Back to Journals » Clinical, Cosmetic and Investigational Dermatology » Volume 15
A Single Center, Prospective, Randomized, Blinded Study to Evaluate the Efficacy and Safety of a Topical Tripeptide/Hexapeptide Anhydrous Gel When Used Pre- and Post- Hybrid Fractional Laser for the Treatment of Acne Scars
Authors Weinstein Velez M, Prezzano J, Bell M, Widgerow A ![]()
Received 13 October 2022
Accepted for publication 2 December 2022
Published 16 December 2022 Volume 2022:15 Pages 2763—2774
DOI https://doi.org/10.2147/CCID.S392459
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Jeffrey Weinberg
Mara Weinstein Velez,1 James Prezzano,1,2 Michaela Bell,3 Alan Widgerow3,4
1Department of Dermatology, University of Rochester, Rochester, NY, USA; 2Fayetteville Dermatology, Fayetteville, NY, USA; 3Clinical Research Dept, Alastin® Skincare, Inc. (A Galderma Company), Carlsbad, CA, USA; 4Plastic Surgery Dept, Center for Tissue Engineering, University of California Irvine, Irvine, CA, USA
Correspondence: Alan Widgerow, Email [email protected]
Background: Acne scarring remains a significant problem. Laser therapy has produced varying results with deeper ablative therapies occasionally associated with side effects including delayed healing, infection, scarring, erythema, acne, milia, edema and dyspigmentation.
Objective: Can adjuvant topical therapy impact the healing process and outcome of patients treated with fractional laser for acne scarring?
Methods and Materials: Ten patients were randomized to receive either Regenerating Skin Nectar with TriHex Technology®– RSN or a bland moisturizer. Patients underwent two laser procedures one month apart with Hybrid Fractional Laser. The topical was applied twice daily for 2 weeks prior to the first laser procedure, and through completion of the study. Seven study visits occurred over a 90-day period. Measurements were conducted in lesional and non-lesional areas – transepidermal water loss (TEWL), erythema, photography, Goodman and Baron qualitative scale, Global Aesthetic Improvement Scale and patient questionnaires – to assess functional recovery and aesthetic outcomes in the scarred areas. One patient from each cohort consented to biopsy before the procedures and 90 days after the first procedure.
Results: Reduced TEWL scores in the RSN group were evident at all time points with statistically significant reductions occurring 4 days after first and second procedures indicating more efficient fluid conservation at a critical point in the healing trajectory. Erythema index demonstrated a consistent decrease in the RSN cohort over the control from day 4 through day 90 on lesional and non-lesional skin. Acne scar assessment scores improved in the RSN cohort compared with the control at all time points. Biopsy results showed early elastin regeneration in the RSN biopsy with controlled non-hypertrophic collagen formation evident.
Conclusion: The use of RSN pre- and post- laser resurfacing significantly decreased postprocedural TEWL and erythema, and increased aesthetic improvement in acne scars and patient satisfaction, when compared with bland moisturizer.
