Back to Journals » Clinical Ophthalmology » Volume 14
A Randomized Fellow-Eye Clinical Trial to Evaluate Patient Preference for Dexamethasone Intracanalicular Insert or Topical Prednisolone Acetate for Control of Postoperative Symptoms Following Bilateral Femtosecond Laser in Site Keratomileusis (LASIK)
Authors Greenwood MD, Gorham RA, Boever KR ![]()
Received 10 June 2020
Accepted for publication 28 July 2020
Published 6 August 2020 Volume 2020:14 Pages 2223—2228
DOI https://doi.org/10.2147/OPTH.S265311
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Michael D Greenwood,1 Richard A Gorham,2 Keeley R Boever2,3
1Vance Thompson Vision, West Fargo, ND, USA; 2Ektropia Solutions LLC, Laguna Beach, CA, USA; 3Vance Thompson Vision, Sioux Falls, SD, USA
Correspondence: Michael D Greenwood
Vance Thompson Vision, 505 32nd Ave E, Suite B, West Fargo, ND 58078, USA
Tel +1 701-566-5390
Fax +1 701-639-7199
Email [email protected]
Purpose: To determine the preference of patients undergoing bilateral LASIK for either the dexamethasone intracanalicular insert or topical prednisolone acetate for control of postoperative symptoms and ocular surface signs.
Methods: In this randomized clinical trial, one eye was randomized to receive the dexamethasone insert or topical prednisolone acetate 1% four times daily for one week and 2 times daily for a second week; the fellow eye received the alternate therapy. One month postoperatively, patient preference for these two therapies was assessed using an adapted COMTOL questionnaire. Ocular comfort was assessed using the SPEED questionnaire. Corneal staining and uncorrected distance visual acuity (UDVA) were also assessed.
Results: Twenty patients participated. At Month 1, 80% of patients preferred the dexamethasone insert, 10% preferred prednisolone acetate, and 10% expressed no preference (p< 0.001). SPEED scores measuring ocular comfort/discomfort related to dry eye symptoms were similar between groups (p=0.72), and both the incidence of patient-reported ocular dryness and the corneal staining scores were similar between groups. Both groups attained the same final UDVA.
Conclusion: Patients undergoing elective bilateral femtosecond LASIK surgery overwhelmingly (by an 8-to-1 margin) preferred the dexamethasone insert to topical prednisolone acetate for postoperative treatment. The insert produced comparable ocular comfort, corneal staining, and visual acuity outcomes to topical prednisolone. The insert is an appropriate means of postoperative symptom control in this quality of life-conscious population.
Keywords: dexamethasone, Dextenza, LASIK, randomized trial, patient preference, ocular surface symptoms
Introduction
Corneal inflammation can occur after laser-assisted in situ keratomileusis (LASIK) and other corneal refractive procedures.1–5 Although clinically evident corneal inflammation is uncommon after LASIK, subclinical inflammation is present involving activation of corneal keratocytes and release of cytokines.1–5 Consequences of postoperative inflammation in the post-LASIK eye can range from mild and transient irritation to chronic postoperative dry eye to the more devastating diffuse lamellar keratitis, which must be differentiated from pressure-related LASIK interface complications such as pressure-induced stromal keratitis or post-LASIK edema-induced keratopathy.2,6-8
Anti-inflammatory prophylaxis is a standard component of perioperative care in eyes undergoing corneal refractive surgery.9 This can take many forms, from single-agent corticosteroids to fixed combinations of steroids and antibiotics for antimicrobial prophylaxis. No widespread standard has been described.
