Back to Journals » Clinical Ophthalmology » Volume 19
A Retrospective Data Analysis of Patients Treated with Difluprednate and Bromfenac for Cystoid Macular Edema After Uveitis or Cataract Surgery
Authors Shah N ![]() , Tran E
, Tran E ![]() , Caballero-Ortiz S
, Caballero-Ortiz S ![]() , Kyveris A, Chan T
, Kyveris A, Chan T
Received 9 April 2025
Accepted for publication 5 June 2025
Published 21 August 2025 Volume 2025:19 Pages 2879—2888
DOI https://doi.org/10.2147/OPTH.S516792
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Scott Fraser
Nirmit Shah,1,2 Edward Tran,2,3 Sandra Caballero-Ortiz,2 Angela Kyveris,2 Toby Chan2,4
1Melbourne Medical School, University of Melbourne, Melbourne, VIC, Australia; 2Ocular Health Centre, Kitchener, ON, Canada; 3Schulich School of Medicine, University of Western Ontario, London, ON, Canada; 4Michael G. DeGroote School of Medicine, McMaster University, Hamilton, ON, Canada
Correspondence: Toby Chan, Ocular Health Centre, 31 Kingsbury Dr Unit # 501, Kitchener, ON, N2A 0K5, Canada, Tel +1 519-208-8104, Email [email protected]
Purpose: Cystoid macular edema (CME) is a condition which severely limits central vision, often occurring secondary to cataract surgery or uveitis. Although commonly treated with non-steroidal anti-inflammatory agents and a corticosteroid adjunct, an optimal medication regime has not yet been evaluated. Hence, we present a comprehensive analysis of the efficacy and relapse rate associated with various agents to treat CME, such as Bromfenac and Difluprednate.
Patients and Methods: A retrospective chart review was conducted on patients aged 18 and above diagnosed with postoperative or uveitic CME via optical coherence tomography from January 1, 2016, to December 31, 2023. Among these eligible patients, we investigated those treated with non-steroidal anti-inflammatory drugs (NSAIDs) and/or corticosteroids. The primary outcome was the duration until complete resolution of CME. Secondary outcomes included improvement of CME and the likelihood of CME recurrence after treatment. Statistical analysis involved ANOVA and Tukey’s HSD test to compare treatment efficacy.
Results: A total of 518 patients were analyzed. Difluprednate and bromfenac (n = 28) demonstrated the shortest mean resolution time (1.45 months) compared to other combinations. The ANOVA test revealed significant differences among treatment groups (F-value: 6.455, P-value: < 0.00001), and Tukey’s HSD test showed that difluprednate and bromfenac significantly outperformed other medications in treating cystoid macular edema (CME) by reducing resolution times by 5.40 months compared to ketorolac alone (P = 0.0011), 4.76 months compared to ketorolac and prednisolone acetate (P = 0.0001), 5.42 months compared to loteprednol and nepafenac (P < 0.0001), 5.40 months compared to dexamethasone and nepafenac (P < 0.0001), and 4.47 months compared to no treatment (P = 0.0240). Difluprednate and bromfenac also had no cases of CME recurrence.
Conclusion: Difluprednate and bromfenac proved to be the most effective treatment regimen for cystoid macular edema (CME), resolving the condition in the shortest amount of time and requiring less frequent dosing.
Keywords: cystoid macular edema, bromfenac, difluprednate, uveitis, cataract surgery
Introduction
Cystoid macular edema (CME) is a prevalent condition characterized by retinal thickening of the macula due to the breakdown of the normal blood-retinal barrier.1 This pathological process results in the accumulation of fluid within the retinal layers, leading to cystic spaces that distort the photoreceptors architecture.1 The consequent retinal thickening and fluid collection can severely impair central vision, making CME a leading cause of vision loss in the developed world.2
The etiology of CME can be multifactorial; however, a prevalent risk factor is being postoperative from ocular surgery, most common being cataract surgery.3,4 Beyond surgical interventions, specific patient demographics, including those with uveitis, retinal vein occlusions, and diabetes, are at an elevated risk of developing CME due to the underlying inflammatory and vascular disruptions associated with these conditions.5–7
Managing CME involves using anti-inflammatory agents, specifically corticosteroids and non-steroidal anti-inflammatory drugs (NSAIDs). These medications aim to reduce the inflammation central to the pathogenesis of CME. In cases where the edema is secondary to another issue, steroids and NSAIDs act as adjunct medications while managing the source of the local inflammatory response. Patients with diabetes or retinal vein occlusion-induced CME are often given intravitreal injections such as anti-VEGF injections, while patients with infectious uveitis are given antivirals or antibacterials. However, CME induced by noninfectious uveitis and post-cataract surgery is similar, wherein no direct external source immediately prevents recovery. The patient may spontaneously resolve over time; however, local control of the inflammation limits the risk of any long-term deficits in visual acuity.5–9
Prednisolone, a potent corticosteroid, and Nepafenac (Nevanac®, Novartis AG, Switzerland), an NSAID, are the most commonly used combination to treat CME.10 Corticosteroids work by blocking phospholipase A2, which acts upstream on the cyclooxygenase pathway to produce prostaglandins. These prostaglandins increase vascular permeability and contribute to the formation of macular edema. NSAID’s work similarly, but act as a direct inhibitor to the cyclooxygenase pathway.11 Long-term administration of corticosteroids carries potential adverse effects, both local and systemic. Locally, it can increase intraocular pressure and promote cataract formation.12 Systemically, corticosteroid use can cause short-term complications such as hypertension, hyperglycemia, pancreatitis, and suppressed immunity, while long-term use may lead to osteoporosis, adrenal insufficiency, and growth suppression.13
The management of CME with prednisolone necessitates a prolonged and carefully monitored tapering schedule, often involving four-times-a-day dosing.10 This regimen can present significant challenges in terms of patient compliance and the overall management of the condition.14–16 Given these challenges, there is a continuous need to explore alternative therapies that are more potent and require less frequent dosing, which could simplify the tapering process and improve patient adherence.
