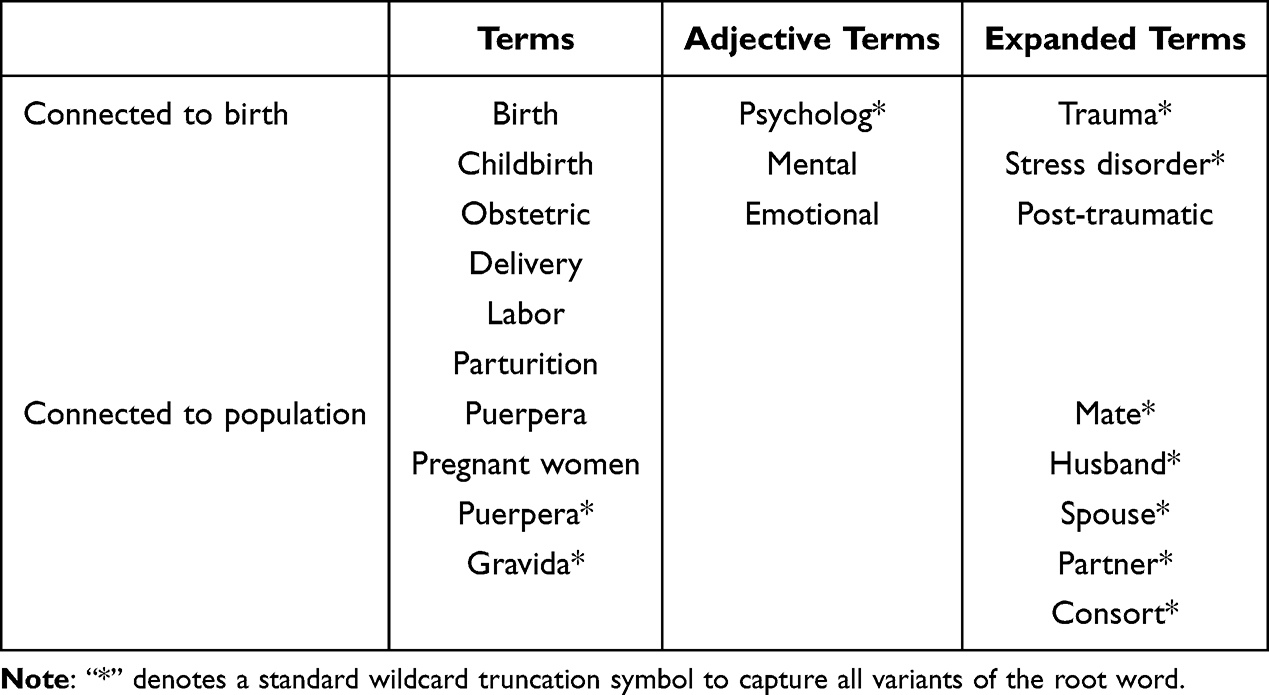 |
Table 1 Search Terms |
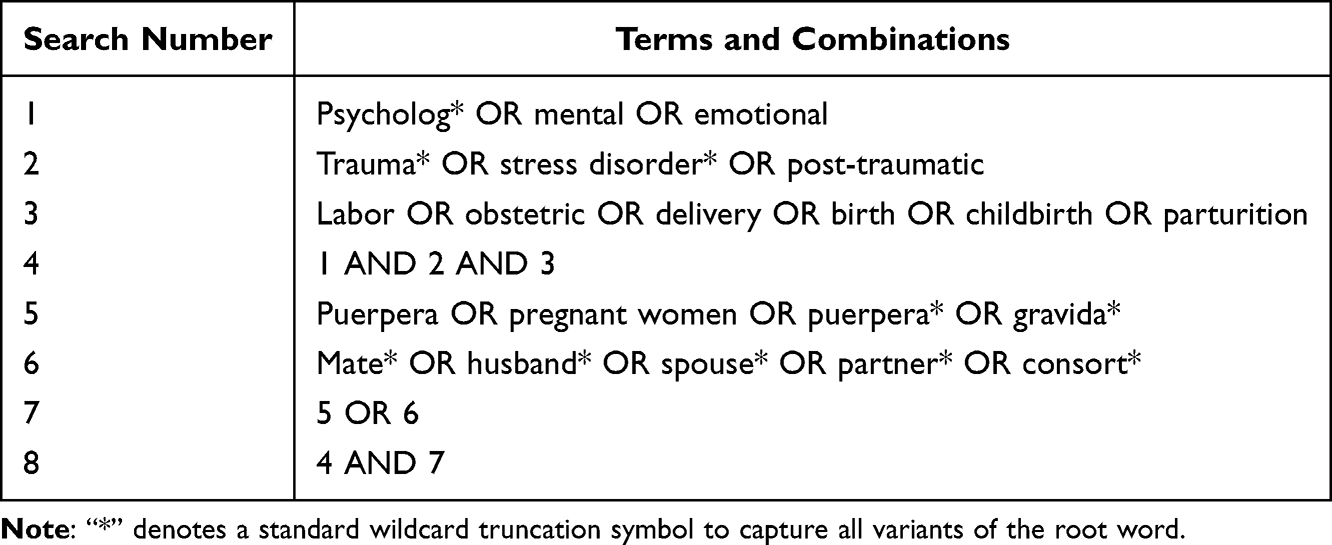 |
Table 2 Search Strategy |
Literature Extraction
All the primary selected literature was imported into Endnote 20.0 to de-duplicate. This process was conducted and cross-checked the databases by two independent researchers, respectively, based on present criteria for two rounds. First, the researcher would look through the titles and abstracts to remove ineligible articles, and afterward a more in-depth screening was carried out by reading the full text of the remained literature. When there was disagreement, both parties discussed together or a third expert researcher assisted to reach a consensus.
