Back to Journals » Therapeutics and Clinical Risk Management » Volume 21
A Stratified Surgical Approach for Convergence Insufficiency-Type Exotropia Based on Near Deviation Magnitude: A Retrospective Cohort Study of Motor and Sensory Outcomes
Received 21 July 2025
Accepted for publication 27 October 2025
Published 7 November 2025 Volume 2025:21 Pages 1559—1567
DOI https://doi.org/10.2147/TCRM.S550542
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Garry Walsh
Feng Dong, Ping Liu, Yanyan Wang
Department of Strabismus and Pediatric Ophthalmology, Eye Good Hospital, Wuhan, People’s Republic of China
Correspondence: Feng Dong, Department of Strabismus and Pediatric Ophthalmology, Eye Good Hospital, No. 8 Longyang Avenue, Longyang Street, Hanyang District, Wuhan, Hubei, 430051, People’s Republic of China, Tel +86-027-85551616, Email [email protected]
Objective: To evaluate the efficacy and safety of a stratified surgical strategy for convergence insufficiency-type exotropia (CIX(T)) tailored to the magnitude of near deviation, with a primary outcome of postoperative motor success (orthophoria) and a secondary outcome of stereopsis improvement.
Methods: This retrospective cohort study included 85 CIX(T) patients (near deviation ≥ distance deviation by 15Δ) treated between July 2015 and June 2022. Patients were stratified into three groups based on near deviation magnitude. Group 1 (n=15, < 30Δ) underwent unilateral medial rectus resection; Group 2 (n=38, 30– 80Δ) received unilateral lateral rectus recession combined with medial rectus resection; Group 3 (n=32, 85– 130Δ) underwent bilateral lateral rectus recession plus unilateral medial rectus resection. Ocular alignment (prism cover test) and stereopsis (Titmus test) were assessed preoperatively, at 1 week (short-term), and 3 months (intermediate-term) postoperatively.
Results: Baseline characteristics were comparable across groups, except for the stratification variable of near deviation. At the 3-month follow-up, motor success was achieved in 20.0% of Group 1, 89.5% of Group 2, and 87.5% of Group 3. Group 1 showed a high rate of undercorrection (80.0%), whereas Groups 2 and 3 demonstrated stable alignment with minimal undercorrection (10.5% and 9.4%, respectively). Stereopsis scores significantly improved from preoperative levels in Group 2 (P< 0.001) and Group 3 (P< 0.001), but regressed in Group 1 (P> 0.05). A planned slight initial overcorrection (10– 15Δ) at distance was significantly correlated with better intermediate-term alignment (r = 0.68, 95% CI: 0.51 to 0.80, P< 0.001).
Conclusion: These findings support a stratified surgical approach for CIX(T) based on near deviation magnitude. While combined recession-resection procedures are effective for moderate-to-large angle deviations, unilateral medial rectus resection for small-angle CIX(T) resulted in high rates of undercorrection. This suggests that the surgical plan for small-angle CIX(T) may require more aggressive dosages or alternative strategies.
Keywords: convergence insufficiency-type exotropia, surgical treatment, retrospective study, near deviation, binocular vision, stratified medicine
Introduction
Convergence insufficiency-type exotropia (CIX(T)) is a distinct subtype of intermittent exotropia, primarily characterized by a near deviation (at 33 cm) that is at least 15 prism diopters (Δ) greater than the distance deviation (at 6 m).1 It is often associated with a reduced accommodative convergence to accommodation (AC/A) ratio and can lead to a progressive deterioration of binocular vision.2,3 Patients, particularly adolescents and young adults, commonly report asthenopic symptoms such as reading fatigue, transient diplopia, and difficulty concentrating on near tasks.4 If left untreated, CIX(T) can progress from an intermittent to a constant exotropia, diminishing asthenopic complaints but severely compromising stereopsis.5 While the prevalence of intermittent exotropia in pediatric populations is well-documented,6 the specific prevalence of the CIX(T) subtype is estimated to be between 6.4% and 19.5% of all exotropia cases, highlighting it as a significant clinical challenge.7,8 Recent studies affirm that intermittent exotropia (IXT) remains the most common exotropia subtype globally,9 with the convergence insufficiency type representing a substantial portion of these cases in clinical cohorts,8 reinforcing its impact on management strategies.
The surgical management of CIX(T) is notoriously complex due to the significant disparity between near and distance deviation, which creates a high risk of postoperative undercorrection at near or overcorrection (consecutive esotropia) at distance.10 Historically, surgical plans based solely on the distance deviation yielded poor motor outcomes, with success rates as low as 18% to 50%.1,2,5 More contemporary strategies, such as basing surgical amounts on the average of near and distance deviations or solely on the near deviation, have improved success rates to approximately 69% to 77%.11,12 Despite these advances, a consensus on the optimal surgical approach remains elusive, particularly for patients at the extremes of the deviation spectrum.
