Back to Journals » Risk Management and Healthcare Policy » Volume 15
A Study of Body Modification Artists’ Knowledge, Attitudes, and Practices Toward Infection Control: A Questionnaire-Based Cross-Sectional Study
Received 9 February 2022
Accepted for publication 13 April 2022
Published 19 April 2022 Volume 2022:15 Pages 713—725
DOI https://doi.org/10.2147/RMHP.S361711
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Jongwha Chang
Aiggan Tamene,1 Bethlehem Yemane2
1Department of Environmental Health, School of Public Health, College of Medicine and Health Sciences, Wachemo University, Hosaena, Southern Nations Nationalities and Peoples’ Region, Ethiopia; 2Department of Environmental Health, College of Medicine and Health Sciences, Hawassa University, Hawaasa, Sidama Region, Ethiopia
Correspondence: Aiggan Tamene, Department of Environmental Health, School of Public Health, College of Medicine and Health Sciences, Wachemo University, Hosaena, Southern Nations Nationalities and Peoples’ Region, Ethiopia, Email [email protected]
Background: Tattoos and piercings, which were once considered taboo, are now widespread like an epidemic, among people of all ages and gender. The rising demand for such body alterations has given rise to a large number of infective complications. This study was, therefore, designed to assess the infection control knowledge, attitudes, and practices of body modification artists in Ethiopia, 2021.
Methods: An anonymous observational cross-sectional study was conducted in Addis Ababa, Ethiopia, from May 25 to June 22, 2021. The data collection instrument was a structured questionnaire that covered the participants’ socio-demographic characteristics, knowledge, attitudes, and practices related to infection control. On the whole, 172 tattoo and body piercing artists participated in the study. SPSS v.20 software was used for data entry and analysis. Pearson’s correlation test, t-test, Tukey’s test, and multiple linear regression analysis were conducted during the data analysis.
Results: Male participants constituted well over three-fourths (96.5%, n = 166) of the sample considered in the study. According to the result, the participants’ knowledge of infection control received the lowest score (7.1 ± 1.22). Participants’ scores of knowledge of infection control increased with an increase in their experience in the multiple linear regression. Experience and training time were also associated with knowledge. Infection control practice was positively associated with the respondents’ attitudes. After controlling other variables, it was found that a one-unit increase in respondents’ attitude scores increased their practice level by 86%.
Conclusion: This is the first study in Ethiopia to examine tattooists’ and body piercers’ infection control knowledge, attitude, and practice. Minimum standards for infection control in inking and piercing establishments are necessary. It is therefore important that local authorities and public health professionals work towards laying down the minimum code of practice for infection control in inking and piercing establishments.
Keywords: tattoo, piercing, infection control, knowledge, attitude, practice
Introduction
Body alteration, commonly known as tattooing, skin piercing, and jewellery insertion, has been practiced by humans for about 5000 years.1 Modern tattooing is done using an electric machine that has a cluster of fast rotating needles that deposit liquid colour into the upper layer of the dermis.2 Body piercing, on the other hand, entails the insertion of a needle into the body to create a fistula and implant decorative ornaments in areas other than the ear lobe.3
Tattoos and piercings which used to be considered taboo in the past, have now become widely accepted forms of body alterations.4 The practice appears to be particularly acceptable among adolescents and youths. The percentage of tattooed people in these age categories ranges from 1 to 24%, whereas the prevalence of body piercing ranges from 4.3% to 51%.5 The rising demand for body alterations worldwide has given rise to many unprofessional body art practitioners. Such practitioners lack the knowledge required to carry out procedures following health and hygiene standards.
Skin that is free of cuts, abrasions, or lesions is called intact skin. Intact skin provides a natural barrier to infection. Cuts, sores, and sharp items that penetrate the skin often allow infections to enter the body.6 Body modification that involves skin penetration, such as tattooing or piercing (T&P), puts people at the risk of contracting blood-borne infections.7,8 It has been proved that blood-borne infections are often etiologically associated with Human Immunodeficiency Viruses (HIV), Hepatitis B, Hepatitis C, Septicaemia, and Tetanus.9 The prevalence of tattoo complications is estimated to be around 2–3%. The majority of these complications are caused by an infection, which can be traced back to a tattooist who uses a non-sterile technique. A tattoo artist has even been known to transmit syphilis by licking the tattoo needle.10,11 Piercing complications are more prevalent, with rates as high as 9%.12,13
Strict adherence to infection control standards throughout the tattooing and/or the body piercing procedure is recommended to limit the risk of infection. The recommended measures need to be observed until the healing of the wound inflicted by tattooing/piercing of the body.14 This implies that the services be provided only by a skilled, competent person with sufficient knowledge of infection control. All blood and bodily fluids should be treated as potentially infectious. Taking extra precautions has the potential to minimize risks in this regard.15 Equally important measures needed to avoid the spread of infection are hand washing, using clean and/or sterile instruments, proper waste disposal, safe procedures, and clean facilities.16
Adherence to such control measures can primarily be influenced by body modification artists’ knowledge of, attitude to, and practices of infection control.17 The “KAP theory” is a health behavior change theory that divides human behavior change into three stages: knowledge acquisition, attitude formulation, and behavior adoption (or practice). A person’s KAP level has been connected to optimal illness prevention and management, as well as personal health promotion in past studies. KAP deficiencies, on the other hand, have been linked to poor health and poor disease prevention behavior.18 This is particularly important for public health because of the immense potential risk of blood-borne infections in nonmedical services. Nonmedical service procedures are conducted with less epidemiological supervision than is required in the healthcare service sector.19
Over the last couple of decades, Ethiopia has grown more and more urbanized. Following this, body modification has dramatically become popular among teenagers and young adults. In more recent years, tattooing and body piercing have increasingly grown among teenagers as a fashion statement or to improve body image. Despite the rapid growth of the tattoo and piercing industry, however, no systematic regulation is in place in the industry. The sparse literature on Ethiopian T&P regulation reveals that we still lack viable models for standards and techniques that can work at scale to maintain safety in contexts where risks are prevalent, compliance costs are high, and enforcement capability is inadequate.
Several European states have conducted studies on the conditions in which tattoo and piercing parlours operate.20 However, due to the immense differences in regulatory regimes, solutions that have succeeded in developed countries cannot be automatically applied to the conditions in developing countries. The motivation for the present study arose from this recognition. The goal of this study was therefore to investigate body piercing and tattoo artists’ knowledge of infection control, their attitude to and practice of infection control. It is hoped that the findings will help stakeholders improve T&P safety guidelines and their implementation. The study will also give policymakers relevant insight that will help them make informed decisions about the industry’s future line of development.
Methods
Study Area and Setting
A cross-sectional infection control practice survey was conducted in Addis Ababa from May 25 to June 22, 2021. Addis Ababa is Africa’s seventh-largest city. It is a self-administered city that has a population of 5,005,524. The city represents 25% of Ethiopia’s total urban population.21
Inclusion and Exclusion Criteria
The study included tattooists and body piercers working in Addis Ababa. Individuals not directly involved in the tattooing and body piercing activities were excluded.
