Back to Journals » Clinical Interventions in Aging » Volume 20
A Retrospective Comparative Analysis of Transforaminal Epidural Steroid Injections and Percutaneous Transforaminal Endoscopic Discectomy for Managing Lumbar Radiculopathy in Super Elderly Patients
Authors Zhou J, Hu A, Zhou X, Dong J
Received 29 September 2025
Accepted for publication 21 December 2025
Published 31 December 2025 Volume 2025:20 Pages 2749—2761
DOI https://doi.org/10.2147/CIA.S566242
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Zhi-Ying Wu
Jian Zhou,* An’nan Hu,* Xiaogang Zhou, Jian Dong
Department of Orthopaedic Surgery, Zhongshan Hospital, Fudan University, Shanghai, 200032, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Jian Dong, Department of Orthopaedic Surgery, Zhongshan Hospital, Fudan University, 180 Fenglin Road, Shanghai, 200032, People’s Republic of China, Tel +86-21-64041990, Fax +86-21-64432673, Email [email protected] Xiaogang Zhou, Department of Orthopaedic Surgery, Zhongshan Hospital, Fudan University, 180 Fenglin Road, Shanghai, 200032, People’s Republic of China, Tel +86-21-64041990, Fax +86-21-64432673, Email [email protected]
Purpose: The rising global population aged over 80 has increased the incidence of degenerative spinal conditions causing lumbar radiculopathy. Minimally invasive treatments such as transforaminal epidural steroid injection (TESI) and percutaneous transforaminal endoscopic discectomy (PTED) are commonly used, yet their comparative effectiveness remains unclear. This study aimed to compare the clinical outcomes, safety, and efficacy of TESI and PTED in patients aged 80 and above.
Patients and Methods: : A retrospective analysis was conducted on 74 patients with conservative treatment-resistant lumbar radiculopathy. Patients were divided into TESI (n=40) and PTED (n=34) groups. Primary outcomes included Visual Analog Scale scores for back and leg pain (VAS-BP, VAS-LP), Oswestry Disability Index (ODI), and modified MacNab criteria. Secondary outcomes were operative time, fluoroscopy frequency, hospital stay, and complications. Assessments occurred preoperatively and at 1 week, 1, 3, 6, and 12 months post-procedure. Statistical analyses used ANOVA and chi-square tests.
Results: Both groups showed significant short-term improvement. At 6- and 12-month follow-ups, the PTED group demonstrated superior and sustained outcomes, with greater pain reduction (VAS-BP, VAS-LP), better functional improvement (ODI), and higher excellent/good MacNab rates (87.9% vs 64.9%, p< 0.05) compared to TESI. The TESI group had a higher recurrence rate (21.62% vs 6.06%). TESI was associated with shorter procedure times and hospital stays. No serious complications occurred in either group.
Conclusion: Both TESI and PTED are effective minimally invasive treatments for lumbar radiculopathy in very elderly patients. TESI offers quicker procedures and rapid symptom relief, while PTED provides more durable pain reduction and functional improvement. Treatment plans should be tailored to each individual, in accordance with established geriatric care principles that emphasize the consideration of comorbid conditions, specific pathology, and patient preferences. Further prospective randomized studies are needed to confirm these results.
Keywords: super elderly, lumbar radiculopathy, transforaminal epidural steroid injection, TESI, percutaneous transforaminal endoscopic discectomy, PTED, less invasive, treatment outcomes
Introduction
The aging population is a worldwide issue. According to the World Health Organization, by 2030, approximately one in six individuals globally will be 60 years or older. Additionally, the demographic of those aged 80 and above is projected to increase threefold from 2020 to 2050, reaching 426 million.1 As the population ages, there is a growing prevalence of degenerative spinal disorders, such as spinal stenosis, degenerative disc disease, and adult spinal deformities.2,3 In older adults, lumbar radiculopathy resulting from disc herniation or foraminal stenosis can cause severe pain and diminish quality of life. Therefore, it is essential to find effective treatments that improve the well-being of these patients.4 When conservative approaches, both non-drug and drug-based, do not yield results, more invasive options are explored.5 The frequency of spinal surgeries among older adults is increasing.6 At the same time, aging is associated with a rise in both the incidence and severity of various underlying health issues, which significantly heightens surgical risks.7 Thus, ensuring a balance between effectiveness and safety is particularly critical for older patients, especially those with pre-existing conditions like coronary heart disease, diabetes, hypertension, and chronic obstructive pulmonary disease. These concerns are particularly pronounced in the “super elderly” (≥80 years), who frequently exhibit elevated rates of multisystem comorbidities, polypharmacy, diminished physiological reserve, and frailty. Collectively, these factors amplify the risks associated with surgical interventions and complicate perioperative management.8,9
The best approach to enhance the quality of life for this age group, especially in terms of balancing effectiveness and safety, is still a topic of debate. Some research has shown positive results from spinal surgeries in older adults,9,10 while other studies suggest that those with worse physical health or multiple health issues experience lower satisfaction after spinal fusion.11 Deyo et al found an 18% complication rate in patients aged 75 and above who underwent lumbar spinal surgery.12 Additionally, Johnsson and his team advised that conservative management might be preferable to surgical options for elderly individuals with lumbar disc herniation, as only a few developed significant complications over a four-year follow-up period.13
Over the past few decades, the advent of minimally invasive methods has transformed the approach to spinal disorders, providing advantages like decreased blood loss, quicker recovery times, and a lower incidence of postoperative complications.14,15 These methods can be divided into two main types: non-surgical minimally invasive techniques and surgical options. One commonly used non-surgical technique is the transforaminal epidural steroid injection (TESI), which effectively alleviates radiculopathy symptoms. This procedure enables the precise administration of corticosteroids into the anterior epidural space, helping to diminish inflammation and alter pain perception.16 TESI has proven to be a reliable and efficient solution for lumbar radiculopathy, with a minimal risk of adverse effects.17,18 Another notable minimally invasive surgical option is the percutaneous transforaminal endoscopic lumbar discectomy (PTED), which is recognized for its benefits, such as a small incision, reduced hospital stay, and low rates of surgical complications.19
Earlier research has indicated that both TESI and PTED are relatively safe and minimally invasive options for addressing lumbar radiculopathy in younger elderly populations, typically comprising patients aged 65 to 79 years.20,21 However, robust evidence specifically focusing on the “super elderly” (≥80 years) remains limited, and the generalizability of findings from younger cohorts to this distinct, frailer population is uncertain. To our knowledge, there has been no direct comparison of the clinical effectiveness of TESI and PTED specifically for patients over 80 years old with lumbar radiculopathy. Therefore, we initiated a retrospective comparative study aimed at assessing the clinical results of these two distinct minimally invasive procedures in treating lumbar radiculopathy among this age group.
