Back to Journals » International Journal of Women's Health » Volume 17
A Retrospective Study of Clinicopathological Features and Survival Outcomes in 305 Surgically Treated Patients with Stage IB–IIA Cervical Squamous Cell Carcinoma
Authors Huang L, Zeng W, Chen L, Liang Y, Lin H, Hou T
Received 12 May 2025
Accepted for publication 19 September 2025
Published 24 October 2025 Volume 2025:17 Pages 3855—3863
DOI https://doi.org/10.2147/IJWH.S529011
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Matteo Frigerio
Lishan Huang, Weihong Zeng, Li Chen, Ye Liang, Haihong Lin, Tao Hou
Department of Gynecology, Meizhou People’s Hospital, Meizhou City, Guangdong Province, 514031, People’s Republic of China
Correspondence: Tao Hou, Department of Gynecology, Meizhou People’s Hospital, Room 1101, Building 9, Yujing Dongfang Field, Meijiang District, Meizhou City, Guangdong Province, 514031, People’s Republic of China, Tel +86 15807535293, Email [email protected]
Objective: To investigate the clinicopathological characteristics and survival outcomes of 305 surgically treated patients with stage IB–IIA cervical squamous cell carcinoma (CSCC).
Methods: Clinical data of 305 CSCC patients treated at our hospital from March 2015 to December 2019 were retrospectively analyzed. Clinicopathological features were summarized, prognostic factors identified, and survival outcomes assessed using Kaplan–Meier and Cox regression analyses.
Results: The most common symptoms were irregular bleeding (49.8%) and contact vaginal bleeding (35.7%). Tumors < 4 cm accounted for 75.1%, and International Federation of Gynecology and Obstetrics (FIGO) stage IIA was more frequent than stage IB (52.8% vs 47.2%). Deep stromal invasion (≥ 1/2) and lymph node metastasis were observed in 75.7% and 19.3% of patients, respectively. Ovarian preservation occurred in 12.8% of cases. Postoperative adjuvant therapy was given in 79.3% of patients, with 41.3% receiving concurrent chemoradiotherapy. Lower apparent diffusion coefficient (ADC) values were significantly associated with higher FIGO stage, deeper invasion, lymph node metastasis, and more intensive adjuvant therapy (P< 0.05). The 3-year overall survival (OS) and disease-free survival (DFS) rates were 88.5% and 84.6%, respectively. Cox analysis identified FIGO stage, lymph node metastasis, depth of invasion, and adjuvant therapy as independent prognostic factors (P< 0.05). Kaplan–Meier analysis showed significantly lower OS in patients with FIGO stage IIA, deep invasion, lymph node metastasis, and no or single-modality adjuvant therapy.
Conclusion: The pathological features of patients with CSCC are closely associated with ADC values derived from diffusion-weighted imaging (DWI). Vaginal bleeding, depth of invasion, FIGO stage, postoperative treatment, and lymph node metastasis are key prognostic factors. Patients with stage IIa, lymph node metastasis, no adjuvant therapy, or invasion depth ≥ 1/2 have a poorer prognosis.