Sample Size Calculation and Sampling Procedure
The sample size was determined using a formula for a single population that took into account various assumptions. No prior research on infection control practices among tattooists and body piercers was identified and accessed in Ethiopia. Because of this, the largest sample size assumption was used, with a prevalence among un-exposed at p=50%, a margin of error (d) of 5%, and a 95% level of confidence. The Epi-InfoTM7 program generated a total sample size of 384 based on these assumptions.
According to the data acquired from Addis Ababa Commerce and Investment Office, there were 146 body art practitioners in 111 businesses in the city during data collection. Firms that had storefront signage advertising T&P and that offered such services online to the general public were also addressed to compensate for the potential incompleteness of the data received from the bureau. This led to the discovery of 29 more body artists in 16 other establishments. In the end, a total of 175 T&P practitioners working in 117 T&P parlours were discovered.
Next, because the sample was taken from a finite population, a correction formula was applied. The ultimate sample size was 152 after accounting for a 10% non-response rate. However, to enhance the study’s precision or accuracy, all of the 175 study subjects were included in the study. It was also noted that data quality and available resources would not be jeopardized since this sample size of 175 did not differ significantly from the calculated sample size.
The Procedure of Data Collection
The data for the study was gathered using an interviewer-administered questionnaire. The questionnaire comprised socio-demographic questions and KAP-related questions that considered the three elements of KAP. Prior studies were used to identify the content relating to KAP concerns and their correct answers.22–24 Six questions were asked about the body modification artists’ age, sex, education, participation in infection control, safety training, and experience.
The KAP assessment was divided into three sections. The knowledge evaluation section had ten objective questions related to daily preventative practices. Topics like personal cleanliness and cross-contamination were considered in this section. The three response options used in the questionnaire were “Yes”; “No” and “I don’t know”. Similarly, the attitude evaluation section had ten questions. The focuses of the questions were the relevance of infection control protocols, the responsibility of body modification artists for preventing work-related infections, and the value of continued infection control practices.
In this study, Attitude was defined as a way of thinking that is mirrored in a person’s conduct. On a three-point scale, the tattooists and body modification artists were asked to express their level of agreement with the following response options: I “agree,” “disagree,” and “don’t know”.
The questionnaire’s final section addressed the evaluation of self-reported practices. The section had ten questions about the respondents’ everyday routines. Each practice was assessed using a five-point rating scale (1 = never, 2 = seldom, 3 = sometimes, 4 = frequently, and 5 = always). The scale was scored in reverse order for practices that were deemed inadequate. For knowledge questions, each correct answer received one point, while each incorrect or ‘I don’t know’ response received zero points. The knowledge block had a range of possible scores from 0 to 10. The attitude questions had a possible score range of 0 to 10 points. The available scores for the practice questions ranged from 10 to 50.
Data Quality Control
Distributing the questionnaire to strangers is often a matter of making a delicate balance between etiquette and expediency. Maintaining authenticity and improving the validity of the responses requires that the questionnaire be anonymous. As a result, all the questionnaires were de-identified during the analysis and the reporting of the data used in this study.
The data collecting instrument was translated from English to Amharic (ie, the country’s official language and the major language used in Addis Ababa). The translation was carried out by a health professional that was familiar with both the language and the health issues considered in the study. Cross-cultural translations took precedence over literal equivalencies during the translation. A two-day long training on the data collection procedures was given to the supervisor and the data collectors. The number of data collectors was 4. The data collection was completed in 28 days from May 25 to June 22, 2021.
The internal consistency (reliability) of the data gathering tools was assessed using Cronbach’s alpha test. The Cronbach’s alpha values for the knowledge, attitude, and practice sections were 0.812, 0.782, and 0.751, respectively. Finally, the questionnaire was beta-tested on 21 T&P practitioners at a comparable studio in the neighbouring city of Adama.
Data Management and Analysis
Throughout the data collection procedure, the completeness of the data was regularly checked. Epi-Info 7 software was used to code, label, validate, categorize, and enter data. The demographics of the participants, as well as their KAP of infection control, were described using frequency, percentage, mean, and standard deviation. The Kolmogorov–Smirnov test was used to determine the data’s normality. Under the circumstances in which a non-normal distribution was found, the data were log normalized before the parametric tests were run. The Pearson correlation test (r) was used to assess the correlation between the KAP scores. This was done taking into account the strength of the correlations and the respective likelihood of errors (p≤5%). The correlations were categorized as negligible (0.01 to 0.09), low (0.10 to 0.29), moderate (0.30 to 0.49), considerable (0.5 to 0.69), and high (0.70) based on their strength.25
To compare the means of the KAP score while considering socio-demographic variables, a t-test and analyses of variance (ANOVA), followed by Tukey’s test, were used. A higher score in the Knowledge, Attitude and Practice domains was indicative of the respondents who had good knowledge, a positive attitude, and safe practice. The variables that influenced the KAP scores were identified using multiple linear regression analysis. The model for multiple linear regression analysis was established to determine the impact of explanatory variables on KAP scores. The variables considered in KAP scores were education, experience, training participation, time since previous training, knowledge, and attitudes. The significance level for all analyses was set at 5%.
Results
Study Demographics
In total, 172 participants took part in the study. A commendable effort of sensitization was made before data collection. This resulted in a 98.2% response rate, with only 1.8% interview refusal. Table 1 shows the socio-demographic characteristics of 172 body modification artists. The majority of the participants (96.5%, n = 166) were male whose ages ranged from 20 to 29 years (44.8%, n = 78). In terms of education, the majority of the participants (57.9%, n = 99) had a high school education while 40.7% (n = 70) attended elementary school. The majority of the participants (39.5%, n = 68) reported having up to 5 years of work experience in body modification. They also reported attending at least two training sessions (74.4%, n = 128). During the data collection, the most recent training the participants claimed to have attended happened within the three months before data collection (52.0%, n = 44) (Table 1).
