Back to Journals » Open Access Journal of Clinical Trials » Volume 9
A randomized controlled trial to improve heart failure disparities: the Mālama Puʻuwai (caring for heart) Study
Authors Mau MKLM, Lim E, Kaholokula JK, Loui TMU, Cheng Y, Seto TB
Received 3 March 2017
Accepted for publication 28 May 2017
Published 3 August 2017 Volume 2017:9 Pages 65—74
DOI https://doi.org/10.2147/OAJCT.S136066
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Greg Martin
Marjorie K Leimomi Mala Mau,1 Eunjung Lim,1 Joseph Keawe‘aimoku Kaholokula,1 Taylor MU Loui,1 Yongjun Cheng,1 Todd B Seto1,2
1Department of Native Hawaiian Health, University of Hawai‘i at Mānoa, John A. Burns School of Medicine, 2Queens Heart Physician Practice, Queens Medical Center, Honolulu, HI, USA
Objective/Background: To conduct a randomized controlled trial to test the efficacy of a culturally tailored heart failure (HF) education program, to reduce HF hospital readmissions and/or cardiovascular disease death (HF outcomes) among Native Hawaiian and Other Pacific Islander (NHOPI) patients with HF.
Methods: One hundred fifty HF patients aged ≥21 years, NHOPI race, and discharged to home were enrolled and randomized to the Mālama Puʻuwai Program (MPP) or the usual care (UC). The MPP group received a culturally tailored HF program, and the UC received similar standard HF education materials. Clinical and health behavior data were measured at baseline and 12 months. HF outcomes were monitored throughout the entire study period. Two-sample t-test, chi-square, and Cox proportional hazard modeling assessed the efficacy of intervention (MPP or UC) on HF outcomes using an intention-to-treat approach. A sensitivity post hoc analysis was performed on patients who completed the full intervention (n=127).
Results: Overall, 69% were men, mean age 54.4±13.4 years, 62% were Native Hawaiian, and 24% reported methamphetamine use. More UC participants reported methamphetamine use (32% vs. 16%), hypertension (81% vs. 63%), but less myocardial infarction (27% vs. 48%). HF outcomes were higher in UC (31%) compared with MPP (19%) with higher risk for HF outcomes (hazard ratio [HR] 1.74; 95% CI: 0.89–3.40). Sensitivity post hoc analysis of intervention compliance revealed that UC was at significantly higher risk for HF outcomes than MPP (HR 2.83; 95% CI: 1.19–6.72).
Conclusions: Culturally tailored HF programs have the potential to reduce HF outcomes among compliant minority patients with HF such as NHOPI.
Keywords: cardiomyopathy, Native Hawaiian, Pacific Islander, heart failure outcomes, culturally tailored education program
Introduction
Heart failure (HF) is a major contributing factor to death and hospitalization that places a significant health burden on the US population because of increased health care costs, lower quality of life, and premature death.1,2 An estimated 5.7 million Americans over the age of 20 years are affected, with total health care costs estimated to reach $30.7 billion.1,3 Most of these costs arise from expensive HF symptom exacerbations requiring emergency visits and hospitalizations.3–5
Racial and ethnic minority populations in the US are particularly at an increased risk for developing HF as well as readmission and reduced survival from HF and cardiovascular disease (CVD). African Americans are at the greatest risk for developing HF followed by Hispanics, Whites, and Chinese, reflecting differences in the prevalence of hypertension (HTN), diabetes, and lower socioeconomic status.6 Moe and Tu found that a few of the key differences in HF across ethnic groups are underlying cause of HF, response to treatment, and age of onset in patients.7 Among Canada’s ethnic minority populations such as Southeast Asians and Chinese, HF is reported to occur at younger ages and occurs comorbidly with HTN and diabetes more frequently than with Whites.7 For African-American patients, the etiology of HF is less likely to be due to coronary heart disease compared with Whites.8–10 Among Native Hawaiian and other Pacific Islanders (NHOPIs), methamphetamine has been associated with HF and may even represent a potentially reversible form of cardiomyopathy.11,12
To improve the health outcomes (i.e., HF readmissions, premature CVD death, and so on) of HF patients, a number of intervention programs have been developed to provide patient-specific personalized educational information.13,14 Several HF educational interventions have been implemented worldwide, yet there remains uncertainty as to their universal effectiveness at reducing hospital readmissions and deaths in HF patients.15,16 In addition, many HF patients remain challenged with HF information that is often culturally irrelevant and difficult to comprehend and to apply in the context of their day-to-day lives.17,18
The objective of this study was to conduct a randomized controlled trial (RCT) to test the efficacy of the Mālama Puʻuwai Program (MPP), a culturally tailored education program, to reduce HF hospital readmissions and/or CVD death among NHOPIs with HF.