Figure 1 shows detailed process of literature search and screening. The initial search yielded 4119 papers. After removing 1489 duplicates, the titles and abstracts of the rest of the papers were reviewed, of which 48 articles remained in the second round of screening. Finally, 28 literatures were successfully included, containing 12 qualitative studies,16,18,19,21–23,25–30 4 quantitative studies,9–11,11,31 4 Meta synthesis,4,17,20,32 2 systematic reviews,33,34 2 mixed studies,35 2 concept analyses,15,36 1 scoping review,37 1 narrative review,38 and 1 discussion article.39 From the perspective of geographical distribution, the existing literature covers many countries and regions, including 8 from China,4,10,15,20,31,32,36,38 7 studies from the United Kingdom,18,23,25,28–30,34 5 from Australia,16,19,212237,40 3 from Turkey,9,11,26 and 1 each from Singapore,17 Sweden,35 South Korea,27 France33 and Germany.39
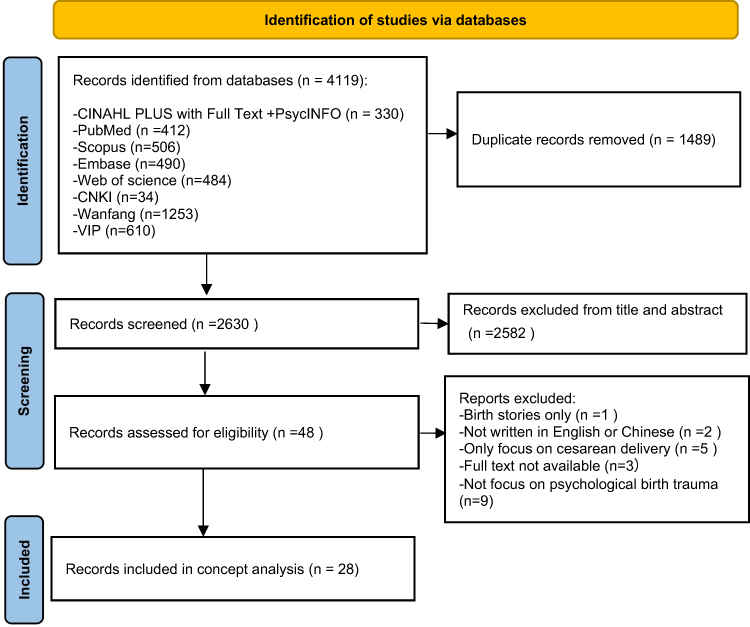 |
Figure 1 Flowchart of literature search and screening. |
Methodology
This study was analyzed following the steps of Walker and Avant’s classical concept analysis.24 It was derived from Wilson’s concept analysis theory41 to help researchers systematically clarify and precisely define vague concepts, so as to promote theoretical development. The method involves selecting a concept, clarifying the purpose of the analysis, identifying its application in the literature, determining the defining characteristics, constructing a case, analyzing its antecedents and consequences, as well as describing the measures available. Table 3 contents based on Walker and Avant’s classical concept analysis is the research procedures and content based on Walker and Avant’s classic concept analysis. Throughout the study, the authors followed the PRISMA checklist.
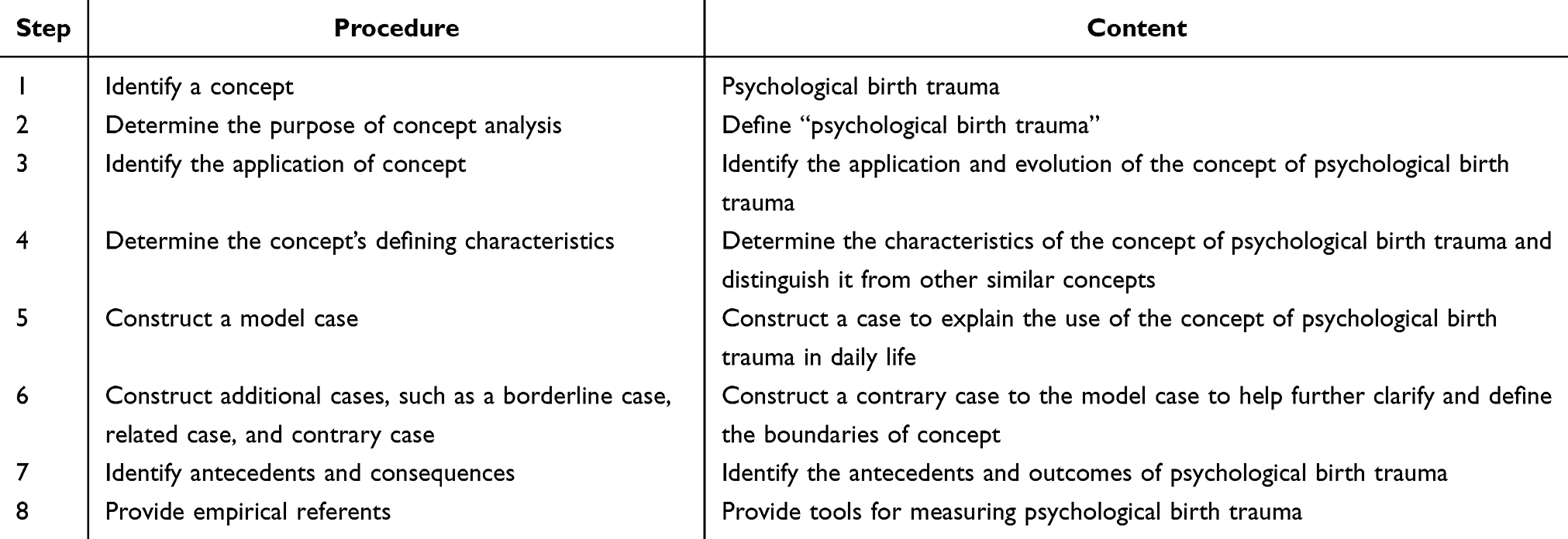 |
Table 3 Content Based on Walker and Avant’s Classical Concept Analysis |
Overview of the Concept
This study defined psychological birth trauma as a long-term state experienced by both spouses throughout labor and the postpartum period, marked by negative emotions and avoidance behaviors, significantly affecting both partners. Figure 2 provides a model diagram of antecedents, attributes, and consequences for psychological birth trauma.
