Back to Journals » International Medical Case Reports Journal » Volume 19
A Successful Single-Stage Reconstruction of an Isolated Female Epispadias in a 14-Year-Old Patient: A Case Report and Literature Review
Authors Mtafu NH, Mitamo AA ![]() , Mtaturu GF, Mhaya JK, Kashaija JM, Ndola I, Nyongole O, Mkony C
, Mtaturu GF, Mhaya JK, Kashaija JM, Ndola I, Nyongole O, Mkony C
Received 11 August 2025
Accepted for publication 31 December 2025
Published 6 January 2026 Volume 2026:19 559971
DOI https://doi.org/10.2147/IMCRJ.S559971
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Xudong Zhu
Naomi Herbert Mtafu,1 Alexandre Amini Mitamo,1,2 Gabriel Francis Mtaturu,3 Joachim Kulwa Mhaya,1 John Mugisha Kashaija,1 Ibrahim Ndola,1 Obadia Nyongole,1 Charles Mkony1
1Department of Surgery, School of Medicine, Muhimbili University of Health and Allied Sciences, Dar Es Salaam, Tanzania; 2Department of Surgery, School of Medicine, Université Catholique du Graben, Butembo, Democratic Republic of the Congo; 3Department of Urology, Muhimbili National Hospital, Dar Es Salaam, Tanzania
Correspondence: Alexandre Amini Mitamo, Department of Surgery, School of Medicine, Université Catholique du Graben, P.O. Box 29, Butembo, Democratic Republic of the Congo, Tel +243995568170, Email [email protected]
Abstract: Epispadias is a rare congenital disorder characterized by an abnormal dorsal opening of the urethra due to the failure of the urethral plate to tubularize. It is usually part of broader conditions like bladder or cloacal exstrophy and rarely occurs in isolation. We present the case of a 14-year-old girl with isolated epispadias who had lifelong urinary incontinence without urgency. Genital examination revealed a bifid clitoris, underdeveloped labia minora, and a widely open urethral meatus with continuous leakage of urine. Urethrocystoscopy showed a short, patulous urethra, a poorly coapting external sphincter, and an open bladder neck. She underwent a successful single-stage surgical repair consisting of urethroplasty, bladder neck reconstruction, and perineoplasty. Two weeks after surgery, following catheter removal, the patient achieved urinary continence. This case supports the effectiveness of single-stage reconstruction even in delayed presentations of isolated female epispadias.
Keywords: isolated female epispadias, single-stage reconstruction, urinary continence
Introduction
Epispadias is a disorder characterized by an abnormal opening of the urethra and the failure of the urethral plate to tubularize on the dorsum. It is most frequently identified as a part of bladder exstrophy.1
Isolated female epispadias is a rare congenital anomaly, occurring in 1 in 484,000 females.2 Three levels of epispadias are described in the Davis (1928) classification for female patients. When epispadias is in its mildest form, the urethral orifice just looks patulous. The urethra is dorsally split along most of its length in intermediate epispadias. When epispadias is at its worst, the patient becomes incontinent due to the urethral cleft affecting the entire length of the urethra and sphincteric mechanism.3
A bifid clitoris is a characteristic of the genital defect. The skin over the mons is smooth and glabrous, giving it a depressed shape. The skin may be closely applied to the anterior and inferior surfaces of the symphysis pubis, or there may be a moderate amount of subcutaneous tissue and fat beneath this region. The anterior half of the bifid clitoris is where the labia minora terminate, usually poorly developed, and may have the beginnings of a preputial fold. These external features are the most distinctive: As previously mentioned, the urethra is visible upon minimal separation of the labia. Usually closed, the symphysis pubis can also be visualized as a narrow band of fibrous tissue. Internal genitalia and the vagina are typically normal.4–6
The surgical objectives encompass restoring urinary continence, preserving the upper urinary tract function, and reconstructing the external genitalia to ensure both functional integrity and an anatomically acceptable appearance.1,4–11