Method
Participant recruitment and eligibility
The Mālama Puʻuwai (Caring for Heart) Study (MPS) enrolled 150 NHOPIs (e.g., Native Hawaiian [NH], Samoan, Tongan, Tahitian, Maori, Marshallese, and so on) with diagnosed cardiomyopathy who were hospitalized at the Queen’s Medical Center, the largest tertiary care hospital in the State of Hawaii, where the largest concentration of NHOPIs resides.19 Between June 2006 and April 2009, potential participants were identified during the index hospitalization if they self-reported NHOPI and/or if they had a past medical history of HF or cardiomyopathy. Patients who were initially screened positive were confirmed by medical records for eligibility. The eligibility criteria included 1) ≥21 years of age, 2) International Classification of Diseases, Ninth Revision (ICD-9) code for HF or cardiomyopathy, and 3) left ventricular ejection fraction (LVEF) of ≤40% or LVEF of ≤60% and evidence of abnormal diastolic function on echocardiogram. Patients were excluded for any of the following: 1) HF due to high-output states or transient noncardiac disease, 2) with a terminal illness (<6-month survival), 3) living in nursing home or institutional facility, and 4) hemodialysis or peritoneal dialysis. All participants provided written informed consent prior to randomization. After collection of baseline data, participants were assigned to either the MPP arm or the usual care (UC) arm using a simple 1:1, unblinded randomization process using a computerized random number generator20 (Figure 1).
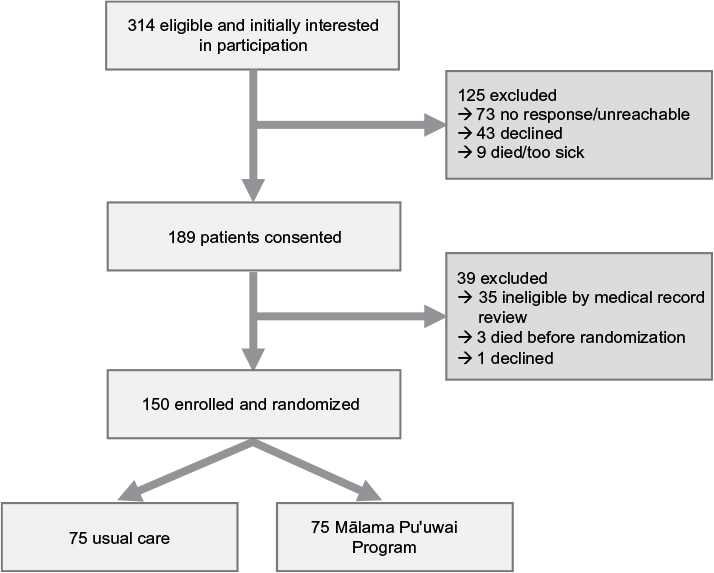 | Figure 1 Flowchart of enrollment and randomization of the Mālama Pu‘uwai Study. |
Assessment instruments
The following clinical, behavioral, medical, social history, and demographic information were collected by certified research staff interviewers at baseline and at 12-month follow-up with key clinical data (i.e., any adverse events) verified by medical record review. The interviewers were trained using a standardized procedure for administering each questionnaire including adherence to the standardized protocol, use of nonjudgmental attitudes, degree and nature of prompting, appropriate problem solving, and proper handling of participants’ comments.21
Three health behavior questionnaires were administered: Kansas City Cardiomyopathy Questionnaire (KCCQ), the 10-item short form of the Center for Epidemiological Studies of Depression Scale (CES-D), and the Short Form (12-item version 2) Health Survey (SF-12 v2). The KCCQ is a well-validated 23-item questionnaire, which has been validated with HF patients.22 The 10-item CES-D is a well-validated measure of the cognitive, affective, and behavioral symptoms of depression in which participants rank the frequency of symptoms experienced in the last week.23 The SF-12 v2 measures the mental and physical aspects of health-related quality of life across eight specific domains.24 All three health behavior questionnaires showed good internal consistency indices at baseline based on this study’s sample (i.e., Cronbach’s alpha=0.82, 0.84, and 0.85 for the KCCQ, CES-D, and SF-12 v2, respectively).
