Back to Journals » International Medical Case Reports Journal » Volume 17
A Rare Case Report of a Congenital Imperforate Hymen Causing Obstructive Uropathy and Constipation in an 11-Year-Old Girl
Authors Tedyanto CP ![]() , Dewi S, Santoso FI, Ere MAP, Oeylex KR
, Dewi S, Santoso FI, Ere MAP, Oeylex KR
Received 13 September 2024
Accepted for publication 22 November 2024
Published 28 November 2024 Volume 2024:17 Pages 985—989
DOI https://doi.org/10.2147/IMCRJ.S494697
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Xudong Zhu
Cecilia Putri Tedyanto,1 Sianty Dewi,2 Fransiscus Iman Santoso,2 Maria Aloysia Praldinya Ere,1 Kevan Ryvanto Oeylex1
1Faculty of Medicine, Universitas Katolik Widya Mandala Surabaya, Surabaya, Indonesia; 2Department of Obstetrics and Gynecology, Faculty of Medicine, Universitas Katolik Widya Mandala Surabaya, Surabaya, Indonesia
Correspondence: Cecilia Putri Tedyanto, Faculty of Medicine, Universitas Katolik Widya Mandala Surabaya, Kalisari, Surabaya, Indonesia, Tel +62-31-99005299, Fax +62-31-99005278, Email [email protected]
Abstract: Imperforate hymen is a rare congenital anomaly that can cause mild to severe complications, which leads to an increase in morbidity rates. The incidence is 1:1000, and there was often a delay in diagnosis since the symptoms were not specific until it caused several complications in other organ systems. We reported a case of obstructive uropathy and constipation in an 11-year-old girl who presented with huge hematocolpos due to imperforate hymen. The main symptom was severe lower abdominal pain with a visual analogue scale of 8. This case shows the significance of a physical examination in diagnosing, increasing efficiency in terms of time and cost, and supporting an earlier diagnosis. A corrective hymenectomy, blood drainage, and hymenoplasty were performed as the definitive management. The patient was able to urinate and defecate within seven hours after surgery. The patient also had her period three weeks after surgery.
Keywords: imperforate hymen, congenital anomaly, vulvovaginal anomaly
Introduction
The genital system is inert throughout the fifth and sixth weeks of fetal development.1 During this period, the mesonephric (Wolffian duct) and paramesonephric (Müllerian duct) pairs of genital ducts are present. The lack of anti-Mullerian hormone (AMH) and the sex-determining region Y (SRY) gene in females causes the Wolffian ducts to recede and the Mullerian ducts to progressively differentiate.2 The urorectal septum, which divides the rectum from the urogenital sinus, occurs in the seventh week of gestation. The Müllerian ducts descend to the urogenital sinus during the ninth week of pregnancy, creating the uterovaginal canal and implant. The Müllerian ducts unite to form a primitive uterovaginal canal during 11–12 weeks of gestation.2,3 The fetal hymen forms from the growth of the sinovaginal bulbs (where the Müllerian ducts meet the urogenital sinus) in the fifth month of gestation, when the vaginal canalization is finished. The hymen perforates typically at approximately 22 weeks of gestation. Failure of perforation during neonatal development causes imperforate hymen.
The hymen is a squamous epithelium-thin membrane that generally circumscribes the opening of the vagina with a small circular opening in the center.4 Imperforate hymen is a congenital anomaly in which the hymen completely covers the vaginal opening, with a prevalence of 0.1% of female births.4,5
Even if the case is rare, it is considered the most common congenital malformation of the female genital tract.6 Delays in diagnosis could cause mild to severe complications in various organ systems.7 The symptoms also usually do not occur until the children reach their menarche age. They often remain unaware of the cyclic abdominal pain and amenorrhea complaints. The accumulation of menstrual blood in the vagina (hematocolpos), or uterine cavities (hematometra), or both (hematocolpometra) may cause severe complications in other organ systems.8,9 This report describes the case of an 11-year-old girl with an imperforate hymen presenting with obstructive uropathy and constipation.