Despite the established use of corticosteroid-NSAID combinations in treating CME, comprehensive studies on the effectiveness of various treatment regimens are insufficient. This gap underscores the need for rigorous clinical research to optimize CME management strategies, enhance therapeutic outcomes, and minimize adverse effects.
Methods
Data Sources
We performed a retrospective data analysis on all patients aged 18 and above who presented to our clinic with post-operative or noninfectious uveitic cystoid macular edema – as confirmed by OCT. These patients were identified using our centralized electronic medical record system (OSCAR Pro, 2001), in which a specific search template was generated to collate all patients with the terms “CME”, “ME”, “Macular Edema”, or “Cystoid Macular Edema” within their impression records between the dates January 1st, 2016 and December 31st, 2023.
Participant Screening
Participants who were identified as having any of the previously mentioned keywords within their impression notes were individually screened for eligibility. Our study population included those who were confirmed as having cystoid macular edema (CME) confirmed via optical coherence tomography. Specifically, those who presented with CME post cataract surgery or due to a complication of noninfectious uveitis and were put on either non-steroidal anti-inflammatory medication and/or corticosteroid medication. Patients were excluded if they presented with a cause of CME outside the two previously mentioned cases, such as retinal vein occlusion; or if they had a previous history of ocular conditions which could influence their outcome – such as an outer retinal layer condition. Additionally, patients were excluded if they were put on a medication course other than nonsteroidal anti-inflammatory medication and/or corticosteroid medication. Patients on medications such as systemic steroids or immunomodulators that may have impacted on the efficacy of the topicals were also excluded. Finally, if OCT images were not taken at diagnosis and resolution or the last visit date before medication cessation – they were also excluded. Patients were followed up from the index date, defined as the first prescribing date for any medications of interest, until discharge from clinical care.
Ethics Review
Patients identified as eligible were contacted for consent procedures via telephone. Potential risks and benefits for this study were outlined in the discussion, and patients were allowed to review a consent form, which was sent to them via hard or soft copy prior to final consent. Prior consent to contact for research purposes was deemed at patient intake into our clinic. Consent forms for this study were developed in conjunction with ADVARRA, the REB responsible for ethical oversight of this study. Our study complies with the declaration of Helsinki. Before study initiation, this study was submitted for ethics approval to the ADVARRA board. Single-site study approval was granted on October 9th, 2023 (PRO00074231). Patients who could not be contacted for research consent or declined to consent were deemed ineligible for our study.
Primary Outcome
Our primary outcome will be assessment of treatment with either non-steroidal anti-inflammatory medications and/or corticosteroid medication. The focus will be the duration of medication treatment, defined as the time from the index date to discharge of clinical care. During this period, changes in macular edema will be classified as resolved (Figure 1), improved but not resolved, unchanged, or worsened. Classifications will be made on clinician analysis of OCT images; wherein changes on OCT images will be compared between index and discharge date. If residual edema remained after a trial of medication despite improvement when compared to baseline, they were classified as improved but not resolved (Figure 2).