Significant gaps persist in the literature. First, there is a lack of evidence-based guidelines for small-angle CIX(T) (eg, near deviation <30Δ), where single-muscle procedures often result in undercorrection, as observed in our cohort. Second, the surgical management of very large-angle CIX(T) (eg, >85Δ) is not well-documented. Third, while motor alignment is often the primary outcome, intermediate-term binocular vision recovery across these different deviation ranges remains understudied. This study aims to address these gaps by evaluating the outcomes of a stratified surgical strategy tailored to the magnitude of near deviation. We categorized patients into small (<30Δ), moderate (30–80Δ), and large (85–130Δ) angle groups and assessed both motor alignment and stereopsis at 1 week and 3 months postoperatively. By analyzing the efficacy of deviation-specific procedures, we seek to provide a preliminary framework for optimizing surgical planning, enhancing intermediate-term stability, and minimizing adverse outcomes.
Materials and Methods
Study Design and Participants
A retrospective cohort study was conducted on patients diagnosed with CIX(T) who underwent surgery at Eye Good Hospital between July 2015 and June 2022. The study protocol was approved by the Institutional Review Board and Ethics Committee of Eye Good Hospital (S2015-03B-02) and adhered to the tenets of the Declaration of Helsinki. Written informed consent was obtained from all adult participants or from the parents or legal guardians of pediatric patients. The study followed the STROBE reporting guidelines.13 A total of 120 patient records were initially screened for eligibility. Of these, 85 patients met the inclusion criteria and were included in the final analysis. The patient selection process is detailed in the study flowchart (Figure 1).
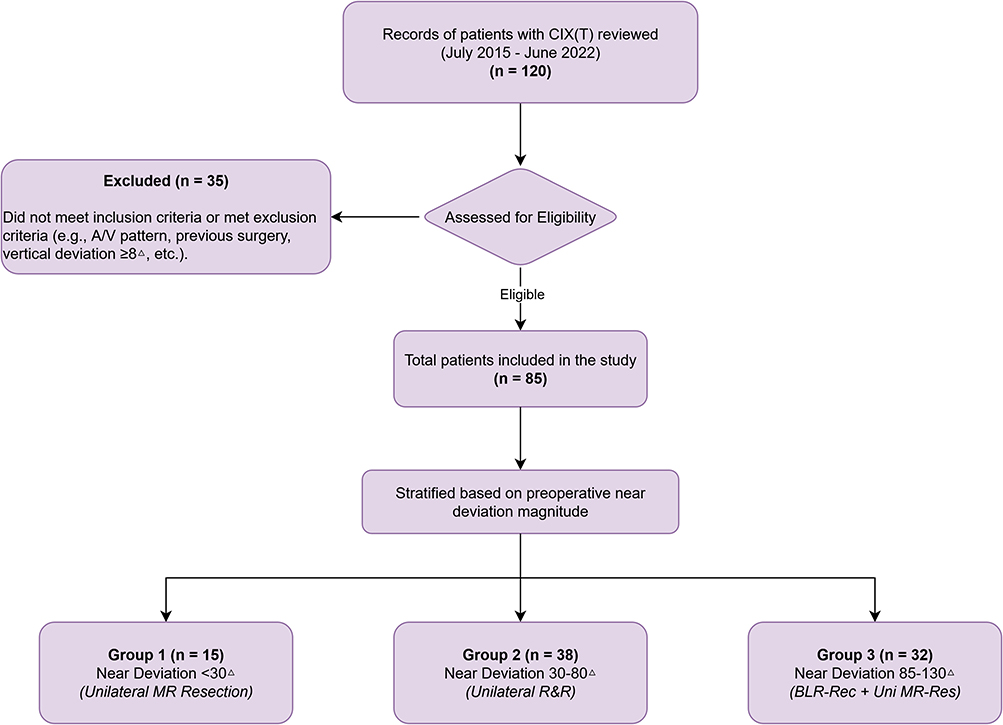 |
Figure 1 STROBE flowchart of the patient selection process. The diagram illustrates the screening of 120 patient records, exclusion of 35 patients, and stratification of the final 85 eligible patients into three study groups based on preoperative near deviation magnitude. |
Inclusion and Exclusion Criteria
Inclusion criteria were: (1) age ≥ 3 years; (2) diagnosis of CIX(T), defined as an exodeviation at near (33 cm) exceeding the distance deviation (6 m) by ≥15Δ, with a distance deviation of at least 10Δ; (3) ability to cooperate with ocular motility examinations; (4) best-corrected visual acuity (BCVA) ≥ 0.6 in each eye, with an inter-ocular difference of ≤2 lines; and (5) no significant preoperative horizontal eye movement limitations. Exclusion criteria were: (1) A- or V-pattern strabismus; (2) significant vertical deviation (≥8Δ); (3) dense amblyopia; (4) history of previous strabismus surgery, ocular trauma, or paretic strabismus; (5) evidence of neurological abnormalities (eg, convergence spasm, supranuclear palsies) confirmed through comprehensive neurological and ophthalmological examination, including full duction and version testing.