Clinical and anthropometric measurements (e.g., blood pressure, pulse, body mass index [BMI]) were measured at baseline and all research visits according to standardized research protocol.25 The medical history variables, assessed by self-report, were myocardial infarction (MI), cardiac arrhythmia, cardiac valvular disease, cerebrovascular disease, HTN, and diabetes mellitus (DM). Cardiac medications were also assessed by self-report and categorized by therapeutic class (e.g., angiotensin-converting enzyme inhibitor, angiotensin II receptor blocker, beta-blocker, diuretic, digoxin, spironolactone, aspirin, warfarin, and calcium channel blocker).
Primary cause of heart disease and Charlson comorbidity index were determined by ICD-9 codes of participants’ medical records reviewed by a physician from the index hospitalization. Ischemic heart disease was identified by the ICD-9 codes of 410–414. Charlson comorbidity index was computed based on three-digit ICD-9 codes of up to 10 diagnoses.26
Intervention program materials
The MPP, the culturally tailored heart health intervention, consisted of four education modules, which were developed based on focus group discussions and informant interviews from NHOPI patients and their caregivers who provided their perspectives on and preferences for managing their health (Supplementary material).27,28 Guidelines and educational materials from the Heart Failure Society of America also informed the development of the MPP educational topics and materials. The MPP was delivered in-person by a trained and certified nurse educator who delivered one of the four modules every 2 weeks for 8 weeks. The UC arm also consisted of four sets of written educational materials of similar content and delivered to the participant by postal mail every 2 weeks for 8 weeks. The UC arm participants also received a follow-up phone call by research staff to verify the receipt of the materials and to inquire about whether the participant had any questions on the educational materials sent. After the 8-week intervention period, all participants (MPP and UC) entered the 10-month monitoring phase when the research staff contacted patients by phone weekly for 4 weeks, then monthly for the remaining months until a total period of 12 months from randomization were completed.
Research visits and outcome assessments
All research visits were conducted according to protocol and performed by staff who were not involved with the MPP educational program delivery. All participants were tracked for hospital readmission and/or mortality until study end. HF readmission and CVD mortality were defined according to standardized protocol.29,30 All death and hospital readmissions were confirmed by medical record review and adjudicated by an independent Outcomes Committee of physicians trained and certified according to a standardized CVD outcomes adjudication protocol.29 The data were electrically captured and monitored to detect data entry errors including omission, errors, and duplicates. An independent data safety monitoring board conducted interim analyses of the MPS data every 6 months to evaluate participant safety and study performance until the end of the study. The study was approved by the Institutional Review Board at the University of Hawaii and the Queens Medical Center. This study is registered at the National Clinical Trials registry as NCT00101465.
Statistical analysis
Descriptive statistics were reported using mean and standard deviation for continuous variables and frequencies and percentages for categorical variables. Differences between the two arms were compared at baseline on all variables using chi-square tests or Fisher’s exact tests for categorical variables and two-sample t-tests for continuous variables. The rate of HF readmission or CVD death was compared using Mantel–Haenszel chi-square test and relative risks were computed.
To evaluate the effect of the MPP, an intention-to-treat (ITT) principle was applied to time-to-event analysis. Time to event was defined as the number of days from baseline to HF readmission or CVD death (defined as HF outcomes), whichever comes first. Kaplan–Meier curves were generated to illustrate the outcome between treatment arms. Cox proportional hazard models were used to assess the effect of the intervention on HF outcomes that significantly differed between study arms at baseline (i.e., history MI and history HTN). A backward elimination method was used to develop a parsimonious model that adjusted for age, gender, and significant baseline variables. As a sensitivity analysis, per-protocol (PP) analyses were performed post hoc to determine the effect of intervention compliance on the primary outcome of the study.31 PP analyses investigated the patterns of “dose–response,” defined as the number of education modules received by participant on HF outcomes. The Cox proportional hazard models were adjusted for the same covariates used in the ITT analysis. The modified ITT analysis included only participants who received all four educational modules (n=127: MPP, n=57; UC, n=70). Comparison of baseline variables and HF outcomes on the participants excluded from the modified ITT analysis found no significant differences in any baseline variables or HF outcomes between subjects in the modified ITT analysis and participants excluded from the modified ITT analysis (data not shown). All analyses were considered statistically significant if p<0.05 and were performed in SAS version 9.4.