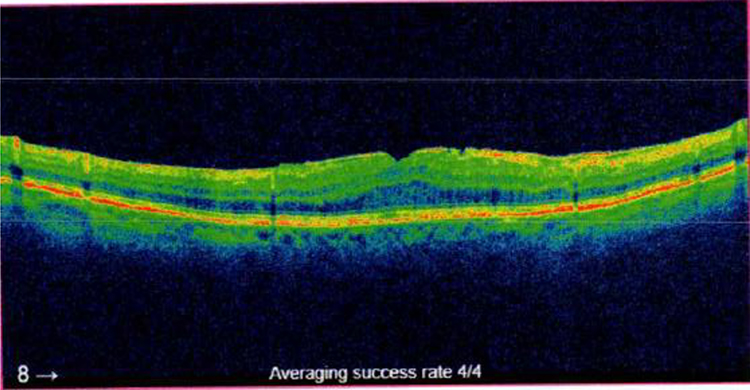 |
Figure 1 Normal OCT Image, with absence of edema and considered as resolved after treatment. |
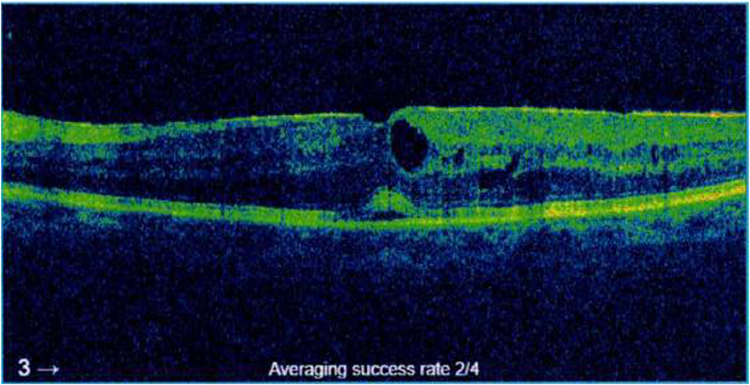 |
Figure 2 OCT Image of a patient classified as improved but not resolved, present with less edema than at baseline, but not completely absent. |
Other Outcomes
Other outcomes assessed will be the variation of recurrence within patients and its association with treatment. If patients who underwent full resolution or improvement without full resolution presented back to our clinic and were subsequently diagnosed with CME, which was worse than at the date of discharge – they were identified as a case of recurrence. Additionally, we will assess the proportion of cases of resolution leading to each classification outcome within each treatment arm.
Patient Characteristics
Patient characteristics such as age, sex, medication(s) of interest, central macular thickness, and diagnosis were collected at baseline. Outcome details such as duration, response, and recurrence were also identified within the datasheet. Patients who underwent the same treatment regime were then collated for the purposes of statistical analysis.
Statistical Analysis
Statistical analyses were conducted using Python 3.8.5 with libraries including pandas 1.1.3, NumPy 1.19.2, SciPy 1.5.2, and statsmodels 0.12.1. Data were imported into Python using pandas and cleaned to remove missing or outlier values. Descriptive statistics such as means, standard deviations, and frequencies were calculated using pandas and NumPy. An analysis of variance (ANOVA) was conducted using the anova_lm function from the statsmodels library to compare mean resolution times across different treatment groups. Post-hoc comparisons were performed using Tukey’s Honest Significant Difference (HSD) test via the pairwise_tukeyhsd function from the statsmodels library. Odds ratios were calculated using the odds_ratio function from the statsmodels library. All analyses were conducted in a reproducible manner with code and data available upon request.
We focus on patient demographics, treatment outcomes including mean resolution time; mean improvement time’ improvement rate and odds; and recurrence rate and odds. Descriptive statistics were conducted on patient demographics. Treatment efficacy was assessed by evaluating the mean resolution and improvement times across different medication regimens using an analysis of variance (ANOVA) test. Post-hoc comparisons were performed using Tukey’s Honest Significant Difference (HSD) test to identify significant differences between treatment groups. Secondary outcomes, such as recurrence and resolution rates, were analyzed using odds ratios to compare the likelihood of these events across treatment arms. This comprehensive approach allowed for a detailed examination of the effectiveness of various medications in treating cystoid macular edema (CME).
Results
Demographic Statistics (Table 1)
A total of 518 patients with cystoid macular edema (CME) were analyzed, with a mean age of 73.27 ± 12.87 years. The average time to resolution of CME was 5.7 ± 4.71 months. The cohort comprised 258 females and 260 males. Of these, 292 cases of CME were postoperative complications from cataract surgery, and 226 were due to uveitis. A post-hoc comparison using Tukey’s Honest Significant Difference test confirmed there were no significant differences between mean central macular thickness of groups at baseline (Table 2). The maximum baseline central macular thickness was 655μm (Figure 3). Since both diagnoses had identical treatment regimens and a similar pathophysiology, there was no impact on results based on diagnosis alone. The most commonly used medications for CME included nepafenac and prednisolone acetate (n = 127), ketorolac and prednisolone acetate (n = 57), dexamethasone and nepafenac (n = 55), and nepafenac alone (n = 35). Of the total cases, 307 resolved completely, 181 showed improvement without full resolution, 29 worsened, and 1 remained unchanged.