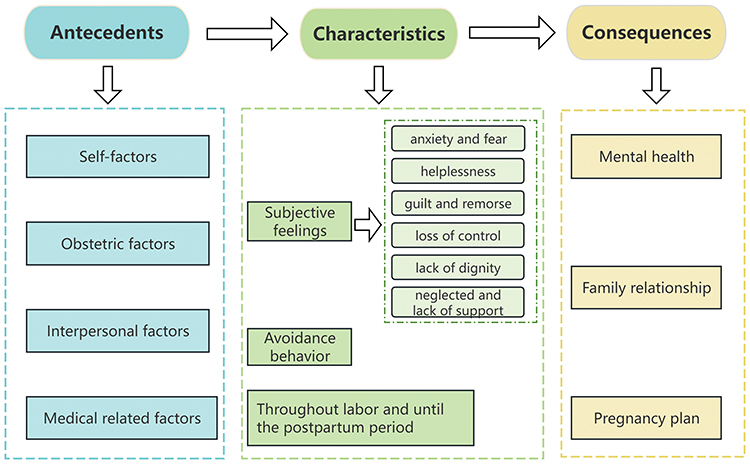 |
Figure 2 Psychological birth trauma: antecedents, characteristics and consequences. |
Use of Concept
The original definition of psychological birth trauma was only limited to physical injuries suffered by the mother or baby during labor, such as lacerations, organ damage, and so on.42 Over time, researchers have realized that psychological birth trauma should also extend to the psychological and emotional aspects.43 Professor Beck was the first one to highlight the psychological experience of psychological birth trauma. He defined it as an event during pending labor and childbirth that involves the risk of serious injuries/death to the mother or baby, resulting in women’s intense feelings of fear, helplessness, and loss of control. Subsequently, in 2015, Beck proposed that birth trauma has 5 attributes:14 deprived of caring, stripped of dignity, terrifying loss of control, neglected communication, and forgotten. Wang Hui36 et al conducted a concept analysis of birth trauma and provided an operational definition: physiological, behavioral, and psychological trauma that occurs after a woman experiences the absence of social support, loss of control, deprivation of dignity, and an inability to interact well with healthcare personnel during childbirth. In a recent concept analysis, Sun15 et al specifically stated that psychological birth trauma was a woman’s subjective feelings caused by events directly or indirectly related to labor, manifested as intertwined emotional experiences originating from the birthing process and continuing into the postpartum period. It has a wide range of negative and, in some cases, positive effects on women. However, the above definitions ignore the traumatic experience of men in childbirth. Men also experience emotional and psychological distress when they play a key support role in birth. This kind of trauma can lead to challenges in dealing with issues such as their partner’s emotions and family conflict. Therefore, adopting “men’s trauma” in the discussion is likely to deepen a comprehensive understanding of the psychological birth trauma for professionals.
Defining Properties
Defining attributes refers to defining characteristics that are unique to a concept and thus distinguish it clearly from other similar concepts.24 This review and analysis of the literature concluded that the following 3 attribute characteristics of psychological birth trauma: (1) the subjective feelings of the women and her partner: mainly in the form of negative emotional experiences; (2) the occurrence of avoidance behaviors; and (3) the fact that it continues throughout labor and until the postpartum period.
Subjective Feelings of Women and Their Partners
Anxiety and Fear
The unfamiliar and confined environment of the ward, the stressful work of the medical staff, the pain of childbirth, and the unpredictability of the birth process9,25–27,32,35,38 can all lead to anxiety and fear for their lives and the health and safety of their babies.
Meanwhile, unpreparedness to witness the physical injuries of their partner during labor, uncertainty about whether the unknown events of labor will affect the safety of the mother and child, and poor communication of information with healthcare personnel cause anxiety and fear in men.16–20 In addition, men take on many responsibilities after birth, such as nurturing the baby and balancing family and work. Those can exacerbate the original anxiety.18,23
Besides, postpartum feeding difficulties and differences in parenting concepts can also lead to anxiety in both couples.21,25,32
Helplessness
Women can feel overwhelmed in the face of intense labor pain and possible birth complications.18 Limited communication with medical staff, coupled with a lack of child-bearing knowledge and companionship, is able to aggravate these feelings.18,25,32,38 Together, these physical and psychological challenges contribute to a strong sense of isolation and helplessness.
Similarly, men may feel helpless due to their unpreparedness for emergencies during their partner’s labor and their inability to accompany their partner during labor.18,20,23 In addition, emotional estrangement between postpartum partners, the oppression of the family atmosphere and the absence of people to tell their emotions aggravate men’s sense of helplessness.21
Guilt and Remorse
Insufficient knowledge about birth or a terrible birth experience in the past can make a woman question whether she will have an easy birth.27 When there is a separation of mother and baby due to asphyxia or health problems, women may think that the “abnormal” birth was due to their faults.18,25,29 This triggers feelings of guilt and self-blame.