Case Report
Patient Consent
The parents gave verbal and written informed consent for the publication of this case, including the patient’s details and clinical images.
Case Presentation
An 11-year-old girl presented to our emergency department with severe lower abdominal pain. The pain lasted for approximately four days and progressively worsened. Past medical history revealed urinary retention symptoms, presenting with a small amount of urine output in an effortful urination. Additional symptoms included dysuria, post-void residue, suprapubic fullness, dark-yellow urine, flank pain, and low-grade fever over the past two days. The patient also complained of constipation. There was no hematuria or hematochezia.
The patient was born from a spontaneous vaginal birth with a weight of approximately 3200 grams at 38 weeks gestational age at the time of delivery. There was a perinatal history of four months of breastfeeding, appropriate growth and developmental milestones, and complete immunization or vaccine records. The patient did not experience her first menarche.
Investigation
Vital signs showed normal blood pressure (110/70 mmHg), respiratory rate (23 bpm), and temperature (36.2 Celsius degree), with tachycardia (124 bpm) and a visual analogue scale of 8. The patient was defined as overweight with a body mass index of 29.7 from the calculated ratio formula of 66 kilograms of body weight and 149 cm of body height.
Physical examination revealed abdominal distension, suprapubic tenderness, secondary sex characteristics, and complete external genitals. There was a bulging hymen showed as a bluish-shiny mass at the vaginal introitus (Figure 1A).
 |
Figure 1 (A) Bulging hymen showed as a bluish-shiny mass at the vaginal introitus; (B) Hymenectomy performed with cross incision method in an imperforate hymen; (C) Drainage results of a hematocolpos showed a large volume of dark color blood; (D) Complete wound healing of two weeks post-hymenectomy with a form of vaginal opening (black arrow). |
