Back to Journals » International Medical Case Reports Journal » Volume 15
A Regenerated Achilles Tendon with Good Function One Year After Total Extirpation Due to Infection – A Case Report
Authors Granath M, Hedlund P, Spang C ![]() , Alfredson H
, Alfredson H
Received 1 February 2022
Accepted for publication 24 March 2022
Published 22 April 2022 Volume 2022:15 Pages 219—223
DOI https://doi.org/10.2147/IMCRJ.S360704
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Ronald Prineas
Martin Granath,1 Pär Hedlund,1 Christoph Spang,2 Håkan Alfredson3,4
1Orthopaedic Department, Hässleholm Hospital, Hässleholm, Sweden; 2Private Orthopaedic Spine Center, Würzburg, Germany; 3Institute of Sports Exercise and Health, University College Hospital London, London, UK; 4Department of Community Medicine and Rehabilitation, Sports Medicine, Umeå University, Umeå, 90187, Sweden
Correspondence: Håkan Alfredson, Department of Community Medicine and Rehabilitation, Sports Medicine, Umeå University, Umeå, 90187, Sweden, Tel +46 702288441, Email [email protected]
Background: Delayed Achilles tendon ruptures leaving large defects are difficult to treat, and the potential for tendon regeneration is thought to be limited. Furthermore, post-operative wound healing problems, sometimes including infections, can be challenging to treat and negatively affect rehabilitation.
Case Presentation: This 74-year-old lady suffered from insertional Achilles tendinopathy. After treatment with a local cortisone injection, she sustained a total insertional Achilles tendon rupture. This rupture was treated conservatively, and after treatment the Achilles re-ruptured in the insertional area. The rupture was then treated with re-insertion into the calcaneal insertion. Early in the post-operative period the patient sustained a deep surgical wound infection and sepsis. Because of poor effect of treatment with antibiotics, and total tendon destruction, the whole Achilles was extirpated. After extirpation there was immobilization in a cast followed by mobilization and gradually increased loading. At a one-year follow-up, the patient was walking without a limp, could do heel-raise halfway up standing on one leg, there was a palpable Achilles tendon and ultrasound scanning showed a structure very similar to a slightly thickened and tendinopathic Achilles tendon. There was an obvious regeneration of the whole Achilles tendon, and the tendon function was surprisingly good.
Conclusion: This case study clearly shows the regeneration potential in the Achilles tendon and provides significant knowledge of importance for clinicians dealing with Achilles tendon injuries.
Keywords: Achilles tendon, tendinopathy, Achilles rupture, infection, regeneration
Introduction
It is well known that Achilles tendon ruptures, especially delayed ruptures, can be challenging to treat.1 The healing process in tendons in general is often slow, and can result in formations of inferior scar tissue and adhesion formation.1,2 The remodeling into functional tissue can take years, and functional impairment such as altered gait, plantarflexion weakness, and impaired ankle function can remain.1,2
Tendon healing is characterized by an acute inflammatory phase followed by production and alignment of extracellular matrix (collagen I and III). The speed of this process can vary between different parts of the tendon, and appropriate alignment of newly created collagen fibers is influenced by application of mechanical load.3,4
To the best of our knowledge, there is no consensus on the optimal treatment algorithm for Achilles tendon healing. There are open questions concerning immobilization and mechanical stimulation during the healing process.4,5 The specific mechanisms involved in tissue regeneration, and the role of ageing, are not fully clarified.5,6 Serious injuries such as chronic (delayed) Achilles ruptures most often need surgical treatment, and there are different procedures aiming to cover the tendon defect.7,8 Skin healing can sometimes be difficult after these procedures, often because of too much tension in the skin after suturing over the underlying repair, and plastic surgery can be needed.9
In this case study we report a complicated and challenging clinical case with a surprisingly comprehensive Achilles tendon regeneration after a series of total ruptures, deep surgical wound infection and extirpation of the whole Achilles tendon. Ethical approval for studies on the Achilles tendon was obtained from Umeå University, Sweden. The patient gave consent to publish the information of this case.