Considering negligence or lack of experience, men are not able to recognize and meet the physical or emotional needs from their partners who are suffering labor pains.16,18,23 Men question their roles either husbands or fathers, believing that they are both incompetent to protect their wives and children when special circumstances arise during labor.21 The combination of these factors leads to feelings of guilt and self-blame during childbirth.
Loss of Control
Women feel that their expectations during labor do not match the reality and that it is difficult for them to participate in the decision-making process, including deciding on the mode of delivery and the use of analgesia.17,18,27,29,33,37 In some specific cases, healthcare professionals just ask women are required to sign consent forms quickly without explaining any reasons for these practices and the risks involved.4,9,18,36 As women’s decision-making power and control diminish, they feel labor is in the hands of the midwife.4 This adds to women’s distress.
Men can lose control over the events that occur during their partner’s labor owing to absenting interaction with healthcare professionals and the shortage of involvement in decision-making.16,17
Lack of Dignity
Women perceive frequent and unexplained internal vaginal examinations as a violation of their bodies and a neglect of their privacy, and the indifferent language and attitude of the midwife can lead to feelings of being undervalued, or even depersonalized, or even to women believing that they have become the trainee’s “teaching aids”.4,17,19,32 All of these result in losing women’s dignity.
Neglected and Lack of Support
During labor, women feel that healthcare professionals are more concerned with medical techniques, routine procedures, and objective delivery criteria, and do not provide them enough information and emotional support.4,10,32,36 After the birth, it is a common phenomenon that the baby is the center of the world and women are always treated as a speechless birthing tool;25 even in the postpartum period, women feel that they do not receive practical support from their partners or family (childcare, financial support, etc).17,29,31,34,37 In addition, birth is often supposed to be a female affair, which undervalues men’s participation and makes them be observers. They are more possible to express negative emotions difficultly and feel neglected.16,21 When women-only postnatal counseling is offered, men feel marginalized and wish they could be equally supported.17,18
Avoidance Behaviors
Avoidance behavior refers to the coping strategies adopted by individuals in the face of situations that cause emotional pain, anxiety or fear, in order to reduce the experience of negative emotions.44 It widely exists in a variety of people who get psychological disorders.
After a traumatic birth, couples may experience avoidance behavior, which stems mainly from the fear of going through a similar painful or upsetting situation again. Except for the avoidance of discussing the birth experience, these behaviors may also extend to sexual difficulties and hesitancy to plan future births.17–19,22,23,32 Trauma may lead to an altered perception of a woman’s body, which in turn brings resistance or discomfort with sexual intimacy.4 Moreover, some women no longer wanted to participate in social activities related to parenting or postpartum recovery.17,37 Additionally, men are prone to become overly cautious or even alienated for fear of exacerbating their partner’s psychological or physical pain,20,23 which may adversely affect women’s self-perception and couples’ physical contact in a way.
Throughout Labor and Until the Postpartum Period
Birth is a complex physiological event, accompanied by both physical and psychological challenges,1 the trauma of which may persist and have a long impact on couples. Whereas, the trauma duration is difficult to determine, it usually lasts from 1 to 18 months,9,11,23 in severe cases, probably up to 3 years.23
Life-threatening events that may occur during labor, especially emergency obstetric interventions, can aggravate a woman’s feelings of trauma.33,39 Inadequate communication or lack of personalized care from healthcare professionals increases the risk of negative feelings, such as being treated like a “pet”.33,37,39 After women giving birth, some unpleasant episodic memories during labor may be repeatedly flash back, which may lead to symptoms of post-traumatic stress disorder (PTSD).4,36,37
Similarly, as partners or fathers-to-be, men who have witnessed the whole process of labor may feel fearful, helpless and guilty, especially when their spouse experiences emergency.16,20 This emotional impact is particularly strong when they were not adequately prepared for it, resulting in their significant psychological stress.17,21 If men were not provided the same emotional support as women received, or were ashamed to seek professional help during postpartum, their stress may be cumulative. Combined with the constant stress of juggling work and caring for the wife and child, the trauma is compounded and overloaded.21,23
However, a small number of couples said that from a long-term perspective, the psychological birth trauma made it more appreciated for each other to company, thus bringing them closer.23 Unfortunately, the exact length of time is not certain.
Constructing a Typical Case
The construction of typical cases has a positive effect on the in-depth understanding of the analyzed concepts and helps to grasp more accurately their content and points. And this case should encompass the full range of defining attributes.24 The construction of this typical case drew on a qualitative study.17
Mrs. W experienced contractions at 39+3 weeks of pregnancy. Mrs. W and her husband were very nervous and quickly went to the hospital for checkups and were admitted for delivery (anxiety and fear). She was wheeled into the waiting room and her husband was asked to wait outside (neglected) and was not allowed to accompany the labor (helplessness). Mrs. W was left alone with the midwives (neglected) and the cries of pain from the other mothers around her (fear). As the labor progressed, Mrs. W cried out in pain but received no response from the midwives (neglected, helplessness and anxiety). Mrs. W lost confidence in having a normal labor and desired to have a cesarean section, which was refused by her family and the midwife (loss of control). While awaiting labor, a male doctor and his trainee performed multiple vaginal examinations without adequate explanation (loss of dignity). When the newborn suffered mild asphyxia, the midwife and doctor began emergency treatment, Mrs. W felt powerless (guilt, self-blame, helplessness). Outside the labor ward, her husband could only wait anxiously, fearing for the safety of his wife and child (guilt, self-blame and fear). Eventually, Mrs. W and the child returned to the ward without incident, with the family all around the child, but no one asked Mrs. W how she was feeling (neglected and lack of support). After discharged from the hospital, Mrs. W recalled the painful childbirth experience, and therefore was reluctant to contact with her child and refused to breastfeed (avoidance behavior). The husband was in constant pain from not being able to be with the birth and from witnessing his wife’s postnatal trauma. Both parties avoided intimate physical contact for a long time afterward (avoidance behavior), and sometimes even woke up with nightmares of the childbirth (continuing into the postpartum period). When Ms. W became pregnant again, the painful experience of birth in the past would make her and her husband hesitate and even seek counseling (continuing into the postpartum period).