Materials and Methods
The Institutional Ethics Committee of Zhongshan Hospital, Fudan University approved this retrospective and comparative clinical study (approval number 2020–130). All participants provided written informed consent prior to enrollment, and the study was conducted in accordance with the principles of the Declaration of Helsinki.
Patient Population
From July 2021 to June 2023, individuals over the age of 80 who experienced lumbar radiculopathy due to disc herniation or foraminal stenosis were enrolled at our facility. The criteria for inclusion included: (1) imaging results indicating single-level disc herniation or foraminal stenosis between L2/3 and L5/S1, with or without accompanying low back pain; (2) unsuccessful attempts at conservative treatments, both non-pharmacological and pharmacological, for a minimum of six weeks; (3) voluntary agreement to participate, confirmed by signed informed consent; and (4) a follow-up duration of at least one year. Exclusion criteria encompassed: (1) inconsistencies between imaging results and clinical symptoms; (2) significant motor deficits or cauda equina syndrome; (3) lumbar spondylolisthesis or instability; (4) other lumbar conditions such as trauma, tumors, or infections; and (5) prior lumbar surgeries, mental or intellectual disorders, infections, communication issues, or incomplete initial data. Ultimately, 74 patients met the study’s criteria. Radiological assessments were conducted using magnetic resonance imaging (MRI), three-dimensional computed tomography (CT), and lumbar spine X-rays. Based on the imaging findings, the pathological causes of nerve root compression were classified into three categories: (1) Bony Foraminal Stenosis (FS), primarily resulting from superior articular process hypertrophy, facet osteophytosis, or ligamentum flavum hypertrophy, without a predominant soft disc component; (2) Soft Lumbar Disc Herniation (LDH), where a herniated nucleus pulposus causes compression in the lateral recess (subarticular stenosis) or foramen (far-lateral herniation); and (3) Mixed Pathology, which features both bony stenosis and disc herniation, often presenting as a hard or calcified herniated disc. The patients were then retrospectively divided into two treatment groups: the TESI group, consisting of 40 patients, and the PTED group, which included 34 patients (Figure 1). Notably, patients in the PTED group did not receive any prior TESI treatment, and the groups were mutually exclusive to ensure distinct cohort comparisons.
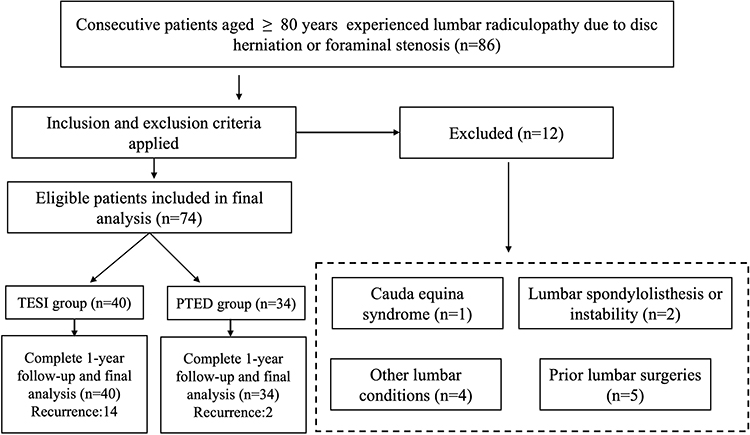 |
Figure 1 Patient inclusion and exclusion flowchart. |
Surgical Technique
All procedures were performed by the same senior surgeon.
TESI
The patient was laid face down on a carbon fiber table within the surgical suite. The operation was guided by a mobile C-arm fluoroscope from United Imaging Healthcare Co., Ltd. in Shanghai, China. Prior to the procedure, the access route was strategically planned using a posterolateral technique through Kambin’s triangle. Following sterilization and draping, local anesthesia was administered with 0.5% bupivacaine HCl. The entry point on the skin was located about 10–12 cm from the midline. An 18 cm, 21-gauge spinal needle featuring a metal core was inserted under fluoroscopic visualization. When the needle tip reached the lateral aspect of the superior articular process (SAP), its direction was modified towards the lower section of the intervertebral space while monitoring with lateral X-ray fluoroscopy. The needle was then advanced through Kambin’s triangle, just beneath the SAP. Proper placement within the foramen was verified using both anteroposterior and lateral fluoroscopy views. Approximately 1 mL of contrast agent was injected while observing in real-time to ensure ventral epidural distribution without any signs of intravascular, subarachnoid, or extra-epidural absorption (Figure 2). Subsequently, all patients received a transforaminal injection consisting of 1 mL of 1% lidocaine and 1 mL of betamethasone (40 mg/mL).
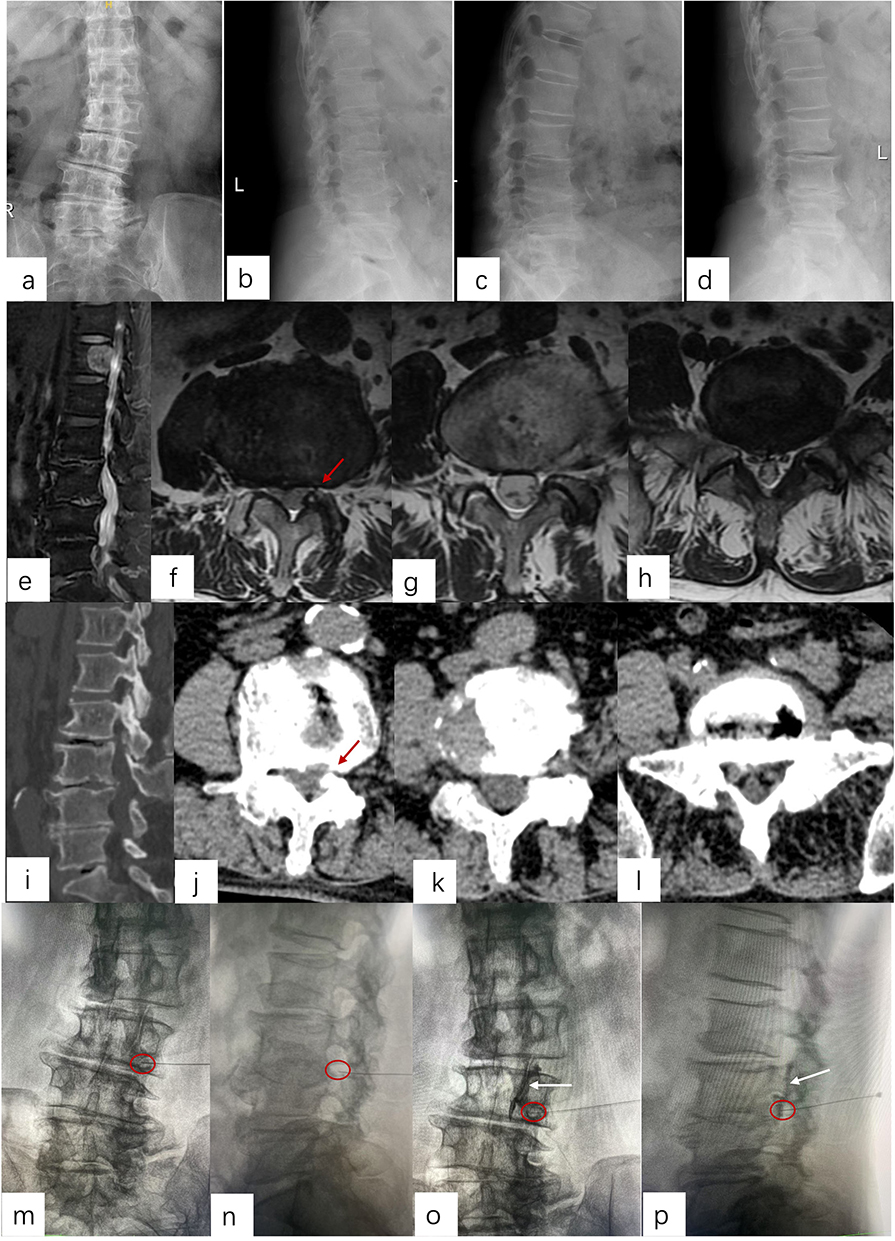 |