Results
The mean age of the entire study population was 54.4 years (±13.4), with 69% men, 44% married, and 62% NH (Table 1). Overall, 24% of the participants reported a history of methamphetamine use, 49% reported a history of DM, and 72% a history of HTN (Tables 1 and 2). The two arms of the study (75 participants per arm) were well balanced with no significant differences in severity of LVEF, mean BMI, number and type of cardiac medications, as well as resting blood pressure levels at baseline (Tables 1 and 2). Significant baseline differences included a greater proportion in the UC arm reporting methamphetamine use (32% vs. 16%, p=0.02), nonischemic cause for HF (65% vs. 48%, p=0.03), and history HTN (81% vs. 63%, p=0.01) (Tables 1 and 2). In the MPP arm, history MI was significantly higher than in the UC arm (32% vs. 16%, p=0.02) (Table 2).
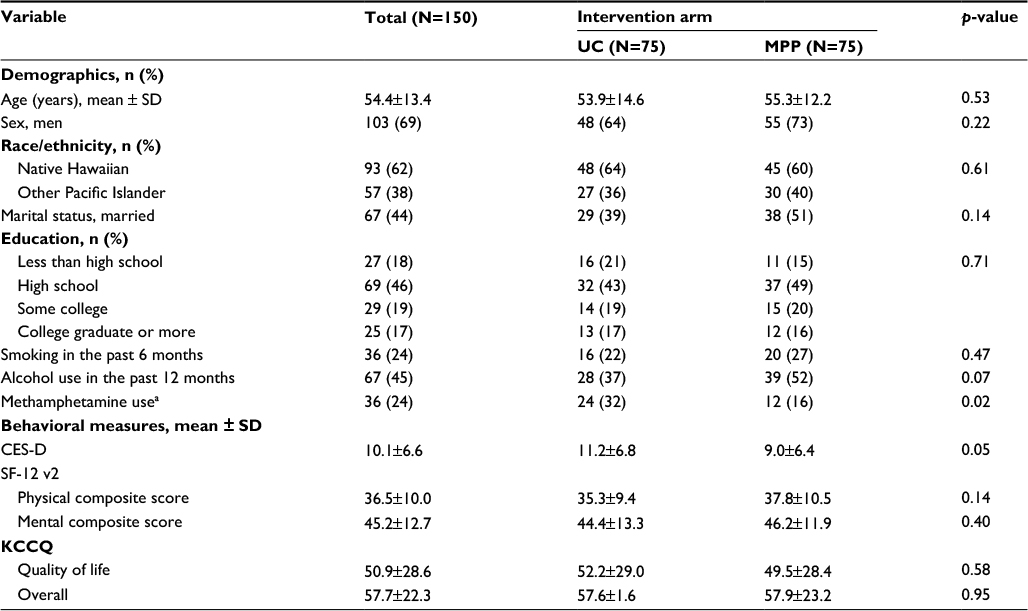 | Table 1 Comparison of baseline demographics and behavioral measures by intervention (the Mālama Pu‘uwai Study, N=150) Note: aBy self-report. Abbreviations: CES-D, Center for Epidemiological Studies of Depression Scale; KCCQ, Kansas City Cardiomyopathy Questionnaire; MPP, Mālama Pu‘uwai Program; SF-12 v2, Short Form 12-item version 2 Health Survey; UC, usual care. |
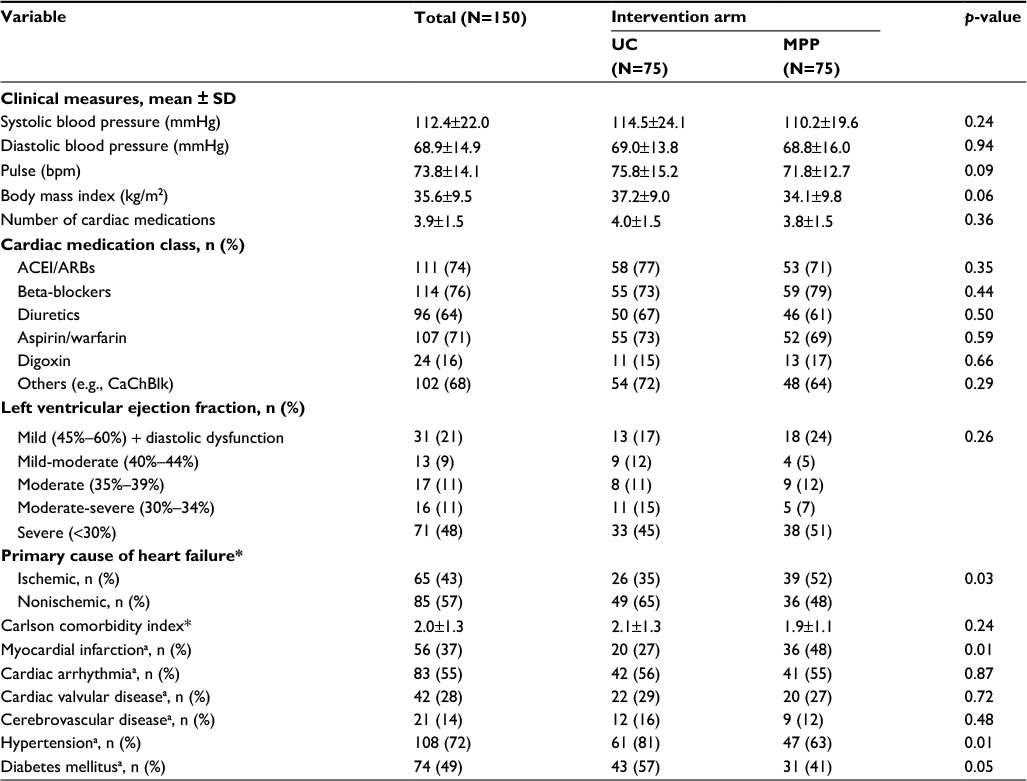 | Table 2 Comparison of baseline clinical characteristics by intervention (the Mālama Pu‘uwai Study, N=150) Notes: aBy self-report. *By medical record review. Abbreviations: ACEI, angiotensin-converting-enzyme inhibitor; ARB, angiotensin II receptor blocker; LVEF, left ventricular ejection fraction; MPP, Mālama Pu‘uwai Program; UC, usual care. |
Among the 150 participants, only 11 deaths occurred during the study period (UC=5 vs. MPP=6) and was not significant (Table 3A). A total of 58 all-cause readmissions occurred with 29 (50%) hospital readmissions due to HF (Table 3B). Eight participants (four in each arm) had CVD death, while HF readmissions were 19 (25%) in UC versus 10 (13%) MPP groups, indicating a 47% reduction in HF readmissions in the MPP arm (p=0.06). Compared with UC, fewer participants in the MPP experienced HF outcomes, a combination of HF readmission and CVD death, resulting in a 39% reduction over UC (p=0.09) although not statistically significant (Table 3A).