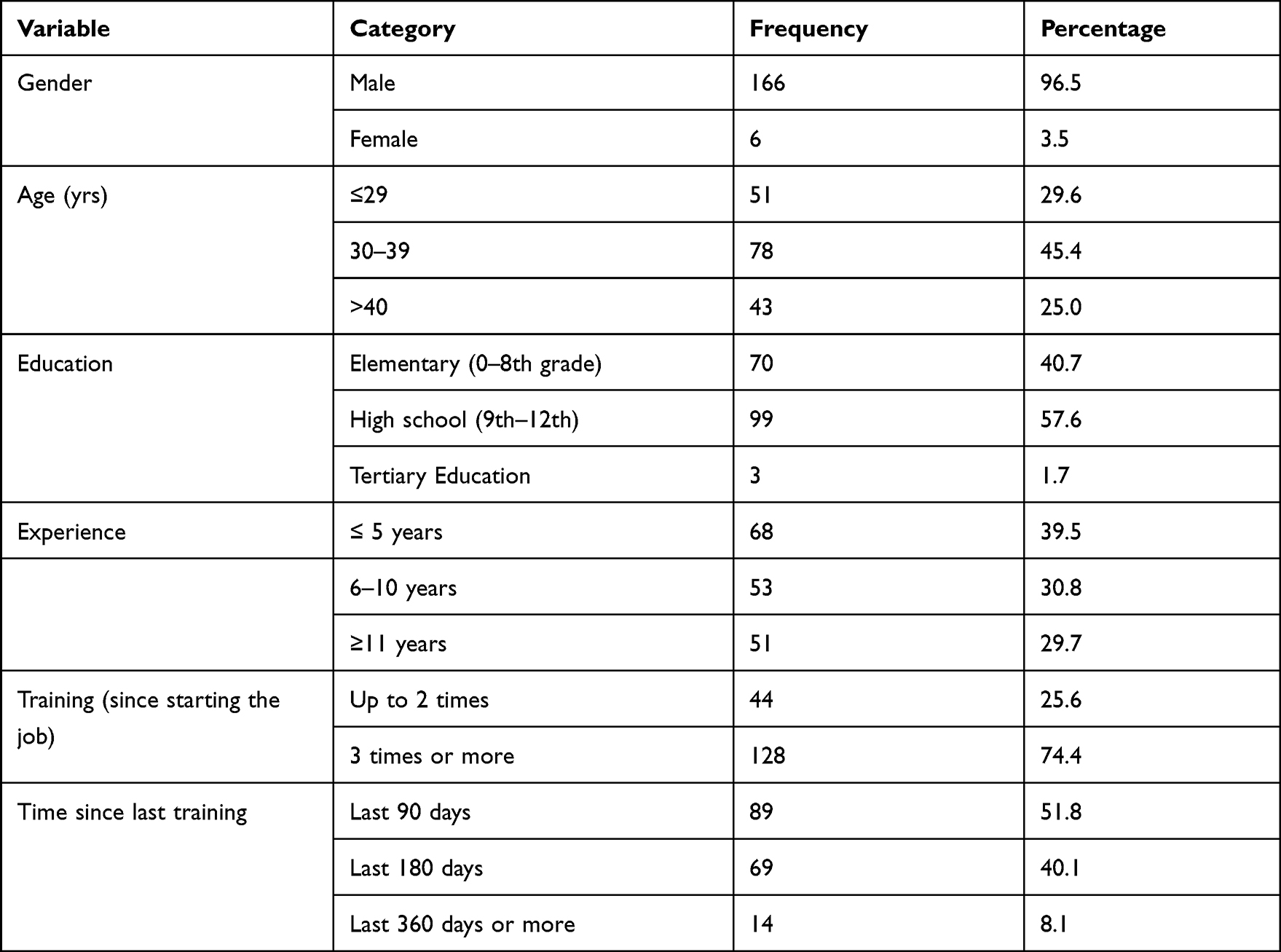 |
Table 1 Socio-Demographic Characteristics of Body Modification Artists in Addis Ababa, Ethiopia |
KAP Towards Infection Control
In the current study, the mean score for knowledge of infection control was 7.1, with a standard deviation of 1.22. On the other hand, participants performed well on the questions about attitudes, with a mean score of 9.4 and a standard deviation of 0.98. The mean reported practice score was 47.2, with a standard deviation of 3.80 (Table 2).
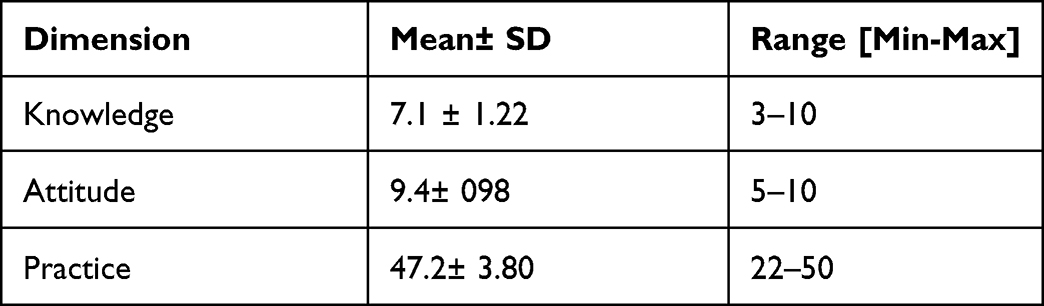 |
Table 2 Score Obtained for Knowledge, Attitudes, and Practices Regarding Infection Control, Addis Ababa, Ethiopia |
Knowledge of Infection Control
The risk of cross-contamination from body artists, the implementation of proper sanitizing measures, and appropriate sharp disposal techniques were among the knowledge-related questions that received a high percentage of correct answers. From the received 91.8% of incorrect answers to Question 1, it was possible to conclude that the respondents found the item to be the most challenging question. The majority of participants (61.6%) incorrectly believed that wearing gloves was a substitute for handwashing. Similarly, three-fourths of the respondents (75%) incorrectly believed dry heating to be one acceptable method of sanitizing needles (Table 3).
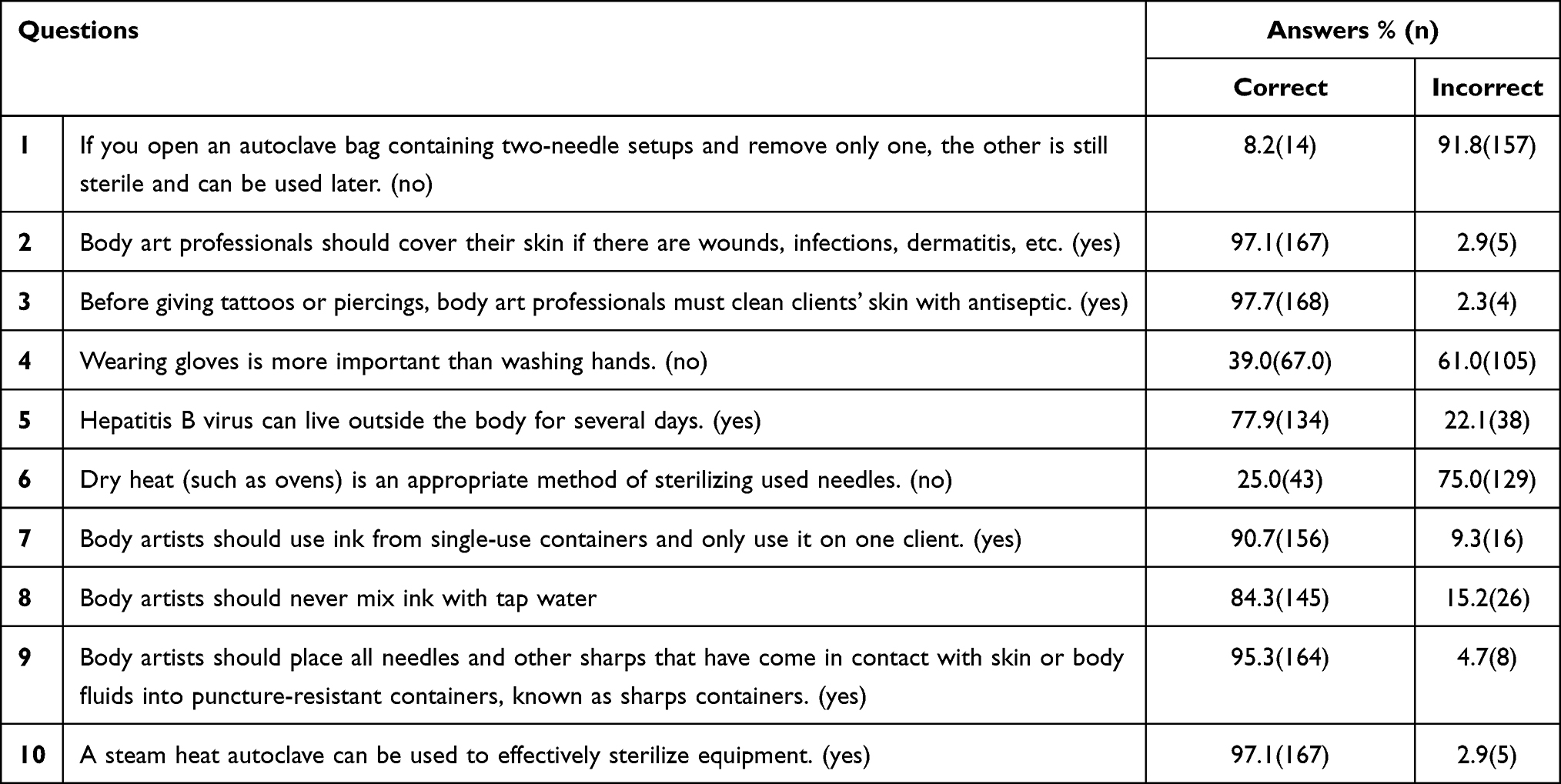 |
Table 3 Knowledge of Infection Control by Body Modification Artists in Addis Ababa, Ethiopia |
Attitude Towards Infection Control
In contrast to the knowledge segment, the participants did well on the questions on Attitudes (See Table 4). Item 6 in the section, for example, was correctly answered by all participants. However, it is important to note that 14.5% of the respondents believed that enforcing strict infection control practices increase business expenditures significantly.