Case History/ Examination
A 14-year-old girl was admitted to our facility complaining of urinary incontinence since birth. The urinary incontinence occurred both during the day and night and was characterized by the absence of the urge to urinate. She reported significant increase in urine leakage with fluid intake, requiring her to wear diapers and change them at least four times per day to stay dry. However, there was no reported history of recurrent urinary tract infection or recurrent fevers. The patient was born through vaginal delivery, at term, with a birth weight of 3.0Kg. The patient had normal developmental milestones. She was the sixth child in a family of eight siblings. Her sisters had no similar complaints, and there was no family history of congenital anomalies on either the maternal or paternal side. The patient was a grade four pupil and reported inability to cope with studies and having to deal with social discrimination due to cloth wetting and smell of urine. During the course of her illness the patient was being treated with herbal medications, and later on went to a nearby health facility where they referred her at our hospital for surgical reconstruction. Physical examination revealed vital signs within the normal range, a body weight of 42 kg, a height of 150 cm and a BMI of 18.67 kg/m2. No mass or bulging was observed in the flank area. The mons pubis was non-hairy and poorly developed (depressed). The patient had a bifid clitoris, underdeveloped labia minora terminating on the respective halves of the bifid clitoris, and a patulous urethral opening anterior to the bifid clitoris with continuous urine leakage. The patient had normal formed labia major, normal vaginal orifice and hymen, and normal position of the anus (Figures 1). The spine examination revealed normal findings with no signs of spina bifida. Other systemic examination was unremarkable. Thus, the diagnosis of isolated female epispadias was made.
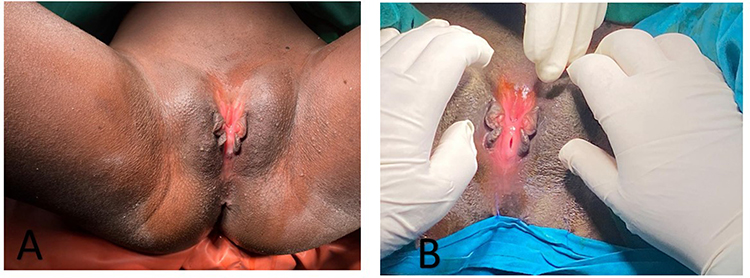 |
Figure 1 A preoperative appearance of an external genitalia examination showing non hairy, poorly formed (depressed) mons, bifid clitoris, underdeveloped labia minora terminating on respective halves of the bifid clitoris, patulous urethra opening anteriorly to bifid clitoris (A and B), and normally located vaginal opening (B). |
Investigations and Treatment
Laboratory results of urine test, full blood picture and serum biochemistry were in normal range. KUB ultrasound revealed a normal scan. Owing to resource limitations at our institution, video-urodynamic studies could not be performed, as this modality is not currently available. However, urethrocystoscopy was performed, revealing a patulous and a very short urethra measuring 0.5cm of length, and a poorly coapting external urethral sphincter, open bladder neck (shark mouth appearance), wide open right ureteric orifice with normal appearing left ureteric orifice, and normal bladder mucosa (Figure 2).
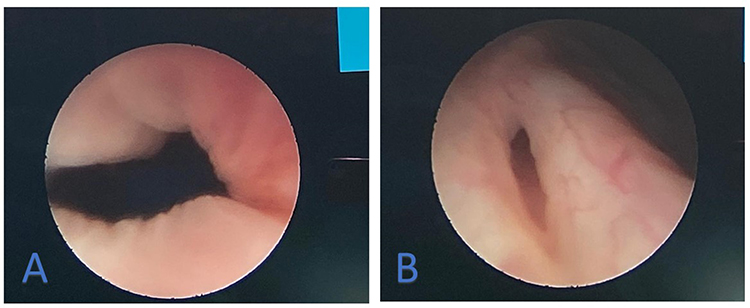 |
Figure 2 The urethrocystoscopy showed a very short urethra with a measured length of 0.5cm, poorly coaptating external urethral sphincter, open bladder neck (shark mouth appearance) (A), wide open right ureteric orifice (B). |
The surgical reconstruction was carried out in lithotomy position, stay sutures were placed in the wall of the urethra on either side. A “smile” incision (from 9 to 3 o’clock) was used to free the urethra from the clitoris and the surrounding tissues. There was no disruption of the plane between the urethra and the vagina (Figures 3). Full mobilization of the urethra and the bladder neck anteriorly was achieved. Suprapubic cystostomy catheter was inserted through a suprapubic stab incision onto a tip of a right-angled forceps that was passed through the bladder neck. A 3-cm-wide patch of bladder wall, extending from mid-trigone across the bladder neck, was excised to facilitate narrowing of the bladder neck.