Further investigation revealed that she had been experiencing lower abdominal pain periodically, with a time interval in between, for the past five months. She did not recognize the pain because it initially perceived as a common abdominal discomfort, which did not significantly impact her quality of life. The patient denied having a family history of congenital conditions. There was a history of complete abortus of her mother and incomplete abortus of her aunt. No history of seizure, antibiotics or cytotoxic drug use, any herbal consumption, or radiation exposure during pregnancy.
Ultrasonography examination revealed a huge hypoechoic fluid-filled mass in the vaginal lumen, indicated as hematocolpos, an accumulated blood-filled dilated vagina (Figure 2A). There was also a typical compression of the vesica urinaria (VU) due to the mass. The uterus was normal. Hematological investigations revealed leukocytosis (WBC 14.25 x 103/μL) with a high neutrophil (78%) and low lymphocyte (16.6%). The rest were within the reference range (Table 1).
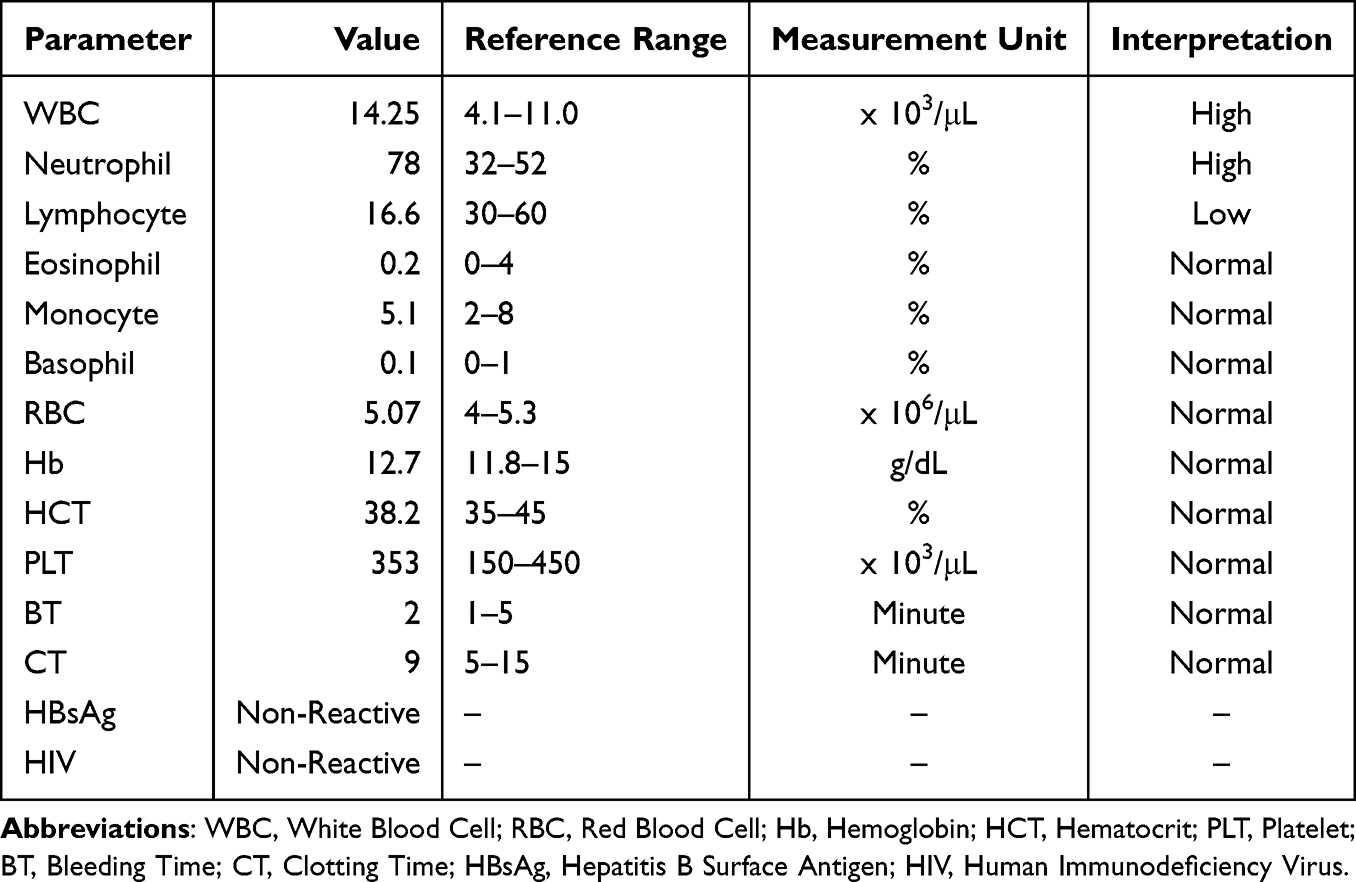 |
Table 1 Hematological Investigations Results |
 |
Figure 2 (A) Hematocolpos showed as hypoechoic mass fulfilled the vagina in an ultrasonography; (B) Post-hymenectomy ultrasonography revealed an empty urinary bladder after a complete urination. |
Final Diagnosis
The patient was diagnosed with an imperforate hymen. Overweight was also established based on nutritional status.
Treatment
Hymenectomy with cross-incision method was performed under general anesthesia (Figure 1B). Approximately 600 mL of dark blood was obtained from the drainage (Figure 1C). Hymen reconstruction, or hymenoplasty, was carried out at the end.
The patient was treated with cefazolin (2x1 grams) and ketorolac (3x30 milligrams) intravenously for the pre-operative treatment. Cefadroxil (3x500 milligrams) and etoricoxib (2x90 milligrams) were prescribed perorally for five days for the take-home medication. The patient was advised to avoid excessive manipulation of the post-operative wound, maintain genital hygiene, follow a healthy diet, increase physical activity, and consult the pediatricians for optimal growth and development.