The US Food and Drug Administration recently approved a novel sustained-release form of dexamethasone (Dextenza, Ocular Therapeutix, Bedford, MA). This small insert, intended for intracanalicular placement, is a polyethylene glycol hydrogel rod impregnated with 0.4 mg of preservative-free dexamethasone.10,11 It is inserted through the punctum into the canaliculus, swells upon hydration, and anchors into place, dissolving over time to deliver a sustained and tapered dose of dexamethasone for up to 30 days without the need for post-treatment removal.10 It can be inserted preoperatively, intraoperatively, or postoperatively at surgeons’ discretion. The hydrogel is conjugated with fluorescein for enhanced visualization during examination.10
The dexamethasone insert is indicated for the control of pain and inflammation following ocular surgery.12 It has been evaluated in three Phase 3 trials for the control of postoperative pain and inflammation following phacoemulsification cataract surgery.10,13 Patients from these studies reported favorable satisfaction, convenience, and comfort with the insert.14 To our knowledge, there are no published reports of its use in controlling postoperative symptoms and ocular surface signs following corneal refractive surgery. In addition to control of symptoms and ocular surface signs arising from the dexamethasone active ingredient, patients undergoing corneal refractive surgery may benefit from the ocular surface effects of punctal occlusion. In this paper, we report the results of a prospective, randomized trial to evaluate patients’ experience and preference for the dexamethasone insert or topical prednisolone acetate for the control of postoperative pain and inflammation following LASIK.
Methods
This was a single-site prospective, randomized, open-label, fellow eye-controlled interventional trial. The protocol was reviewed and approved by an ethics committee (Aspire IRB) on January 23, 2020. All prospective subjects provided written informed consent to participate, and the study was conducted in accordance with the Declaration of Helsinki. The study was entered into clinicaltrials.gov (NCT04281862) on February 19 and finalized on February 24, 2020, after addressing several technical errors unrelated to the protocol; consecutive consenting subjects were enrolled between February 20, 2020, and February 27, 2020. Data sharing requests addressed to the corresponding author will be considered on a case by case basis.
Participants were adults aged 18 years or older undergoing elective bilateral femtosecond LASIK surgery whose inter-eye preoperative spherical refractive difference was ≤2 diopters. Potential subjects were excluded if they desired monovision LASIK, or in the presence of corneal pathology that might interfere with surgical outcomes, contraindications to ocular corticosteroid or antimicrobial therapy, use of systemic nonsteroidal anti-inflammatory drugs (NSAIDs) >1200mg/day, any current corticosteroid therapy (including ocular implants), concurrent ocular comorbidities (such as ocular inflammatory disease, macular edema, proliferative diabetic retinopathy, etc.), prior laser or incisional ocular surgery within 6 months of study entry, or history of prior punctal cauterization.
Potential subjects underwent a comprehensive medical and ocular history and ophthalmological examination to establish eligibility 1–30 days before surgery. Eligible subjects underwent standard LASIK surgery in both eyes in a single session. The procedure was performed using the WaveLight FS200 femtosecond laser for the flap creation and the WaveLight EX500 Excimer laser for the LASIK treatment (Alcon, Ft. Worth, TX). Corneal flaps were created on both eyes, then the patient was moved under the excimer laser. The first eye to be operated upon was randomized to receive either a dexamethasone 0.4mg intracanalicular insert (Dextenza, Ocular Therapeutix, Bedford, MA) inserted into the inferior canaliculus or prednisolone acetate 1% four times daily for 1 week and 2 times daily for 1 week beginning on the day of surgery; the second eye to be operated upon received the alternate therapy. In this design, every subject experienced both treatments simultaneously. Randomization was accomplished using a randomization sequence generated at Random.org; a numbered envelope system was utilized to reveal the next assignment in sequence. In the eye that received the dexamethasone intracanalicular insert, it was placed prior to lifting the flap and performing the excimer laser treatment. The punctum was dilated with a small probe, the insertion site was dried with a cellulose sponge, and the insert was placed in the canaliculus. The procedure then resumed as normal. Rescue therapy—the need for which was at the discretion of the investigator—consisted of topical prednisolone acetate in dexamethasone-randomized eyes or increased frequency of dosing in prednisolone-randomized eyes. All eyes received topical moxifloxacin 0.5% 4 times daily for 1 week, and artificial tears were recommended for use as needed. Subjects were re-evaluated 1 day, 1 week, and 1 month postoperatively.