Preoperative Assessment and Surgical Strategy
All patients underwent a comprehensive ophthalmic examination, including visual acuity, slit-lamp biomicroscopy, and fundus examination. Cycloplegic refraction was performed for all patients under 14 years old (1% atropine for age <6; 0.5% compound tropicamide for age 6–14). Ocular alignment was measured using the prism and alternate cover test (PACT) with accommodative targets at both near (33 cm) and distance (6 m). All measurements were performed by two experienced orthoptists and repeated three times to ensure reliability. For large deviations (≥85Δ), a stepwise prism superposition method was used to ensure accuracy. Stereopsis was assessed using the Titmus stereo test (at 33 cm). The Titmus stereo test was used for its consistent availability and standardized use in our clinic throughout the study period, allowing for uniform longitudinal assessment.
Patients were stratified into three groups based on their preoperative near deviation magnitude. The surgical procedure was selected according to a predefined institutional protocol tailored to the deviation size. The thresholds, including the discrete gap between Group 2 (30–80Δ) and Group 3 (85–130Δ), were based on established institutional protocols designed to differentiate standard versus extensive surgical interventions based on clinical experience with deviation stability. The 3-month follow-up was chosen as the primary endpoint, as this period typically reflects the stabilization of ocular alignment before significant long-term drift may occur.10 For unilateral or asymmetric procedures (Groups 2 and 3), surgery was preferentially performed on the non-dominant eye, as determined by the hole-in-the-card test.
- Group 1 (n=15, near deviation <30Δ): Unilateral medial rectus resection (MR-Res). Surgical dosage was based on the near deviation, with a target correction of approximately 10Δ per 1mm of resection.14
- Group 2 (n=38, near deviation 30–80Δ): Unilateral lateral rectus recession (LR-Rec) combined with medial rectus resection (R&R). The surgical dosage was calculated based on the near deviation, with the recession and resection amounts adjusted to balance near and distance alignment.
- Group 3 (n=32, near deviation 85–130Δ): Bilateral lateral rectus recession (BLR-Rec) combined with unilateral medial rectus resection (MR-Res). This three-muscle surgery was designed to address the very large near angle without inducing significant distance overcorrection.15
Outcome Measures and Efficacy Evaluation
The primary outcome was motor success at the 3-month postoperative follow-up, defined as orthophoria (a residual horizontal deviation of ≤8Δ at both near and distance). Deviations >8Δ were classified as undercorrection (residual exotropia) or overcorrection (consecutive esotropia). The secondary outcome was the change in binocular vision, assessed by stereopsis. For analysis, Titmus stereopsis results were converted to a 4-point ordinal scale: 0 points for no stereopsis (>800״); 1 point for gross stereopsis (400״–800״); 2 points for moderate stereopsis (140״–200״); and 3 points for fine stereopsis (≤100״).
Statistical Analysis
Data were analyzed using SPSS version 26.0 (IBM Corp., Armonk, NY, USA). Baseline characteristics between groups were compared using one-way ANOVA for continuous variables and the chi-square (χ2) test for categorical variables. Postoperative motor outcomes (orthophoria rates) were compared using the χ2-test or Fisher’s exact test. For post-hoc pairwise comparisons of categorical outcomes between the three groups, a Bonferroni correction was applied, with statistical significance set at P<0.017. Pre- and postoperative stereopsis scores and deviation angles within each group were compared using paired t-tests or Wilcoxon signed-rank tests, depending on data distribution as assessed by the Shapiro–Wilk test. Effect sizes for significant changes in stereopsis were calculated using Cohen’s d. The correlation between short-term overcorrection and intermediate-term deviation was assessed using Pearson’s correlation coefficient. A p-value of <0.05 was considered statistically significant for all tests, unless otherwise adjusted.
Results
Baseline Characteristics
The study included 85 patients (47 male, 38 female) with a mean age of 13.2 ± 2.3 years (range, 3–45 years). The baseline demographic and clinical characteristics of the three groups are presented in Table 1. There were no statistically significant differences among the groups in terms of age, gender distribution, preoperative distance deviation, or duration of symptoms (all P>0.05). As expected, the preoperative near deviation and near-distance disparity were significantly different across the groups (P<0.001), consistent with the stratification criteria.