Constructing the Opposite Case
Contrary cases are those do not include any of the defined properties and are the exact opposites of the defined properties.24
At 39+1 weeks of pregnancy, Mrs. L started to feel pain in her abdomen and noticed a small amount of vaginal bleeding. She and her husband, both of whom had attended women school classes, quickly contacted the doctor and went to the hospital as instructed (sense of control). Upon arrival at the hospital, Ms. L was carefully examined by her doctor. After meticulous conversation, she was admitted to the hospital to await delivery, while her husband was allowed to accompany (gaining support). Upon entering the waiting room, Mrs. L’s husband accompanied her at all times (sense of involvement), and the midwife kept a constant eye on her, providing timely help and comfort (gaining support). As the labor progressed, Mrs. L was frightened by the pain and her husband’s company encouraged her (reducing anxiety and fear). She was taught how to breathe to ease the pain by her midwife (sense of control), which provided Mrs. L confidence to proceed with normal labor (sense of control). Mrs. L felt comfortable and respected, because the midwife fully explained the reasons and gained her permissions before each vaginal examination (maintaining dignity). After the baby was successfully born, Mrs. L felt her first close contact with the baby. Her husband stayed with her to share the moment (reducing guilt and self-blame). Back in the ward, Ms. L received concerns from her family and was well taken care of by her mother-in-law and husband (gaining support). On discharge from the hospital, both Mrs. L and her husband were happy with the birth experience and Mrs. L was willing to cuddle and feed her baby (positive response). The relationship between the couple was closer as a result of this positive experience, making deeper trust and understanding (no avoidance behavior). When they became pregnant again, Mrs. L and her husband were excited and looking forward to the baby (persistent effect).
Antecedents and Consequences of Psychological Birth Trauma
Antecedents
Antecedents are necessary conditions that precede or lead to the occurrence of concepts.24 Our study concluded that the antecedents of psychological birth trauma in couples include self-factors, obstetric factors, medical related factors, and interpersonal factors.
Self-factors (demographic characteristics, past history, and personality traits) were considered to have strong relationship with psychological birth trauma. Studies have shown that low income,11 low education,10,35 inadequate knowledge of labor and delivery,10,38 and first-time mothers9,33 are more likely to experience trauma; mothers that have a history of trauma,19,22,33 unplanned pregnancies,11 fear of labor26,35 and those whose expectations of labor are different from what they actually experience also have a higher risk16,17,20,29,37 of psychological birth trauma. In addition, the participation of couples’ prenatal training courses11,33 can reduce the level of psychological birth trauma.
Obstetric factors include intense labor pains, obstructed labor, vaginal assisted labor techniques, prolonged labor, and complications such as emergency cesarean section and fetal distress.10,11,15,16,20,31,33,37,38 These factors not only increase the psychological burden on women but also cause fear, and guilt in men. Parent–child separation due to preterm birth or neonatal health problems can lead to feelings of guilt, and helplessness for couples.18,21,25,29
The medical related factors involve both the environment in which the birth takes place and the medical staff. The unfamiliar and closed environment and the sound of medical equipment may cause fear and helplessness in women, while at the same time triggering worry and self-blame in men. Indifferent attitudes, insufficient information support, inadequate provision of emotional support, and a stressful working atmosphere4,9,16–20,36 among healthcare workers may all contribute to couples experiencing psychological birth trauma.
Interpersonal relationship factors are mainly family, friends and work relationships. Husbands return to work and relatives pay more attention to the baby after childbirth, which makes women feel neglected and unsupported.15,17,31,34,37 Some women say that it is difficult to integrate themselves into friends’ activities due to childcare and other reasons, which leads to alienation of friends.36,37 Men also often feel traumatized by the fact that postnatal counseling services are mainly for women and that they do not receive enough attention.17,18,23 This can lead to psychological birth trauma.
Consequences
Consequences are those that occur after or as a result of the concepts.24 The consequences of psychological birth trauma included both positive and negative aspects. Negative outcomes were predominant, covering mental health, family relationships, and planning for a another pregnancy.