The study had two primary outcomes. The first was patient preference among the two treatments at postoperative month 1 assessed using an adaptation of the Comparison of Ophthalmic Medications for Tolerability (COMTOL) questionnaire, which has been validated for consistency, reliability, and reproducibility.15 This 18-question instrument captures information on overall treatment preference as well as the nature, frequency, and severity of side effects and effects on visual function of topical ophthalmic therapy with sufficient performance to support its use as a supplement to spontaneous adverse event reporting in clinical trials.15 This questionnaire was administered to subjects by an experienced member of the research team at the 1 month postoperative visit. The second primary outcome was dry eye symptom assessment at postoperative month 1 using the Standardized Patient Evaluation of Eye Dryness (SPEED) questionnaire. This 4-item (per eye) instrument’s reproducibility and correlation with clinical signs has been validated for use in assessing ocular comfort or discomfort related to dry eye symptoms.16 This questionnaire was administered by experienced research staff at preoperative baseline as well as at each of the three postoperative visits. Secondary outcomes included tear film break-up time (TBUT), the mean change from baseline to Month 1 in corneal fluorescein staining using the National Eye Institute corneal fluorescein staining scale (0–3 representing no, mild, moderate, or severe staining),17 and mean change in uncorrected distance visual acuity (UDVA), also assessed at each postoperative visit. Ocular pain was a planned secondary analysis, but the absence of pain in all eyes precluded analysis. Safety endpoints included the incidence of intraocular pressure (IOP) increases of ≥10 mmHg above baseline IOP, the proportions of eyes in each group requiring rescue anti-inflammatory therapy, and the nature and incidence of adverse events.
Statistical analysis of overall treatment preference from the COMTOL survey was performed using the chi-square test. SPEED scores, TBUT, and changes in corneal staining scores were compared using the nonparametric Mann Whitney U-test for non-normally distributed ordinal data. Changes in UDVA (measured in logMAR units) were assessed using paired t-tests. The level of significance was taken to be 0.05. No formal power calculations were conducted to determine sample size, and a convenience sample of 20 subjects (40 eyes) was selected to characterize outcomes.
Results
A total of 20 subjects (40 eyes) participated in this trial. All were Caucasian, 12 (60%) were male, and their average age was 33 years. Of these 20 subjects, 15 subjects were seen at the Month 1 visit, and the remaining 5 subjects did not attend the final visit due to concerns related to the novel SARS-CoV-2 pandemic; these 5 subjects completed the COMTOL and SPEED questionnaires by phone.