Figure 2 An 83-year-old individual presented with left lumbar radiculopathy symptoms lasting five months, during which conventional medical interventions proved ineffective. The patient subsequently received a transforaminal epidural steroid injection. (a and b) illustrate preoperative anteroposterior and lateral X-ray images; (cand d) provide flexion-extension radiographs of the lumbar spine. (e) (sagittal MRI), (f) (L34 axial MRI), (g) (L45 axial MRI), and (h) (L5S1 axial MRI) showcase preoperative MRI results, revealing left foraminal stenosis at the L34 level. (i) (sagittal CT), (j) (L34 axial CT), (k) (L45 axial CT), and (l) (L5S1 axial CT) further validate the presence of left foraminal stenosis at L34 through preoperative CT scans. (m and n) present anteroposterior and lateral X-rays for the purpose of needle placement intraforaminally, while (o and p) depict anteroposterior and lateral X-rays taken after the administration of contrast (red arrow: Stenotic Foramen; red circle: needle tip; white arrow: contrast spread). |
PTED
The procedure utilized the Transforaminal Endoscopic Spine System (TESSYS, Joimax, Karlsruhe, Germany). In summary, patients were positioned face down on a radiolucent table with a slight bend in the lumbar region, while a C-arm fluoroscope was employed.
The operation utilized the Transforaminal Endoscopic Spine System (TESSYS, Joimax, Karlsruhe, Germany) methodology. Patients were positioned face down on a radiolucent table, with a slight flexion of the lumbar spine. A mobile C-arm fluoroscope (United Imaging Healthcare Co., Ltd. Shanghai, China) facilitated the procedure. Prior to surgery, Kirschner wires were employed to outline the puncture path, and the entry point on the skin was marked. The area surrounding the puncture site was disinfected using iodophor and covered with sterile drapes. Local anesthesia was administered with 40 mL of 2.235 mg/mL ropivacaine methanesulfonide, with 5 mL injected into the skin and subcutaneous layers, 10 mL into the deep fascia, and another 10 mL around the periarticular process. An 18-gauge spinal needle featuring a metal core was inserted from the designated entry point towards the midline, guided by intermittent fluoroscopy. Upon contacting the anterior side of the SAP without penetrating the foramen, the needle was substituted with a guidewire. Sequential dilation was conducted to expand the soft tissues until the final protective cannula was accurately positioned, as confirmed by anteroposterior and lateral fluoroscopic views. Foraminoplasty was carried out using a 10-mm diameter trephine through the transforaminal route. The protective cannula was then exchanged for an 8-mm working cannula. The endoscope was advanced to visualize the herniated disc directly. Routine discography was not performed. The hypertrophied ligamentum flavum and herniated disc were excised using flexible endoscopic forceps to achieve decompression. The ventral epidural space was examined with an endoscopic nerve hook to ensure the complete removal of the herniated disc and sufficient decompression of the traversing nerve root. Any epidural bleeding was managed with a radiofrequency probe (Joimax, Karlsruhe, Germany) while continuously irrigating with saline. Finally, the working cannula and endoscope were withdrawn, and the skin was sutured closed (Figure 3).
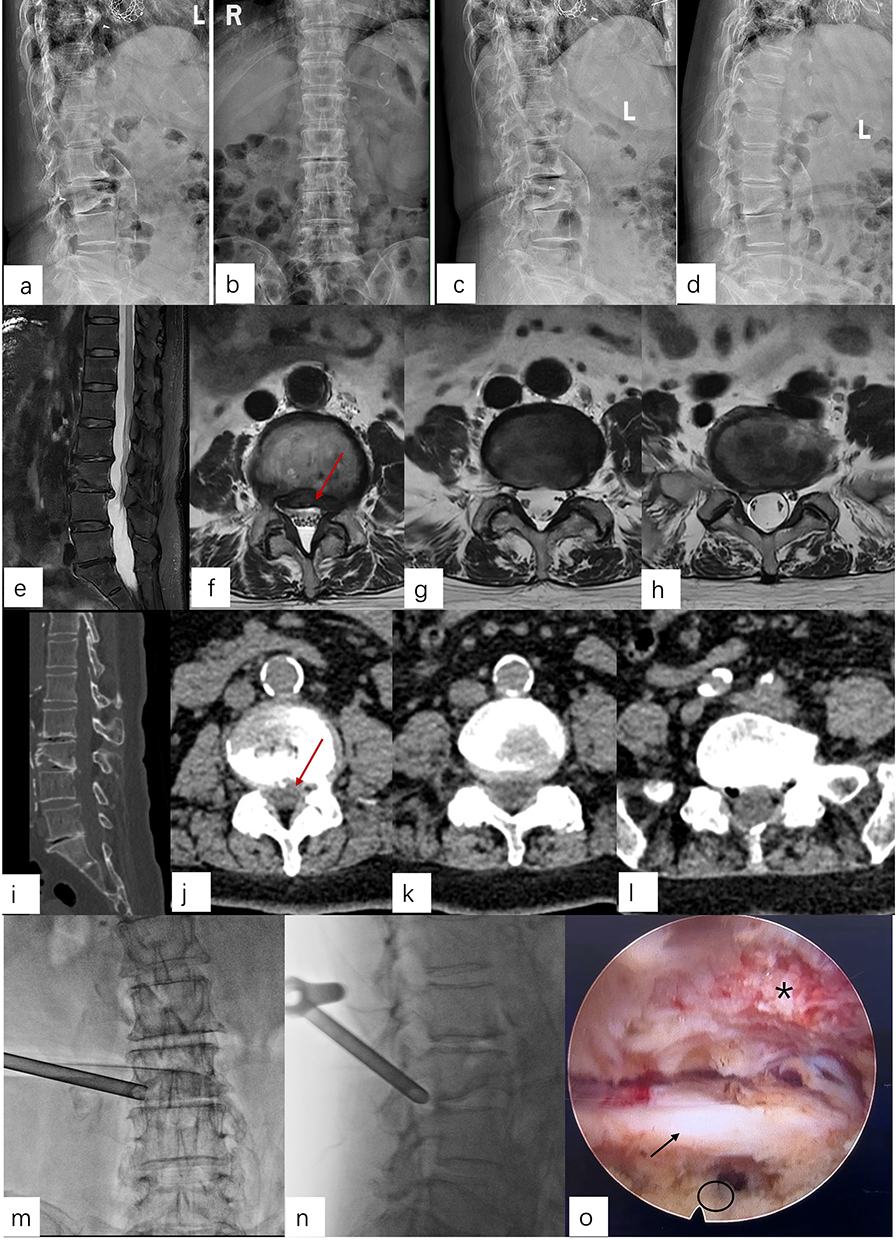 |
Figure 3 An 84-year-old individual exhibited signs of left lumbar radiculopathy for a duration of three months, during which conservative treatment methods were ineffective. The patient then underwent a percutaneous transforaminal endoscopic discectomy. (a and b) show the anteroposterior and lateral X-ray images taken before the operation, while (c and d) present the outcomes of flexion-extension radiography of the lumbar spine. The preoperative MRI results, illustrated in (e) (sagittal MRI), (f) (L34 axial MRI), (g) (L45 axial MRI), and (h) (L5S1 axial MRI), indicate disc herniation and left foraminal stenosis at the L34 level. Additionally, (i) (sagittal CT), (j) (L34 axial CT), (k) (L45 axial CT), and (l) (L5S1 axial CT) further confirm the existence of disc herniation and left foraminal stenosis at the L34 level through CT imaging conducted prior to surgery. Lastly, (m and n) present anteroposterior and lateral X-ray images for the insertion of the working cannula, while (o) depicts the L4 nerve root following discectomy and decompression (red arrow: soft herniated disc; black arrow: L4 nerve root; black asterisk: L5 superior articular process; black circle: intervertebral disc). |