Keywords: acne scars, laser resurfacing, post procedure, topical
Background
Acne and subsequent scarring have been linked to emotional debilitation, embarrassment, and anxiety.1 The prevalence of acne scarring is 1–11% of the general population and can affect up to 95% of patients with acne vulgaris.2–4
Three primary acne scars include icepick (<2 mm, deep with tracts to dermis), rolling (circular or linear, >4 mm, gently sloped edges merging with normal skin) and boxcar (wide based 1.5–4 mm diameter; shallow <0.5 mm, deep >0.5 mm).5 Various medical and procedural modalities have been employed to reduce acne scarring. Medical management includes retinoids, topical/injectable steroids, and silicone dressings. Surgical management includes punch excision, elliptical excision, punch elevation, skin grafting, subcision and debulking. Procedural management includes lasers, cryosurgery, electrodesiccation, radiation, chemical peels, microneedling, and dermabrasion.6,7
Amongst laser therapy, ablative modalities have been shown to reduce the appearance of shallow boxcar and ice-pick scars.8 Side effects of ablative laser therapy include delayed healing, infection, scarring, erythema, acne, milia, edema and dyspigmentation. In order to improve side effect profile, fractional photothermolysis has become a reasonable option for resurfacing. It ablates tissue in a columnar fashion, creating microscopic thermal zones and leaving areas of native epidermis and dermis to provide for collagen remodeling and neogenesis. After fractional ablation, basal keratinocytes begin to re-establish a continuous basement membrane with 24 hours and complete epidermal regeneration by 7 days.9 Graber et al noted a 7.6% complication rate (of 961 patients) after fractional ablative laser therapy for photodamage. The most frequent complications were acneiform eruptions and herpes simplex virus outbreaks (both approximately 1.7%).10
The standard of post-procedural laser care is varied but has included vitamin E, vitamin C, aloe vera, bovine collagen, petrolatum and bland creams. Data to support the superiority of one over another are limited.11 More recently, a tripeptide and hexapeptide (TriHex) anhydrous gel was formulated to aid in the removal of protein degradation and stimulate basal keratinocytic stem cells and fibroblasts resulting in elastogenesis and collagenesis and promoting overall wound repair.12
The anhydrous gel with TriHex and synergistic actives is used as a pre-conditioning aid before the procedure to prepare the extracellular matrix (ECM) and following the procedure to optimize healing. This has been shown in numerous clinical studies to accelerate healing with improved symptomatic relief (less redness, exudate, pain, itching, etc.) following invasive resurfacing and microneedling procedures.11–18
As such, this study evaluated skin recovery and outcomes of an anhydrous gel with tripeptide and hexapeptides compared with a bland moisturizer used pre and post laser resurfacing for the improvement of acne scars.
Methods
This prospective, randomized study was IRB approved by the University of Rochester Medical Center, College Town Dermatology. Eligible subjects included males and females over 18, with evidence of grade II–III (mild to moderate) acne scars on the face, as determined by the Goodman and Baron qualitative global acne scar grading system.14 This grading system was chosen, given its widespread acceptance as a simple and effective means of normalizing objective appearances among patients. Individuals were excluded who had undergone treatment to the face with any energy device within 6 months, tanning within 7 days, dermabrasion or chemical peel within 3 months, use of systemic steroids within 6 months, current use of systemic retinoids, keloidal scarring in the treatment area or use of topical products with retinoid, alpha-hydroxy acid, salicylic acid, or vitamin C or E within 14 days. Individuals who were pregnant, lactating, or planning on becoming pregnant during the study duration were also excluded.
Eligible subjects were consented and randomized to either Regenerating Skin Nectar with TriHex Technology®– RSN (Alastin Skincare, Inc., Carlsbad, CA) or a bland moisturizer (Cetaphil lotion, Galderma, Fort Worth, TX) to apply twice daily for 2 weeks prior to the first laser procedure, through the completion of the study. Both products were blinded in identical bottles and all subjects were dispensed the same gentle cleanser and SPF 30+ to use throughout the course of the study. A total of seven study visits occurred; screening and baseline at least 2 weeks prior to the first laser treatment, 2 laser treatment visits one month apart, follow-up visits post each laser treatment at day 4, and a final visit 60 days post the last laser treatment. The study adhered to the guidelines from the University of Rochester in performing human research subject research in the COVID-19 Era. TriHex technology includes a set of peptides (Tripeptide 1 and Hexapeptide −12) and other actives (phosphatidylserine, oleuropein) which have been demonstrated to aid in removing fragmented collagen and elastin (collected through photodamage and aging), decreasing glycation end products and promoting increased autophagy and proteasome efficiency.12
The following measurements were performed by either the blinded investigator or a blinded study team member.
