Back to Journals » International Medical Case Reports Journal » Volume 17
A Sleeping Giant: Late HBV Reactivation After Rituximab-Based Chemotherapy Despite Correct Prophylaxis
Authors Nowicka AA ![]() , Szymanek-Pasternak A, Janocha-Litwin J
, Szymanek-Pasternak A, Janocha-Litwin J ![]() , Simon K
, Simon K
Received 20 September 2024
Accepted for publication 4 December 2024
Published 21 December 2024 Volume 2024:17 Pages 1063—1067
DOI https://doi.org/10.2147/IMCRJ.S495506
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Xudong Zhu
Anna A Nowicka,1– 3 Anna Szymanek-Pasternak,1,2 Justyna Janocha-Litwin,1,2,4 Krzysztof Simon1,2
1Clinical Department of Infectious Diseases and Hepatology, Wroclaw Medical University, Wroclaw, Poland; 2First Department of Infectious Diseases, J. Gromkowski Specialistic Regional Hospital, Wroclaw, Poland; 3Infermedica Sp. z o. o., Wrocław, Poland; 4Novum Clinic, sp. z o. o., Wrocław, Poland
Correspondence: Anna A Nowicka, Department of Infectious Diseases and Hepatology, Wroclaw Medical University, Koszarowa 5, Wroclaw, 51-149, Poland, Email [email protected]; [email protected]
Abstract: Hepatitis B virus (HBV) reactivation is a recognized complication of long-term immunosuppressive or cytotoxic therapy, typically occurring during immunosuppression or within a few months after treatment. To mitigate this risk, hepatological societies recommend the use of nucleos(t)ide analogues (NA) for HBV reactivation prophylaxis, along with post-treatment monitoring; though, these recommendations are not universally consistent across different guidelines. We present a case of late HBV reactivation in a 76-year-old male with occult HBV infection who received rituximab-based therapy for chronic lymphocytic leukemia. In accordance with HBV reactivation guidelines, the patient was prescribed entecavir 0.5 mg daily during chemotherapy and for 18 months following the completion of hematological treatment. Despite adherence to these recommendations, the patient developed HBV reactivation 2 years and 5 months after the cessation of rituximab-based therapy, which progressed to acute HBV hepatitis. Our case emphasizes the need for extended follow-up in patients undergoing rituximab-based immunosuppression. It highlights the critical importance of vigilance for HBV reactivation and the potential consequences of delayed treatment. This case supports evidence on the unpredictability of HBV reactivation timelines and underscores the need for standardized monitoring protocols.
Keywords: HBV reactivation, hepatitis B, rituximab, leukemia, HBV reactivation prophylaxis, entecavir
Introduction
The reactivation of hepatitis B virus (HBV) is a known complication of long-term immunosuppressive or cytotoxic therapy, typically emerging during immunosuppression or a few months post-treatment.1 While there is no universal consensus on the definition of HBV reactivation, it is generally understood to encompass two scenarios: (1) HBV reactivation in chronic infection, defined by a rise in HBV DNA levels in individuals with existing viremia, or the reemergence of detectable HBV DNA in previously undetectable cases; and (2) Reverse seroconversion, characterized by the reappearance of serum HBsAg and HBV DNA in individuals with occult HBV infection.2 HBV reactivation arises when immune-mediated control of viral replication is disrupted, often as a result of immunosuppression. A variety of treatments, including cytotoxic chemotherapy, biologics, B or T cell-depleting agents, corticosteroids, conventional immunosuppressants, and novel cell-based therapies, can impair the immune system’s ability to suppress HBV activity. In particular, B-cell depleting therapies, like rituximab, are strongly associated with HBV reactivation.2–6 This is attributed to their mechanism of action, which involves the depletion of circulating B cells and partial depletion of B cells in the lymphatic system and bone marrow. Consequently, a significant drop in anti-HBs antibody titers has been observed in patients receiving rituximab therapy, with reactivation being most prevalent among those who experience a complete loss of anti-HBs Ab.7
Guidelines on HBV reactivation recommend the use of nucleos(t)ide analogue (NA) - entecavir (ETV) 0.5mg/daily or tenofovir disoproxil (TDF) 245 mg/daily - during therapy and for 6 to 18 months thereafter to mitigate this risk of reactivation.8 However, sporadic cases of late-onset HBV reactivation, occurring up to 10 years post-therapy, have been reported.9 We present a case of HBV reactivation 2 years and 5 months after rituximab-based treatment despite adequate reactivation prophylaxis.