Data Collection and Outcome Evaluations
The gathered information included patient demographics, existing health conditions prior to surgery (such as diabetes, high blood pressure, lung, heart, and brain vascular issues), the surgical site, the frequency of fluoroscopy, duration of the procedure, hospital stay duration, as well as complications occurring during and after the operation. Complications during the perioperative period involved sensations of discomfort, nerve root damage, tears in the dura mater, hematomas post-surgery, and infections. Complications following the surgery consisted of the return of symptoms and the reoccurrence of herniation.
Postoperative follow-up assessments were carried out at intervals of 1 week, 1 month, 3 months, 6 months, and 1 year. An unbiased physician reviewed the clinical and functional results. Patients were monitored either in the outpatient clinic or through phone consultations. Pain levels were measured using the visual analog scale for back pain (VAS-BP) and leg pain (VAS-LP), where 0 indicates no pain and 10 signifies the most severe pain possible. The Oswestry Disability Index (ODI) was utilized to assess functional status. If patients experienced recurring symptoms, radiological evaluations (X-ray, CT, and MRI) were conducted. The modified MacNab classification was employed to determine clinical effectiveness at the 3-month and 1-year marks post-surgery. This classification categorizes outcomes into four groups: excellent (complete symptom resolution and return to normal work and daily life), good (minor symptoms with slight activity limitations, not significantly affecting work or daily life), fair (symptom improvement but with activity restrictions that notably impact normal work and daily life), and poor (no improvement or worsening of symptoms after treatment). Outcomes classified as excellent or good were deemed successful, while fair and poor outcomes were regarded as failures.
Statistical Analysis
Data analysis was conducted using SPSS Version 20.0 (IBM Corporation, Armonk, NY). Continuous data were reported as mean values with standard deviation (± SD), while categorical data were presented as frequencies and percentages. To investigate demographic variations, one-way analysis of variance (ANOVA) and chi-square (or Fisher’s exact) tests were employed. Differences in clinical outcomes between groups were assessed using one-way ANOVA, and within-group variations were analyzed with repeated measures ANOVA. For significant main effects identified in the repeated measures ANOVA, post-hoc pairwise comparisons were conducted with Bonferroni correction to adjust for multiple comparisons and to control the family-wise error rate. Effect sizes for all key outcomes were calculated: Cohen’s d was employed for continuous variables (interpreted as small: 0.2, medium: 0.5, large: 0.8), and Cramér’s V was utilized for categorical variables. A significance threshold of P < 0.05 was established for all statistical evaluations. All analyses were performed on a complete-case basis, excluding patients with missing data at any follow-up time point.
Results
All procedures involving TESI and PTED were carried out successfully. Each patient from both cohorts was monitored for a minimum of 12 months, and the follow-up periods did not show any notable differences between the groups (average of 14.6 months for TESI compared to 13.8 months for PTED). A summary of the demographic and clinical features of the patients can be found in Table 1. No significant variations in baseline characteristics were observed between the two groups.