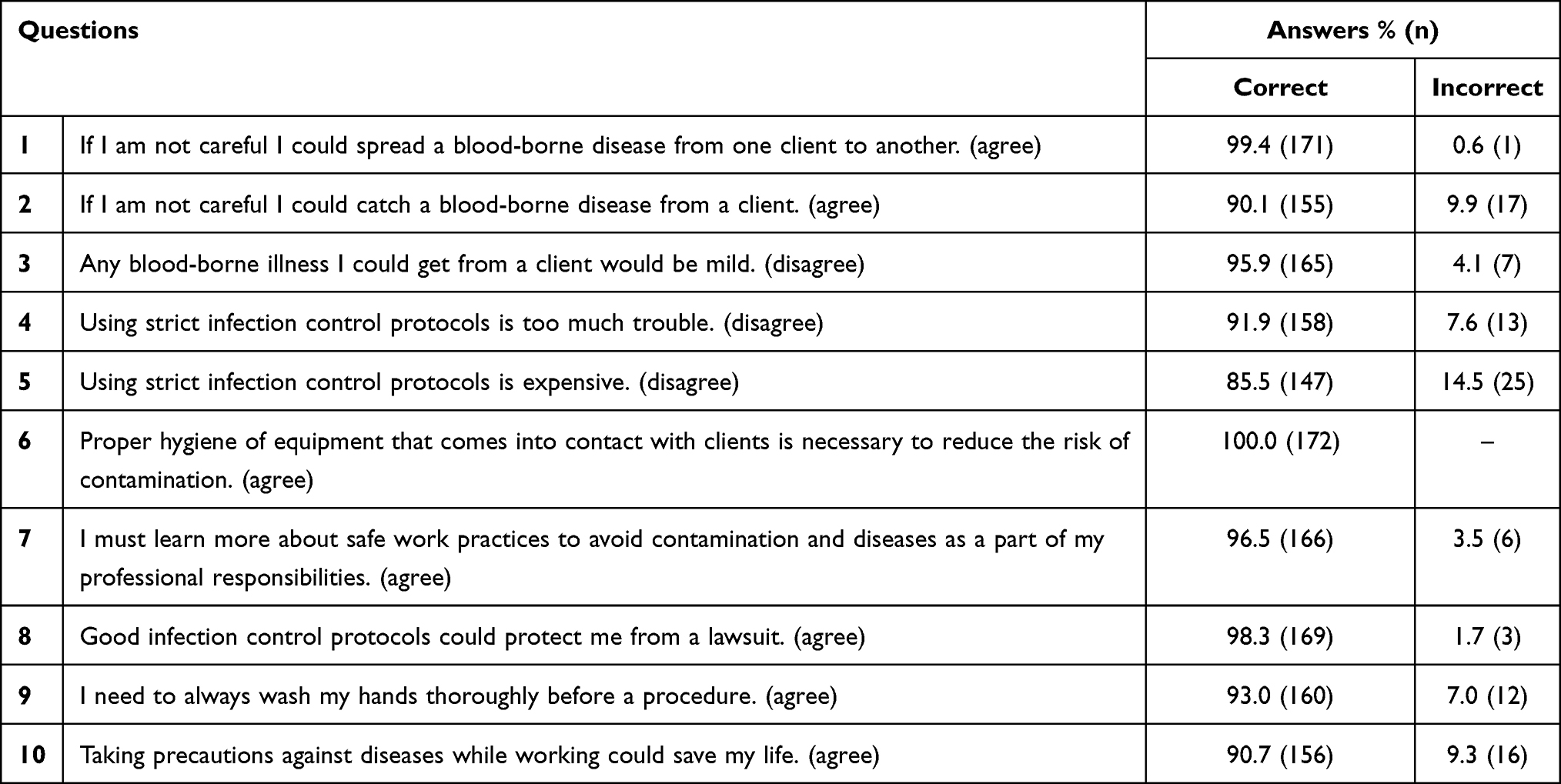 |
Table 4 Attitude Towards Infection Control by Body Modification Artists in Addis Ababa, Ethiopia |
Self-Reported Practice of Infection Control
Hand hygiene was reported to be performed by 72.7% of the respondents before performing a procedure. On the other hand, 84.3% said they wore gloves during procedures. Similarly, 87.8%, of the tattooists and piercing artists reported disposing of contaminated needles, syringes, and gloves. 83.1% reported never using sealed bags when autoclaving equipment (Table 5).