Transepidermal water loss (TEWL) AquaFluxTM Model AF200 (Biox Systems Ltd, London, England): measures the volume of water passing through the epidermal layer assessing skin barrier function. Therefore, a decrease in TEWL signifies an improved skin barrier. Measurements were conducted on lesional and non-lesional facial skin in the same area, at every study visit. Measurements were collected in duplicate on clean skin.
Chromameter CR-400 Chroma Meter (Konica Minolta, Ramsey, NJ): Standardized device measurements to quantify the intensity of erythema a*. Colorimetry measurements on lesional and non-lesional skin were conducted in the same facial area at every visit registering the average of three measures of a* value for every tested field. Facial skin was clean prior to measurements.
Photography
Photography of the left and right sides of the face were taken at every visit with the LifeViz Micro 3D camera system (Quantificare Inc., Cumming, GA).
Goodman and Baron Qualitative Scale
A 4-point scar grading scale, Table 1, was completed at screening, pre procedure at both laser treatment visits and at the final visit, post day 60, following laser treatment 2.
 |
Table 1 Goodman and Baron Qualitative Scale |
Global Aesthetic Improvement Scale (GAIS)
Grading was completed by the blinded investigators prior to the laser treatment, at day 30 post laser treatment 1 and at the final visit, post day 60, following laser treatment 2. The 5-point GAIS consisted of the following: 1 = worse: appearance has worsened compared with the original condition; 2 = no change: appearance remains the same as the original condition; 3 = improved: better than the initial condition; 4 = much improved: marked improvement but not completely optimal; 5 = very much improved: excellent or exceptional improvement.
Subjects Satisfaction Assessment
At every visit, each subject assessed their acne scars, using the following rating assessment. 1 = poor, 2 = fair, 3 = good, 4 = very good, and 5 = excellent.
Biopsies
One subject from each cohort consented to a 3 mm punch biopsy on the face prior to the use of the designated products and at the last study visit, 60 days post laser treatment 2. Biopsies were analyzed by a blinded dermatopathologist.
Laser Treatment
Sixty minutes prior to both laser treatments, topical anesthesia (tetracaine 7% with lidocaine 23% ointment) was applied to the face. Subjects then underwent treatment with the HALO™ Hybrid Fractional Laser (Sciton®, Inc. Palo Alto, CA). Laser settings were determined by skin type and the investigators’ standard of care.
Statistical Analyses
GraphPad Prism Software (San Diego, CA) was utilized to compute the differences between baseline and follow-up visits for TEWL, colorimetry and assessments. To test for a significant difference in the outcome between the two treatments, parametric test (i.e., paired t-test) was performed.
Results
Five men and 5 women enrolled into the study, ages 19–45, mean age 33.4, with the following skin types: 4 = type I, 2 = type II, 3 = type III, 1 = type IV. The study initiated in January 2020 with the last subject completing in May 2021. One participant, in the control cohort, discontinued post treatment 1 due to a melasma flare.
TEWL
In lesional skin measurements, there was a statistically significant difference at day 4 post both laser treatments. At day 4, post laser treatment 1, participants in the RSN arm had a mean change of 6.502 compared with the control arm of 21.59 (p=0.02). At day 4, post laser treatment 2, there was even a great statistical difference of p = 0.0001, RSN arm mean change of 2.858 and control 39.07. In non-lesional skin, measurements of subjects using RSN decreased prior to the first laser treatment, −5.098, whereas the control arm increased, 2.061. RSN subjects continued to have less TEWL measured at each visit, although not statistically significant different from the control (Figure 1).
 |
Figure 1 TEWL results in lesional and non-lesional skin measurements: In lesional skin measurements, there was a statistically significant difference at day 4 post both laser treatments. In non-lesional skin, measurements of subjects using RSN decreased prior to the first laser treatment, whereas the control arm increased. RSN subjects continued to have less trans epidermal water loss measured at each visit, although not statistically significant different from the control. |
Colorimetry
Erythema index a* demonstrated a consistent decrease in the RSN cohort over the control from day 4 post the first laser procedure through day 90 on lesional and non-lesional skin. Measurements of lesional skin in the RSN cohort had less erythema from day 30 onwards compared with the control, that never decreased from baseline (Figure 2).