Among the 20 subjects undergoing bilateral LASIK surgery and receiving both treatments—one in each eye—16 (80%) reported a preference for the dexamethasone insert, 2 (10%) for topical prednisolone, and 2 (10%) reported no preference (p<0.0001; Figure 1) using the COMTOL instrument. Analysis of responses to the additional items in the COMTOL instrument did not reveal a clear basis for this preference. The SPEED questionnaire was completed at Month 1 by 19 subjects. The distribution of SPEED scores—representing ocular comfort or discomfort related to dry eye symptomatology—was comparable for both treatments (p=0.72), with median scores of 0 (no symptoms) in both groups (Figure 2). Ocular dryness was reported in comparable numbers of eyes in both groups at all time points (p>0.05 for all).
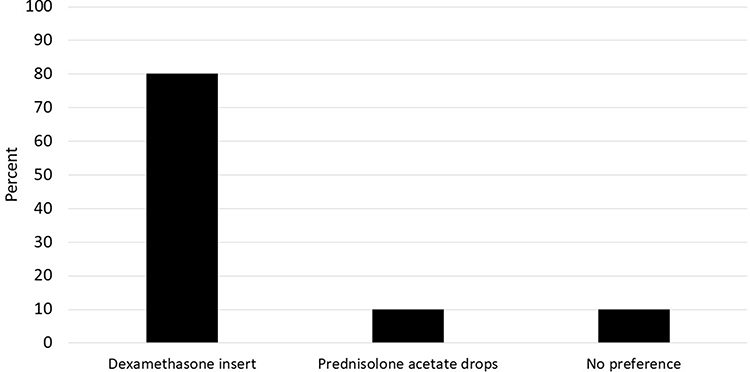 |
Figure 1 Patient preferences for dexamethasone insert or prednisolone acetate assessed using an adapted COMTOL questionnaire (n=20). |
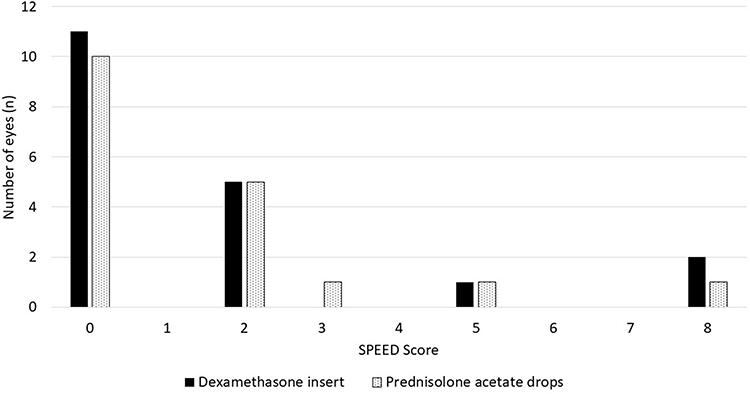 |
Figure 2 Distribution of ocular comfort scores as measured by the SPEED questionnaire in both treatment groups at Month 1. |
The number of eyes with normal (≥10 seconds) TBUT values were similar (p≥0.2) between groups at baseline and each postoperative time point (Figure 3). Corneal staining at baseline and Month 1 was available in 15 subjects. Overall, the mean change in corneal staining scores was 0 in 13/15 dexamethasone insert eyes and in 9/15 prednisolone eyes, with equal numbers manifesting slightly better or worse scores at Month 1 versus baseline in both groups (p=0.47). Mean (standard deviation) logMAR UDVA (n=15) improved from 0.88 (0.35) preoperatively to −0.14 (0.11) at Month 1 in dexamethasone insert eyes and from 0.88 (0.33) to −0.16 (0.05) in prednisolone eyes; the difference in UDVA change from baseline between groups was not statistically significant (p=0.75). The effects of these treatments on postoperative ocular pain could not be assessed as no patients reported any pain at any visit.
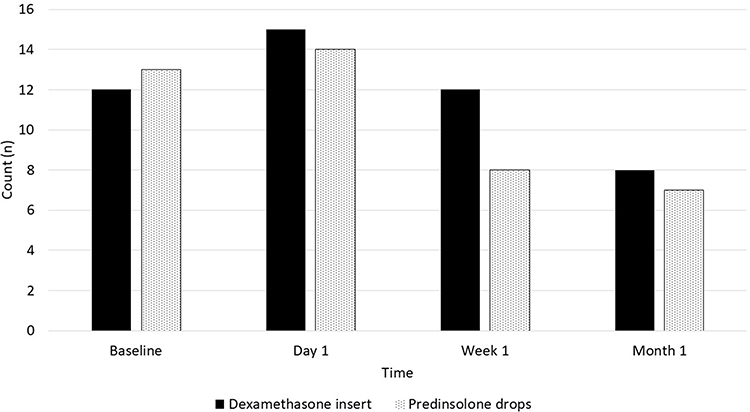 |
Figure 3 Number of eyes with normal tear film break-up time (TBUT ≥10 seconds) by treatment group and time point. |
No intraoperative or postoperative complications occurred. No eyes manifested IOP elevations ≥10 mmHg from baseline at any postoperative visit, and no eyes required rescue anti-inflammatory therapy.
Discussion
This prospective, randomized clinical trial demonstrated that patients undergoing bilateral LASIK overwhelmingly preferred the one-time insertion of a dexamethasone intracanalicular insert over daily topical therapy with prednisolone acetate for postoperative symptoms control. Ocular comfort was similar between groups using the SPEED instrument, indicating no discomfort from the insert, and both the incidence of patient-reported ocular dryness and the corneal staining scores were similar between groups. Both groups attained the same excellent final UDVA as well.