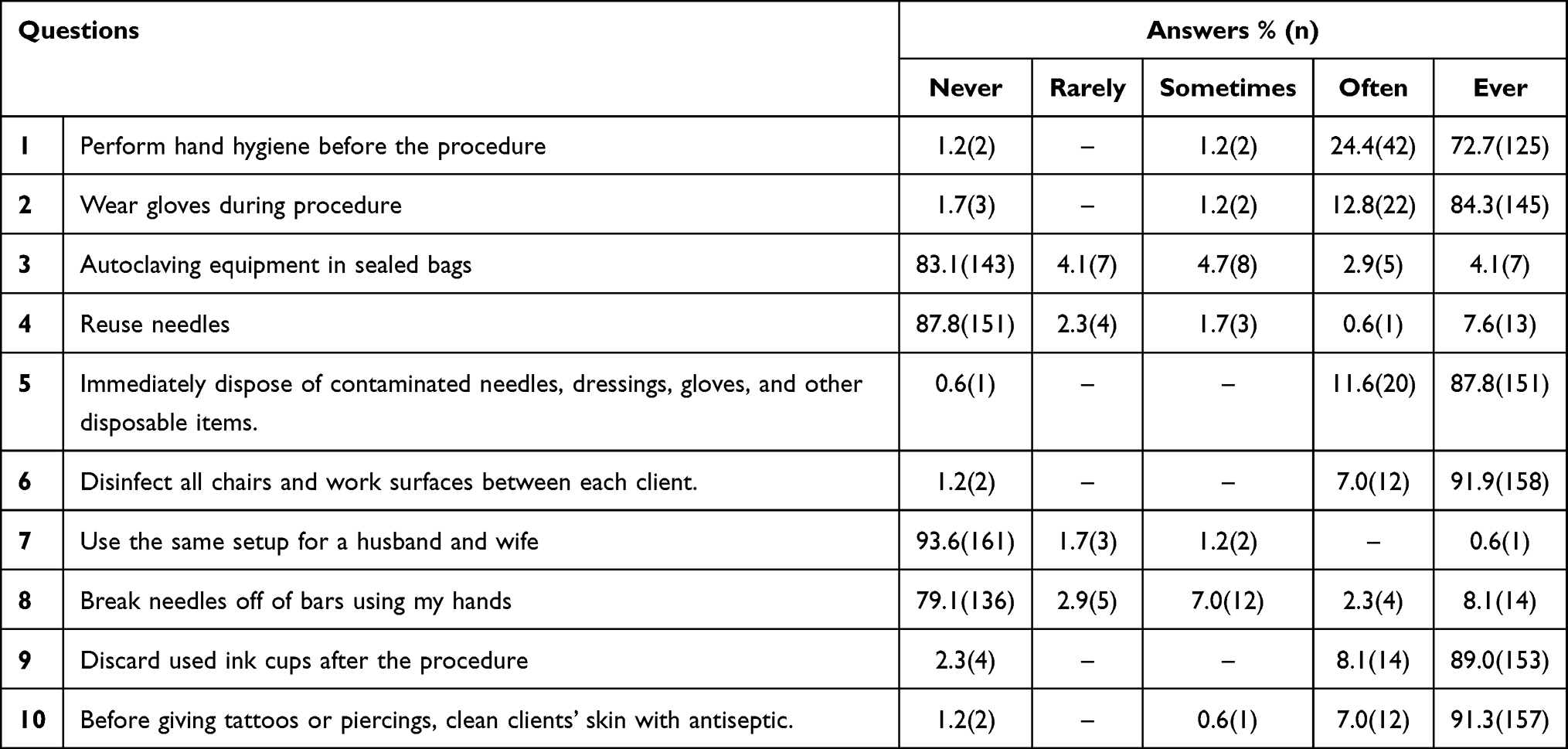 |
Table 5 Self-Reported Practice Towards Infection Control by Body Modification Artists in Addis Ababa, Ethiopia |
The Pearson correlation test (r) was performed to determine the correlation between the KAP scores, taking into account the strength of the correlations as well as the possibility of errors (p<5%). Knowledge and attitude, as well as attitude and practice, were associated. No association was observed between Self-reported practices and Knowledge scores (Table 6).
 |
Table 6 Pearson’s Correlation (r) Among the Scores Obtained in the Evaluation of KAP of Body Artists. Addis Ababa, 2021 |
Table 7 compares the mean scores obtained by body modification artists when socio-demographic characteristics are taken into account. Accordingly, there were significant variances in knowledge scores with regards to the amount of experience in the occupation and the time elapsed since their reported most recent training. Similarly, there was a substantial difference in attitude scores concerning schooling and the time they received the most recent training before data collection. Analysis of the data also revealed no significant differences in the scores obtained for infection control practices.
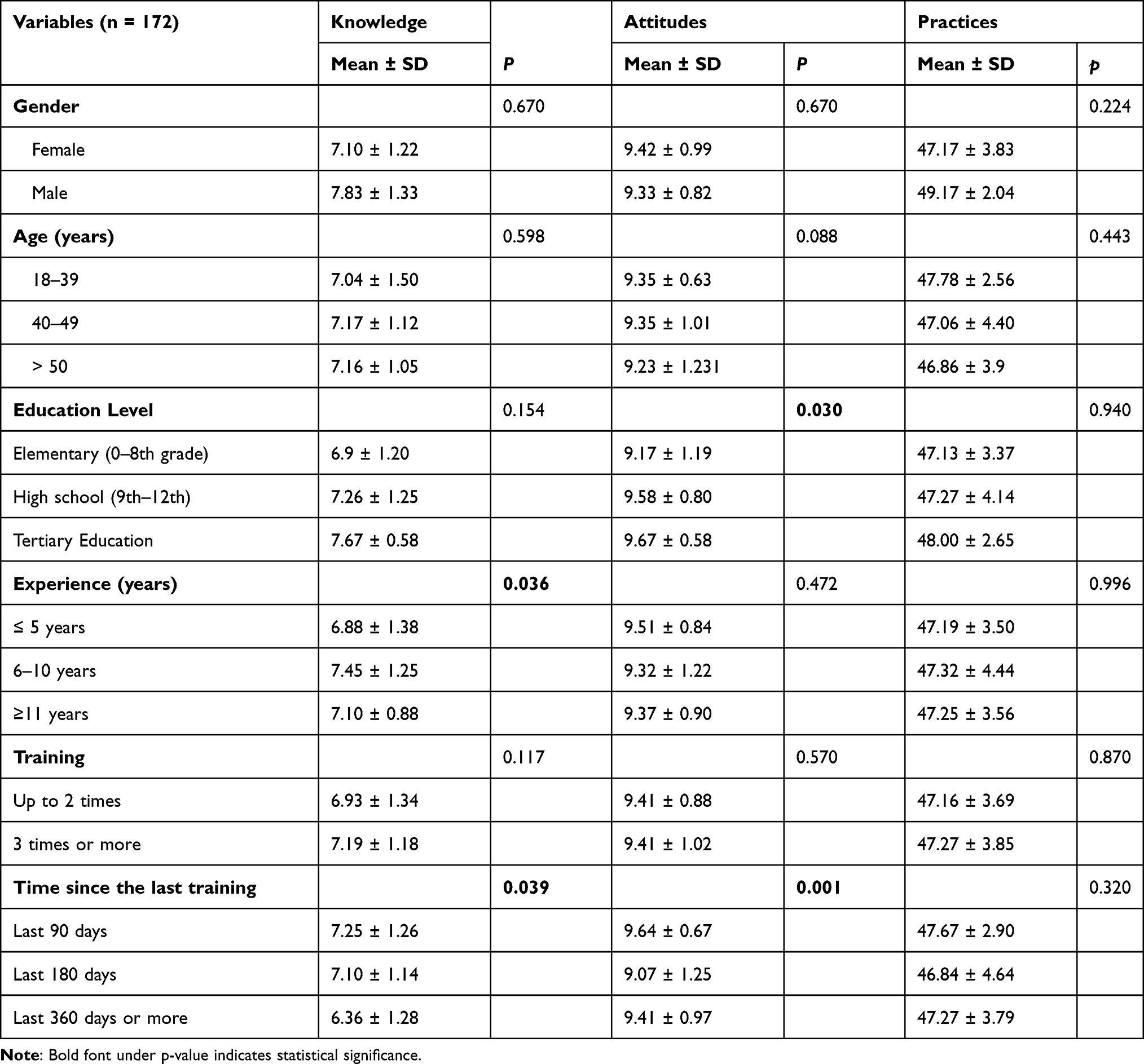 |
Table 7 Relationship Between the Scores Obtained for Knowledge, Attitudes, and Practices of Body Artists |
The model for multiple linear regression analysis was generated to determine the impact of explanatory variables (education, experience, training participation, previous training duration, knowledge, and attitudes) on KAP scores. Only variables with statistically significant findings were included in the bivariate analysis. The KAP score considered the assumption of the effect of knowledge on the change in attitudes and practices. The influence of attitudes on practices was also considered in determining the association between the variables. The F-test yielded significant findings, suggesting a good model fit, and the Durbin Watson residual autocorrelation test yielded results ranging from 1.4 to 2.6.