Keywords: cervical squamous cell carcinoma, Phase Ib~IIa, clinical pathology, prognosis
Introduction
Cervical cancer (CC) is a leading cause of death and disability among various gynecological diseases. In 2020, there were approximately 604,000 new cases and 342,000 deaths globally, with cervical squamous cell carcinoma (CSCC) being the most common pathological type, accounting for about 70%.1 Early screening and diagnosis of cervical cancer are of great significance. With technological advancements, diffusion-weighted imaging (DWI) has been increasingly applied in clinical practice, effectively compensating for the limitations of conventional MRI and providing detailed visualization of tumor invasion. Moreover, the quantitative parameter of DWI—the apparent diffusion coefficient (ADC) value—can effectively differentiate between lesion tissues and tumor subtypes.2 Although cervical squamous cell carcinoma (CSCC) incidence has decreased due to widespread screening and vaccination, challenges persist in improving treatment outcomes, even with effective early-stage therapies like surgery and adjuvant treatments.3 Novel approaches, such as immunotherapy and antibody-drug conjugates, offer new options for advanced disease.4 While the role of persistent human papillomavirus (HPV) infection in CSCC pathogenesis is well-established, further research is essential to uncover the molecular mechanisms driving disease progression and therapeutic resistance.5 The incidence of CSCC is showing a trend towards younger age groups due to increased societal pressure, early sexual debut (<16 years old), HPV infection, malnutrition, smoking, lifestyle changes, and higher levels of psychological stress, indicating a challenging situation for CSCC prevention and control.6 Currently, treatment methods for CSCC include radical surgery, chemotherapy, radiation therapy, etc. The maturation of comprehensive treatment techniques have improved outcomes, but some patients still do not receive effective and timely treatment, leading to recurrence, metastasis, and even death.7 Reports from the United States indicate a 3-year disease-free survival rate (DFS) of 87% for patients in stage Ia1-IIa1 who underwent surgical treatment;8 the 3-year overall survival rate (OS) after radical surgery for stage Ib2-IIa2 CSCC patients was 87.8%, with a DFS of 81.9%.9 Therefore, identifying risk factors that affect treatment outcomes is crucial for developing timely and appropriate treatment plans to reduce mortality. Based on this, this study analyzed the clinical data of 305 patients with stage Ib-IIa CSCC to further explore post-treatment influencing factors. Survival analysis of clinical and pathological parameters influencing the 3-year OS aims to provide assistance and reference value for the diagnosis and treatment of this disease.
Data and Methods
General Data
Data was collected from 305 CSCC patients in our hospital from March 2015 to December 2019. All patients were histologically confirmed, aged 21 to 71 years, with an average age of (49.83±10.66) years. Inclusion criteria: (1) complete clinical data; (2) Pathologically confirmed as FIGO 2018 stage Ib to IIa; (3) no history of treatment before admission; (4) no infectious diseases; (5) surgical treatment as the initial treatment. Exclusion criteria: (1) secondary CSCC; (2) severe organ failure; (3) pregnancy; (4) treatment abandonment, loss to follow-up, incomplete follow-up data; (5) abnormal coagulation function; (6) concurrent other malignant tumors. This study was approved by the Medical Ethics Committee of Meizhou People’s Hospital. See follow Figure 1.
 |
Figure 1 Flow chart of case screening. |
Research Methods
Clinical symptoms (such as irregular bleeding, abnormal discharge, etc.) and pathological data were collected, including age, tumor size (<4 cm, ≥4 cm), FIGO stage, depth of invasion (<1/2, ≥1/2), postoperative pathological examination results, lymph node metastasis (yes/no), and treatment modalities [surgical approach (radical hysterectomy: radical hysterectomy with pelvic lymph node dissection, pelvic lymph node dissection: biopsy-confirmed breast cancer metastasis to pelvic lymph nodes, with concurrent ovarian cancer or endometrial cancer, unilateral or bilateral salpingo-oophorectomy: Unilateral, Unilateral ovarian lesion, with a need to preserve fertility, and a strong patient preference to retain one ovary. Bilateral, Hormone receptor-positive breast cancer, high-risk premenopausal patients, inability to tolerate long-term medication, high genetic risk, need to reduce the risk of breast and ovarian cancer recurrence, and postmenopausal patients) and postoperative adjuvant therapy (Concurrent chemoradiotherapy refers to the simultaneous administration of radiotherapy and chemotherapy, typically indicated for patients with locally advanced disease who are unable to tolerate systemic chemotherapy. Single-modality radiotherapy or chemotherapy refers to the use of either radiotherapy or chemotherapy alone, typically for intermediate- to high-risk patients and those with lymph node metastasis; No adjuvant therapy: early-stage, low-risk patients)].