Case Report
A 76-year-old man was diagnosed with chronic lymphocytic leukemia in 2019 and enrolled in a chemotherapy clinical trial with rituximab, fludarabine, and cyclophosphamide in 2020. During the initial workup, occult hepatitis B virus was detected: hepatitis B surface antigen (HBsAg) negative, antibody to hepatitis B surface antigen (anti-HBs Ab) less than 3.1 mIU/mL, hepatitis B e antigen (HBeAg) negative, antibody to hepatitis B e antigen (anti-HBe Ab) negative, antibody to hepatitis B core antigen (anti-HBc Ab) positive, and hepatitis B virus DNA negative. He was placed on HBV reactivation prophylaxis per Polish guidelines,3 starting ETV 0.5 mg daily in early September of 2020, with chemotherapy initiated later that year. Rituximab-based treatment concluded in March 2021, and ETV prophylaxis was stopped 18 months later, after a total of 25 months. He was monitored quarterly in an outpatient reactivation prophylaxis clinic with HBV DNA and ALT levels ordered every visit, throughout the whole prophylaxis period and during subsequent monitoring phase, as required by Polish Ministry of Health Program for HBV Reactivation Prophylaxis. The patient achieved disease stabilization and remained under hematological observation.
At a follow-up in July 2023, HBV viral load was elevated (144 IU/mL) with normal ALT (8 U/L). By early October 2023, HBV DNA was 874061921IU/mL, HBsAg was positive; ALT (18 U/L) and INR (1,04) remained normal. In late October 2023, hepatitis due to HBV reactivation was diagnosed, with elevated biochemical and serological markers: ALT 863 U/L, AST 597 U/L, GGTP 229 U/L, INR 1.14, HBsAg(+), HBeAg(+), anti-HBe Ab(-), anti-HBs Ab 0.25 mIU/mL, anti-HBc Ab(+), and HBV DNA 47883905IU/mL. Entecavir 0.5 mg daily was reintroduced.
In November 2023 patient was hospitalized with jaundice, dark urine, diminished appetite, and general malaise. Laboratory results from outpatient clinic and hospital admission are summarized in Table 1. Coinfections with CMV, HAV, HCV, HDV, HEV were excluded serologically. By December 2023, the patient achieved biochemical remission. In April 2024, seroconversion to anti-HBe Ab(+) was observed, though the patient remained both HBsAg- and HBeAg-positive with a detectable HBV viral load until July 2024, when the viral load became undetectable The patient remained under the care of the outpatient clinic and continued ETV 0.5 mg daily. As of September 2024, following the initial submission of this manuscript, the patient achieved seroclearance of both HBsAg and HBeAg.
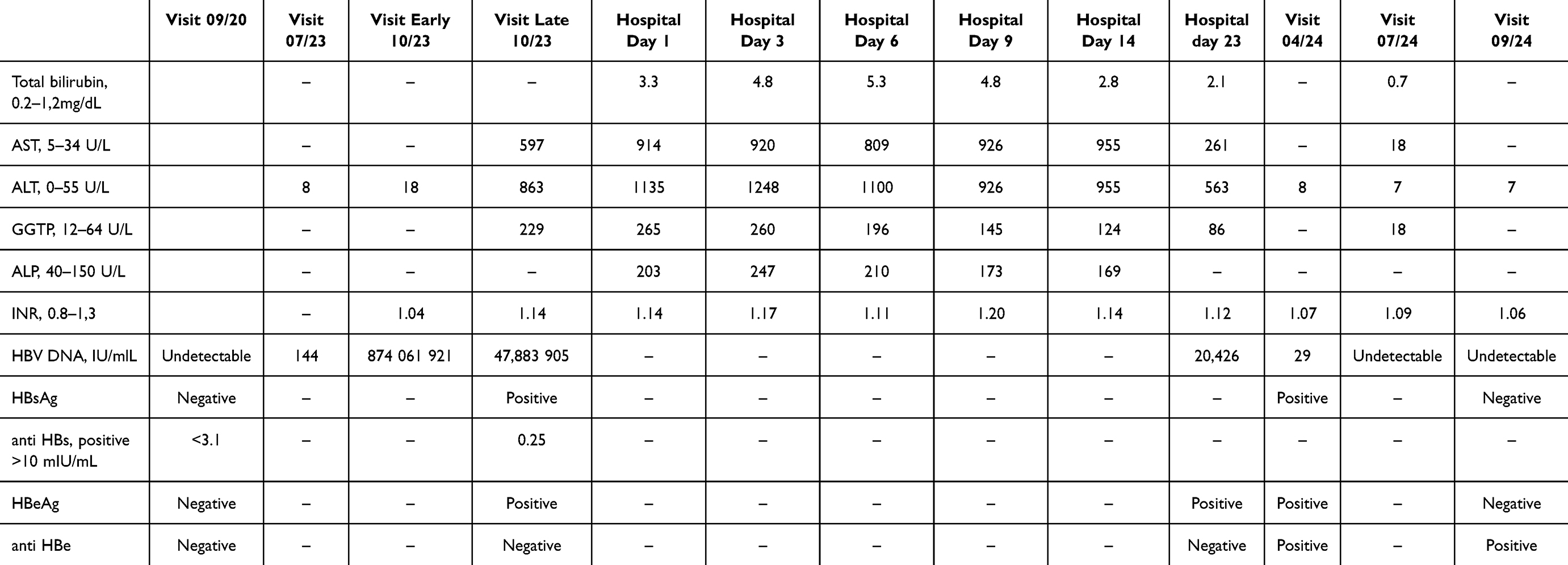 |
Table 1 Laboratory Results from Hospitalization and Outpatient Care |
Discussion
B-cell depleting agents and hematopoietic stem cell transplantation carry a significant risk (>10%) of HBV reactivation.1–3,5–8 Low anti-HBs Ab and anti-HBc Ab titers have been identified as additional risk factors for HBV reactivation.4,9 Scholars describe HBV reactivation rates double in patients with negative anti-HBs Ab compared to those with positive anti-HBs Ab following rituximab-based chemotherapy.2 Some authors suggest a protective anti-HBs Ab titer as >100 mIU/mL; however, this recommendation has yet to be reflected in practice guidelines.10