 |
Figure 2 Colorimetry results: Erythema index demonstrated a consistent decrease in the RSN cohort over the control from Day 4 post the first laser procedure through day 90 on lesional and non-lesional skin. |
Goodman and Baron Scale
Blinded investigator scores of acne scars improved in the RSN cohort compared with the control. At day 30 post laser procedure 1, RSN had a mean score improvement of −0.33 from baseline and −0.25 in the control cohort. At day 90 post laser procedure 2, RSN had a mean score improvement of −0.83 from baseline whereas the control had a −0.40 improvement in acne scars (Figure 3).
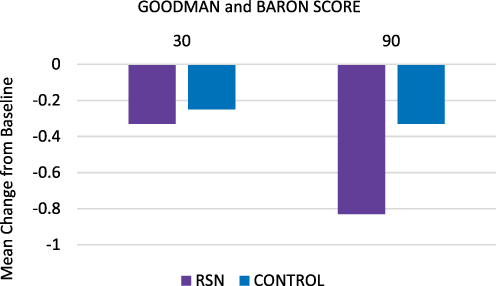 |
Figure 3 Goodman and Baron scale demonstrating improvement of blinded investigator scores of acne scars in the RSN cohort compared with the control. |
GAIS
The blinded investigator graded the global assessment of improvement in a majority of the subjects using RSN as improved at days 30 and 60. The control subjects were graded in an equal distribution as no change or improved at day 30 and no change, improved, and much improved at day 90 (Figure 4).
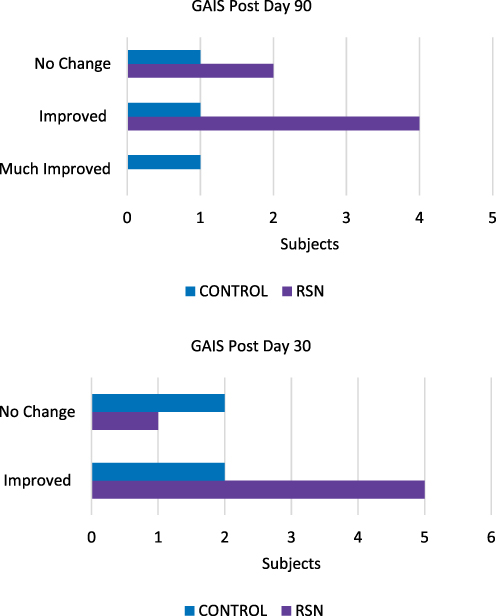 |
Figure 4 GAIS: The blinded investigator graded the global assessment as improvement in the majority of the subjects using RSN at days 30 and 60 as compared with control. |
Subject Satisfaction
At every visit post the first laser procedure, subjects randomized to RSN rated their satisfaction of the improvement of their acne scars higher than the control and significantly greater at day 90 (Figure 5).