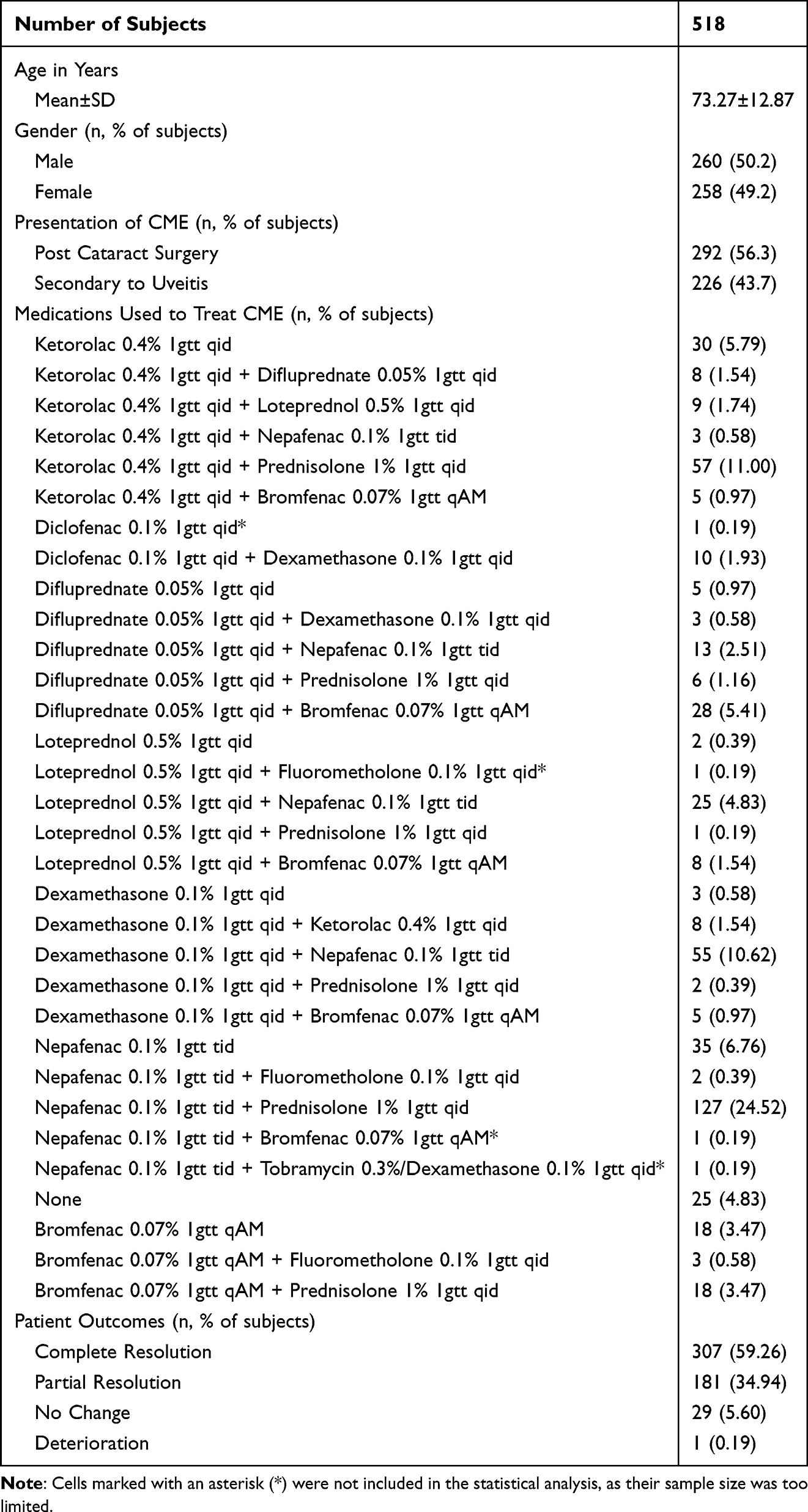 |
Table 1 Demographics and Characteristics of Study Population |
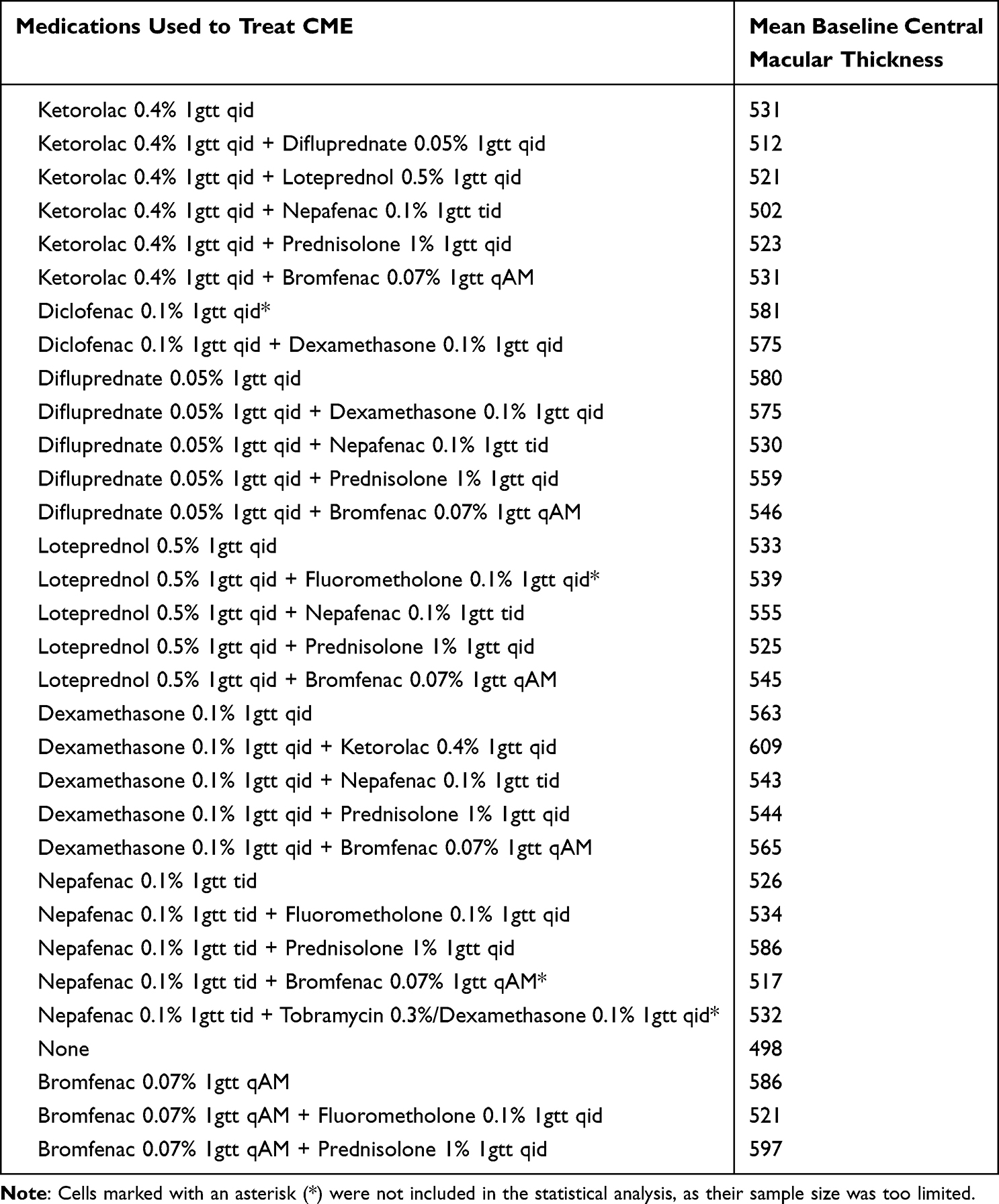 |
Table 2 Mean Baseline Central Macular Thickness of Groups Treated for Cystoid Macular Edema |
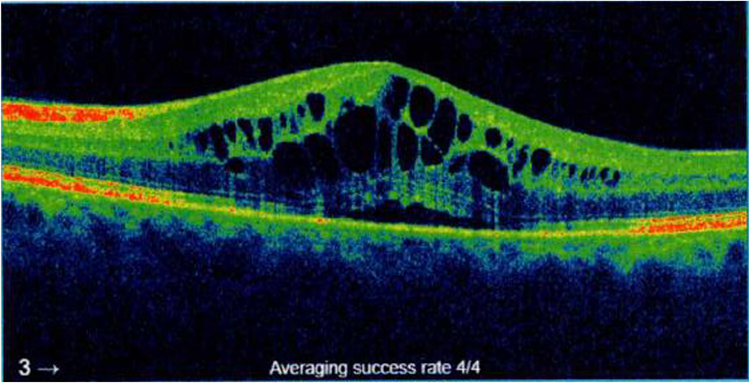 |
Figure 3 Pathological OCT Image, present with edema and a maximum central macular thickness of 655μm. |
Mean Resolution Time (Figure 4)
Looking at the cohort of patients whose CME resolved, we found that difluprednate and bromfenac had the shortest mean resolution time. Difluprednate and bromfenac (n = 28) had a mean resolution time of 1.45 months. In comparison, nepafenac and prednisolone acetate (n = 92), the most frequently used combination, had a resolution time of 6.93 months. Ketorolac and prednisolone acetate (n = 29), had a resolution time of 6.21 months. Similarly, dexamethasone and nepafenac (n = 26) also show a prolonged resolution time of 6.85 months.