 | Table 3A Relative risk of HF outcomes using intention-to-treat principle (the Mālama Pu‘uwai Study, N=150) Notes: Percent reduction was calculated by dividing the percent difference between groups by the UC group percentage. Positive reduction indicates the MPP group is better. Abbreviations: CVD, cardiovascular disease; HF, heart failure; MPP, Mālama Pu‘uwai Program; RR, relative risk; UC, usual care. |
 | Table 3B Relative risk of HF outcomes among participants completing all education modules using modified intention-to-treat principle (N=127) Notes: Percent reduction was calculated by dividing the percent difference between groups by the UC group percentage. Positive reduction indicates that the MPP group is better. Abbreviations: CVD, cardiovascular disease; HF, heart failure; MPP, Mālama Pu‘uwai Program; RR, relative risk; UC, usual care. |
Figure 2 illustrates a Kaplan–Meier curve using an ITT approach. At 6 months, HF outcomes occurred for 16 UC participants (21%) and 12 MPP participants (16%). To assess the efficacy of the MPP, a Cox proportional hazard model was performed using a backward elimination method with age, gender, the significant baseline variables (i.e., methamphetamine use; primary cause of heart disease; history of MI, HTN, DM, and CES-D), and their interactions with treatment arm. None of the significant baseline variables remained in the final model, resulting in adjusting for age and gender only. In the final model, the UC arm had a higher risk for HF outcomes compared with the MPP arm though it did not reach statistical significance (hazard ratio [HR] 1.74, 95% CI: 0.89–3.40, p=0.11). PP sensitivity analyses were performed to determine the impact of intervention compliance on primary HF outcomes. Compared to UC, we found improved readmission-free intervals for the MPP with increasing number of modules received in a “dose–response” pattern. The HRs for the UC versus the MPP were 1.72 (95% CI=0.89–3.40), 2.19 (95% CI=1.02–4.70), 2.10 (95% CI=0.98–4.49), and 2.83 (95% CI=1.19–6.72) with completion of 1, 2, 3, or 4 education modules, respectively (data not shown).