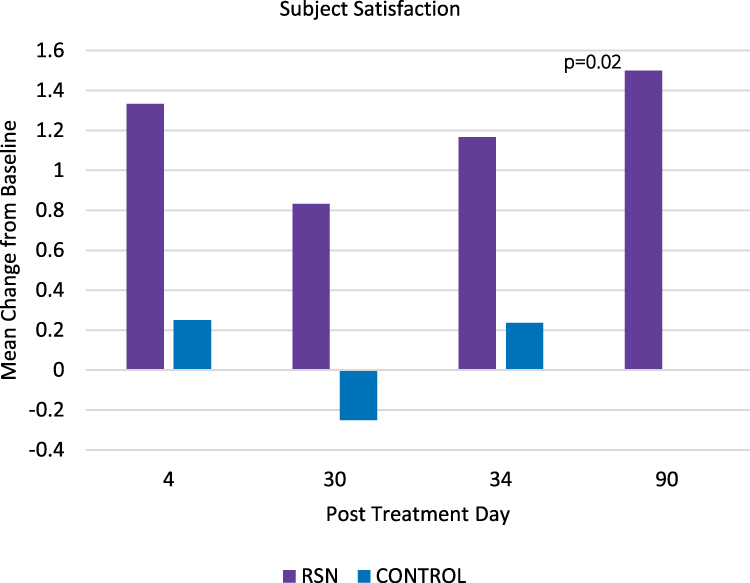 |
Figure 5 Subject satisfaction demonstrating superior assessment of scar appearance for RSN group. |
Biopsies (Figures 6–9)
Two subjects underwent biopsies pre topical and laser procedures and post day 90. One subject was in the RSN cohort and one in the control cohort. Biopsies were evaluated by an independent dermatopathologist.
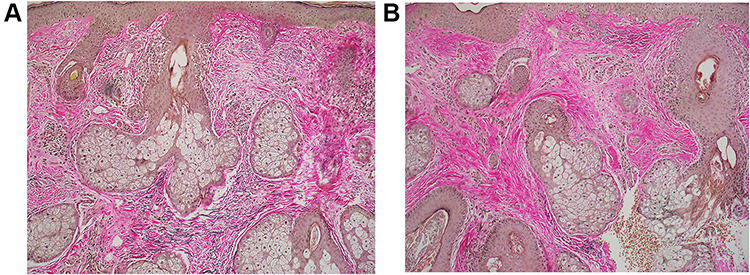 |
Figure 6 (A and B) Biopsies of subject treated with bland moisturizer pretreatment and at 90 days post treatment. Elastic fibers disappear after treatment with an early re-appearance in reticular dermis at 90 days after treatment. |
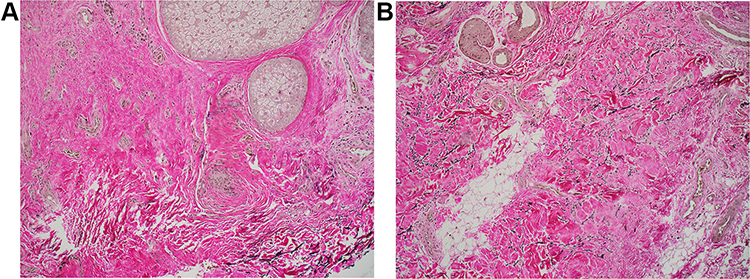 |
Figure 7 Biopsies of subject treated with RSN showing almost completely absent elastic fibers in the center of the specimen, in both the superficial and deep dermis pre-treatment (A), but on day 90 the biopsy shows relatively normal elastic fibers in the papillary dermis with additional fibers in the reticular dermis (B). |
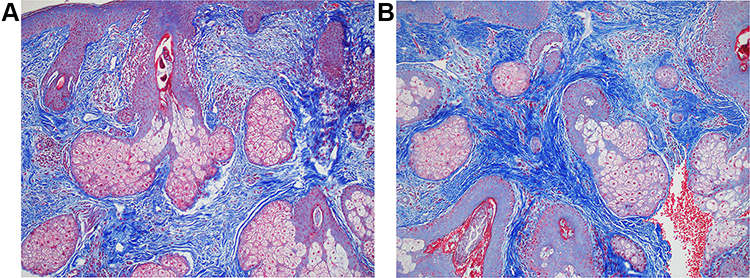 |
Figure 8 (A and B) Trichrome stain in subject using bland moisturizer shows thin collagen bundles in the papillary and mid reticular dermis pre-treatment (A), while day 90 shows markedly increased thickness of collagen bundles (B). |
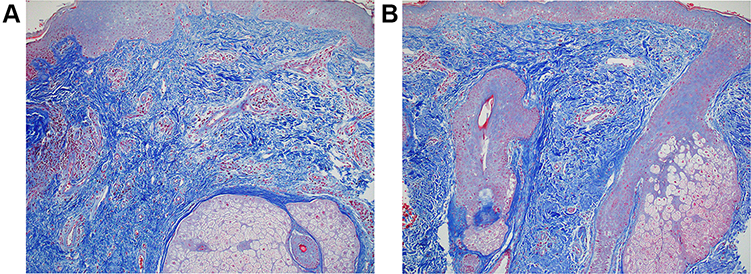 |
Figure 9 (A and B) Trichrome stain in subject using RSN shows day 0 shows focally abnormally thin collagen bundles (A) while day 90 shows a modest increase in normal-density collagen bundles (B). |
In the subject treated with the bland moisturizer, elastic tissue stain on day 0 shows absent elastic fibers in the papillary dermis, and abnormally fragmented elastic fibers in the reticular dermis. On day 90 there is continued absence of elastic fibers in the papillary dermis but early improvement in the characteristics of the elastin fibers in the reticular dermis is evident in Figure 6A and B.