There is no consensus among guidelines regarding the optimal duration of HBV prophylaxis and subsequent monitoring. Standard prophylaxis time varies between 6–12 months and 12–18 months for rituximab-based treatment.8 For subsequent monitoring, guidelines from the European Association for the Study of the Liver (EASL), the American Association for the Study of Liver Diseases (AASLD), and Polish expert recommendations on HBV reactivation prevention suggest observation for 12 months after prophylaxis cessation, with liver function tests and HBV DNA monitored every 3–6 months.3,8 However, the optimal monitoring period is not uniformly stated across the guidelines. Both the American Gastroenterological Association (AGA) and the Asian Pacific Association for the Study of the Liver (APASL) do not provide a specific stance on the recommended length of monitoring.8 Evidence suggests that this observation period may be inadequate for certain patients. In fact, HBV reactivation has been reported in 35.3% of patients within 2 to 24 months after completing adequate prophylaxis course.1 Furthermore, rituximab-based treatments have been documented to induce HBV reactivation long after immunosuppression cessation, with a median time of 25 months (range 3–128 months).4 Reports of delayed reactivation in patients undergoing hematological treatments underscore the necessity for revisiting the recommended durations of HBV reactivation prophylaxis and subsequent monitoring, as some patients may experience HBV reactivation beyond the standard 12-month monitoring period.
In the presented case, the first sign of HBV infection reactivation was present in early July 2023; however, treatment was initiated 3.5 months later, after the patient had already developed fully pronounced HBV-related hepatitis. This raises the question of whether stricter monitoring following the detection of HBV DNA in July 2023 would have allowed for earlier initiation of NA therapy. The patient was monitored every three months in the outpatient reactivation prophylaxis clinic by different physicians, in accordance with the Polish Ministry of Health Program for HBV Reactivation Prophylaxis. HBV DNA and ALT were routinely monitored at each visit. However, at that time, there was a systemic procedural delay in processing HBV DNA results in our hospital, which were typically available only 2–3 weeks after testing and often reviewed during subsequent visits, up to three months later. It is plausible that, given the normal ALT levels and the lack of clinical suspicion, the positive HBV DNA result from July 2023 was only acknowledged during the October 2023 visit, leading to a missed opportunity for an earlier intervention. However, initiating treatment at that timepoint remains debatable, as EASL 2017 Clinical Practice Guidelines (CGP) on the management of hepatitis B virus infection state that HBV DNA detection leads to HBsAg seroreversion and hepatitis in only 50% of cases.9
The decision not to initiate NA therapy at the early October visit, when the patient became HBsAg-positive, also warrants discussion. EASL CGP guidelines on HBV infection underscore the need to start NA treatment as soon as HBsAg seroreversion is acknowledged, regardless of ALT levels.9 We believe the lack of such intervention may have been influenced by the Polish Ministry of Health’s Chronic HBV Treatment Programme. At the time of early October 2023 visit, the patient did not meet these criteria, which would have allowed treatment to be provided cost-free under the universal health insurance system. Consequently, the treatment initiation was delayed by 22 days. Furthermore, the missed diagnostic and therapeutic decisions in this patient may have stemmed from the overall low prevalence of late HBV reactivations.11 This case underscores the need for increased awareness and vigilance in patients with chronic or occult hepatitis treated with rituximab, particularly in older individuals. It also highlights the importance of revising the inclusion criteria for Poland’s HBV Treatment Programme to better accommodate such cases.