ADC Value Measurement
MRI Examination Method
All subjects underwent MRI examinations during the non-menstrual period. If an intrauterine device (IUD) was present, it was removed prior to the scan. Participants were instructed to drink 500 mL of warm water before the examination to ensure bladder filling. Imaging was performed using a GE 1.5T MRI scanner. After assisting the patient into the supine position, a routine scan was conducted, covering the region from the abdominal aortic bifurcation to the lower edge of the pubic symphysis. The scan parameters were set as follows: T1-weighted imaging (T1WI), axial plane: Field of view (FOV) 36×36 cm, matrix 320 × 224, echo time (TE) 7.4 ms, repetition time (TR) 600 ms, slice thickness 6 mm, interslice gap 1 mm. T2-weighted imaging (T2WI) and fat-suppressed T2 sequence: FOV 36×36 cm, matrix 320 × 224, TE 87.5 ms, TR 3820 ms, slice thickness 6 mm, interslice gap 1 mm.
DWI Examination
Patients were instructed on thoracic breathing techniques and asked to maintain even breathing. A spin-echo echo-planar imaging (SE-EPI) sequence was used with fat suppression achieved via a STIR sequence. Parameters were set as follows: 30 slices, FOV 385×385 cm, matrix 144 × 192, interslice gap 0.5 mm, TE 68 ms, TR 7500 ms, slice thickness 5 mm, acquisition time 180 seconds, and b-values of 800 s/mm² and 0 s/mm².
Image Processing
DWI and conventional MRI images were transferred to the corresponding workstation for processing. Artifacts were excluded, and only clear images were analyzed to obtain the ADC values.
Follow-Up Methods
During follow-up visits, tumor markers, pelvic MRI, chest X-ray, gynecological examination, etc, were performed. If necessary, local pathological biopsies, CT scans, MRI scans, and PET-CT scans were conducted. Overall survival (OS) was defined as CSCC-related death or last follow-up. Disease-free survival (DFS) was defined as the time from surgery until distant metastasis or local recurrence. All recurrences were confirmed through pathological examination. Follow-up is scheduled as follows: monthly check-ups during the first year after treatment, every three months during the second year, and every six months starting from the third year.
Statistical Analysis
Data were analyzed using SPSS 24.0 software. For quantitative data, the K–S test was used to check for normal distribution. If the data follows a normal distribution, it is expressed as ( ). The t-test was used for comparisons between two groups (age, tumor size, FIGO stage, depth of invasion, lymph node metastasis, HPV infection, cervical internal os, tumor morphology, surgical method), and one-way ANOVA was used for comparisons among three groups (adjuvant therapy). Count data (clinical presentation) were described as n (%). Survival curve analysis was conducted using the Kaplan-Meier method and Log rank test. Cox regression model was used to analyze prognostic factors for CSCC patients. A significance level of P<0.05 was considered statistically significant.
). The t-test was used for comparisons between two groups (age, tumor size, FIGO stage, depth of invasion, lymph node metastasis, HPV infection, cervical internal os, tumor morphology, surgical method), and one-way ANOVA was used for comparisons among three groups (adjuvant therapy). Count data (clinical presentation) were described as n (%). Survival curve analysis was conducted using the Kaplan-Meier method and Log rank test. Cox regression model was used to analyze prognostic factors for CSCC patients. A significance level of P<0.05 was considered statistically significant.
Results
Clinical Presentation of 305 CSCC Patients
The clinical presentations of the 305 CSCC patients in this group are shown in Table 1. The main symptoms were irregular bleeding (49.8%), followed by contact vaginal bleeding (35.7%).