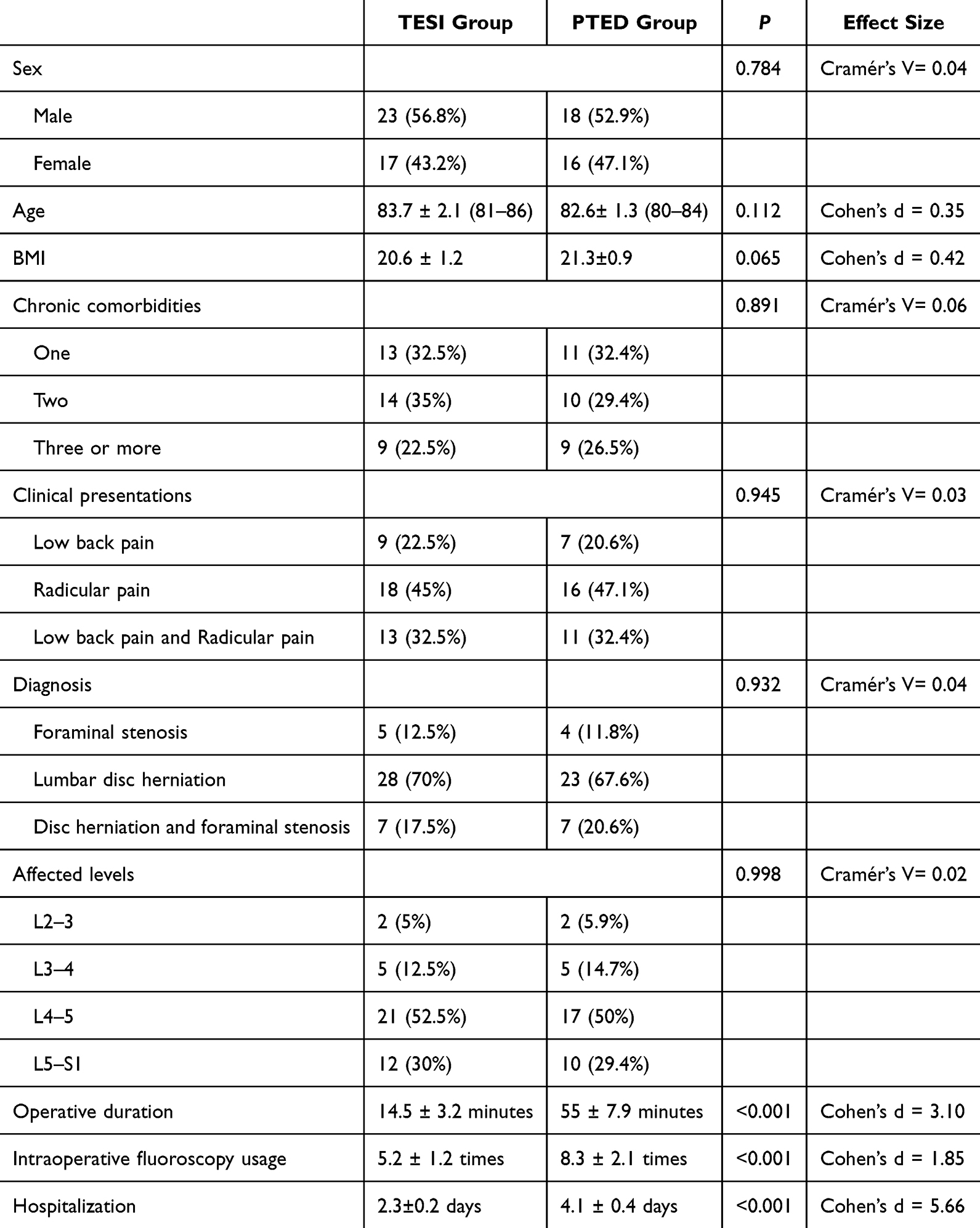 |
Table 1 Patient Demographic and Clinical Characteristics |
The TESI group demonstrated a notably reduced surgical time in comparison to the PTED group, with average durations of 14.5 ± 3.2 minutes versus 55 ± 7.9 minutes, respectively (P<0.001, Cohen’s d=3.10). The use of intraoperative fluoroscopy was significantly less frequent in the TESI group (average: 5.2 ± 1.2 times; range: 4–8) than in the PTED group (average: 8.3 ± 2.1 times; range: 6–12; P<0.001, Cohen’s d=1.85). Additionally, patients undergoing TESI had a hospital stay of 2–3 days (average: 2.3 ± 0.2 days), whereas those in the PTED group were admitted for 3–5 days (average: 4.1 ± 0.4 days; P<0.001, Cohen’s d=5.66). There were no instances of neurological decline following surgery, and neither group reported cases of dysesthesia, nerve root damage, dural tears, epidural hematomas, or infections.
Preoperative scores for ODI, VAS-BP, and VAS-LP did not reveal any notable differences between the two cohorts. Repeated-measures ANOVA revealed a significant group × time interaction for VAS-BP (F[5, 360] = 18.23, P < 0.001), VAS-LP (F[5, 360] = 15.47, P < 0.001), and ODI (F[5, 360] = 21.56, P < 0.001), indicating distinct recovery trajectories between the TESI and PTED groups over the follow-up period. As illustrated in Figures 4A and B, both groups exhibited a marked reduction in VAS-BP and VAS-LP scores at one week postoperatively compared to their preoperative levels. Subsequent Bonferroni-adjusted post-hoc analyses demonstrated that while no significant intergroup differences were observed at the 1- and 3-month time points, the PTED group achieved significantly superior pain relief at the 6-month (VAS-BP: adjusted P = 0.003, Cohen’s d = 1.03; VAS-LP: adjusted P < 0.001, Cohen’s d = 1.32) and 12-month (VAS-BP: adjusted P < 0.001, Cohen’s d = 1.45; VAS-LP: adjusted P < 0.001, Cohen’s d = 1.64) follow-ups. Similarly, for functional improvement assessed by ODI (Figure 5), Bonferroni-corrected comparisons confirmed significantly better outcomes in the PTED group at 6 months (adjusted P = 0.004, Cohen’s d = 1.01) and 12 months (adjusted P < 0.001, Cohen’s d = 1.62).
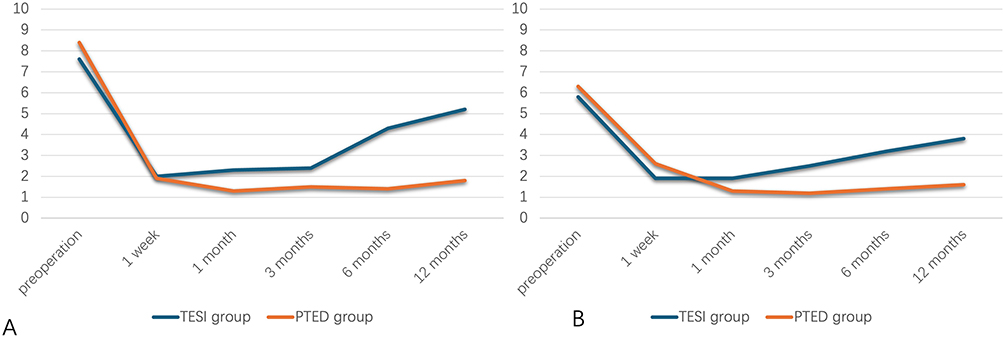 |
Figure 4 (A) the visual analog scale for back pain (VAS-BP) recorded before and after surgery at various follow-up points. (B) the visual analog scale for leg pain (VAS-LP) assessed preoperatively and postoperatively at each follow-up interval. |
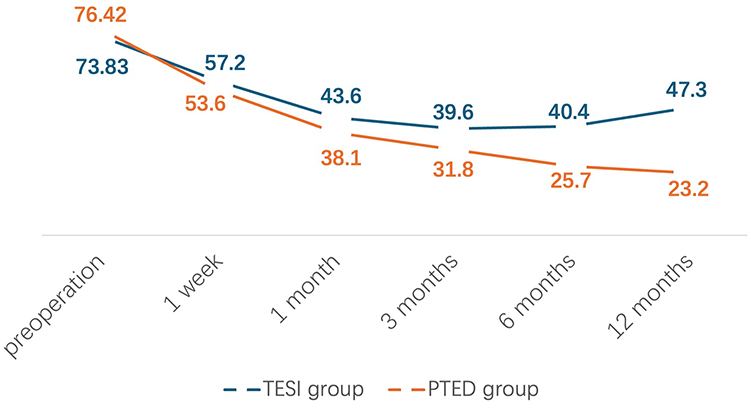 |
Figure 5 The ODI scores at each follow-up time point in the groups. |
Based on the Mac Nab criteria, there was no notable difference in the proportions of excellent and good results among the two patient groups three months following treatment (87.5% for TESI and 91.18% for PTED, P=0.835, Risk Difference [RD] = −3.68%). In the TESI cohort, outcomes were categorized as 19 excellent, 16 good, 3 fair, and 2 poor. Conversely, the PTED cohort had 18 excellent, 13 good, 2 fair, and 1 poor outcome. However, at the one-year mark post-surgery, the rates of excellent and good outcomes showed a significant disparity between the two groups (65% for TESI and 88.24% for PTED, P=0.007, RD = −23.24%). The TESI group reported 10 excellent, 14 good, 8 fair, and 5 poor outcomes, while the PTED group had 17 excellent, 12 good, 3 fair, and 1 poor outcome.