Conclusions
This case highlights the potential for late HBV reactivation in patients treated with B-cell-depleting agents, even years after immunosuppression cessation and despite adherence to recommended prophylaxis protocols. Current guidelines for HBV prophylaxis and monitoring may not adequately address the needs of patients at risk for delayed reactivation, particularly after rituximab-based treatments with reactivation occurring many months or years after stopping HBV reactivation prophylactic treatment. To improve outcomes, this report advocates for unified guidelines on HBV prophylaxis and monitoring durations, as a subset of patients may experience reactivation outside the currently defined timeframes. Additionally, heightened clinical vigilance is warranted, particularly for high-risk patients undergoing rituximab-based therapy with low anti-HBs titers. These findings emphasize the need for revisiting current guidelines to better account for the complexities of HBV reactivation risk and management.
Abbreviations
ALP, alkaline phosphatase; ALT, alanine aminotransferase; anti Hbe, antibodies against hepatitis B “e” antigen; AST, aspartate aminotransferase; GGTP, gamma-glutamyl transpeptidase; HBeAg, hepatitis B “e” antigen; HBsAg, hepatitis B “s” antigen; HBV DNA, hepatitis B virus deoxyribonucleic acid; INR, international normalized ratio.
Ethics and Consent
This study was conducted in compliance with ethical standards and institutional policies. Institutional approval was not required for the publication of this case report. Written informed consent for publication of their details was obtained from the patient.
Disclosure
The authors confirm that they have no financial interests or conflicts of interest that could have influenced the outcomes or content of this work.
References
1. Salpini R, Battisti A, Colagrossi L, et al. A snapshot of virological presentation and outcome of immunosuppression-driven HBV reactivation from real clinical practice: evidence of a relevant risk of death and evolution from silent to chronic infection. J Viral Hepat. 2019;26(7):846–855. doi:10.1111/jvh.13101
2. Shi Y, Zheng M. Hepatitis B virus persistence and reactivation. BMJ. 2020;370:m2200. doi:10.1136/bmj.m2200
3. Pawłowska M, Flisiak R, Gil L, et al. Profilaktyka reaktywacji zakażeń HBV – rekomendacje grupy roboczej profilaktyki reaktywacji HBV. Acta Haematol Pol. 2019;50(4):192–198. doi:10.2478/ahp-2019-0031
4. Lau G, Yu ML, Wong G, et al. APASL clinical practice guideline on hepatitis B reactivation related to the use of immunosuppressive therapy. Hepatol Int. 2021;15:1031–1048.
5. Flisiak R, Halota W, Jaroszewicz J, et al. Recommendations for the treatment of chronic viral hepatitis B in 2018 by Polish Group of Experts for HBV [in Polish]; 2018.
6. Lampertico P, Agarwal K, Berg T, et al. EASL 2017 clinical practice guidelines on the management of hepatitis B virus infection. J Hepatol. 2017;67(2):370–398. doi:10.1016/j.jhep.2017.03.021
7. Wang B, Mufti G, Agarwal K. Reactivation of hepatitis B virus infection in patients with hematologic disorders. Haematologica. 2019;104(3):435–443. doi:10.3324/haematol.2018.210252
8. Myint A, Tong MJ, Beaven SW. Reactivation of hepatitis B virus: a review of clinical guidelines. Clin Liver Dis. 2020;15(4):162–167. doi:10.1002/cld.883
9. Ohkubo M, Seo E, Doki K, et al. Impact of hepatitis B surface and core antibody levels on hepatitis B virus reactivation. Biol Pharm Bull. 2024;47(5):941–945. doi:10.1248/bpb.b23-00907
10. Poola S, Kratzer M, Sewell K, Tillmann HL. Size matters! Anti-HBs titer and HBV reactivation during anti-TNF therapy. Dig Dis Sci. 2023;68(12):4511–4520. doi:10.1007/s10620-023-08141-7
11. Etienne S, Vosbeck J, Bernsmeier C, Osthoff M. Prevention of hepatitis B reactivation in patients receiving immunosuppressive therapy: a case series and appraisal of society guidelines. J Gen Intern Med. 2023;38(2):490–501. doi:10.1007/s11606-022-07806-9
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.