The multiple linear regression analysis revealed that an increase in the respondents’ experience was followed by a similar increase in their knowledge scores. However, this gain was only significant for individuals who had spent 6–10 years in the job (β: 0.56; p=0.01). The length of time that has elapsed since the last training has a substantial impact on the respondents’ knowledge of infection control. When all other variables were adjusted for, those who received training for one year (β: −0.89; p=0.01) and six months before the survey (β: −0.14; p=0.01) had lower levels of knowledge than those who had the training in the last 90 days preceding the data collection time.
Two variables, the respondents’ educational level, and their training status were found to be significantly associated with a good attitude towards infection control. Participants who had a tertiary level of education (β: 0.48; p=0.01) and those with a high school education (β: 0.41; p=0.01), had significantly higher attitude scores. Those who received training six months before the study, on the other hand, had a lower level of attitude towards infection control than those who received the training within the last 90 days (β: −0.56; p<0.001) before data collection.
The respondents’ attitude was positively associated with good infection control practices. After adjusting for other variables, it was found that a one-unit rise in the attitude score of respondents was found to increase the practice level by 86% (β: 0.86; p<0.001) (Table 8).
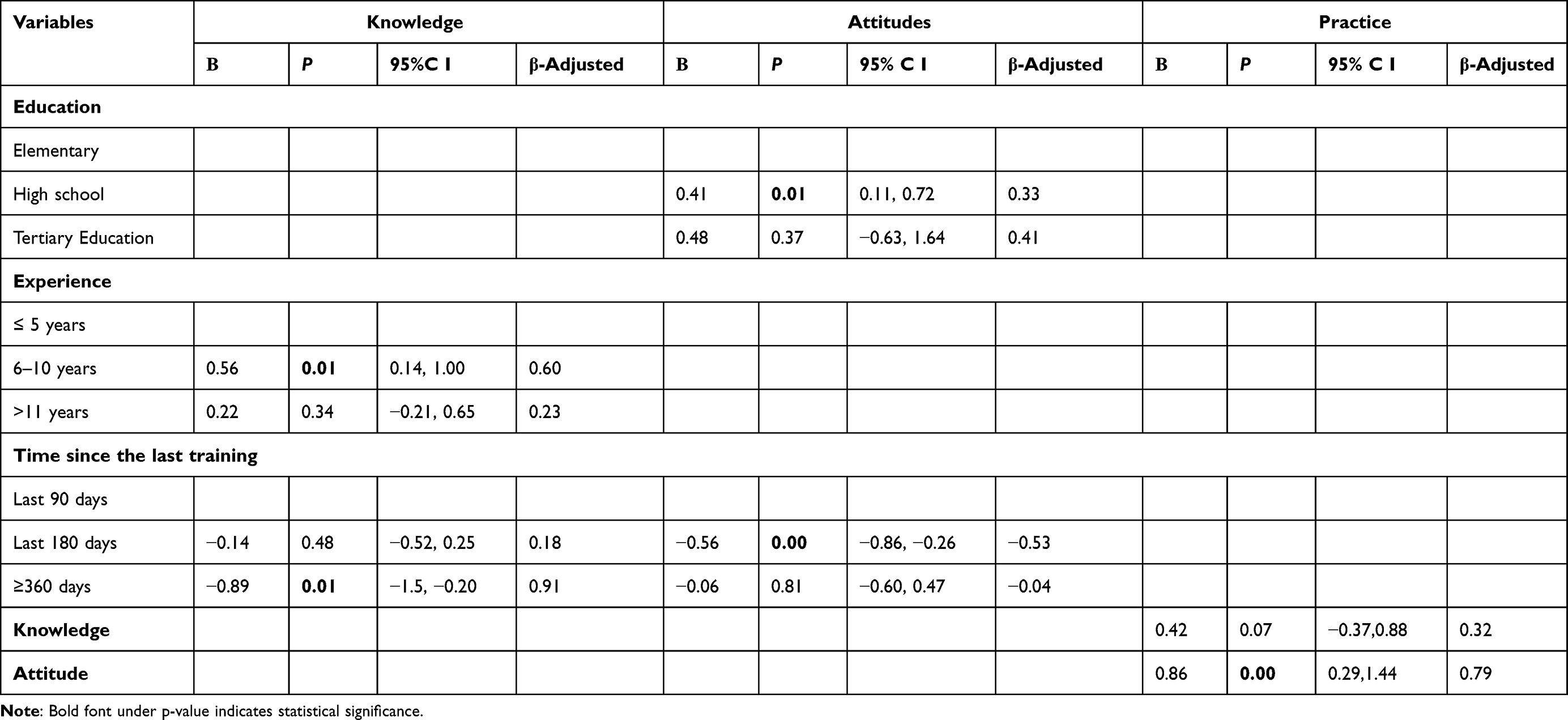 |
Table 8 Multiple Linear Regression Analysis Between Scores Obtained for Knowledge, Attitudes and Practices, and Socio-Demographic Variables |
Discussion
Tattoos and piercings have become more popular than ever before as a result of increased social acceptance. T&P parlours, on the other hand, are directly responsible for a rise in hospital visits due to both immediate and delayed problems.26 For such issues to be adequately and sustainably handled in the body art community, they must be acknowledged as a major public health concern.27 From a public health perspective, many European studies have identified critical areas for action within the body modification industry where preventative measures are required to avoid infections. These efforts include education and training, a regulated service infrastructure, client safety insurance, and an ongoing effort to improve personnel knowledge and skill.9,28 Ethiopia, on the other hand, is a country that is undergoing a unique economic transition that includes changes to its social infrastructure still lacks evidence-based infection prevention recommendations.
In any workplace, a high level of knowledge and scientific evidence is required to support safe practices.29 Many T&P artists are indeed uninformed on subjects that should be part of their professional background, according to past findings.30 A lack of anatomical knowledge, as well as tattoo and piercing aftercare, are significant challenges to safe practices.31 In the current study, respondents who received training a year before this study had lower knowledge levels than those who received some training within the last 90 days before collection for the present study.