In the follow-up phase, fourteen individuals from the TESI cohort reported a return of symptoms that were similar in intensity to those experienced prior to surgery. Each of these patients underwent an additional TESI procedure, which effectively alleviated their symptoms, and all maintained symptomatic relief until the final follow-up. Conversely, two patients from the PTED group experienced a recurrence of herniation. One patient opted for conservative management, resulting in satisfactory symptom resolution, while the other underwent a transforaminal lumbar interbody fusion, which also yielded a successful outcome; both patients remained stable throughout the subsequent follow-up period.
Discussion
As life expectancy around the world continues to rise, the population of older individuals suffering from spinal disorders is expected to grow.22 Conditions such as radicular pain, often stemming from lumbar disc herniation and neural foraminal stenosis, are becoming increasingly prevalent among the elderly.23 Chronic radicular and lower back pain can endure for extended durations,24 and in severe instances, it can significantly diminish patients’ quality of life.25 Although many individuals with lumbar radiculopathy see improvement through conservative treatments, guidelines suggest a gradual approach, recommending that more invasive options like epidural steroid injections or surgery be considered only when conservative strategies fail and pain remains debilitating.26 Older patients, especially those with additional health issues, are at a heightened risk for adverse reactions to medications27 and complications from surgery,28 with advancing age itself being a contributing factor to unfavorable outcomes following spinal procedures.29 In the context of minimally invasive surgical techniques, endoscopic methods have gained popularity for treating lumbar disc disease, with numerous reports highlighting their positive clinical outcomes.30,31 Endoscopic discectomy is poised to potentially set the standard for managing lumbar disc issues.32 TESI is a well-regarded minimally invasive option for alleviating lumbosacral radicular pain and is increasingly being utilized in older patients as a surgical alternative.20 A 2024 evidence-based review revealed that numerous randomized controlled trials and high-quality observational studies endorse the effectiveness of epidural steroid injections compared to placebo in alleviating pain and enhancing functionality.33
As far as we are aware, no prior studies have directly compared the clinical effectiveness of TESI and PTED in elderly patients aged 80 and above suffering from lumbar radiculopathy. This retrospective comparative analysis is the inaugural effort to assess the clinical results of TESI against PTED for lumbar radiculopathy in this very elderly demographic. Our primary results reveal that although both minimally invasive methods yield considerable short-term pain alleviation and functional enhancement, PTED demonstrated greater long-term effectiveness, prolonged functional recovery, and reduced recurrence rates in comparison to TESI.
Both cohorts experienced notable decreases in VAS-BP, VAS-LP, and ODI scores at both 1 week and 3 months following surgery, when compared to their preoperative measurements (P<0.05), aligning with previous research on minimally invasive techniques.17,20,21 This indicates that both TESI and PTED are effective for managing symptoms in the short term. The swift onset of pain relief emphasizes the effectiveness of TESI as a strong anti-inflammatory treatment.16 Nevertheless, the effectiveness of the two approaches diverged significantly over time. In the TESI group, there was a gradual reduction in VAS and ODI scores after 3 months, leading to a 35% recurrence rate, which highlights a key limitation: while it targets the inflammatory aspect of pain, it does not resolve the underlying mechanical compression. This observation aligns with existing literature; a comprehensive review by Manchikanti et al34 found that the advantages of epidural injections are typically short to medium-term, and Friedly et al35 indicated limited long-term effectiveness for spinal stenosis, which was present in 30% of the TESI participants in our study. In contrast, the PTED group exhibited consistent improvements over the 12-month follow-up period, with a significantly lower recurrence rate of 5.88%. This enhanced durability is attributed to the procedure’s capacity to directly relieve pressure on neural structures by excising herniated disc material or stenotic components. Our long-term success rate of 88.24% classified as excellent or good according to MacNab criteria is well-supported by research on endoscopic discectomy in older patients, such as the favorable 2-year results reported by Liu et al.36
A key finding of this research is the lack of significant complications, such as dural tears, nerve root damage, or infections, in both study groups. This is especially noteworthy considering that more than 88% of participants in each cohort had several chronic health issues. The favorable safety profile observed here sharply contrasts with previous studies that indicated high complication rates among older adults undergoing traditional lumbar surgery.37,38 Our results are more in line with recent assessments of minimally invasive techniques. For example, Telfeian et al found that octogenarians who received minimally invasive lumbar decompression had low rates of morbidity and high safety.39 Similarly, Son and Chernysh reported comparable results for endoscopic procedures aimed at treating degenerative lumbar conditions in older patients.40,41 We believe this safety can be attributed to reduced soft tissue trauma, the application of local anesthesia, and accurate fluoroscopic guidance, all of which help lower the risks linked to general anesthesia and extensive surgical dissection in this sensitive age group.
The decision to use TESI or PTED should be based on individual patient characteristics such as existing health conditions, the source of pain, and expected lifespan, rather than treating them as direct competitors. TESI is advantageous due to its quicker procedure time (14.5 minutes compared to 55 minutes) and shorter hospital stays (2.3 days versus 4.1 days), making it particularly suitable for patients at high surgical risk, those experiencing significant inflammatory pain, or individuals with limited life expectancy where immediate relief is essential. On the other hand, PTED, while more complex, should be regarded as a primary minimally invasive surgical choice for healthier elderly patients who show clear signs of nerve compression and are expected to gain long-term benefits from effective decompression. This method supports the principles of enhanced recovery after surgery (ERAS), striking a balance between the immediate advantages of injections and the substantial risks linked to open fusion, particularly for the elderly population.