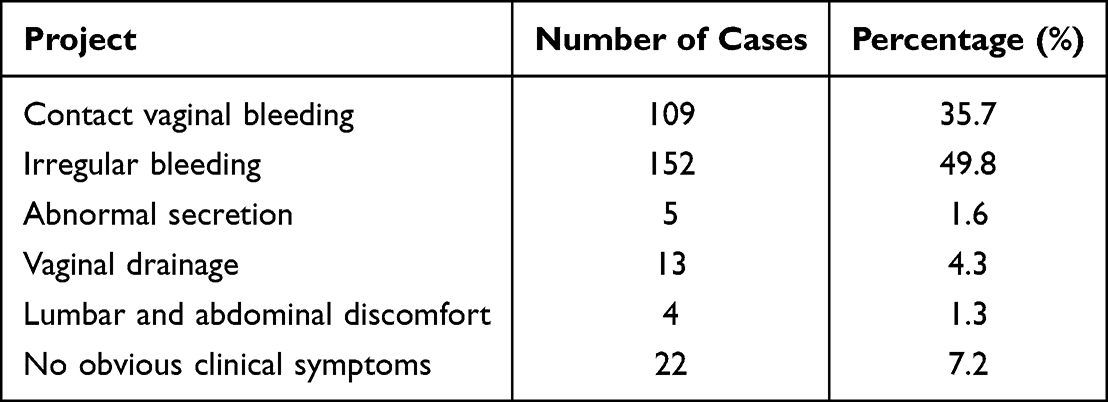 |
Table 1 Analysis of Clinical Manifestations of 305 Patients with CSCC |
Distribution of Clinical and Pathological Characteristics and ADC Values in 305 CSCC Patients
As shown in Table 2, among the main clinical and pathological characteristics, 183 cases (60.0%) had tumor size <4 cm, 192 cases (63.0%) were classified as FIGO stage Ib, and 113 cases (37.1%) were classified as stage IIa. Among them, 125 cases (41.0%) had invasion depth <1/2, while 180 cases (59.0%) had invasion depth ≥1/2, indicating a higher incidence of CSCC with invasion depth ≥1/2. Lymph node metastasis occurred in 91 cases (29.8%), while 214 cases (70.2%) had no lymph node metastasis, indicating a higher proportion of cases without lymph node metastasis. All 305 CSCC patients in this study underwent surgical treatment, with 79 cases (25.9%) preserving the ovaries and 226 cases (74.1%) undergoing bilateral oophorectomy. Postoperatively, adjuvant therapy was administered based on intermediate-risk factors, with 70 cases (23.0%) receiving no adjuvant therapy, 112 cases (36.7%) undergoing concurrent chemoradiotherapy, and 123 cases (40.3%) receiving single modality radiotherapy or chemotherapy. In terms of ADC values, FIGO stage Ib was lower than stage IIa (P<0.05); invasion depth ≥1/2 was lower than invasion depth <1/2 (P<0.05); lymph node metastasis was lower than no lymph node metastasis (P<0.05); concurrent chemoradiotherapy was lower than single-modality radiotherapy or chemotherapy and no adjuvant therapy (P<0.05).
 |
Table 2 Clinicopathologic Features of 305 Patients with CSCC |
Prognosis of 305 CSCC Patients
Cox regression analysis was performed with the 3-year mortality of CSCC patients (No = 0, Yes = 1) as the dependent variable, and the factors with significant differences in Table 2 as independent variables. During the follow-up period, a total of 35 patients died, resulting in a 3-year overall survival (OS) rate of 88.5% (See Figure 2A). Among them, 47 cases experienced recurrence or metastasis, including 16 cases of regional recurrence (bladder, pelvic lymph nodes), 9 cases of local recurrence in the vaginal stump, and 22 cases of distant metastasis (lung, bone, brain). The 3-year disease-free survival (DFS) rate was 84.6% (See Figure 2B).
 |
Figure 2 Progression-free survival and overall survival curves of 305 patients with CSCC. (A) OS; (B) DFS. |
Analysis of Factors Affecting Overall Survival Rate in 305 CSCC Patients
Univariate analysis and multivariate Cox regression analysis revealed that FIGO stage, lymph node metastasis, depth of invasion, and adjuvant therapy were independent factors affecting the 3-year overall survival rate in CSCC patients (P<0.05). See Table 3.
 |
Table 3 Univariate and Multivariate Analysis of Overall Survival of 305 Patients with CSCC |
Subgroup Analysis of Overall Survival Rate in CSCC Patients
Kaplan-Meier analysis showed that the 3-year OS rate of patients with FIGO stage Ib was significantly higher at 92.2% (177/192) compared to 82.3% (93/113) for stage IIa (Log rank χ2=6.985, P=0.008) (See Figure 3A). Patients with invasion depth <1/2 had a significantly higher 3-year OS rate of 93.6% (117/125) compared to 85.0% (153/180) for those with ≥1/2 invasion depth (Log rank χ2=5.077, P =0.024) (See Figure 3B). The 3-year OS rate for patients with lymph node metastasis was 79.1% (72/91), significantly lower than the 92.5% (198/214) for those without lymph node metastasis (Log rank χ2=11.521, P=0.001) (See Figure 3C). Regarding postoperative adjuvant therapy, the 3-year OS rate was 81.4% for patients without adjuvant chemotherapy, 87.0% for those receiving single modality radiotherapy or chemotherapy, and 94.6% for those undergoing concurrent chemoradiotherapy (Log rank χ2=7.854, P=0.020) (See Figure 3D).