Outcome and Follow-Up
Seven hours after surgery, the patient felt mild pain in the post-operative wound. She was able to urinate and defecate. A post-surgery ultrasonography revealed an empty urinary bladder after a complete urination (Figure 2B). Within seven days, the wound showed a substantial improvement with no pain. Complete wound healing was observed two weeks after surgery (Figure 1D). The patient also had no complaints and reported her period three weeks after surgery.
Discussion
A bulging hymen, characterized by a bluish-shiny mass in the vaginal introitus, does not always occur in an early case.10 In a late complication, bladder compression can lead to urinary retention, hydronephrosis, or kidney injury. Mechanical obstruction in the urinary tract disrupts the urine outflow, further manifesting urinary tract diseases such as stones, infection, and hydronephrosis, leading to acute kidney injury.11,12 In more severe cases, the mass may obstruct the intestinal tract, leading to constipation. Diagnosis in cases of imperforate hymen with complications can be a challenge due to a lack of knowledge or an incomprehensive examination. Therefore, the wide range of differential diagnoses necessitates a precise and conscientious physical examination.
Imperforate hymen is rarely diagnosed during the neonatal period and is usually present later in puberty as cyclic abdominal pain, primary amenorrhea, or accumulating as a pelvic mass. The complications of these congenital anomalies can actually occur from the perinatal period, such as fetal hydrometrocolpos (HMC).13 Although it is a rare complication, HMC can occur due to cervical or endometrial mucus.13,14 In a further period of age, a congenital vaginal obstruction can cause infertility and is associated with endometriosis.15–17
Education related to risk factors for imperforate hymen is also important to minimize reoccurrences in subsequent pregnancies. Even though the evidence-based etiology is still unclear, several things can still be attempted, including avoiding radiation exposure, cytotoxic drug usage, and non-standardized herb consumption.18,19 Seeking optimal nutrition during pregnancy is also necessary.20
Surgical correction is a definitive medical management for imperforate hymen. Post-operative wound observations should be carried out periodically to evaluate the healing process. Consider installing a plug to prevent wound closure after the surgery. Other congenital anomalies are often associated with other congenital vaginal obstruction. A comprehensive organ screening also needs to be performed, considering the possibility of other congenital abnormalities in different body parts.
There were several limitations in this report. First, the pre-operative size of hematocolpos was not measured in this report, whereas the data could be important to determine the minimum size or volume of blood accumulation that can cause urinary and gastrointestinal obstruction. Second, the follow-up data in this case was not conducted over a long period, whereas there could be a possibility of post-operative obstruction recurrence of cases with no post-operative dilatator.
Conclusion
Imperforate hymen is a condition that needs attention and consideration as a differential diagnosis in pre-menarche or menarche-age children with complaints in the urinary tract or intestines, as well as post-menarche-age children with complaints of primary amenorrhea, especially if both are accompanied by cyclic abdominal pain. Physical examination of the genitals is simple yet often forgotten, whereas it can be crucial for diagnosis. Check for anatomical abnormalities and congenital screening at an earlier age to prevent a late diagnosis and further complications.
Abbreviations
VU, vesica urinaria; AMH, anti-Mullerian hormone; SRY, sex-determining region Y.
Disclosure
The author(s) report no conflicts of interest in this work.