Given the lack of federal T&P regulations and the scarcity of opportunities for body modification artists to acquire more than a basic understanding of aseptic techniques, the negative impact of inadequate new and refresher training cannot be something unexpected. With a more concerted effort among the concerned parties, seeking strategies of infusing actions into the curriculum of the limited training opportunities may serve as a remedy until further and more lasting solutions can be sought.32
Similarly, the multiple linear regression analysis revealed that an increase in experience has a positive impact on knowledge scores. Experience is a core element required for success in the workplace.33 In many occupations, after some time of practicing a discipline, a person begins to take on responsibilities. They begin to collaborate with colleagues, learn from superiors, and work in teams. The need to acquire the necessary qualifications for the job also begins to emerge in their process of practicing the discipline.34,35
Modern occupational health and safety approaches place a greater emphasis on learning and adapting than the emphasis they place on arriving at a job with all of the requisite skills.34 This makes it necessary for public health experts to commit more effort to foster knowledge-sharing by enlisting the help of veteran body artists.
In this study, attitude was defined as a way of thinking that is reflected in a person’s behavior. Attitude is influenced by situational or extrinsic circumstances. These circumstances are difficult to control. Attitude can also be influenced by dispositional or intrinsic elements such as personal skills.36 In other professions, the impact of different aspects of education and training on people’s attitudes toward infection prevention and control has been demonstrated.37–39 Likewise, in the current study, the respondents’ educational level and training status were found to be significantly associated with a positive attitude towards infection control. This can be taken as proof for education and training to help in breaking down attitudinal obstacles to safe care.
Furthermore, the respondents’ attitudes were positively associated with good infection control practices. After adjusting for other variables, a one-unit rise in the attitude score of respondents was found to increase the practice level by 86%. In psychology, the link between people’s attitudes and behaviors is widely recognized, as explained by the Theory of Planned Behaviour.40 Attitude formation, or a learned tendency to think, feel, and act in a certain way towards a specific set of items, is a crucial motivating factor for behavior adoption. People who are more concerned about T&P infections can engage in more effective protective practices. Such people’s concern about T&P can be revealed in terms of the efforts they make to understand the origin of infection, the occurrence, and frequency of severe episodes, the sterile techniques needed to minimize the extent of infection, and their understanding of the economic and health-related implications of the infection.
While there is evidence for knowledge-practice links among body modification artists,7,12 the hypothesized correlation between the level of awareness (knowledge) and practice was found to be insignificant in this study. A lack of an action learning strategy may have led to a reduced level of transfer of research and medical evidence in the study context. This has a negative impact on the diffusion of ideal infection control practices. The discrepancy might also be a symptom of a broader lack of understanding of the magnitude of public health issues surrounding infections during and after T&P in Ethiopia.
There are some limitations to this study. This is a single-site study. This may make the findings less likely to be representative of all T&P parlours in the country. Other establishments will inevitably have their characteristics that mediate barriers to optimal infection control, though those identified in this study are likely to have a resonance there as well. Furthermore, participant responses may be biased due to their desire to provide socially preferred responses. This means that some participants may be more hesitant than others to share their true experiences. There is also a likelihood of over, under, or misreporting of behavior and practices in self-reported surveys.
Future Direction for Research
A lack of sufficient resources for the research had an impact on the sample size and the areas focused on in this study. For example, it was difficult to collect data from a larger number of body artists and/or their clients who have fallen ill as a result of infectious diseases caused by the practitioners’ unsafe practices. A future study is recommended to consider embracing a larger number of body artists and their clients. Likewise, future research may also be needed to tell us the costs associated with unsafe work practice-related injuries and worker and process downtime due to the injuries caused by unsafe practice in the occupation.
Similarly, there seems to be a need for future research to identify barriers to the implementation of infection control procedures. Other potential research areas include issues related to individuals who perform cosmetic tattoos in beauty parlours and tattooists working outside of legitimate businesses. This may provide a more complete picture of the industry In addition, the current study evidenced training as an important determinant of infection control knowledge acquisition, attitude formation, and behaviour adoption (or practice) in a broader context. Future research may need to further disaggregate and investigate the type and frequency of training, the content delivered, and the effect of body artists’ knowledge on the health of the clients.
Conclusion
This is the first study in Ethiopia to examine tattooists’ and body piercers’ infection control knowledge, attitude, and practice. We hope the study has laid the foundation for a preliminary understanding of the factors related to infection control in the personal appearance service industry. Minimum standards for infection control in inking and piercing establishments are necessary. Local authorities, as well as body artists, should come together and work in unison to put in place such standards. A consistent follow-up of the quality of services offered in this industry is lacking. In addition, there are no systems in place to record complications arising from tattooing and piercing. These lacks deny us the opportunity to assess the scale and type of health-related risks. Public health inspectors, in particular, should not monitor only the facilities but also should consider tattooing and piercing procedures. However, before these steps can be taken, public health officials must become sufficiently aware of the distinct nature of tattooing and piercing. Inspectors can only properly evaluate facilities and procedures if they understand the process. As a result, educational efforts should also be directed at public health officials.
Abbreviations
ANOVA, analysis of variance COVID-19- Covid-19; T&P, tattooing or piercing; HIV, human immunodeficiency viruses; KAP, knowledge, attitude, and practices.
Data Sharing Statement
All the data supporting the findings are included in this paper.
Ethics Approval and Consent to Participate
All methods used in this study were carried out following all relevant guidelines and regulations (Declaration of Helsinki). The Ethical Review Committee at Hawassa University provided ethical clearance. The Addis Ababa City Health Bureau provided the required letter of support. The purpose of the study was fully disclosed to all participants, and all participants provided informed consent. In addition, all data gathered for the study was kept private and secure. All study participants received health education as well as occupational health and safety training on the job site.
Acknowledgments
The authors wish to thank the respondents and the data collectors for their remarkable contributions to the success of the study. All the firms that took part in the study deserve the authors’ appreciation.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Disclosure
The authors declare no competing interests in this work.
References
1. Ball J, Elsner R. Tattoos increase self-esteem among college students. Coll Stud J. 2019;53(3):293–300.
2. Wohlrab S, Stahl J, Kappeler PM. Modifying the body: motivations for getting tattooed and pierced. Body Image. 2007;4(1):87–95. doi:10.1016/j.bodyim.2006.12.001
3. Tiggemann M, Hopkins LA. Tattoos and piercings: bodily expressions of uniqueness? Body Image. 2011;8(3):245–250. doi:10.1016/j.bodyim.2011.03.007
4. Antoszewski B, Sitek A, Fijałkowska M, Kasielska A, Kruk-Jeromin J. Tattooing and body piercing-what motivates you to do it? Int J Soc Psychiatry. 2010;56(5):471–479. doi:10.1177/0020764009106253
5. Carmen RA, Guitar AE, Dillon HM. Ultimate answers to proximate questions: the evolutionary motivations behind tattoos and body piercings in popular culture. Rev Gen Psychol. 2012;16(2):134–143. doi:10.1037/a0027908