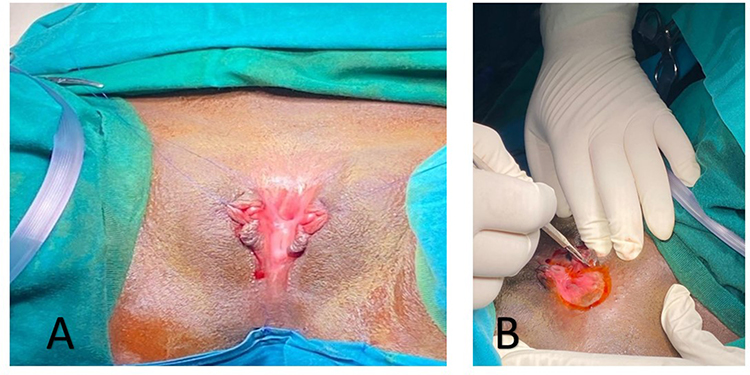 |
Figure 3 Showing stay sutures at 3 and 9 o’clock (A) and the incision mark (B). |
The bladder neck was reconstructed by Marshall technique followed by tubularization of the urethra with 5/0 PDS sutures over a 12 Fr Foley catheter, achieving a urethral length of 4cm. Subcutaneously the bifid clitoral structures and labia minora were joined in the midline. The surgical procedure was completed, achieving a cosmetically acceptable mons pubis through approximation of the bifid clitoris, incising the lateral sulci between the labia majora and minora, allowing the superomedial rotation of the labia majora and underlying peripubic adipose tissue. The surgical wound was dressed with Mupirocin (Figure 4).
 |
Figure 4 Final appearance after surgical reconstruction with 12Fr SPC catheter and urethral catheter insitu. |
Outcome and Follow-up
The patient was kept on intravenous antibiotics for seven days with daily surgical wound care. On day 5 postoperatively she had surgical wound gaping and pus discharge with no urine leakage; she was managed with daily sitting baths, continuation of intravenous antibiotics and Mupirocin cream. The per-urethral and SPC catheters were removed on postoperative day 10 and 14, respectively (Figure 5), the latter being removed after satisfactory voiding through the reconstructed urethra was confirmed. After removal of urethral catheter, the patient was able to attain continence for the first time in her life, as she felt bladder fullness, the urge to urinate and feeling of complete bladder emptying. The patient was instructed on performing Kegel exercises to strengthen pelvic muscles. She was discharged home on day 20 postoperatively, with a two weeks follow-up plan at the outpatient department clinic where she reported urge and control over micturition, no dysuria, no straining during micturition, and no leakage with stress maneuvers (laughing, coughing). The patient was lost to follow-up after two outpatient visits, preventing completion of the planned postoperative assessments, including renal ultrasonography and voiding cystourethrogram (VCUG).