 |
Figure 3 Subgroup analysis of overall survival in patients with CSCC. (A) FIGO stage; (B) Depth of infiltration; (C) Lymph node metastasis; (D) Postoperative adjuvant therapy. |
Discussion
Cervical cancer (CC) is the most common cancer in the female reproductive system, with approximately 250,000 deaths worldwide each year.10 Early screening and diagnosis of cervical cancer (CC) are of great significance. MRI is one of the commonly used diagnostic methods; however, conventional MRI has certain limitations in staging cervical cancer. With the development of MRI technology, Diffusion-Weighted Imaging (DWI) has become increasingly used in clinical practice, effectively overcoming the drawbacks of conventional MRI and providing detailed information about tumor invasion. DWI, primarily through directional indicators, can effectively assess cervical cancer. Tumor tissues have a higher tissue density than surrounding normal tissues, and factors such as changes in intracellular structures, reduced extracellular space, increased cell density, and elevated interstitial fluid pressure all significantly impact the diffusion of water molecules, leading to high DWI signals in tumors, while the ADC value decreases.11 The progression and prognosis of cervical cancer (CC) are closely related to tumor characteristics such as clinical staging, invasion depth, and lymph node metastasis. In this study, the apparent diffusion coefficient (ADC) values in FIGO stage Ib were lower than those in stage IIa; ADC values in tumors with an invasion depth ≥ 1/2 were lower than those with invasion depth < 1/2; ADC values were also lower in patients with lymph node metastasis compared to those without. Additionally, ADC values were lower in patients undergoing concurrent chemoradiotherapy than in those receiving single-modality chemoradiotherapy or no adjuvant therapy. Regression model analysis showed that lymph node metastasis, adjuvant therapy, FIGO stage, and invasion depth were independent prognostic factors for 3-year overall survival (OS) in patients with cervical squamous cell carcinoma (CSCC). These findings indicate that ADC values are associated with clinicopathological features and prognosis, suggesting that diffusion-weighted imaging (DWI) can partially assess the lesion details of CSCC and predict the prognosis of CC. Kang et al12 reported that age and tumor size are also clinicopathological factors influencing OS and disease-free survival (DFS) in CC patients. The differences between their results and ours may be due to variations in clinical staging, geographic regions, ethnicity, culture, and pathological types among the included cases.
Tabatabaei et al13 found that the 3-year overall survival (OS) of cervical squamous cell carcinoma (CSCC) was 78.2%, and the disease-free survival (DFS) was 62.7%, with FIGO stages ranging from I to IV. In China, a study of 833 patients with stages I b1 to IV who received radiotherapy and chemotherapy showed a 3-year OS of 84%.14 Other studies have also demonstrated that the 3-year DFS for patients with stages I a1 to II a1 who underwent surgical treatment was 87%,8 and for patients with stages I b1 to IV a, the 3-year DFS was 81%.15 In this study, a prognosis analysis of 305 patients with stages I b to II a CSCC revealed a 3-year OS of 88.52% and a 3-year DFS of 84.59%, which is similar to the aforementioned reports. FIGO stage reflects the severity of the disease and has a definite relationship with post-treatment prognosis. It has been widely used to predict the prognosis of cervical cancer patients. However, there are differences in prognosis among patients with different FIGO stages, and as FIGO stage increases, the 3-year OS of patients decreases.16