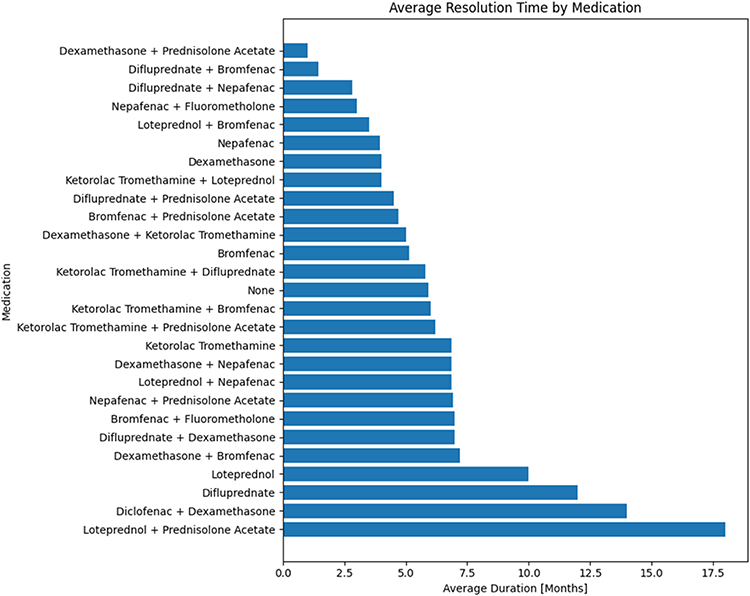 |
Figure 4 Average Time to Complete Resolution of Cystoid Macular Edema (in months) for Each Medication. |
An analysis of variance (ANOVA) test was performed to assess the differences in mean resolution times among various medication regimens for CME. The results indicated significant variance among the treatment groups (F-value: 6.455, P-value: <0.00001), suggesting differences in medication efficacy. A post-hoc comparison using Tukey’s Honest Significant Difference (HSD) test further elucidated these differences. Difluprednate and bromfenac significantly outperformed other medications in treating cystoid macular edema (CME). Specifically, they reduced the resolution time by 5.40 months compared to ketorolac alone (P = 0.0011) and were more effective than the combination of ketorolac and prednisolone acetate, with a decrease of 4.76 months (P = 0.0001). Additionally, difluprednate and bromfenac showed further efficacy by reducing resolution times by 5.42 months compared to loteprednol and nepafenac (P < 0.0001), by 5.40 months compared to dexamethasone and nepafenac (P < 0.0001), and by 4.47 months compared to no treatment (P = 0.0240).
Mean Improvement Time (Figure 5)
Looking at the cohort of the improved CME, we found that difluprednate and bromfenac (n = 28) showed a mean improvement time of 1.45 months. Nepafenac and prednisolone acetate (n = 126), the most commonly used treatment regimen, had a longer resolution time of 6.35 months. Similarly, dexamethasone and nepafenac (n = 53) exhibited an even longer resolution period of 6.55 months. Ketorolac and prednisolone acetate (n = 52) presented a resolution time of 6.77 months.
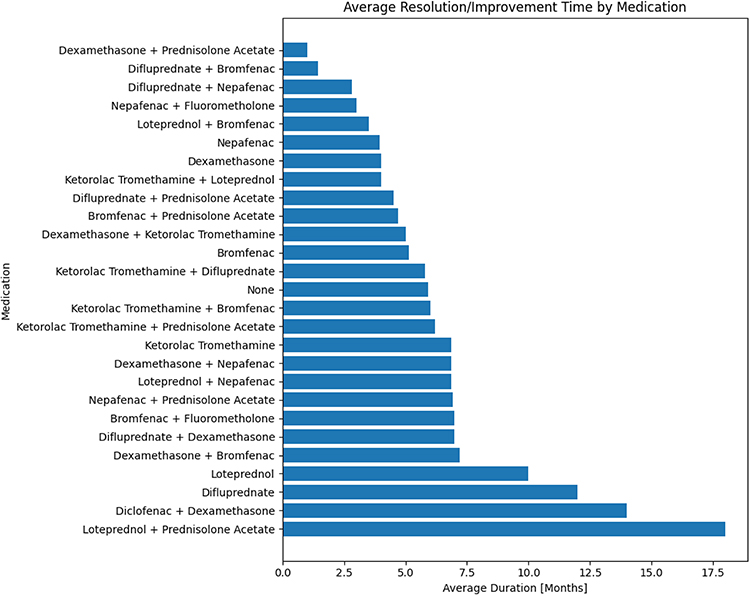 |
Figure 5 Average Time to Initial Symptom Improvement of Cystoid Macular Edema for Different Medications. |
An ANOVA test was performed to assess the differences in mean improvement times among various treatments for CME. The results indicated significant variance among the treatment groups (F-value: 6.455, P-value: <0.00001), highlighting differences in medication efficacy. A post-hoc comparison using Tukey’s Honest Significant Difference (HSD) test further clarified these differences. Specifically, difluprednate and bromfenac significantly outperformed other medications. Comparisons showed that difluprednate and bromfenac reduced the resolution time more effectively compared to ketorolac and prednisolone acetate by 5.32 months (p < 0.0001), to loteprednol and nepafenac by 4.51 months (p = 0.005), to dexamethasone and nepafenac by 5.10 months (p < 0.0001), and to nepafenac and prednisolone acetate by 4.90 months (p < 0.0001).