Three previous phase 3 clinical trials evaluating the dexamethasone insert were conducted in patients undergoing phacoemulsification cataract extraction; in these studies, eyes receiving the insert were significantly more likely to be free of anterior chamber inflammation than in control eyes.10,13 This pharmacodynamic effect supports the bioavailability of dexamethasone in the anterior chamber, reached presumably through the tear film and the ocular surface. In contrast to intraocular surgery, the goal of anti-inflammatory prophylaxis in corneal refractive surgery is to prevent or minimize ocular surface inflammation. The bioavailability of dexamethasone on the ocular surface when administered via the intracanalicular insert would be expected to be at least as high as in the anterior chamber, and logically perhaps even more so. As evidenced in this study, clinical outcomes—including UDVA, ocular comfort, and corneal staining—indicate that the dexamethasone insert provided comparable inflammation control to topical prednisolone acetate. This was accomplished safely, with no IOP elevations and no need for rescue therapy in any eyes. Other approaches to ocular surface delivery of steroid therapy have been described—including contact lens-based deliver systems—although these have not attained regulatory approval or commercialization to date.18,19
Patients seeking LASIK and other corneal refractive procedures undergo surgery with the desire to reduce or eliminate the need for glasses. Thus, it is of little surprise that these patients would prefer to reduce or eliminate their need for daily topical medical therapy as well. Consistent with this expectation, 80% of all patients—and 89% of those expressing a preference—preferred the insert over topical medical therapy in this study. This finding is consistent with the results of a qualitative study conducted in a subset of participants in the dexamethasone phase 3 phacoemulsification trials, in which the insert was found to be comfortable, convenient; 88% of subjects reported that they would prefer the insert over eye drops in future cataract surgery procedures.14
Another benefit of the dexamethasone insert is that it minimizes reliance on adherence with perioperative self-administration of medications, which has been shown to be poor after cataract surgery.20 Additionally, the insert minimizes or obviates hand-face contact for eye drop instillation. The recent SARS-CoV-2 pandemic has underscored the importance of avoiding face-touching wherever possible, and this study in specific was affected by the pandemic in that 5 of 20 subjects were not seen at Month 1. These five had risk profiles that made office-based visits imprudent. For patients who require assistance with eye drop instillation, a sustained release product such as the dexamethasone insert also reduces the frequency of close face-to-face proximity required for a caregiver to instill topical medications.
This study’s strengths include its design. Randomized clinical trials provide Level 1 evidence in support of the relative outcomes of therapies.21 Also, the use of fellow eyes as controls permitted subjects to experience both treatments and determine their preferences rather than comparing the perceptions of different groups receiving different treatments. The small size of this study is a limitation. Larger studies will be necessary to confirm these findings.
Conclusions
In summary, patients undergoing elective bilateral LASIK surgery overwhelmingly (by an 8-to-1 margin) preferred the dexamethasone insert to topical prednisolone acetate for postoperative control of symptoms and ocular surface signs. The insert produced comparable ocular comfort, corneal staining, and visual acuity outcomes to topical prednisolone. The insert is an appropriate means of postoperative inflammation control in this quality of life-conscious population.
Disclosure
Michael D Greenwood reports grants from Ocular Therapeutix, during the conduct of the study; personal fees from Ocular Therapeutix, outside the submitted work. He is an employee of Vance Thompson Vision. Richard A Gorham reports personal fees from Vance Thompson Vision, during the conduct of the study; personal fees from Vance Thompson Vision, outside the submitted work. He is an employee of Ektropia Solutions LLC. Keeley R Boever reports grants from Ocular Therapeutix, during the conduct of the study. She is an employee of Vance Thompson Vision. The authors report no other conflicts of interest in this work.
References
1. Alio JL, Perez-Santonja JJ, Tervo T, et al. Postoperative inflammation, microbial complications, and wound healing following laser in situ keratomileusis. J Refract Surg. 2000;16(5):523–538.
2. Alio JL, Javaloy J. Corneal inflammation following corneal photoablative refractive surgery with excimer laser. Surv Ophthalmol. 2013;58(1):11–25. doi:10.1016/j.survophthal.2012.04.005
3. Abahussin M, Hayes S, Edelhauser H, Dawson DG, Meek KM. A microscopy study of the structural features of post-LASIK human corneas. PLoS One. 2013;8(5):e63268. doi:10.1371/journal.pone.0063268
4. Marino GK, Santhiago MR, Torricelli AA, Santhanam A, Wilson SE. Corneal molecular and cellular biology for the refractive surgeon: the critical role of the epithelial basement membrane. J Refract Surg. 2016;32(2):118–125. doi:10.3928/1081597X-20160105-02
5. Resan M, Vukosavljevic M, Vojvodic D, Pajic-Eggspuehler B, Pajic B. The acute phase of inflammatory response involved in the wound-healing process after excimer laser treatment. Clin Ophthalmol. 2016;10:993–1000.