This study has several limitations. Its retrospective design may introduce selection bias, as healthier patients might be more likely to undergo the less invasive PTED procedure. Although baseline characteristics showed no significant differences (Table 1), unmeasured confounders could still exist. The single-center design and limited sample size reduced statistical power and precluded meaningful subgroup analyses, particularly regarding the role of comorbidity severity in modifying outcomes, which should be a focus of future research. Outcome assessments were not blinded, creating potential for assessment bias, despite being performed by an independent physician. Although multiple comparisons were adjusted for post hoc, a priori power calculations would strengthen future findings. The one-year follow-up is insufficient to evaluate long-term outcomes such as late recurrence or adjacent segment degeneration; thus, longer-term data are essential. Additionally, the use of complete-case analysis could introduce bias if data were not missing at random. While ANOVA assumptions were verified, more robust methods, such as intention-to-treat analyses or multiple imputation, are recommended for handling missing data in future studies.
Conclusion
In patients over 80 years old suffering from lumbar radiculopathy, both TESI and PTED are considered safe minimally invasive treatments. While TESI can deliver quick short-term relief with less invasiveness, it tends to have higher rates of recurrence. On the other hand, PTED is known for providing better long-term pain management, improved functional recovery, and greater durability, although it requires longer procedures and hospital stays. Treatment plans should be tailored to each individual, in accordance with established geriatric care principles that emphasize the consideration of comorbid conditions, specific pathology, and patient preferences. Further prospective randomized studies are needed to confirm these results.
Abbreviations
TESI, transforaminal epidural steroid injection; PTED, percutaneous transforaminal endoscopic discectomy; VAS, visual analog scale; ODI, oswestry disability index; MRI, magnetic resonance imaging; CT, computed tomography; SAP, superior articular process; ANOVA, analysis of variance.
Data Sharing Statement
The datasets used in this study are not publicly available because of patient confidentiality but are available from the corresponding author (Jian Dong) on reasonable request.
Ethics Approval and Consent to Participate
The study was conducted in accordance with the principles of the Declaration of Helsinki and approved by the institutional ethics committee of Zhongshan hospital, fudan university (approval number 2020–130), which granted permission to access deidentified patient data for this retrospective study, thereby obviating the need for consent to participate.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This work was supported by Shanghai Municipal Central Guided Local Science and Technology Development Fund Project (grant number YDZX20253100002003).
Disclosure
The authors report no conflicts of interest in this work.
References
1. World Health Organization. Ageing and health. 2024. Available from: https://www.who.int/news-room/fact-sheets/detail/ageing-and-health.
2. Ravindra VM, Senglaub SS, Rattani A, et al. Degenerative lumbar spine disease: estimating global incidence and worldwide volume. Global Spine J. 2018;8(8):784–794. doi:10.1177/2192568218770769
3. Aizawa T, Kokubun S, Ozawa H, et al. Increasing incidence of degenerative spinal diseases in japan during 25 years: the registration system of spinal surgery in tohoku university spine society. Tohoku J Exp Med. 2016;238(2):153–163. doi:10.1620/tjem.238.153
4. Rihn JA, Hilibrand AS, Zhao W, et al. Effectiveness of surgery for lumbar stenosis and degenerative spondylolisthesis in the octogenarian population: analysis of the Spine Patient Outcomes Research Trial (SPORT) data. J Bone Joint Surg Am. 2015;97(3):177–185. doi:10.2106/JBJS.N.00313
5. Deer TR, Grider JS, Pope JE, et al. Best practices for Minimally Invasive Lumbar Spinal Stenosis Treatment 2.0 (MIST): consensus guidance from the American Society of Pain and Neuroscience (ASPN). J Pain Res. 2022;15:1325–1354. doi:10.2147/JPR.S355285
6. Fehlings MG, Tetreault L, Nater A, et al. The aging of the global population: the changing epidemiology of disease and spinal disorders. Neurosurgery. 2015;77:S1–5. doi:10.1227/NEU.0000000000000953
7. Piñera AR, Duran C, Lopez B, Saez I, Correia E, Alvarez L. Instrumented lumbar arthrodesis in elderly patients: prospective study using cannulated cemented pedicle screw instrumentation. Eur Spine J. 2011;20(Suppl 3):408–414. doi:10.1007/s00586-011-1907-2
8. Liu C, Guo C, Meng F, Zhu Z, Xia W, Liu H. Perioperative risk factors related to complications of lumbar spine fusion surgery in elderly patients. BMC Musculoskelet Disord. 2023;24(1):573. doi:10.1186/s12891-023-06689-z
9. Sanusi TD, Momin S, Sachdev B, Leung A. Super-elderly, spinal surgery, evaluating the risks and benefits: a retrospective single-centre cohort study. Acta Neurochir. 2024;166(1):248. doi:10.1007/s00701-024-06135-6
10. Zhang JK, O’Neill LK, Farbar SH, et al. Clinical and radiographic outcomes after lateral lumbar interbody fusion in patients older than 75 years. J Neurosurg Spine. 2024;42(1):15–23. doi:10.3171/2024.5.SPINE23831
11. Katz JN, Lipson SJ, Brick GW, et al. Clinical correlates of patient satisfaction after laminectomy for degenerative lumbar spinal stenosis. Spine. 1995;20(10):1155–1160. doi:10.1097/00007632-199505150-00008
12. Deyo RA, Cherkin DC, Loeser JD, Bigos SJ, Ciol MA. Morbidity and mortality in association with operations on the lumbar spine. The influence of age, diagnosis, and procedure. J Bone Joint Surg Am. 1992;74(4):536–543. doi:10.2106/00004623-199274040-00009