References
1. Robbins JB, Broadwell C, Chow LC, Parry JP, Sadowski EA. Müllerian duct anomalies: embryological development, classification, and MRI assessment. J Magn Reson Imaging. 2015;41(1):1–12. doi:10.1002/jmri.24771
2. Roly ZY, Backhouse B, Cutting A, et al. The cell biology and molecular genetics of Müllerian duct development. Wiley Interdiscip Rev Dev Biol. 2018;7(3):e310. doi:10.1002/wdev.310
3. Guioli S, Sekido R, Lovell-Badge R. The origin of the Mullerian duct in chick and mouse. Dev Biol. 2007;302(2):389–398. doi:10.1016/j.ydbio.2006.09.046
4. Heger AH, Ticson L, Guerra L, et al. Appearance of the genitalia in girls selected for nonabuse: review of hymenal morphology and nonspecific findings. J Pediatr Adolesc Gynecol. 2002;15(1):27–35. doi:10.1016/S1083-3188(01)00136-X
5. Kahn R, Duncan B, Bowes W. Spontaneous opening of congenital imperforate hymen. J Pediatr. 1975;87(5):768–770. doi:10.1016/S0022-3476(75)80306-4
6. Shaw LM, Jones WA, Brereton RJ. Imperforate hymen and vaginal atresia and their associated anomalies. J R Soc Med. 1983;76(7):560–566. doi:10.1177/014107688307600707
7. Khemchandani S, Devra A, Gupta S. An unusual case of urinary tract obstruction due to imperforate hymen in an 11-month-old infant. Indian J Urol. 2007;23(2):198–199. doi:10.4103/0970-1591.32076
8. Lee KH, Hong JS, Jung HJ, et al. Imperforate hymen: a comprehensive systematic review. J Clin Med. 2019;8(1):56. doi:10.3390/jcm8010056
9. Chang JW, Yang LY, Wang HH, Wang JK, Tiu CM. Acute urinary retention as the presentation of imperforate hymen. J Chin Med Assoc. 2007;70(12):559–561. doi:10.1016/S1726-4901(08)70061-3
10. Ramareddy RS, Kumar A, Alladi A. Imperforate hymen: varied presentation, new associations, and management. J Indian Assoc Pediatr Surg. 2017;22(4):207–210. doi:10.4103/0971-9261.214451
11. Rosenblum H, Bar-Dayan Y, Dovrish Z, et al. The endless differential diagnosis of acute obstructive renal failure: unusual challenges for the sharp-sighted clinician. Isr Med Assoc J. 2010;12(5):280–282.
12. Flores-Mireles AL, Walker JN, Caparon M, Hultgren SJ. Urinary tract infections: epidemiology, mechanisms of infection and treatment options. Nat Rev Microbiol. 2015;13(5):269–284. doi:10.1038/nrmicro3432
13. Bicha MM, Workneh ZA. Antenatal ultrasound diagnosis of huge fetal hydrometrocolpos secondary to imperforate hymen and successful postnatal treatment: a case report. Case Rep Perinat Med. 2023;12(1):20230019. doi:10.1515/crpm-2023-0019
14. Bannour B, Abbassi H, Guerbej E, Bannour I, Boughizane S. Prenatal diagnosis of isolated fetal hydrometrocolpos: a case report. Radiol Case Rep. 2024;19(12):6147–6151. doi:10.1016/j.radcr.2024.08.150
15. Sugi MD, Penna R, Jha P, et al. Müllerian duct anomalies: role in fertility and pregnancy. Radiographics. 2021;41(6):1857–1875. doi:10.1148/rg.2021210022
16. Kapczuk K, Zajączkowska W, Madziar K, Kędzia W. Endometriosis in adolescents with obstructive anomalies of the reproductive tract. J Clin Med. 2023;12(5):2007. doi:10.3390/jcm12052007
17. Takahashi N, Harada M, Kanatani M, Wada-Hiraike O, Hirota Y, Osuga Y. The association between endometriosis and obstructive Müllerian anomalies. Biomedicines. 2024;12(3):651. doi:10.3390/biomedicines12030651
18. World Health Organization. Congenital Anomalies. World Health Organization; 2015.
19. Lemmens M, van Vugt JMG, Willemsen M, van der Voorn P, van Bokhoven H, ten Donkelaar HJ. Causes of congenital malformations. In: Ten Donkelaar HJ, Lammens M, Hori A, editors. Clinical Neuroembryology.
20. Lassi ZS, Padhani ZA, Rabbani A, Rind F, Salam RA, Bhutta ZA. Effects of nutritional interventions during pregnancy on birth, child health and development outcomes: a systematic review of evidence from low- and middle-income countries. Campbell Syst Rev. 2021;17(2):e1150. doi:10.1002/cl2.1150
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.