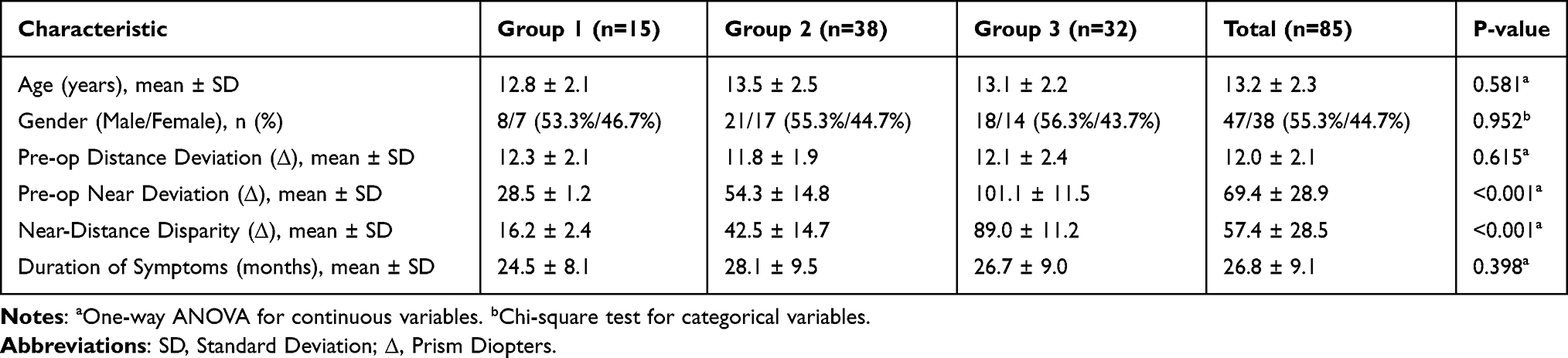 |
Table 1 Baseline Demographic and Clinical Characteristics of Patients |
Postoperative Ocular Alignment
Postoperative motor outcomes at the short-term (1 week) and intermediate-term (3 months) follow-ups are summarized in Table 2 and visualized in Figure 2. At the 1-week follow-up, the orthophoria rates were 73.3% in Group 1, 84.2% in Group 2, and 81.3% in Group 3. However, at the 3-month follow-up, the orthophoria rate in Group 1 dropped sharply to 20.0%, with 80.0% of patients developing significant undercorrection. In contrast, Groups 2 and 3 maintained high success rates of 89.5% and 87.5%, respectively. The intermediate-term undercorrection rates in these groups were substantially lower (10.5% and 9.4%).
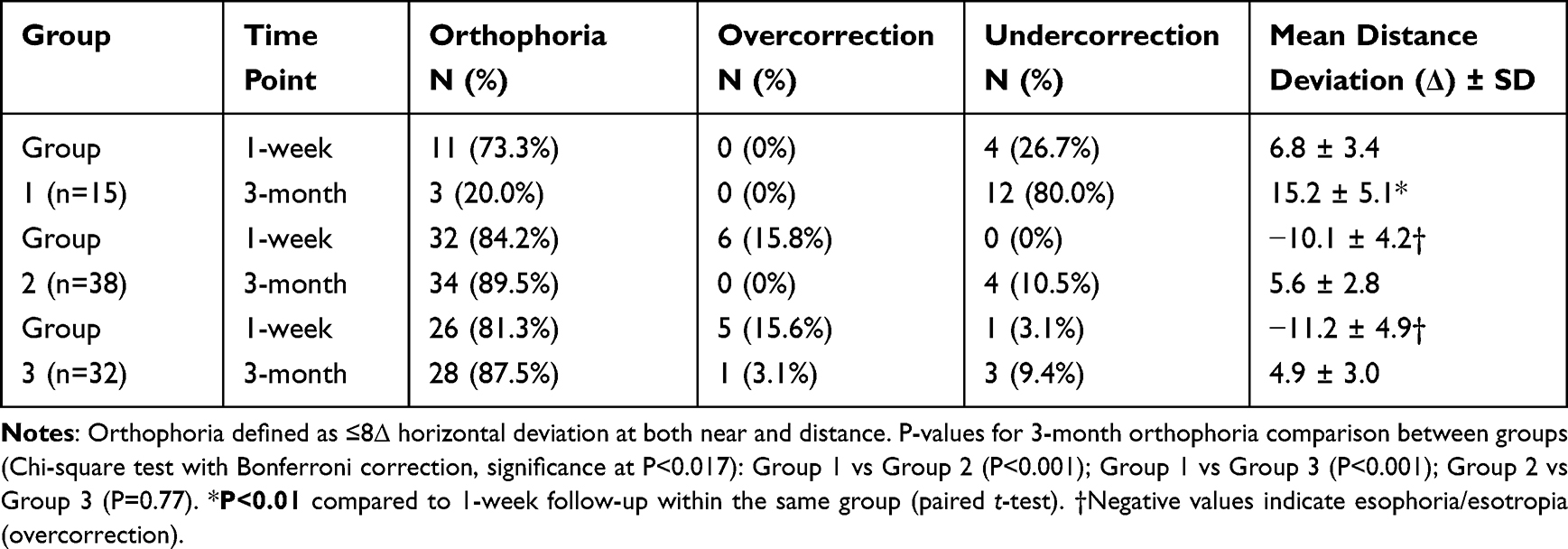 |
Table 2 Postoperative Ocular Alignment Outcomes |
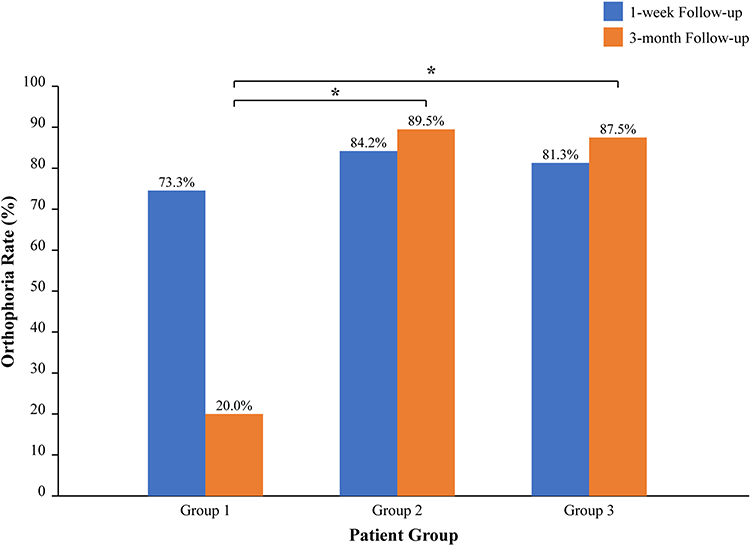 |
Figure 2 Comparison of motor success (orthophoria) rates at 1-week and 3-month postoperative follow-ups across the three surgical groups. Group 1 shows a significant decline in success, whereas Groups 2 and 3 maintain high success rates (*P<0.001 vs Group 1 at 3 months). |
Postoperative Binocular Vision Function