Improvement Rate and Odds
Difluprednate and bromfenac (n = 28) demonstrated a 100% resolution rate. Nepafenac and prednisolone acetate (n = 127) also showed a high-resolution rate of 72.44% with an odds ratio of 2.57. Dexamethasone and nepafenac (n = 55) demonstrated a resolution rate of 47.27% and odds ratio of 0.89. Ketorolac and prednisolone acetate (n = 57) reported a resolution rate of 50.88% and odds ratio of 1.04. In comparison, ketorolac alone (n = 29) showed a resolution rate of 44.83% with an odds ratio of 0.82.
Recurrence Rate and Odds
There were 204 instances of CME recurrence. Difluprednate and Bromfenac (n = 28) showed no recurrence of CME. No treatment (n = 25) showed a recurrence rate of 16.0% and an odds ratio of 0.19. Nepafenac and prednisolone acetate (n = 127) displayed a recurrence rate of 40.2% with an odds ratio of 0.67. Dexamethasone and nepafenac (n = 55) also showed a considerable recurrence rate of 47.27% and an odds ratio of 0.89. Ketorolac and prednisolone acetate (n = 57) reported a recurrence rate of 45.61% with an odds ratio of 0.85. Ketorolac alone (n = 30) had a high recurrence rate of 56.67% and an odds ratio of 1.33.
Discussion
CME is a condition that can hinder visual acuity and is often seen as a complication due to uveitis or post-cataract surgery.3–7 While the standard of care for patients with CME is a combination of NSAID and corticosteroid, some clinicians choose to use alternative treatment regimes.8,9 In some cases, usage of an NSAID and corticosteroid combination can be eliminated entirely – such as in the case of retinal vein occlusions, which are treated via anti-VEGF intravitreal injections.17 However, our focus was to compare the efficacy of standard-of-care prednisolone and nepafenac – the most commonly utilized dual therapy treatment for uveitic and post-cataract surgery-induced macular edema.
To our knowledge, there has not yet been a large-scale study that compares the efficacy of different treatment combinations. Furthermore, no study assessed the combination of difluprednate and bromfenac – two medications that have independently been suggested as monotherapeutic first-line for treating and preventing CME.18,19 There have only been two documented cases of resolution from macular edema when treated with dual therapy of difluprednate and bromfenac.20,21 Therefore, we aimed to bridge the gap between literature documenting this dual therapy’s success and comparing different medication regimes to treat macular edema by retrospectively analyzing all of our eligible patients who received various regimes, and were documented in our electronic medical record.
Our findings suggested that dual therapy of Difluprednate and Bromfenac offered the most effective solution for resolving CME of all medication combinations assessed. Its mean resolution time of 1.45 months was significantly lower than all other medication regimes, especially the current standard of care Prednisolone and Nepafenac, which had a mean resolution time of 6.85 months. Additionally, improvement odds while on Difluprednate and Bromfenac were significantly higher than any other combination, while the odds of recurrence were also considerably lower. Overall, our findings showed that Difluprednate and Bromfenac should be assessed as the current first-line treatment for uveitic and/or post-cataract surgery cystoid macular edema. We propose that the major reason for improved recovery from CME is due to the reduced number of drops required for administration each day. Given that Bromfenac is only dosed at one drop per day verses three drops per day of Nepafenac, it is likely that patients are much more compliant with this regimen, due to its ease and efficacy. Additionally, there is some evidence which suggests that difluprednate may be more effective than prednisolone at controlling inflammation – supporting its superior efficacy at managing CME when combined with an NSAID.22
Our study still has significant limitations. Since this study was retrospectively completed based on electronic medical data, several key pieces of information could not be collected. Mainly, changes in visual acuity. Although visual acuity was assessed in consultation when deciding whether to discontinue a medication, these values were not collected as part of our study. A comprehensive list of medications that may have influenced patients’ overall outcomes were not collected. Other confounding variables, such as race and OCT parameters such as IS/OS segmentation were also not accounted for. Finally, due to irregularities in medication supply, there are drastically different sample sizes of medication combinations between each treatment arm.
Although patient factors highly influence the outcome of any treatment regime, the current standard of care for CME forces patients to be on potentially harmful medications for extended periods. Therefore, it is prudent to find a more optimal way of treating these patients so they are not forced to stay on these medications for long durations. We hope that in creating this manuscript, we take one step closer to finding the most efficient way to treat patients presenting with uveitic or post cataract surgery-induced cystoid macular edema.
Conclusion
Despite the limitations of our study, this piece of evidence represents the first documented study which compared various combinations of medications for the treatment of uveitic and post-cataract surgery cystoid macular edema. Moreover, it represents the first case in which a systematic assessment of Difluprednate and Bromfenac demonstrated efficacy as a dual therapy treatment. Future research should aim to have more stringent data collection, with retrospective data analysis focusing on the collection of visual acuity, race, concomitant medications, and other confounding variables. Prospective studies should aim to directly compare the efficacy of these medications, possibly in the form of a randomized control trial, with equivalent sample sizes between treatment arms.
Funding
This work was not supported by any external, internal, or scholarship grants.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Gass JD, Norton EW. Follow-up study of cystoid macular edema following cataract extraction. Trans Am Acad Ophthalmol Otolaryngol. 1969;73:665–682.