This study found through survival analysis that patients with FIGO stage I b had a significantly higher 3-year OS than those with stage II a, similar to the aforementioned studies. This indicates that postoperative care should be given special attention for patients with stage IIa CSCC, and for those with high-risk pathological factors, a reasonable and effective CCRT (concurrent chemoradiotherapy) treatment plan should be implemented. Lymph node metastasis is an important factor in CC spread, with an incidence rate of 17–33% in early CC. Early CC patients without lymph node metastasis have a 5-year overall survival (OS) rate as high as 90%, whereas those with lymph node metastasis have a 5-year OS of only 65%.17 This study found that patients without lymph node metastasis had a higher 3-year OS. Consistent with the above studies, invasion depth is related to lymph node extranodal extension and can reflect the extent and range of tumor cell infiltration to some degree. Therefore, assessing invasion depth is particularly important before formulating treatment plans.18 The standard treatment for cervical cancer (CC) mainly includes radical hysterectomy and concurrent chemoradiotherapy (CCRT) combined with adjuvant chemotherapy based on specific cases. Surgery is typically used for early clinical stages (Ia, Ib1, IIa1), small lesions, and fertility-preserving cases.19 Patients with one or more adverse histopathological factors (such as positive or close surgical margins, positive lymph nodes, or microscopic parametrial involvement) have a higher risk of recurrence.20 Compared with the adjuvant radiotherapy group, the adjuvant chemoradiotherapy group showed significant improvements in 4-year progression-free survival (PFS) (80% vs 63%) and 4-year overall survival (OS) (81% vs 71%).20 This study also found that patients with infiltration depth <1/2 had a higher OS than those with infiltration depth ≥1/2. The 3-year OS was 81.4% for patients without adjuvant chemotherapy, 87% for those who underwent single modality radiotherapy or chemotherapy, and 94.6% for CCRT patients, which is consistent with the above findings.
In conclusion, the pathological characteristics of CSCC patients are closely associated with their DWI parameter, the ADC value. This study found that the common manifestations were vaginal bleeding, and the factors influencing prognosis included depth of infiltration, FIGO staging, postoperative adjuvant treatment, and lymph node metastasis. Poor prognosis was observed in CSCC patients with stage II a, lymph node metastasis, no postoperative adjuvant treatment, and infiltration depth ≥1/2. However, the relatively small sample size and lack of multicenter validation in this study may limit the generalizability of the results. Future research will involve larger sample sizes and incorporate multicenter data to validate the findings, enabling more in-depth investigation of the related molecular mechanisms and enhancing the study’s originality.
Data Sharing Statement
The datasets used and analyzed during the present study are available from the corresponding author on reasonable request.
Ethics
This retrospective study was approved by the Medical Ethics Committee of Meizhou People’s Hospital (Approval No. 2025-C-27). The committee waived the requirement for individual informed consent due to the use of anonymized, routinely collected data and the retrospective nature of the study. All procedures were conducted in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Declaration of Helsinki and its later amendments.
Consent for Publication
All authors have reviewed and approved the final manuscript and consent to its publication.
Disclosure
Authors declared no conflict of interest.
References
1. Liu H, Xu R, C Gao, et al. Metabolic molecule PLA2G2D is a potential prognostic biomarker correlating with immune cell infiltration and the expression of immune checkpoint genes in cervical squamous cell carcinoma. Front Oncol. 2021;11:755668. doi:10.3389/fonc.2021.755668
2. Lura N, S Wagner-Larsenk, Ryste S, et al. Tumor ADC value predicts outcome and yields refined prognostication in uterine cervical cancer. Cancer Imaging. 2025;25(1):23. doi:10.1186/s40644-025-00828-6
3. Arbyn M, Weiderpass E, Bruni L, et al. Estimates of incidence and mortality of cervical cancer in 2018: a worldwide analysis. Lancet Glob Health. 2020;8(2):e191–e203. doi:10.1016/S2214-109X(19)30482-6