Changes in stereopsis are presented in Table 3 and Figure 3. In Group 1, there was no significant change in stereopsis from preoperative levels to the 3-month follow-up (mean score: 2.00 vs 1.80; P=0.334), mirroring the motor outcome regression. In stark contrast, both Group 2 and Group 3 demonstrated highly significant and sustained improvements in stereopsis at the 3-month follow-up compared to preoperative levels (Group 2: pre-op vs 3-month mean score: 0.92 vs 1.53; P<0.001, Cohen’s d=0.88, indicating a large effect size; Group 3: 0.56 vs 1.68; P<0.001, Cohen’s d=1.58, indicating a very large effect size). Furthermore, stereopsis continued to improve from the short-term to the intermediate-term follow-up in these two groups (P<0.05).
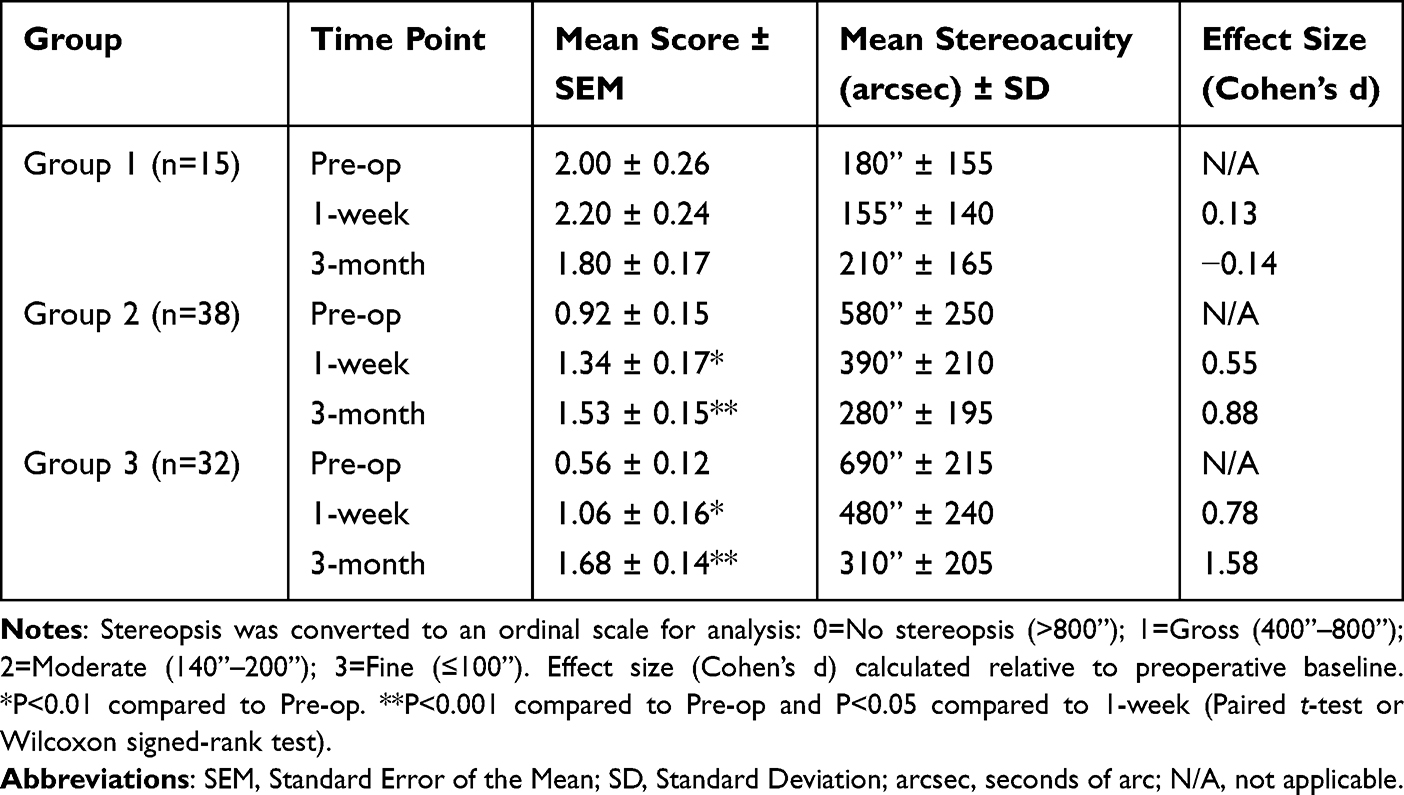 |
Table 3 Preoperative and Postoperative Binocular Vision Function (Stereopsis) |
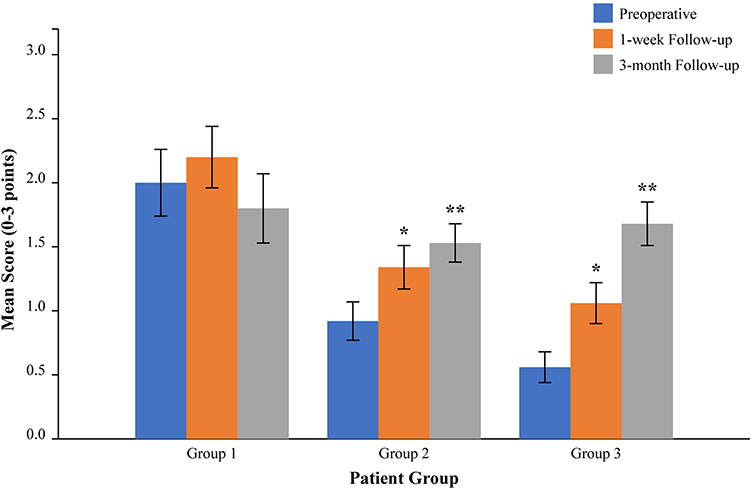 |
Figure 3 Mean stereopsis scores (on a 0–3 point scale) at preoperative, 1-week, and 3-month time points. Groups 2 and 3 show significant and sustained improvement, while Group 1 shows regression by the 3-month follow-up. Error bars represent SEM. (*P<0.01 vs Pre-op; **P<0.001 vs Pre-op). |
Correlation and Dose-Response Analysis