In contrast, in the RSN treated subject, elastic tissue stain in the day 0 biopsy shows almost completely absent elastic fibers in the center of the specimen, in both the superficial and deep dermis (Figure 7A), but on day 90 the biopsy shows relatively normal elastic fibers in the papillary dermis with additional fibers in the reticular dermis (Figure 7B).
As far as collagen replacement was concerned, bland moisturizer Trichrome stain shows thin collagen bundles in the papillary and mid reticular dermis on day 0 (Figure 8A), while 90 shows markedly increased thickness of collagen bundles (Figure 8B).
The RSN subject biopsy Trichrome stain on day 0 shows focally abnormally thin collagen bundles (Figure 9A) while day 90 shows a modest increase in normal-density collagen bundles (Figure 9B).
Photography
Changes in volume depth of acne scars and skin topography were measured using the Quantificare 3D micro images and software. Comparisons were made between the two cohorts of subjects with similar acne scar types. The subjects with deep scars had a greater improvement in volume depth using RSN than the control and similarly subjects using RSN, with rolling acne scars, had an improvement in skin smoothness and texture (Figures 10–12).
 |
Figure 10 (A and B) 3D Micro Imaging monitoring skin texture difference in subject with bland moisturizer (A) and patient treated with RSN (B). |
 |
Figure 11 (A and B) 3D Micro Imaging demonstrating differences in improvement in scar depth in in subject with bland moisturizer (A) and patient treated with RSN (B). The deeper the blue the greater the depth. |
 |
Figure 12 (A and B) 3D Micro Imaging. Example of decreased erythema and inflammation post laser treatment 1 at day 30 between control/bland moisturizer (A) and RSN (B). |
Discussion
In the last 5 years, preconditioning the skin prior to energy based treatments has become more prevalent. RSN with TriHex Technology® has a proprietary recycling mechanism to aid in the removal of aged, damaged fragments and restore new, healthy collagen and elastin. Clinically it has been demonstrated to promote healing and outcomes following laser and microneedling treatments, as well as surgery.11–18 Wilson et al showed tripeptide/hexapeptide post-procedural care was associated with a shortened downtime and decreased symptoms following laser resurfacing of the face.11 Patients reported a significantly higher level of satisfaction compared with controls.11 Robinson et al showed superior healing at post-procedure day 4 (blinded investigator and patient impression), significantly better skin tone, and higher levels of patient satisfaction compared with the control regimen.13
Further, in a randomized, split-faced trial conducted by Nelson et al, the postoperative effects of a pre and post treatment skin care regimen using tripeptide and hexapeptide in an anhydrous base provided improved outcomes and reduced healing time following hybrid laser resurfacing of the face when compared with the standard of care regimen.14 Preference for the anhydrous gel was also noted for the majority of subjects when compared with the standard of care regimen.14
In this study the use of RSN pre and post procedure demonstrated a significant decrease in transepidermal water loss compared with the control post 4 days of the laser procedure and continued decrease in erythema as measured by the chromameter. The decrease in TEWL measurement would signify a change in skin physiology from one of scarred inefficient conservation of water to skin performing closer to normal with re-established water conservation. This is a very useful indirect marker of scar tissue transformation. This is particularly evident in the short term in this study when the period at 4 days after procedure may be associated with excessive fluid loss before barrier function has recovered. RSN appears to conserve fluid very efficiently at this important time period as opposed to the bland moisturizer. Blinded investigators graded an improvement in acne scars at day 90 in the RSN cohort as compared with the control, with a mean score of −0.83 from baseline compared with −0.40 in the control. Subject satisfaction was consistently higher with the RSN cohort with statistical significance at day 90.