Case Presentation
The patient is a healthy 74-year-old lady, physically active with walking and horse riding. One month after cortisone injection treatment of insertional Achilles tendinopathy she sustained a total insertional Achilles tendon rupture during push off when biking. This rupture was treated conservatively in a Walker boot for 8 weeks. Then, during horse riding, a push off caused a total re-rupture in the insertion. The rupture was surgically treated with re-insertion of the Achilles into the calcaneus, using suture anchors. This was followed by immobilization in a cast. Postoperatively the patient sustained a deep wound infection not responding to antibiotics, signs of sepsis, and surgical exploration was indicated. During surgery the whole Achilles was found to be severely affected by infection, more or less destroyed, and the distal 7 cm of the Achilles (the whole free Achilles) had to be removed. This left a large defect without any tendon tissue, and the skin was sutured over the defect. After this procedure, immobilization and treatment with cloxacillin antibiotics, cured the infection and the wound healed properly. The foot was immobilized in a cast the first 10 weeks, from maximum plantarflexion initially, then gradually decreased plantarflexion until reaching neutral position. This was followed by immobilization in a dorsal cast, preventing from stretching of the Achilles in dorsiflexion, for another 3 months. She was told to gradually increase the load during walking, but to avoid stretching for altogether 6 months. After 6 months she was offered surgical reconstruction with a flexor hallucis longus graft, but because she then had a satisfactory function, she decided to wait and see. Her function gradually improved, and one year postoperatively when seeking help for pain in the other Achilles, the good function on the operated side was noticed (Figure 1). Ultrasound scanning surprisingly showed a tendon looking very similar to a slightly tendinopathic Achilles (Figures 2–4).
 |
Figure 1 Bilateral heel raises 1 year after right Achilles tendon removal. |
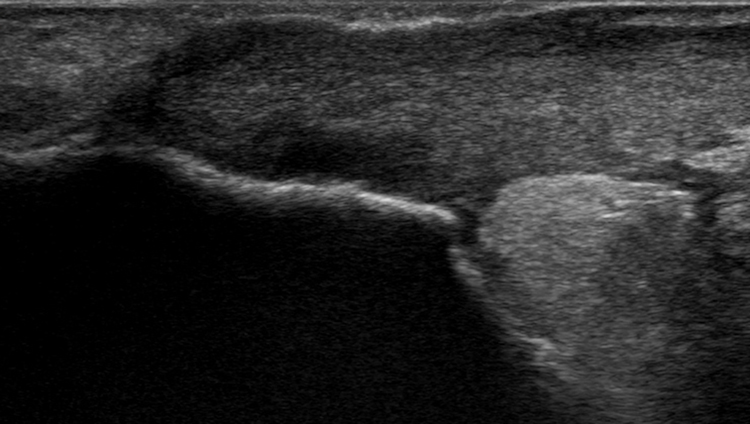 |
Figure 2 Longitudinal ultrasound view showing the Achilles insertion-regenerated tendon like structure including tendinopathy like features inserted into the calcaneus. |
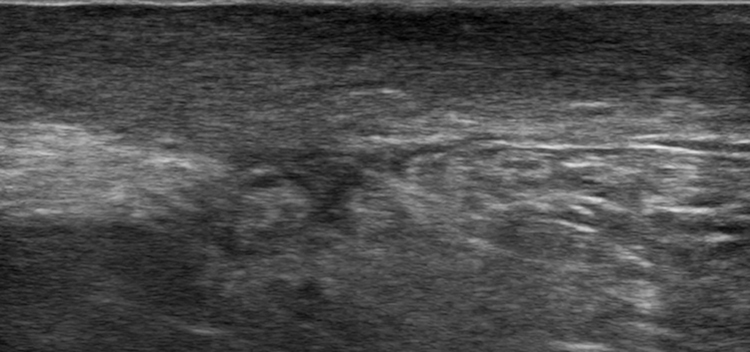 |
Figure 3 Longitudinal ultrasound view showing the Achilles midportion-regenerated tendon like structure including irregular tendinopathy like features. |
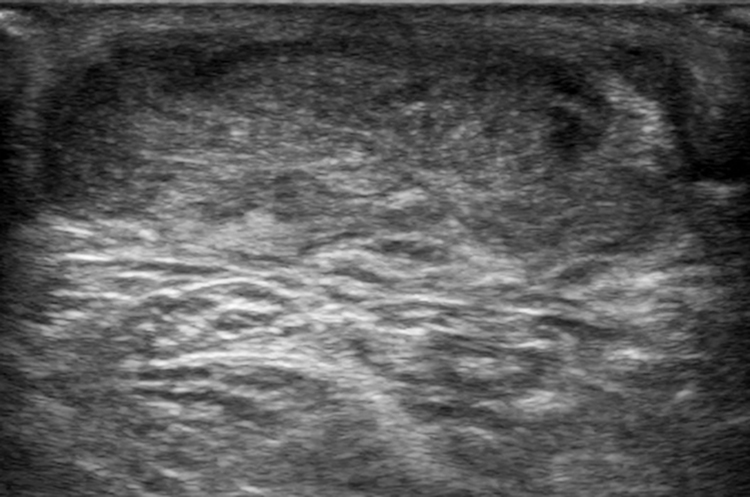 |
Figure 4 Transversal ultrasound view showing the Achilles midportion-regenerated tendon like structure including irregular tendinopathy like features. |
Conclusion and Discussion
We have here presented a patient that had a comprehensive regeneration of the whole Achilles tendon and surprisingly good function, after sustaining two total tendon ruptures, post-operative deep wound infection and sepsis, and treatment with extirpation of the whole tendon. One year after the extirpation the patient had good function, and ultrasound imaging showed a tendon that looked very similar to a slightly tendinopathic Achilles tendon. This case study clearly shows the regeneration potential in the Achilles tendon, and provides significant knowledge of importance for clinicians dealing with Achilles tendon injuries.