First, psychological birth trauma can have a direct impact on the mental health of the couple. Not only does it cause psychological distress for the couple at the time, it can even lead them to long-term anxiety and depression.17,21,23 They may frequently recall the painful experience of childbirth later in life17 and excessive worry about the baby’s health.30 As a result, they may develop strong emotions such as fear, anger, and sadness. In serious cases, they may suffer from postnatal depression, post-traumatic stress disorder, and other problems.9,21,34
Second, it can cause changes in family relationships, including parent-child and husband–wife relationships. Women may lack affection for their infants, leading to estrangement of the mother–infant relationship and negative patterns of interaction.15,19,27,30 However, some men feel that this motivates them to become more involved in caring for their babies.20 In addition, psychological birth trauma can also damage the couple’s relationship, negative traumatic experiences can lead to reduced communication between couples, avoidance of sex, emotional disconnection, and even divorce.4,15–19
Third, the psychological birth trauma can affect couple’s plans for another pregnancy. Pain, complications, or poor outcomes during labor can make women fearful of giving birth and thus refuse to get pregnant again.4,15 Similarly, research has shown that men who experience psychological birth trauma may become anxious about having children or even avoid pregnancy.20
While negative outcomes of psychological birth trauma are predominant in the literature, there are also studies describing positive impacts. Research had confirmed that some women draw on different internal and external resources to heal themselves, promoting recovery from trauma while strengthening their own beliefs.15,25,29 In addition, one study suggested that men understood their spouses better after experiencing psychological trauma and that they developed a closer relationship with them, as well as an increased sense of empathy.23
Empirical Measures of Psychological Birth Trauma
Empirical indicators are instruments that measure how and to what extent the described concept exists in practice, contribute to a better understanding of the concept’s defining attributes. The scales used to measure psychological birth trauma in childbirth are relatively few and their reliability has only been validated in local populations, and they have not been widely used in other countries.
The Scale of Traumatic Childbirth Perception (STCP) is a self-report scale developed by Yalniz40 to collect information about physical, emotional, and mental trauma associated with childbirth, and is mainly used to assess the level of maternal perception of birth trauma. The scale contains 13 items, each of which is rated from 0 to 10, with a total score from 0 to 130. Higher scores indicate higher levels of perceived labor trauma, namely, 0 to 26 is grouped into a very low level, 27 to 52 is grouped into a low level, 53 to 78 explains a moderate level, 79 to 104 is a high level, and 105 to 130 represents a very high level. The Cronbach’s alpha coefficient of the scale was 0.895, and the reliability and validity of the scale were good among Turkish pregnant women.
The City Birth Trauma Scale City (BiTS) was developed by Ayers.45 The scale consists of 29 questions in 2 dimensions: general symptoms and symptoms related to childbirth. The scoring system of the scale is whether or not the traumatic event was experienced, the frequency of related symptoms, whether or not it was accompanied by dissociative symptoms, the time of symptom onset, symptom duration, and whether or not there was pain and social dysfunction and whether the symptoms were related to medication, with a total score of 0 to 60 points, and the higher the score is, the severer the maternal labor trauma is. The reliability and validity of the scale was good, with an overall Cronbach’s alpha coefficient of 0.925.
A questionnaire on Psychological Birth Trauma (QPBT) was developed by Taghizadeh46 to assess the level of psychological birth trauma in labor. The questionnaire covers 5 dimensions of anxiety and pain in labor, psychological performance, feelings of helplessness, feelings of collapse and death, and somatic performance with a total of 30 items. The scale is based on a Likert 5-point scale with a total score of 30 to 150, with higher scores indicating higher levels of psychological birth trauma. The reliability and validity of the questionnaire was good among Iranian mothers with a Cronbach’s alpha coefficient of 0.949.
It is worth noting that all three of the above scales were measured among women, whereas assessments regarding male psychological birth trauma are usually conducted by using qualitative research methods.
Discussion
The results of this concept analysis indicate that the concept of psychological birth trauma has undergone a dynamic process of evolution. This process extended beyond the concept of trauma at the physiological level to the psychological level. Compared with the previous analysis of the psychological birth trauma limited to women,15 this study innovatively included the psychological trauma of male partners into the scope of discussion. Traditionally, researches on the psychological birth trauma have focused on the mother, ignoring the emotional and psychological stress that partners. However, there is growing evidence that men also experience strong emotional reactions when witnessing their wives go through labor or face a medical emergency.16,18,20,21,23 Therefore, this study breaks through the traditional framework and aims to more fully understand the impact of psychological birth trauma and calls for more attention and support for the mental health of men.
Analyzing the consequences of previous studies, it has been found that psychological birth trauma could make a profound impact on the mental health of the couple, on family relationships, and on the planning of another pregnancy, and psychological birth trauma might even lead to the development of postnatal post-traumatic stress disorder (PTSD) and other disorders without intervention. Therefore, identifying the antecedents of psychological birth trauma, including self-factors, obstetric factors, medical related factors, and interpersonal factors can be preventive.15,36 This suggested that healthcare professionals should consider the variability of their own factors, such as literacy, age, and income in future medical planning. At the same time, healthcare professionals should strengthen communication with couples and provide them with adequate information support and emotional support. In addition, unnecessary obstetric interventions should be avoided as much as possible and a comfortable birthing environment should be provided. However, future more in-depth studies should be conducted to assess the antecedents of birth trauma, so as to form high-quality evidence.
While this concept analysis endeavors to provide a comprehensive understanding of psychological birth trauma, certain limitations must be acknowledged. On the one hand, literature consisted of studies conducted after the introduction of the three-child policy in 2021, which, while more representative of the recent state of research on psychological birth trauma, also limited the sources of available data to a certain extent. On the other hand, most of the studies included in the current study were qualitative, with insufficient quantitative evidence.
Conclusion
Through Walker and Avant’s classical concept analysis,24 the antecedents, attributes, and consequences were elaborated to reduce the ambiguity of the concept of psychological birth trauma. This expansion from the traditional female-only research perspective has certain clinical importance. Partners’ psychological birth trauma experiences can not only affect their own long-term mental well-being but also exert bidirectional impacts on their partners’ perinatal emotional state and the overall health of the family unit. This also helps researchers to better understand the connotation of psychological birth trauma, explore the issue of psychological birth trauma in couples in various aspects, and provide a theoretical basis for solving the problem of clinical psychological birth trauma. In turn, this can improve mental health outcomes for both birthing women and their partners, support the development of tools to assess partners’ psychological birth trauma, and ultimately advance the discipline.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agreed to be accountable for all aspects of the work.