Limitations to this study include a minimal sample size conducted at one center. In addition, although only one patient from each cohort was randomly selected, the histological changes seen coincided very well with the observed clinical outcomes. The premise here when considering scar tissue replacement is controlled collagen replacement without overexuberant collagen fibers and more importantly a demonstrated increase in elastin fibers denoting regenerative replacement of scar tissue. Thus, early generated elastin was observed in the RSN treated biopsy with some signs of regeneration occurring much later in the bland moisturizer biopsy. Controlled collagen replacement was also observed in the RSN subject biopsy, in contrast to less organized collagen fiber formation observed in the bland moisturizer subject biopsy.
With a small sample size, it is also difficult to stratify different cohorts according to skin types and draw conclusions. We did observe a trend of more severe scarring in darker skin types but response to treatment appeared to be similar among the groups. This may reflect the small sample size and it would be interesting to observe differences among different skin types in larger numbers of patients. That noted, the response and improvement of combined device and topical therapy appears to be constant among all skin types.
Conclusions
A comparative study was undertaken to assess the effect of adjunctive topical therapy on the outcome of HALO™ Hybrid Fractional Laser treatment of acne scars. A product containing tripeptide and hexapeptides was applied in one cohort and compared with a group receiving treatment with a bland moisturizer following laser treatment. Although this was a small 10 patient study, the results demonstrated that use of RSN pre and post laser resurfacing significantly decreased postprocedural TEWL and erythema, and increased improvement in acne scars and patient satisfaction. In addition, biopsy results showed good regenerative effects with the RSN product.
Data Sharing Statement
Individual de-identified participant data may be shared with readers requesting such data – this includes details of analysis and certain photographs that are de-identified. Data will be made available on specific request to the author for the following year after publication.
Ethics and Consent Statements
This study complies with the Declaration of Helsinki. All research participants provided written informed consent.
Acknowledgements
The authors would like to acknowledge Dr Kathleen Mannava, Dermatopathologist University of Rochester, for her contribution to the histological analysis.
Funding
University of Rochester Medical Center, College Town Dermatology and Alastin®Skincare, Inc.
Disclosure
Dr Mara Weinstein Velez reports grants from Alastin Skincare, during the conduct of the study. Ms Michaela Bell reports grants from Alastin Skincare Inc., during the conduct of the study is the director of Clinical Research for Alastin Skincare, outside the submitted work. Professor Alan Widgerow is the Chief Scientific Officer for Galderma. In addition, Professor Alan Widgerow has a patent Widgerow issued to Galderma. The authors report no other conflicts of interest in this work.