To investigate factors associated with stable motor outcomes, a correlation analysis was performed across all patients. This revealed a significant positive correlation between the magnitude of distance deviation at the 1-week follow-up and the final deviation at 3 months (r = 0.68, 95% CI: 0.51 to 0.80, P<0.001), as shown in Supplementary Figure S1. This suggests that achieving a planned initial overcorrection (represented by negative values) is associated with a higher likelihood of intermediate-term orthophoria. The surgical dosages applied and the corresponding corrective effects are detailed in Table 4. The dose-response data shows that in Group 1, the mean medial rectus resection was insufficient for stable correction, whereas the combined procedures in Groups 2 and 3 provided a more robust and lasting effect on the near deviation.
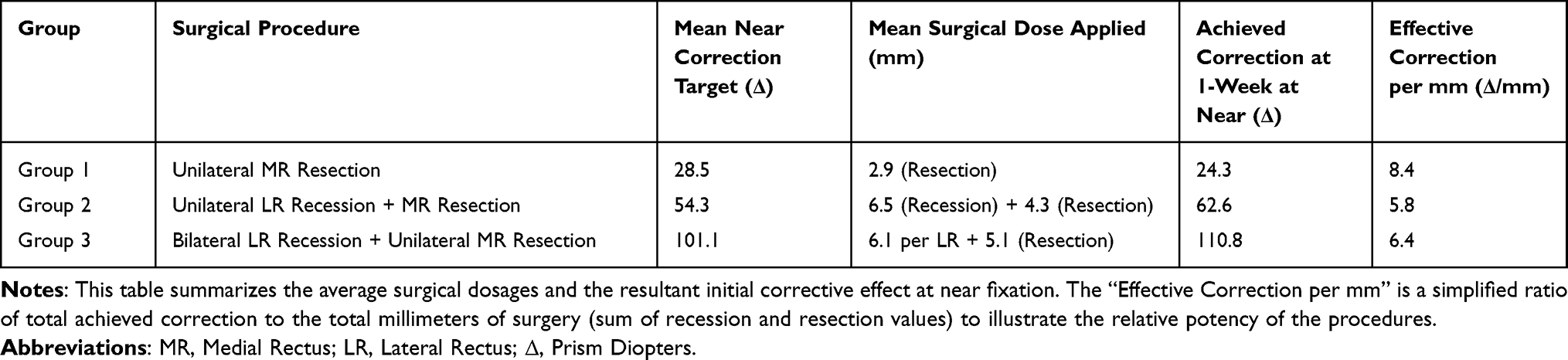 |
Table 4 Surgical Dose-Response Summary by Group |
Discussion
This study evaluated a stratified surgical strategy for CIX(T) based on the magnitude of near deviation. Our findings indicate that while this tailored approach appears effective for moderate- and large-angle CIX(T), the management of small-angle cases remains a significant clinical challenge. The core issue in CIX(T) management is to adequately correct the large near deviation without causing a consecutive esotropia at distance.10 Our stratified protocol was designed to address this dilemma directly.