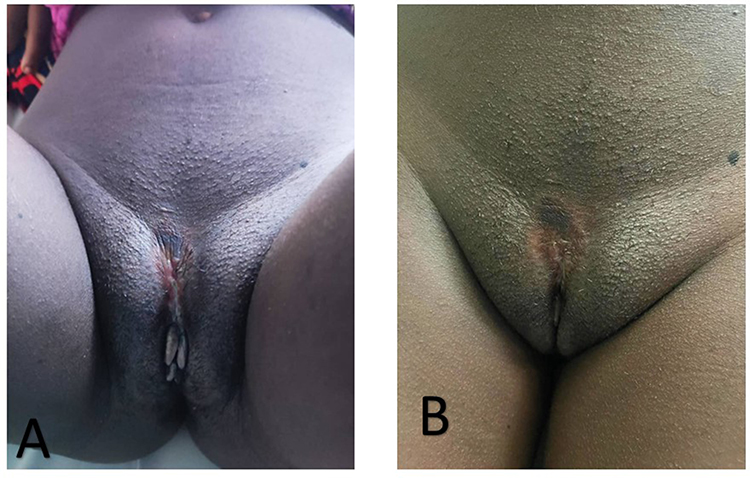 |
Figure 5 External genitalia condition 3 weeks post-surgical reconstructions (A) and 5 weeks post-surgical reconstructions (B). |
Discussion
Isolated Female Epispadias (IFE) is a rare congenital anomaly of the lower urogenital tract that affects 1 in 484,000 females, with cases ranging from newborns to 39-year-old adults, according to published research.1 The majority of the published cases showed different levels of urine incontinence. Davis categorized isolated female epispadias into three groups based on their appearance: mild, moderate, and severe. In mild cases, the urethra may only be patulous. The urethra’s dorsal surface is split in mild cases. Urinary incontinence is a symptom of severe cases in which the bladder neck and the urethra are both relatively short and wide, and deficient in the sphincteric mechanism.3 Because mild cases are difficult to identify, they are rarely discussed in the literature. Without separating the labia majora and doing a thorough physical examination, which is often overlooked when assessing neonates, it would be very difficult to diagnose these cases.4,5,8,9 The severe form is readily diagnosed due to urinary incontinence resulting from an inadequate sphincteric mechanism and an underdeveloped bladder neck. However, the hymen and vagina are typically well developed in the affected individuals.8,9
Low urethral pressure, low bladder capacity, and incomplete bladder neck are the most common causes of incontinence in IFE patients.4
In general, surgical repair is required to achieve functional and aesthetic restoration of the external genitalia, ensure preservation of the upper urinary tract, and establish urinary continence.1,4–11
Acceptable anatomical appearance and functional outcomes are achieved through urethral reconstruction combined with clitoral and labia minora reconstruction. The definitive IFE operation is described as a two-stage operation in the majority of the literature. The initial phase generally involves genito-urethral reconstruction, followed by bladder neck repair after one to two years to restore continence.4,5,9,11
Hendren originally advocated for a single-stage approach to genito-urethral and bladder neck reconstruction. In their study involving six cases, three patients underwent the single-stage procedure, while the remaining three received the conventional combination approach. The current IFE treatment strategy focuses on improving cosmetic outcomes by releasing the patulous urethra through an incision from the 9 to 3 o’clock positions. This step is immediately followed by the simultaneous creation of a functional neourethra and genitoplasty.4,5,9,11
Our patient had double bladder drainage through a suprapubic and a transurethral urinary catheter. The transurethral catheter was removed first, followed by the suprapubic, after assessing the voiding patterns. Contemporary reconstructive urology practice and case series report maintaining SPC as protective drainage while the urethral catheter is removed and voiding is tested; the SPC is then clamped/removed only after satisfactory voiding and/or imaging confirmation (VCUG). For example, in a series of modified Cantwell–Ransley epispadias repairs the per-urethral catheter was removed on postoperative day 14 while the suprapubic catheter was clamped and retained until successful voiding was demonstrated.12 Similarly, combined bladder-exstrophy/epispadias protocols report earlier removal of per-urethral catheters with SPC retained for several weeks to ensure safe bladder drainage.13
Per the Davis criteria, our patient was a severe case. Her condition included low urethral resistance, an incomplete bladder neck, and low bladder capacity. With bladder neck and urethral reconstruction, we were able to create a 4-cm urethra in a single surgical session. We were able to restore normal urethral resistance 14 days after the removal of the urethral catheter and SPC, as evidenced by the patient’s desire to urinate and the resolution of their incontinence. Postoperative continence was assessed clinically, based on subjective reports and observation during hospital stay and outpatient visits.
In epispadias, the ureterovesical junction is inherently deficient, and the ureters often enter the bladder laterally along a straight course, both of which predispose to vesicoureteral reflux. According to reports, between 30% and 75% of patients with isolated female epispadias have reflux.1 Therefore, postoperative follow-up of upper urinary tracts is critically important, as correction of incontinence may exacerbate vesicoureteral reflux.