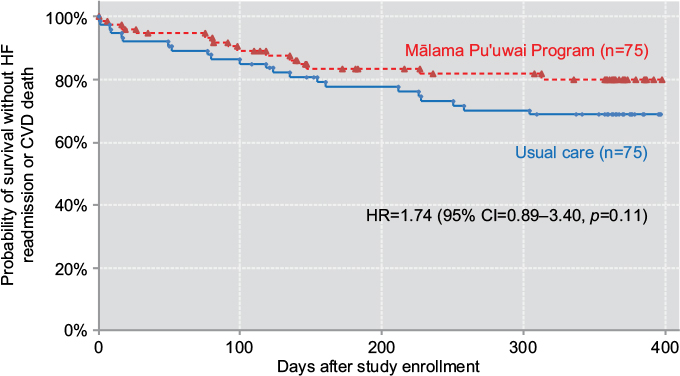 | Figure 2 Kaplan–Meier curve of heart failure outcomes (heart failure readmission and cardiovascular disease death) using modified intention-to-treat approach (N=150). Notes: For time-to-event analysis, Cox proportional hazard model was used adjusted for age and gender. Event was defined as heart failure readmission or mortality due to cardiovascular disease. Abbreviations: CVD, cardiovascular disease; HF, heart failure; HR, hazard ratio; CI, confidence interval. |
Using a modified ITT approach that included only participants who received all four modules/sets (n=127, MPP=57, UC=70), we found 7 participants (12%) in the MPP readmitted for HF or CVD death compared with 21 participants (30%) in the UC (relative risk 0.41, 95% CI 0.19–0.89, p=0.02), indicating a 59% reduction (Table 3B). Cox proportional HR for the UC was 2.83 times higher than those of MPP (95% CI=1.19–6.72, p=0.02), indicating that the MPP had reduced HF outcomes by more than twofold compared with UC participants who received the full HF education program (Figure 3). The Cox proportional hazard model using a modified ITT approach parallels the primary analysis trends using an ITT approach and suggests that intervention compliance of the MPP is likely to have been a key factor in reducing HF outcomes in NHOPIs with HF.
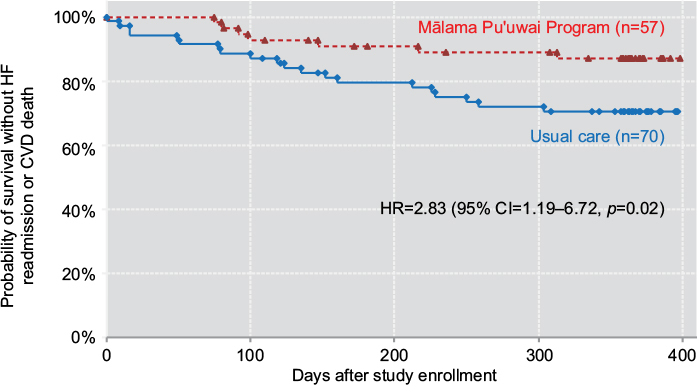 | Figure 3 Kaplan–Meier curve of heart failure outcomes (heart failure readmission and cardiovascular disease death) using modified intention-to-treat approach* (N=127). Notes: *Modified intention to treat = inclusive of all participants who completed entire education program (four modules). Abbreviations: CVD, cardiovascular disease; HR, hazard ratio; CI, confidence interval; HF, heart failure. |
Conclusion
To our knowledge, this is the first study to investigate the efficacy of a culturally tailored HF education program, entitled the MPP, to reduce HF outcomes in NHOPIs. The MPP was designed to address cultural factors (e.g., cultural value of health, cultural foods relevant to HF [i.e., salt], and coping with emotions culturally) while ensuring that core HF self-management skills would be enabled to educate patient’s and/or their family support system as a means to improve health outcomes.27,28,32 Our study focused solely on NHOPIs with HF because they are at high risk for HF disparities and are often excluded or nonexistent in larger HF efficacy trials aimed at improving HF outcomes.27,33 We hypothesized that a culturally tailored intervention would be necessary and better than UC among NHOPIs with HF because NHOPIs have a unique sociocultural, linguistic, and demographic background that influences health behaviors that are fundamental to patient self-management of HF care.11,27,33–35 Interestingly, NHOPIs enrolled in this study were also clinically different compared to the general HF population as they were younger (mean age 54.4 years), had a higher BMI (mean 35.6 kg/m2), a higher proportion were methamphetamine users (24%), and had a primary nonischemic cause of HF (57%).1,6–8,12 We propose that the cumulative effect of these risk factors could pose important challenges to day-to-day management of HF.36,37 Although the MPP was not specifically designed to address illicit drug use or other social determinants experienced by NHOPI HF patients, the program did include NHOPI cultural factors (i.e., eating cultural foods, NH language, and motivational NH proverbs). Thus, the MPP provided a cultural context for the learning of evidence-based HF self-management to NHOPI patients who are at high risk for adverse health outcomes. In this study, we found that culturally tailored HF education programs, such as MPP, are effective at preventing adverse health outcomes (i.e., HF readmissions or CVD death), but only with full compliance of the program.