Delayed Achilles tendon ruptures are difficult to treat, and surgery is often needed to repair the tendon defect.7,8 Surgical repair of delayed ruptures can be complicated by skin healing problems occasionally complicated by deep infections.9 This female patient was severely affected by a deep wound infection and signs of sepsis, where the whole 7–8 cm free tendon that was destroyed by infection had to be removed. This left a large defect without any tendon tissue. It seemed very unlikely that this defect over time would be filled with tendon-like tissue, allowing for good function, and the patient was offered the possibility of reconstructive surgery after wound healing. However, one year later the patient was satisfied and had good clinical function and ultrasound imaging findings showing a tendon looking very similar to a slightly tendinopathic Achilles.
A limitation with the current study is that we have limited information from the operation. We only have the notes, and the information from the operating surgeon that the whole Achilles was removed.
Despite extensive research on tendon tissue healing there are still many questions on the underlying processes of regeneration, and concerning the ideal application of immobilization and mechanical stimulation.2,3 For this patient, stretching of the tendon was avoided for 6 months, and maybe this is of importance for the tendon tissue regeneration.
In conclusion, the information from this case study is related to only one patient, but hopefully it is of clinical interest and can stimulate research on the regeneration capacity of the Achilles tendon.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Leong NL, Kator JL, Clemens TL, James A, Enamoto-Iwamoto M, Jiang J. Tendon and ligament healing and current approaches to tendon and ligament regeneration. J Orthop Res. 2020;38(1):7–12. doi:10.1002/jor.24475
2. Counihan M, Leahy T, Nuss C, et al. Limited scar resection for chronic achilles tendon repair: use of a rat model. Am J Sports Med. 2021;49(10):2707–2715. doi:10.1177/03635465211023096
3. Notermans T, Tanska P, Korhonen RK, Khayyeri H, Isaksson H. A numerical framework for mechano-regulated tendon healing-Simulation of early regeneration of the Achilles tendon. PLoS Comput Biol. 2021;17(2):e1008636. doi:10.1371/journal.pcbi.1008636
4. Hillin CD, Fryhofer GW, Freedman BR, et al. Effects of immobilization angle on tendon healing after achilles rupture in a rat model. J Orthop Res. 2019;37(3):562–573. doi:10.1002/jor.24241
5. Zabrzyński J, Łapaj Ł, Paczesny Ł, Zabrzyńska A, Grzanka D. Tendon - function-related structure, simple healing process and mysterious ageing. Folia Morphol. 2018;77(3):416–427. doi:10.5603/FM.a2018.0006
6. Paredes JJ, Andarawis-Puri N. Therapeutics for tendon regeneration: a multidisciplinary review of tendon research for improved healing. Ann NY Acad Sci. 2016;1383(1):125–138. doi:10.1111/nyas.13228
7. Maffulli N, Leadbetter WB. Free gracilis tendon graft in neglected tears of the Achilles tendon. Clin J Sports Med. 2005;15(2):56–61. doi:10.1097/01.jsm.0000152714.05097.ef
8. Nilsson-Helander K, Grävare Silbernagel K, Thomeé R, Faxén E, Eriksson BI, Karlsson J. A new surgical method to treat chronic ruptures and re-ruptures of the Achilles tendon. Knee Surg Sports Traumatol Arthrosc. 2008;16(6):614–620. doi:10.1007/s00167-008-0492-3
9. Periasamy M, Venkatramani H, Sabapathy R. Management of chronic Achilles tendon injuries-Review of current protocols and surgical options. Indian J Plastic Surg. 2019;52(1):109–116. doi:10.1055/s-0039-1687923
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.