This case report has several limitations. First, urodynamic studies were not performed preoperatively or postoperatively due to their unavailability at our institution. Second, long-term outcomes could not be assessed because of loss to follow-up.
Conclusion
A thorough genital examination in female children is essential to ensure early detection of rare anomalies such as isolated female epispadias. Even in cases of delayed diagnosis, effective management can be achieved through a single-stage surgical approach combining urethroplasty, bladder neck reconstruction, and perineoplasty.
Ethics Statement
Institutional approval was not required for publication of the case details.
Consent
Written informed consent was obtained from the parent of the patient for the publication of this case report, including authorization to use any accompanying images.
Acknowledgments
We would like to express our gratitude to the entire surgical team for their unwavering support throughout the entire hospital stay of the patient.
Author Contributions
All authors contributed significantly to the development of this case report, including: clinical management of the patient, collection and interpretation of clinical information, literature review, and preparation of the manuscript. All authors participated in drafting, revising, and critically reviewing the article. All authors approved the final version to be published, agreed on the journal of submission, and accept accountability for all aspects of the work.
Funding
There is no funding to report.
Disclosure
All authors declare no competing interest in this work.
References
1. Tantibhedhyangkul J, Copland SD, Haqq AM, Price TM. A case of female epispadias. Fertil Sterility. 2008;90(5):2017–7. doi:10.1016/j.fertnstert.2007.12.055
2. Gearhart JP. Exstrophy, epispadias, and other bladder anomalies. Campbell Urolog. 2002;3:2136–2196.
3. Davis DM. Epispadias in females and its surgical treatment. J Urol. 1928;20(6):673–678. doi:10.1016/S0022-5347(17)73196-5
4. Rangganata E, Wahyudi I. Single-stage repair for female epispadias with urinary incontinence: a case report and literature review. Int J Surg Case Rep. 2022;94:107013. doi:10.1016/j.ijscr.2022.107013
5. Lazarus J, van den Heever A, Kortekaas B, Alexander A. Female epispadias managed by bladder neck plication via a perineal approach. J Pediatric Urolog. 2012;8(3):244–248. doi:10.1016/j.jpurol.2011.06.006
6. Macedo A, da Cruz ML, Trivelato R, et al. Complete female epispadia: the case for perineal approach. J Pediatric Urolog. 2015;11(1):49–50. doi:10.1016/j.jpurol.2014.08.013
7. Apicella A, Marzuillo P, Marotta R, La Manna A. Female Epispadias. J Pediatr. 2015;167(5):1164. doi:10.1016/j.jpeds.2015.08.001
8. Atilgan D, Uluocak N, Erdemir F, Parlaktas BS. Female epispadias: a case report and review of the literature. Kaohsiung J Med Sci. 2009;25(11):613–616. doi:10.1016/S1607-551X(09)70565-0
9. Arslan MS, Arslan S, Zeytun H, et al. A case of isolated female epispadias and our approach to treatment. African J Urolog. 2016;22(3):193–195. doi:10.1016/j.afju.2015.09.008
10. Jonuzi A, Popovic N, Zvizdic Z, Milišic E, Karavdic K, Paddy D. Female epispadias presenting as urinary incontinence. APSP J Case Rep. 2017;8(2):10. doi:10.21699/ajcr.v8i2.548
11. Bhat AL, Bhat M, Sharma R, Saxena G. Single-stage perineal urethroplasty for continence in female epispadias: a preliminary report. Urology. 2008;72(2):300–303. doi:10.1016/j.urology.2007.09.073
12. Gite VA, Jain HM, Bote SM, Nikose JV. Modified Cantwell-Ransley repair for isolated continent epispadias in adult: our experience. Indian J Plast Surg. 2017;50(1):68–73. doi:10.4103/ijps.IJPS_243_16
13. Chaudhary R, Apte A, Mehta R, et al. Combined bladder exstrophy and epispadias repair. BMJ Case Rep. 2011;2011:bcr0420114141. doi:10.1136/bcr.04.2011.4141
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.