For patients with small-angle CIX(T) (<30Δ), our use of a single medial rectus resection resulted in an 80% undercorrection rate at 3 months. This is consistent with previous reports highlighting the inadequacy of conservative, single-muscle surgery for this condition.16,17 The high regression rate may be multifactorial. First, the surgical dosage, while based on a standard nomogram, may have been insufficient to counteract the underlying convergence weakness and any progressive nature of the disease.14,18 Our dose-response data (Table 4) supports this, showing a less potent effect than desired. An alternative or adjunctive approach, such as combining the resection with postoperative vision therapy, might be necessary to achieve stable long-term outcomes.19
In contrast, patients with moderate (30–80Δ) and large (85–130Δ) angle CIX(T) who received combined recession-resection procedures (R&R or three-muscle surgery) achieved excellent motor success (around 90%) and significant, sustained improvement in stereopsis. This success is likely attributable to two factors. First, the combination of weakening an antagonist (lateral rectus) and strengthening an agonist (medial rectus) creates a more powerful and balanced corrective effect.15,20 Second, our strategy of aiming for a slight initial overcorrection of 10–15Δ at distance appears to be a key factor for intermediate-term stability, as demonstrated by our correlation analysis. This controlled overcorrection is a widely accepted strategy designed to compensate for the natural tendency of exotropia to drift outward over time, thereby improving long-term motor stability.21
The management of the very large deviation group (Group 3) is noteworthy. A three-muscle surgery (bilateral LR recession plus unilateral MR resection) proved highly effective. This approach provides a powerful effect at near by addressing three horizontal recti, while the symmetric recession of the lateral recti helps to minimize the risk of significant ductional imbalances.15 The excellent outcomes in this unique cohort provide valuable evidence for managing this challenging clinical scenario.
Improving long-term binocular vision outcomes remains a central goal. Our results clearly link stable motor alignment with stereopsis recovery. The failure to improve stereopsis in Group 1 was directly tied to motor regression. Conversely, the stable alignment in Groups 2 and 3 facilitated a progressive recovery of stereopsis. This underscores that achieving and maintaining orthophoria is a prerequisite for functional success. However, optimizing these outcomes likely requires a comprehensive approach that extends beyond surgery alone. While postoperative vision therapy was recommended, adherence was not systematically tracked in this retrospective analysis, and its potential contribution to the observed outcomes could not be measured.19,22
This study has several limitations inherent to its retrospective design, including susceptibility to selection bias, information bias from reliance on medical records, and unmeasured confounding variables. Second, the sample size, particularly in the small-angle group, is limited, which reduces the statistical power and generalizability of the findings. Third, the 3-month follow-up period is intermediate-term; longer-term studies are needed to assess the true stability of these surgical outcomes. Fourth, the wide age range of participants introduces potential confounding from factors like accommodative ability. Furthermore, the reliance on the Titmus test, which can be susceptible to monocular cues, may not reflect the full spectrum of binocular sensory status; future studies could benefit from including random-dot stereotests. Finally, this was not a comparative study; we evaluated a single, stratified protocol, and therefore cannot make direct claims about the superiority of one surgical technique over another. Future prospective, randomized controlled trials are needed.
Conclusion
This study provides evidence supporting a stratified surgical strategy for CIX(T) based on the magnitude of near deviation. For moderate-to-large angle deviations (≥30Δ), combined recession-resection procedures, aimed at achieving a slight initial overcorrection, yield excellent motor and sensory outcomes at 3 months. However, for small-angle CIX(T), unilateral medial rectus resection as performed in our cohort appears an insufficient primary procedure, leading to a high rate of undercorrection. This highlights an urgent need to refine surgical strategies for this specific subgroup, potentially through more aggressive surgical dosages or the integration of non-surgical therapies.
Data Sharing Statement
The data generated and analyzed during this study are included in this published article.
Ethics Approval and Consent to Participate
The study protocol was approved by the Ethics Committee of Eye Good Hospital (S2015-03B-02). The study was performed in accordance with the Declaration of Helsinki, and written informed consent was obtained from all participants or their legal guardians.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
No funding was received for this study.
Disclosure
The authors declare that they have no competing interests in this work.