6. Balakrishnan J, Appalasamy JR. Skin infection and the global challenges: a review. Int J Pharm Pharm Sci. 2016;8:1–3.
7. Dieckmann R, Boone I, Brockmann SO, et al. The risk of bacterial infection after tattooing: a systematic review of the literature. Dtsch Ärztebl int. 2016;113(40):665. doi:10.3238/arztebl.2016.0665
8. Jafari S, Buxton JA, Afshar K, Copes R, Baharlou S. Tattooing and risk of hepatitis B: a systematic review and meta-analysis. Can J Public Health. 2012;103(3):207–212. doi:10.1007/BF03403814
9. Juszczyk GP. The risk of blood-borne infections in Poland–opportunities and threats to public health, nationwide qualitative research. Ann Agric Environ Med. 2021;28(3):469–474. doi:10.26444/aaem/124709
10. Kluger N. Cutaneous and systemic complications associated with tattooing. Presse Méd. 2016;45(6):567–576. doi:10.1016/j.lpm.2016.02.016
11. Thum CK, Biswas A. Inflammatory complications related to tattooing: a histopathological approach based on pattern analysis. Am J Dermatopathol. 2015;37(1):54–66. doi:10.1097/DAD.0b013e3182974558
12. Messahel A, Musgrove B. Infective complications of tattooing and skin piercing. J Infect Public Health. 2009;2(1):7–13. doi:10.1016/j.jiph.2009.01.006
13. Sosin M, Weissler JM, Pulcrano M, Rodriguez ED. Transcartilaginous ear piercing and infectious complications: a systematic review and critical analysis of outcomes. Laryngoscope. 2015;125(8):1827–1834. doi:10.1002/lary.25238
14. Tohme RA, Holmberg SD. Transmission of hepatitis C virus infection through tattooing and piercing: a critical review. Clin Infect Dis. 2012;54(8):1167–1178. doi:10.1093/cid/cir991
15. Lehman EJ, Huy J, Levy E, Viet SM, Mobley A, McCleery TZ. Bloodborne pathogen risk reduction activities in the body piercing and tattooing industry. Am J Infect Control. 2010;38(2):130–138. doi:10.1016/j.ajic.2009.07.008
16. Hellard M, Aitken C, Mackintosh A, Ridge A, Bowden S. Investigation of infection control practices and knowledge of hepatitis C among body-piercing practitioners. Am J Infect Control. 2003;31(4):215–220. doi:10.1067/mic.2003.61
17. Qiquan Z. The KAP theory. In: The Logic of China’s New School Reforms. Brill; 2021:38–50.
18. Quaranta A, Napoli C, Fasano F, Montagna C, Caggiano G, Montagna MT. Body piercing and tattoos: a survey on young adults’ knowledge of the risks and practices in body art. BMC Public Health. 2011;11(1):1–8.
19. Gębska Kuczerowska A, Błoński A, Kuczerowska J, Gajda R. Strengths and weaknesses in the risk management of Blood-Borne infections: qualitative research in public health. Int J Environ Res Public Health. 2020;17(18):6650. doi:10.3390/ijerph17186650
20. Gębska-Kuczerowska A, Kucharska I, Segiet-Święcicka A, Kuczerowski M, Gajda R. Disposal of waste from tattoo and beauty parlors in Poland: a survey-based analysis on epidemiological safety. Int J Environ Res Public Health. 2021;18(23):12673. doi:10.3390/ijerph182312673
21. Ethiopia Demographic and Health Survey 2016. Addis Ababa, Ethiopia: CSA and ICF; 2017.
22. Oberdorfer A, Wiggers JH, Bowman J, Lecathelinais C. Infection control practices among tattooists and body piercers in Sydney, Australia. Am J Infect Control. 2003;31(8):447–456. doi:10.1016/S0196-6553(03)00082-8
23. Raymond MJ, Pirie PL, Halcón LL. Infection control among professional tattooists in Minneapolis and St Paul, MN. Public Health Rep. 2001;116(3):249. doi:10.1016/S0033-3549(04)50040-7
24. Hellard ME, Aitken C, Hocking J. Tattooing in prisons—not such a pretty picture. Am J Infect Control. 2007;35(7):477–480. doi:10.1016/j.ajic.2006.08.002
25. Kafle SC. Correlation and regression analysis using SPSS. OCEM J Manag Tech Soc Sci. 2019;1(1):126–132.
26. Urdang M, Mallek JT, Mallon WK. Tattoos and piercings: a review for the emergency physician. West J Emerg Med. 2011;12(4):393. doi:10.5811/westjem.2011.4.2268
27. Prüss-Ustün A, Bartram J, Clasen T, Colford JM, Cumming O, Curtis V. Burden of disease from inadequate water, sanitation and hygiene in low-and middle-income settings: a retrospective analysis of data from 145 countries. Trop Med Int Health. 2014;19(8):894–905. doi:10.1111/tmi.12329
28. Gębska-Kuczerowska A, Kucharska I, Segiet-Święcicka A, Kuczerowski M, Gajda R. Assessment of epidemiological safety in the cosmetic service industry in Poland: a cross-sectional questionnaire study. Int J Environ Res Public Health. 2021;18(11):5661. doi:10.3390/ijerph18115661
29. John A, Tomas ME, Cadnum JL, et al. Are health care personnel trained incorrect use of personal protective equipment? Am J Infect Control. 2016;44(7):840–842. doi:10.1016/j.ajic.2016.03.031
30. Covello F, Salerno C, Giovannini V, Corridore D, Ottolenghi L, Vozza I. Piercing and oral health: a study on the knowledge of risks and complications. Int J Environ Res Public Health. 2020;17(2):613. doi:10.3390/ijerph17020613
31. Vozza I, Fusco F, Bove E, Ripari F, Corridore D, Ottolenghi L. Awareness of risks related to oral piercing in Italian piercers. Pilot study in Lazio Region. Ann Stomatol. 2014;5(4):128.
32. Begossi A. Local knowledge and training towards management. Environ Dev Sustain. 2008;10(5):591–603. doi:10.1007/s10668-008-9150-7
33. Gyekye SA. Occupational safety management: the role of causal attribution. Int J Psychol. 2010;45(6):405–416. doi:10.1080/00207594.2010.501337
34. Wareing M. Being a worker and a learner. BJHCA. 2016;10(11):554–561. doi:10.12968/bjha.2016.10.11.554
35. Ayim Gyekye S, Salminen S. Organizational safety climate and work experience. Int J Occup Saf Ergon. 2010;16(4):431–443. doi:10.1080/10803548.2010.11076856
36. Schwarz N. Attitude construction: evaluation in context. Soc Cogn. 2007;25(5):638–656. doi:10.1521/soco.2007.25.5.638
37. Ibrahim AA, Elshafie SS. Knowledge, awareness, and attitude regarding infection prevention and control among medical students: a call for educational intervention. Adv Med Educ Pract. 2016;7:505. doi:10.2147/AMEP.S109830
38. Ogoina D, Pondei K, Adetunji B, Chima G, Isichei C, Gidado S. Knowledge, attitude, and practice of standard precautions of infection control by hospital workers in two tertiary hospitals in Nigeria. J Infect Prev. 2015;16(1):16–22. doi:10.1177/1757177414558957
39. Khanghahi BM, Jamali Z, Azar FP, Behzad MN, Azami-Aghdash S. Knowledge, attitude, practice, and status of infection control among Iranian dentists and dental students: a systematic review. J Dent Res Dent Clin Dent Prospects. 2013;7(2):55. doi:10.5681/joddd.2013.010
40. De Pretto L, Acreman S, Ashfold MJ, Mohankumar SK, Campos-Arceiz A. the link between knowledge, attitudes, and practices concerning atmospheric haze pollution in Peninsular Malaysia. PLoS One. 2015;10(12):e0143655–e. doi:10.1371/journal.pone.0143655
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.