2. Hogan P, Dall T, Nikolov P. American diabetes association: economic costs of diabetes in the US in 2002. Diabetes Care. 2003;26:917–932.
3. Chu CJ, Johnston RL, Buscombe C, et al. Risk factors and incidence of macular edema after cataract surgery. Ophthalmology. 2016;123:316–323. doi:10.1016/j.ophtha.2015.10.001
4. Loewenstein A, Zur D. Postsurgical cystoid macular edema. Dev Ophthalmol. 2017;58:178–190. doi:10.1159/000455280
5. Jonas JB, Kreissig I, Degenring RF. Intravitreal triamcinolone acetonide as treatment of macular edema in central retinal vein occlusion. Graefes Arch Clin Exp Ophthalmol. 2002;240:782–783. doi:10.1007/s00417-002-0529-0
6. Řehák J, Rehák M. Branch retinal vein occlusion: pathogenesis, visual prognosis, and treatment modalities. Curr Eye Res. 2008;33(2):111–131. doi:10.1080/02713680701851902
7. Shelsta H, Jampol L. Pharmacologic therapy of pseudophakic cystoid macular edema. Retina. 2011;31(1):4–12. doi:10.1097/iae.0b013e3181fd9740
8. Zur D, Fischer N, Tufail A, Monés J, Loewenstein A. Postsurgical cystoid macular edema. Eur J Ophthalmol. 2011;21(6_suppl):62–68. doi:10.5301/ejo.2010.6058
9. Kim S, Schoenberger S, Thorne J, Ehlers J, Yeh S, Bakri S. Topical nonsteroidal anti-inflammatory drugs and cataract surgery. Ophthalmology. 2015;122(11):2159–2168. doi:10.1016/j.ophtha.2015.05.014
10. Hariprasad SM, Akduman L, Clever JA, Ober M, Recchia FM, Mieler WF. Treatment of cystoid macular edema with the new-generation NSAID nepafenac 0.1%. Clin Ophthalmol. 2009;3:147–154. PMID: 19668559; PMCID: PMC2709014. doi:10.2147/opth.s4684
11. Guo S, Patel S, Baumrind B, et al. Management of pseudophakic cystoid macular edema. Surv Ophthalmol. 2015;60(2):123–137. doi:10.1016/j.survophthal.2014.08.005
12. Manabe S, Bucala R, Cerami A. Nonenzymatic addition of glucocorticoids to lens proteins in steroid-induced cataracts. J Clin Invest. 1984;74(5):1803–1810. doi:10.1172/JCI111599
13. Buchman AL. Side effects of corticosteroid therapy. J Clin Gastroenterol. 2001;33(4):289–294. PMID: 11588541. doi:10.1097/00004836-200110000-00006
14. Green EKY, McGrath O, Steeples L, Ashworth JL. Monitoring compliance to topical therapy in children and young people with uveitis. Eye. 2024;38(3):572–577. PMID: 37932371; PMCID: PMC10858091. doi:10.1038/s41433-023-02736-0
15. Olthoff CM, Schouten JS, van de Borne BW, Webers CA. Noncompliance with ocular hypotensive treatment in patients with glaucoma or ocular hypertension: an evidence-based review. Ophthalmology. 2005;112:953–61.e7. doi:10.1016/j.ophtha.2004.12.03
16. Dreer LE, Girkin C, Mansberger SL. Determinants of medication adherence to topical glaucoma therapy. J Glaucoma. 2012;21:234. doi:10.1097/IJG.0b013e31821dac86
17. Campa C, Alivernini G, Bolletta E, Parodi MB, Perri P. Anti-VEGF Therapy for Retinal Vein Occlusions. Curr Drug Targets. 2016;17(3):328–336. doi:10.2174/1573399811666150615151324
18. Sheppard JD. Topical bromfenac for prevention and treatment of cystoid macular edema following cataract surgery: a review. Clin Ophthalmol. 2016;10:2099–2111. doi:10.2147/OPTH.S86971
19. Koronis S, Stavrakas P, Balidis M, Kozeis N, Tranos PG. Update in treatment of uveitic macular edema. Drug Des Devel Ther. 2019;13:667–680. doi:10.2147/DDDT.S166092
20. Mali J. Changing the game in treatment of acute pseudophakic CME. Ophthalmol Times. 2017;42(12):1.
21. Nguyen KH, Smith AK, Kim BT, Browne AW. A case report of cystoid macular edema, uveitis and vitreomacular traction in a patient taking Anastrozole. Am J Ophthalmol Case Rep. 2022;25:101339. doi:10.1016/j.ajoc.2022.101339
22. KhalafAllah MT, Basiony A, Salama A. Difluprednate versus prednisolone acetate after cataract surgery: a systematic review and meta-analysis. BMJ Open. 2019;9(11):e026752. doi:10.1136/bmjopen-2018-026752
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.