13. Johnsson KE, Rosén I, Udén A. The natural course of lumbar spinal stenosis. Clin Orthop Relat Res. 1992;279:82–86.
14. Wang X, Borgman B, Vertuani S, Nilsson J. A systematic literature review of time to return to work and narcotic use after lumbar spinal fusion using minimal invasive and open surgery techniques. BMC Health Serv Res. 2017;17(1):446. doi:10.1186/s12913-017-2398-6
15. Goldstein CL, Macwan K, Sundararajan K, Rampersaud YR. Perioperative outcomes and adverse events of minimally invasive versus open posterior lumbar fusion: meta-analysis and systematic review. J Neurosurg Spine. 2016;24(3):416–427. doi:10.3171/2015.2.SPINE14973
16. Manchikanti L, Singh V, Pampati V, Falco FJ, Hirsch JA. Comparison of the efficacy of caudal, interlaminar, and transforaminal epidural injections in managing lumbar disc herniation: is one method superior to the other? Korean J Pain. 2015;28(1):11–21. doi:10.3344/kjp.2015.28.1.11
17. Wei WB, Dang SJ, Wei L, Liu T, Wang J. Transforaminal epidural steroid injection combined with radio frequency for the treatment of lumbar disc herniation: a 2-year follow-up. BMC Musculoskelet Disord. 2021;22(1):347. doi:10.1186/s12891-021-04209-5
18. Smith CC, McCormick ZL, Mattie R, MacVicar J, Duszynski B, Stojanovic MP. The effectiveness of lumbar transforaminal injection of steroid for the treatment of radicular pain: a comprehensive review of the published data. Pain Med. 2020;21(3):472–487. doi:10.1093/pm/pnz160
19. Liao Z, Chen W, Wang CH. Transforaminal percutaneous endoscopic surgery for far lateral lumbar intervertebral disk herniation. Orthopedics. 2014;37(8):e717–727. doi:10.3928/01477447-20140728-58
20. Li H, Ou Y, Xie F, Liang W, Tian G, Li H. Linical efficacy of percutaneous endoscopic lumbar discectomy for the treatment of lumbar spinal stenosis in elderly patients: a retrospective study. J Orthop Surg Res. 2020;15(1):441. doi:10.1186/s13018-020-01968-0
21. Kim HJ, Nam HJ, Kim SH. Influence of frailty status on the efficacy of epidural steroid injections in elderly patients with degenerative lumbar spinal disease. Pain Res Manag. 2024;2024:5038496. doi:10.1155/2024/5038496
22. Deyo RA, Gray DT, Kreuter W, Mirza S, Martin BI. United States trends in lumbar fusion surgery for degenerative conditions. Spine. 2005;30(12):1441–1445. doi:10.1097/01.brs.0000166503.37969.8a
23. Martin BI, Turner JA, Mirza SK, Lee MJ, Comstock BA, Deyo RA. Trends in health care expenditures, utilization, and health status among US adults with spine problems, 1997-2006. Spine. 2009;34(19):2077–2084. doi:10.1097/BRS.0b013e3181b1fad1
24. Wu A, March L, Zheng X, et al. Global low back pain prevalence and years lived with disability from 1990 to 2017: estimates from the global burden of disease study 2017. Ann Transl Med. 2020;8(6):299. doi:10.21037/atm.2020.02.175
25. Tagliaferri SD, Miller CT, Owen PJ, et al. Domains of chronic low back pain and assessing treatment effectiveness: a clinical perspective. Pain Pract. 2020;20(2):211–225. doi:10.1111/papr.12846
26. Liu C, Ferreira GE, Abdel Shaheed C, et al. Surgical versus non-surgical treatment for sciatica: systematic review and meta-analysis of randomised controlled trials. BMJ. 2023;381:e070730. doi:10.1136/bmj-2022-070730
27. Horgas AL, Snigurska U, Farland MZ, Marsiske M. Analyzing analgesic medications in community-dwelling older adults. Pain Med. 2019;20(1):58–67. doi:10.1093/pm/pnx340
28. Fan N, Yuan S, Du P, et al. Complications and risk factors of percutaneous endoscopic transforaminal discectomy in the treatment of lumbar spinal stenosis. BMC Musculoskelet Disord. 2021;22(1):1041. doi:10.1186/s12891-021-04940-z
29. Tan JY, Kaliya-Perumal AK, Oh JY. Is spinal surgery safe for elderly patients aged 80 and above? Predictors of mortality and morbidity in an asian population. Neurospine. 2019;16(4):764–769. doi:10.14245/ns.1836336.168
30. Demirel A, Oz M, Ulger O. The effect of minimal invasive techniques and physiotherapy on pain and disability in elderly: a retrospective study. J Back Musculoskelet Rehabil. 2019;32(1):63–70. doi:10.3233/BMR-171113
31. Leyendecker J, Prasse T, Rückels P, et al. Full-endoscopic spine-surgery in the elderly and patients with comorbidities. Sci Rep. 2024;14(1):29188. doi:10.1038/s41598-024-80235-2
32. Chung AS, McKnight B, Wang JC. Scientific view on endoscopic spine surgery: can spinal endoscopy become a mainstream surgical tool? World Neurosurg. 2021;145:708–711. doi:10.1016/j.wneu.2020.05.238
33. Peene L, Cohen SP, Kallewaard JW, et al. Lumbosacral radicular pain. Pain Pract. 2024;24(3):525–552. doi:10.1111/papr.13317
34. Manchikanti L, Knezevic E, Knezevic NN, et al. Epidural injections for lumbar radiculopathy or sciatica: a comparative systematic review and meta-analysis of cochrane review. Pain Physician. 2021;24(5):E539–E554.
35. Friedly JL, Comstock BA, Turner JA, et al. A randomized trial of epidural glucocorticoid injections for spinal stenosis. N Engl J Med. 2014;371(1):11–21. doi:10.1056/NEJMoa1313265
36. Liu L, Dong J, Wang D, Zhang C, Zhou Y. Clinical outcomes and quality of life in elderly patients treated with a newly designed double tube endoscopy for degenerative lumbar spinal stenosis. Orthop Surg. 2022;14(7):1359–1368. doi:10.1111/os.13304
37. Puvanesarajah V, Jain A, Shimer AL, et al. Complications and mortality following 1 to 2 level lumbar fusion surgery in patients above 80 years of age. Spine. 2017;42(6):437–441. doi:10.1097/BRS.0000000000001759
38. Deyo RA, Mirza SK, Martin BI, Kreuter W, Goodman DC, Jarvik JG. Trends, major medical complications, and charges associated with surgery for lumbar spinal stenosis in older adults. JAMA. 2010;303(13):1259–1265. doi:10.1001/jama.2010.338
39. Telfeian AE, Sastry R, Oyelese A, et al. Awake, transforaminal endoscopic lumbar spine surgery in octogenarians: case series. Pain Physician. 2022;25(2):E255–E262.
40. Son S, Yoo BR, Kim HJ, Song SK, Ahn Y. Efficacy of transforaminal endoscopic lumbar discectomy in elderly patients over 65 years of age compared to young adults. Neurospine. 2023;20(2):597–607. doi:10.14245/ns.2346192.096
41. Chernysh AA, Leyendecker J, Leary OP, et al. Comparison of pain and functional outcomes among geriatric and nongeriatric adults following full endoscopic spine surgery for degenerative lumbar pathology. Int J Spine Surg. 2025;19(1):27–38. doi:10.14444/8693
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.