Disclosure
All authors declare no conflicts of interest in this work.
References
1. Wigert H, Nilsson C, Dencker A, et al. Women’s experiences of fear of childbirth: a metasynthesis of qualitative studies. Int Journal Qual Stud Health Well-Being. 2020;15(1):1704484. doi:10.1080/17482631.2019.1704484
2. Jouhki MR, Suominen T, Åstedt-Kurki P. Giving birth on our own terms-women’s experience of childbirth at home. Midwifery. 2017;53:35–12. doi:10.1016/j.midw.2017.07.008
3. The World Bank Group. Fertility rate, total (births per woman); 2022. Available from: https://data.worldbank.org/indicator/SP.DYN.TFRT.IN.
4. Liu J, Qiao JH, Zhou SJ, et al. Meta synthesis of qualitative research on women’s real experience of birth trauma. Chin J Modern Nurs. 2022;28:2–8. doi:10.3760/cma.j.cn115682-20210813-03598
5. Hosseini Tabaghdehi M, Kolahdozan S, Keramat A, Shahhossein Z, Moosazadeh M, Motaghi Z. Prevalence and factors affecting the negative childbirth experiences: a systematic review. Journal Maternal-Fetal Neonatal Med. 2020;33(22):3849–3856. doi:10.1080/14767058.2019.1583740
6. Garthus-Niegel S, Horsch A, von Soest T, et al. Posttraumatic stress symptoms following childbirth: associations with prenatal attachment in subsequent pregnancies. Arch Women’s Mental Health. 2020;23(4):547–555. doi:10.1007/s00737-019-01011-0
7. Abdollahpour S, Khosravi A, Motaghi Z, Keramat A, Mousavi SA. Effect of brief cognitive behavioral counseling and debriefing on the prevention of post-traumatic stress disorder in traumatic birth: a randomized clinical trial. Commu Mental Health J. 2019;55(7):1173–1178. doi:10.1007/s10597-019-00424-6
8. Asadzadeh L, Jafari E, Kharaghani R, Taremian F. Effectiveness of midwife-led brief counseling intervention on post-traumatic stress disorder, depression, and anxiety symptoms of women experiencing a traumatic childbirth: a randomized controlled trial. BMC Pregnancy Childbirth. 2020;20(1):142. doi:10.1186/s12884-020-2826-1
9. Türkmen H, Yalniz Dilcen H, Özçoban FA. Traumatic childbirth perception during pregnancy and the postpartum period and its postnatal mental health outcomes: a prospective longitudinal study. J Reprod Infant Psychol. 2021;39(4):422–434. doi:10.1080/02646838.2020.1792429
10. Chen Y, Ismail F, Xiong Z, et al. Association between perceived birth trauma and postpartum depression: a prospective cohort study in China. Int J Gynaecol Obstet. 2022;157(3):598–603. doi:10.1002/ijgo.13845
11. Bay F, Sayiner FD. Perception of traumatic childbirth of women and its relationship with postpartum depression. Women Health. 2021;61(5):479–489. doi:10.1080/03630242.2021.1927287
12. Stankovic B. Women’s experiences of childbirth in Serbian Public Healthcare Institutions: a qualitative study. Int J Behav Med. 2017;24(6):803–814. doi:10.1007/s12529-017-9672-1
13. First MB, Gaebel W, Maj M, et al. An organization- and category-level comparison of diagnostic requirements for mental disorders in ICD-11 and DSM-5. World Psychiatry. 2021;20(1):34–51. doi:10.1002/wps.20825
14. Beck CT. Middle range theory of traumatic childbirth: the ever-widening ripple effect. Global Qual Nurs Res. 2015;2:2333393615575313. doi:10.1177/2333393615575313
15. Sun X, Fan X, Cong S, et al. Psychological birth trauma: a concept analysis. Front Psychol. 2023;13:1065612. doi:10.3389/fpsyg.2022.1065612
16. Kothari A, Bruxner G, Callaway L, Dulhunty JM. “It’s a lot of pain you’ve got to hide”: a qualitative study of the journey of fathers facing traumatic pregnancy and childbirth. BMC Pregnancy Childbirth. 2022;22(1):434. doi:10.1186/s12884-022-04738-4
17. Shorey S, Wong PZE. Traumatic childbirth experiences of new parents: a meta-synthesis. Trauma Violence Abuse. 2022;23(3):748–763. doi:10.1177/1524838020977161
18. Butterworth S, Butterworth R, Law GU. Birth trauma: the elephant in the nursery. J Reprod Infant Psychol. 2023;1–22. doi:10.1080/02646838.2023.2264877
19. Gregory EM, Maddern R. The psychosocial experience of traumatic birth in couples: an interpretative phenomenological study. J Reprod Infant Psychol. 2023;1–15. doi:10.1080/02646838.2023.2225073
20. Guo YY, Zeng GH, Ren YL, Feng GF. Meta synthesis of qualitative research on male participation in traumatic childbirth experience. Chin J Pract Nurs. 2023;15:1188–1194. doi:10.3760/cma.j.cn211501-20221008-03081
21. Elmir R, Schmied V. A qualitative study of the impact of adverse birth experiences on fathers. Women Birth. 2022;35(1):e41–e48. doi:10.1016/j.wombi.2021.01.005
22. Tsakmakis PL, Akter S, Bohren MA. A qualitative exploration of women’s and their partners’ experiences of birth trauma in Australia, utilising critical feminist theory. Women Birth. 2023;36(4):367–376. doi:10.1016/j.wombi.2022.12.004
23. Charman C, Masterson C, Russell AM. ‘Would I risk it again?’ The long-term impacts of a traumatic birth, as experienced by fathers. J Reprod Infant Psychol. 2024;1–15. doi:10.1080/02646838.2024.2346893