4. Tewari KS, Monk BJ. New strategies in advanced cervical cancer: from angiogenesis blockade to immunotherapy. Clin Cancer Res. 2014;20(21):5349–5358. doi:10.1158/1078-0432.CCR-14-1099
5. Cohen PA, Oaknin A, Jhingran A, et al. Cervical cancer. Lancet. 2019;393(10167):169–182. doi:10.1016/S0140-6736(18)32470-X
6. Beckmann MW, Stübs FA, C Kochm, et al. Diagnosis, therapy and follow-up of cervical cancer. guideline of the DGGG, DKG and DKH (S3-Level, AWMF Registry No. 032/033OL, May 2021) - Part 1 with recommendations on epidemiology, screening, diagnostics and therapy. Geburtshilfe Frauenheilkd. 2022;82(2):139–180. doi:10.1055/a-1671-2158
7. Xiu Y-T, Meng F-X, Wang Z, et al. Prognostic factors for IB2-IIIB cervical cancer patients treated by radiation therapy with high-dose-rate brachytherapy in a single-institution study [J]. J Contemp Brachyther. 2022;14(4):332–340. doi:10.5114/jcb.2022.118674
8. Amboree TL, Damgacioglu H, Sonawane K, et al. Recent trends in cervical cancer incidence, stage at diagnosis, and mortality according to county-level income in the United States, 2000-2019. Int J Cancer. 2024;154(9):1549–1555. doi:10.1002/ijc.34860
9. Jing H, Xiuhong W, Ying Y, et al. Neoadjuvant chemotherapy combined with radical surgery for stage IB2/IIA2 cervical squamous cell carcinoma: a prospective, randomized controlled study of 35 patients. World J Surg Oncol. 2021;19(1):209. doi:10.1186/s12957-021-02318-y
10. An Q, W Liu, Yang Y, et al. Preoperative fibrinogen-to-albumin ratio, a potential prognostic factor for patients with stage IB-IIA cervical cancer. BMC Cancer. 2020;20(1):691. doi:10.1186/s12885-020-07191-8
11. Ninkova RV, Calabrese A, Curti F, et al. The performance of the node reporting and data system 1.0 (Node-RADS) and DWI-MRI in staging patients with cervical carcinoma according to the new FIGO classification (2018). Radiol Med. 2024;129(7):1062–1075. doi:10.1007/s11547-024-01824-9
12. Kang S, Wu J, Li J, et al. Prognostic significance of clinicopathological factors influencing overall survival and event-free survival of patients with cervical cancer: a systematic review and meta-analysis. Med Sci Monit. 2022;28:e934588. doi:10.12659/MSM.934588
13. Tabatabaei F-S, Saeedian A, Azimi A, et al. Evaluation of survival rate and associated factors in patients with cervical cancer: a retrospective cohort study. J Res Health Sci. 2022;22(2):e00552. doi:10.34172/jrhs.2022.87
14. Wang W, X Liu, Meng Q, et al. Nomograms predicting survival and patterns of failure in patients with cervical cancer treated with concurrent chemoradiotherapy: a special focus on lymph nodes metastases. PLoS One. 2019;14(4):e0214498. doi:10.1371/journal.pone.0214498
15. Kawashima A, Isohashi F, Mabuchi S, et al. A 3-year follow-up study of radiotherapy using computed tomography-based image-guided brachytherapy for cervical cancer. J Radiat Res. 2019;60(2):264–269. doi:10.1093/jrr/rry104
16. Meng Q, Wang W, X Liu, et al. Nomograms predicting survival of cervical cancer patients treated with concurrent chemoradiotherapy based on the 2018 FIGO staging system. Front Oncol. 2022;12:870670. doi:10.3389/fonc.2022.870670
17. Ran C, Sun J, Qu Y, et al. Clinical value of MRI, serum SCCA, and CA125 levels in the diagnosis of lymph node metastasis and para-uterine infiltration in cervical cancer. World J Surg Oncol. 2021;19(1):343. doi:10.1186/s12957-021-02448-3
18. Jeong SY, Park H, Kim MS, et al. Pretreatment lymph node metastasis as a prognostic significance in cervical cancer: comparison between disease status. Cancer Res Treat. 2020;52(2):516–523. doi:10.4143/crt.2019.328
19. Zhou F, Tang X, Shao Z, et al. Radical surgery for stage IB2/IIA2 cervical cancer: a large retrospective study. Front Oncol. 2022;12:948298. doi:10.3389/fonc.2022.948298
20. Zhou Y, Rassy E, Coutte A, et al. Current standards in the management of early and locally advanced cervical cancer: update on the benefit of neoadjuvant/adjuvant strategies. Cancers. 2022;14(10):2449.
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.