References
1. Koo J. The psychosocial impact of acne: patients’ perceptions. J Am Acad Dermatol. 1995;32(5 Pt 3):S26–S30. doi:10.1016/0190-9622(95)90417-4
2. Cunliffe WJ, Gould DJ. Prevalence of facial acne vulgaris in late adolescence and in adults. Br Med J. 1979;1(6171):1109–1110. doi:10.1136/bmj.1.6171.1109
3. Layton AM, Henderson CA, Cunliffe WJ. A clinical evaluation of acne scarring and its incidence. Clin Exp Dermatol. 1994;19(4):303–308. doi:10.1111/j.1365-2230.1994.tb01200.x
4. Goulden V, Stables GI, Cunliffe WJ. Prevalence of facial acne in adults. J Am Acad Dermatol. 1999;41(4):577–580.
5. Jacob CI, Dover JS, Kaminer MS. Acne scarring: a classification system and review of treatment options. J Am Acad Dermatol. 2001;45(1):109–117. doi:10.1067/mjd.2001.113451
6. Rivera AE. Acne scarring: a review and current treatment modalities. J Am Acad Dermatol. 2008;59(4):659–676. doi:10.1016/j.jaad.2008.05.029
7. Goodman GJ, Baron IA. The management of postacne scarring. Dermatol Surg. 2007;33(10):1175–1188. doi:10.1111/j.1524-4725.2007.33252.x
8. Woo SH, Park JH, Kye YC. Resurfacing of different types of facial acne scar with short-pulsed, variable-pulsed, and dual-mode Er: YAGlaser. Dermatol Surg. 2004;30(4 Pt 1):488–493. doi:10.1111/j.1524-4725.2004.30161.x
9. Laubach HJ, Tannous Z, Anderson RR, Manstein D. Skin responses to fractional photothermolysis. Lasers Surg Med. 2006;38(2):142–149. doi:10.1002/lsm.20254
10. Graber EM, Tanzi EL, Alster TS. Side effects and complications of fractional laser photothermolysis: experience with 961 treatments. Dermatol Surg. 2008;34(3):301–5; discussion 305–7. doi:10.1111/j.1524-4725.2007.34062.x
11. Vanaman Wilson MJ, Bolton J, Fabi SG. A randomized, single-blinded trial of a tripeptide/hexapeptide healing regimen following laser resurfacing of the face. J Cosmet Dermatol. 2017;16(2):217–222. doi:10.1111/jocd.12339
12. Widgerow AD, Cohen SR, Fagien S. Preoperative skin conditioning: extracellular matrix clearance and skin bed preparation, a new paradigm. Aesthet Surg J. 2019;39(Suppl_3):S103–S111. doi:10.1093/asj/sjz022
13. Robinson DM, Frulla AP. Randomized, split-face/décolleté comparative trial of procedure enhancement system for fractional non-ablative laser resurfacing treatment. J Drugs Dermatol. 2017;16(7):707–710.
14. Nelson AM, Ortiz AE. Effects of anhydrous gel with TriHex peptides on healing after hybrid laser resurfacing. J Cosmet Dermatol. 2020;19(4):925–929. doi:10.1111/jocd.13270
15. Gold MH, Sensing W, Biron JA. A topical regimen improves skin healing and aesthetic outcomes when combined with a radiofrequency microneedling procedure. J Cosmet Dermatol. 2019;1–10. doi:10.1111/jocd.13037
16. Wang JV, Christman MP, Feng H, Ferzli G, Jeon H, Geronemus RG. Tripeptide and hexapeptide topical as adjunct to nonablative fractional resurfacing for photodamage: a randomized split-face trial. J Cosmet Dermatol. 2020;19:3245–3250. doi:10.1111/jocd.13795
17. McGuinn KP, Ross NA, Wang JV, Saedi N. Combination tripeptide/hexapeptide serum with 1540 nm nonablative fractional laser for the treatment of striae distensae: a pilot study. Skinmed. 2020;18(6):337–341. PMID: 33397562.
18. Wang JV, Hattier G, Saedi N. Tripeptide/hexapeptide topical in esthetics: evidence behind the skincare formulation. Skinmed. 2021;19(2):116–119. PMID: 33938433.
19. Garg S, Baveja S. Combination therapy in the management of atrophic acne scars. J Cutan Aesthet Surg. 2014;7:18–23. doi:10.4103/0974-2077.129964
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.