References
1. Yang HK, Hwang J-M. Surgical outcomes in convergence insufficiency-type exotropia. Ophthalmology. 2011;118(8):1512–1517. doi:10.1016/j.ophtha.2011.01.004
2. Wang B, Wang L, Wang Q, Ren M. Comparison of different surgery procedures for convergence insufficiency-type intermittent exotropia in children. Br J Ophthalmol. 2014;98(10):1409–1413. doi:10.1136/bjophthalmol-2013-304442
3. Goseki T, Ishikawa H. The prevalence and types of strabismus, and average of stereopsis in Japanese adults. Japan J Ophthalmol. 2017;61(3):280–285. doi:10.1007/s10384-017-0505-1
4. Lavrich JB. Intermittent exotropia: continued controversies and current management. Curr Opinion Ophthalmol. 2015;26(5):375–381. doi:10.1097/ICU.0000000000000188
5. Choi M, Hyung S, Hwang J. Unilateral recession–resection in children with exotropia of the convergence insufficiency type. Eye. 2007;21(3):344–347. doi:10.1038/sj.eye.6702197
6. Wang Y, Zhao A, Zhang X, et al. Prevalence of strabismus among preschool children in eastern China and comparison at a 5-year interval: a population-based cross-sectional study. BMJ open. 2021;11(10):e055112. doi:10.1136/bmjopen-2021-055112
7. Stepanets IR, Kulikov AN, Koskin SA, Kovalevskaya IS. Intermittent exotropia with convergence insufficiency—diagnostics, methods of invasive treatment. Ophthalmol Rep. 2022;15(4):75–83. doi:10.17816/OV112480
8. Jung JW, Lee SY. A comparison of the clinical characteristics of intermittent exotropia in children and adults. Korean J Ophthalmol. 2010;24(2):96–100. doi:10.3341/kjo.2010.24.2.96
9. Chen H, Jiang X, Liu W, et al. Quantitative interocular suppression in children with intermittent exotropia. Front Neurosci. 2023;17:1204061. doi:10.3389/fnins.2023.1204061
10. Chougule P, Kekunnaya R. Surgical management of intermittent exotropia: do we have an answer for all? BMJ Open Ophthalmol. 2019;4(1):e000243. doi:10.1136/bmjophth-2018-000243
11. Lee H-J, Yu YS, Kim S-J. Long-term surgical outcomes of patients with consecutive exotropia. Graefes Arch Clin Exp Ophthalmol. 2019;257(5):1037–1044. doi:10.1007/s00417-019-04293-3
12. Jeon H, Choi H-Y. Long-term surgical outcomes of basic-type exotropia in patients with hyperopia. BMC Ophthalmol. 2023;23(1):187. doi:10.1186/s12886-023-02909-1
13. von Elm E, Altman DG, Egger M, Pocock SJ, Gøtzsche PC, Vandenbroucke JP. Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement: guidelines for reporting observational studies. BMJ. 2007;335(7624):806–808. doi:10.1136/bmj.39335.541782.AD
14. Kim KH, Lee JY. Surgical outcomes of modified medial rectus resections in recurrent intermittent exotropia. J Korean Ophthalmol Soc. 2019;60(11):1098–1104. doi:10.3341/jkos.2019.60.11.1098
15. Mattout HK, Fouda SM, El-Haig WM. Botulinum toxin augmented bilateral lateral rectus recession versus three muscles surgery in large-angle intermittent exotropia. Int J Ophthalmol. 2022;15(10):1665–1670. doi:10.18240/ijo.2022.10.15
16. Chun BY, Oh JH, Choi HJ. Comparison of surgical outcomes of slanted procedure for exotropia with convergence insufficiency according to their response to preoperative monocular occlusion. Sci Rep. 2020;10(1):7261. doi:10.1038/s41598-020-64251-6
17. Fry MC, Pineles S, Velez FG. Treatment of convergence insufficiency exotropia in adults using a selective muscle fiber surgery algorithm. CLEVER Clin Experi Vision Eye Res. 2018;1(2):6. doi:10.15713/ins.clever.13
18. Lee S, Lee D, Kim SY. Correlation between frisby-davis distance stereoacuity scores and long-term surgical outcomes in intermittent exotropia. J Korean Ophthalmol Soc. 2022;63(6):535–541. doi:10.3341/jkos.2022.63.6.535
19. Zhao G, Fu J, Qi Y, Wang Y, Wei W. Six-month binocular stereopsis recovery and its influencing factors in children with intermittent exotropia. BMC Ophthalmol. 2024;24(1):139. doi:10.1186/s12886-024-03412-x
20. Choi YS, Chun BY. Comparison of surgical outcomes of two-muscle surgery in children with large-angle intermittent exotropia. J Korean Ophthalmol Soc. 2022;63(10):859–864. doi:10.3341/jkos.2022.63.10.859
21. Kim S, Ha SG, Suh YW, Kim SH. Clinical factors affecting the rate of exodrift after surgery in patients with basic intermittent exotropia. Sci Rep. 2021;11(1):6484. doi:10.1038/s41598-021-86004-9
22. Zhang H, Yang SH, Chen T, et al. The effect of virtual reality technology in children after surgery for concomitant strabismus. Indian J Ophthalmol. 2023;71(2):625–630. doi:10.4103/ijo.IJO_1505_22
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.