Not surprisingly, our results are similar to other minority populations in which HF is not a “cardiogeriatric” syndrome.34,38 Indeed, our results parallel the demographic profile and clinical characteristics of African Americans in the US, Asians in Canada, and Australian Aborigines with HF in which the mean age of HF patients are 10–15 years younger than Whites with HF.13,34 Our results are consistent with the literature on HF intervention programs that reported that most, but not all, nonpharmacological interventions were found to reduce HF outcomes compared with the UC.13,39 Our results similarly showed trends toward improved outcomes that reached significance only after conducting a sensitivity analysis for compliance that included only participants who received the full four modules/sets of educational materials (modified ITT).
One strength of our study is the long-term outcomes (12 months) and the RCT design to test an intervention that integrates social, cultural, and clinical factors in a high-risk minority population. More alternative approaches are needed to engage high-risk patient populations and their families to overcome the complex task of HF disease management that is patient centered and family supported.7,40–42 The majority of HF RCTs examined readmission at 30 days to 6 months postdischarge compared with our study that followed participants for 12 months.34 Of note, we acknowledge a number of limitations of our study including enrollment of a single racial population of HF patients, NHOPIs, which may limit the generalizability of our findings on efficacy of the MPP to other minority populations such as Blacks, Hispanic/Latino, or Asian HF patients who are also at high risk but have distinctly different cultural and sociodemographic circumstances. Our study does suggest that appropriately designed nonpharmacological programs for high-risk HF patients may be a promising population-specific approach to improve HF outcomes. Another limitation of our study was the recruitment of patients from a single tertiary care hospital, though it is the largest hospital in a state that has the highest concentration of NHOPI in the US. These factors may have contributed to the relatively small sample size of NHOPIs enrolled. This, in turn, may have impacted the study’s ability to reach statistical significance despite positive trends.
In summary, the results of the MPS demonstrate the importance of intervention compliance in educational or behavioral interventions to optimize clinical outcomes. Many studies have found a “dose effect” with educational interventions for disease management in which the number of lessons received or attended was associated with better clinical outcomes.43–45 This is especially important for severe and complicated medical conditions, such as HF, in which it is important that patients learn about and manage all aspects related to their medical condition (e.g., complex medication regime, drastic sodium reduction in diet, and reducing edema). A “dose–response” of behavior changes according to the number of educational modules received has been reported in other behavior interventions similar to the MPP.43–45 The MPP effectiveness in reducing HF outcomes is also consistent with other educational intervention studies in which intervention “compliance” has an important role in determining efficacy.
Our study also contributes to our understanding of HF disparities, but only in a single minority population, NHOPIs, and this may limit the generalizability of our results to other HF patients. However, the MPS is the largest HF outcome RCT among NHOPIs, and our results are consistent with multiple studies among other racial/ethnic minorities that have reported positive results with educational programs to improve readmission rates.34,40,46 This suggests that among similar high-risk ethnic minority patients, ethnic-specific, tailored interventions may offer promising tools for improving health outcomes.
Acknowledgments
This study was funded by the National Institutes of Health (NIH) through the following grants: U01 HL 079163, P20 MD 000173 and MKLMM was partially supported by S21 MD 000228. EL was partially supported by U54 MD 007584. The content is solely the responsibility of the authors and does not necessarily reflect the official opinion of the NIH, the National Heart, Lung and Blood Institute (NHLBI), or the National Institute on Minority Health and Health Disparities (NIMHD).
From multiple grant awards of the NIH (specifically, U01 HL 0179163–NHLBI, P20 MD 000173–NIMHD and U01 HL 079152-NHLBI).
Disclosure
The authors report no conflicts of interest in this work.