24. Walker LO, Avant KC. Strategies for Theory Construction in Nursing.
25. Brown A, Nielsen JDJ, Russo K, Ayers S, Webb R. The Journey towards resilience following a traumatic birth: a grounded theory. Midwifery. 2022;104:103204. doi:10.1016/j.midw.2021.103204
26. Aksu DF, Serçekuş P. Traumatic childbirth experiences, effects and coping: a qualitative study. Sex Reprod Healthcare. 2023;37:100898. doi:10.1016/j.srhc.2023.100898
27. Yeo JH, Sagong H. Korean women’s perceptions of traumatic childbirth: a qualitative descriptive study. BMC Pregnancy Childbirth. 2023;23(1):687. doi:10.1186/s12884-023-05986-8
28. Kuipers YJ, Thomson G, Goberna-Tricas J, et al. The social conception of space of birth narrated by women with negative and traumatic birth experiences. Women Birth. 2023;36(1):e78–e85. doi:10.1016/j.wombi.2022.04.013
29. Ketley R, Darwin Z, Masterson C, McGowan L. Women’s experience of post-traumatic growth following a traumatic birth: an interpretive phenomenological analysis. J Reprod Infant Psychol. 2024;42(1):126–137. doi:10.1080/02646838.2022.2070608
30. Molloy E, Biggerstaff DL, Sidebotham P. A phenomenological exploration of parenting after birth trauma: mothers perceptions of the first year. Women Birth. 2021;34(3):278–287. doi:10.1016/j.wombi.2020.03.004
31. Ma D, Sun S, Qian J, et al. Predictors of pregnancy stress and psychological birth trauma in women undergoing vaginal delivery: a cross-sectional study in China. BMC Pregnancy Childbirth. 2023;23(1):596. doi:10.1186/s12884-023-05890-1
32. Lian ZR, Yuan Z, Zheng LL, et al. Birth trauma experiences in women: a meta-synthesis. China Nurs Manag. 2022;009:022.
33. Chabbert M, Panagiotou D, Wendland J. Predictive factors of women’s subjective perception of childbirth experience: a systematic review of the literature. J Reprod Infant Psychol. 2021;39(1):43–66. doi:10.1080/02646838.2020.1748582
34. McKelvin G, Thomson G, Downe S. The childbirth experience: a systematic review of predictors and outcomes. Women Birth. 2021;34(5):407–416. doi:10.1016/j.wombi.2020.09.021
35. Viirman F, Hess Engström A, Sjömark J, et al. Negative childbirth experience in relation to mode of birth and events during labour: a mixed methods study. Eur J Obstet Gynecol Reprod Biol. 2023;282:146–154. doi:10.1016/j.ejogrb.2023.01.031
36. Wang H, Liang Y, Zhou L, et al. A concept analysis of birth trauma. Chin J Modern Nurs. 2022;29(19):2652–2657. doi:10.3760/cma.j.cn115682-20220819-04052
37. Watson K, White C, Hall H, Hewitt A. Women’s experiences of birth trauma: a scoping review. Women Birth. 2021;34(5):417–424. doi:10.1016/j.wombi.2020.09.016
38. Fan XM, Pu CS, Zhang AX, Zhou CX, Zhu Z. Research progress of maternal psychological birth trauma. Chin J Nurs. 2022;10:1256–1262. doi:10.3761/j.issn.0254-1769.2022.10.016
39. Leinweber J, Fontein-Kuipers Y, Thomson G, et al. Developing a woman-centered, inclusive definition of traumatic childbirth experiences: a discussion paper. Birth. 2022;49(4):687–696. doi:10.1111/birt.12634
40. Yalnız H, Canan F, Genç RE, Kulo˘glu MM, Geçici Ö. Development of a scale of traumatic childbirth perception. Turk J Med Sci. 2016;8:81–88. doi:10.5505/ttd.2016.40427
41. Wilkinson JM. Moral distress in nursing practice: experience and effect. Nurs Forum. 1988;23(1):16–29. doi:10.1111/j.1744-6198.1987.tb00794.x
42. Meyer S, Hohlfeld P, Achtari C, Russolo A, De Grandi P. Birth trauma: short and long term effects of forceps delivery compared with spontaneous delivery on various pelvic floor parameters. BJOG. 2000;107(11):1360–1365. doi:10.1111/j.1471-0528.2000.tb11648.x
43. Beck CT. Birth trauma: in the eye of the beholder. Nurs Res. 2004;53(1):28–35. doi:10.1097/00006199-200401000-00005
44. Baker KG. Evaluation of DSM-5 and IWG-2 criteria for the diagnosis of Alzheimer’s disease and dementia with Lewy bodies. Diagnosis. 2016;3(1):9–12. doi:10.1515/dx-2015-0031
45. Ayers S, Wright DB, Thornton A. Development of a measure of postpartum PTSD: the city birth trauma scale. Front Psychiatry. 2018;9:409. doi:10.3389/fpsyt.2018.00409
46. Taghizadeh Z, Arbabi M, Kazemnejad A, Irajpour A, Lopez V. Iranian mothers’ perceptions of the impact of the environment on psychological birth trauma: a qualitative study. Int J Nurs Pract. 2015;21 Suppl 2:58–66. doi:10.1111/ijn.12286
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.