6. Chao CW, Azar DT. Lamellar keratitis following laser-assisted in situ keratomileusis. Ophthalmol Clin North Am. 2002;15(1):35–40. doi:10.1016/S0896-1549(01)00014-1
7. Tello A, Galvis V, Mendoza BF. LASIK interface complications: pressure-induced stromal keratitis (PISK), interface fluid syndrome (IFS) and post-LASIK edema-induced keratopathy (PLEK). Int Ophthalmol Clin. 2016;56(3):185–187. doi:10.1097/IIO.0000000000000129
8. Galvis V, Tello A, Revelo ML, Valarezo P. Post-LASIK edema-induced keratopathy (PLEK), a new name based on pathophysiology of the condition. BMJ Case Rep. 2012;2012.
9. Chuck RS, Jacobs D, Lee JK, et al. Refractive Errors and Refractive Surgery Preferred Practice Pattern. San Francisco, CA: American Academy of Ophthalmology; 2017.
10. Walters T, Bafna S, Vold S, et al. Efficacy and safety of sustained release dexamethasone for the treatment of ocular pain and inflammation after cataract surgery: results from two phase 3 studies. J Clin Exp Ophthalmol. 2016;7:1–11. doi:10.4172/2155-9570.1000572
11. Brooks CC, Jabbehdari S, Gupta PK. Dexamethasone 0.4mg sustained-release intracanalicular insert in the management of ocular inflammation and pain following ophthalmic surgery: design, development and place in therapy. Clin Ophthalmol. 2020;14:89–94. doi:10.2147/OPTH.S238756
12. Ocular Therapeutix, Inc. Dextenza. Highlights of Prescribing Information. Available from: https://www.dextenza.com/wp-content/uploads/2019/06/NDA-208742-S001-Dextenza-labeling-19Jun19.pdf.
13. Tyson SL, Bafna S, Gira JP, et al. Multicenter randomized phase 3 study of a sustained-release intracanalicular dexamethasone insert for treatment of ocular inflammation and pain after cataract surgery. J Cataract Refract Surg. 2019;45(2):204–212. doi:10.1016/j.jcrs.2018.09.023
14. Gira JP, Sampson R, Silverstein SM, Walters TR, Metzinger JL, Talamo JH. Evaluating the patient experience after implantation of a 0.4 mg sustained release dexamethasone intracanalicular insert (Dextenza): results of a qualitative survey. Patient Prefer Adherence. 2017;11:487–494. doi:10.2147/PPA.S126283
15. Barber BL, Strahlman ER, Laibovitz R, Guess HA, Reines SA. Validation of a questionnaire for comparing the tolerability of ophthalmic medications. Ophthalmology. 1997;104(2):334–342. doi:10.1016/S0161-6420(97)30314-5
16. Ngo W, Situ P, Keir N, Korb D, Blackie C, Simpson T. Psychometric properties and validation of the standard patient evaluation of eye dryness questionnaire. Cornea. 2013;32(9):1204–1210. doi:10.1097/ICO.0b013e318294b0c0
17. Lemp MA. Report of the National Eye Institute/Industry workshop on clinical trials in dry eyes. CLAO J. 1995;21(4):221–232.
18. Dixon P, Ghosh T, Mondal K, Konar A, Chauhan A, Hazra S. Controlled delivery of pirfenidone through vitamin E-loaded contact lens ameliorates corneal inflammation. Drug Deliv Transl Res. 2018;8(5):1114–1126. doi:10.1007/s13346-018-0541-5
19. Kim J, Peng CC, Chauhan A. Extended release of dexamethasone from silicone-hydrogel contact lenses containing vitamin E. J Control Release. 2010;148(1):110–116. doi:10.1016/j.jconrel.2010.07.119
20. An JA, Kasner O, Samek DA, Levesque V. Evaluation of eyedrop administration by inexperienced patients after cataract surgery. J Cataract Refract Surg. 2014;40(11):1857–1861. doi:10.1016/j.jcrs.2014.02.037
21. Center for Evidence-Based Medicine. Available from: http://www.cebm.net.
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.