References
Mozaffarian D, Benjamin EJ, Go AS, et al. Heart disease and stroke statistics – 2015 update: a report from the American Heart Association. Circulation. 2015;131(4):e29–e322. | ||
Fonarow GC. Heart failure disease management programs: not a class effect. Circulation. 2004;110(23):3506–3508. | ||
Rich MW, Nease RF. Cost-effectiveness analysis in clinical practice: the case of heart failure. Arch Intern Med. 1999;159(15):1690–1700. | ||
Russo CA, Andrews RM. The national hospital bill: the most expensive conditions, by payer, 2004: statistical brief #13. Healthcare Cost and Utilization Project (HCUP) Statistical Briefs. Rockville, MD: Agency for Healthcare Research and Quality (US); 2006. | ||
Ross JS, Mulvey GK, Stauffer B, et al. Statistical models and patient predictors of readmission for heart failure: a systematic review. Arc Intern Med. 2008;168(13):1371–1386. | ||
Bahrami H, Kronmal R, Bluemke DA, et al. Differences in the incidence of congestive heart failure by ethnicity: the multi-ethnic study of atherosclerosis. A Interl Med. 2008;168(19):2138–2145. | ||
Moe GW, Tu J. Heart failure in the ethnic minorities. Curr Opin Cardiol. 2010;25(2):124–130. | ||
Yancy CW. Heart failure in African Americans: a cardiovascular engima. J Card Fail. 2000;6(3):183–186. | ||
Afzal A, Ananthasubramaniam K, Sharma N, et al. Racial differences in patients with heart failure. Clin Cardiol. 1999;22(12):791–794. | ||
Hunt SA, Abraham WT, Chin MH, et al. ACC/AHA 2005 Guideline Update for the Diagnosis and Management of Chronic Heart Failure in the Adult: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines (Writing Committee to Update the 2001 Guidelines for the Evaluation and Management of Heart Failure): developed in collaboration with the American College of Chest Physicians and the International Society for Heart and Lung Transplantation: endorsed by the Heart Rhythm Society. Circulation. 2005;112(12):e154–e235. | ||
Yeo KK, Wijetunga M, Ito H, et al. The association of methamphetamine use and cardiomyopathy in young patients. Am J Med. 2007;120(2):165–171. | ||
Mau MK, Asao K, Efird J, et al. Risk factors associated with methamphetamine use and heart failure among native Hawaiians and other Pacific Island peoples. Vasc Health Risk Manag. 2009;5(1):45–52. | ||
Gwadry-Sridhar FH, Flintoft V, Lee DS, Lee H, Guyatt GH. A systematic review and meta-analysis of studies comparing readmission rates and mortality rates in patients with heart failure. Arch Intern Med. 2004;164(21):2315–2320. | ||
Krumholz HM, Amatruda J, Smith GL, et al. Randomized trial of an education and support intervention to prevent readmission of patients with heart failure. J Am Coll Cardio. 2002;39(1):83–89. | ||
Jaarsma T, van der Wal MH, Lesman-Leegte I, et al. Effect of moderate or intensive disease management program on outcome in patients with heart failure: coordinating study evaluating outcomes of advising and counseling in heart failure (COACH). Arch Intern Med. 2008;168(3):316–324. | ||
Faxon DP, Schwamm LH, Pasternak RC, et al. Improving quality of care through disease management: principles and recommendations from the American Heart Association’s Expert Panel on Disease Management. Circulation. 2004;109(21):2651–2654. | ||
Pattenden JF, Roberts H, Lewin RJ. Living with heart failure; patient and carer perspectives. Eur J Cardiovasc Nurs. 2007;6(4):273–279. | ||
Ross A, Ohlsson U, Blomberg K, Gustafsson M. Evaluation of an intervention to individualise patient education at a nurse-led heart failure clinic: a mixed-method study. J Clin Nurs. 2015;24(11–12):1594–1602. | ||
U.S. Census Bureau. Native Hawaiian and other Pacific Islander alone or in combination with one or more other races. American Fact Finder 2015; U.S. Census Bureau, 2011-2015 American Community Survey 2015-year Estimates. Available from: http://factfinder.census.gov/faces/tableservices/jsf/pages/productview.xhtml?pid=ACS_15_5YR_B02012&prodType=table. Accessed May 24, 2017. | ||
Schulz KF, Altman DG, Moher D; Group C. CONSORT 2010 statement: updated guidelines for reporting parallel group randomised trials. BMJ. 2010;340:c332. | ||
Trochim WMK, Donnelly JP. Survey research. In: Baird M; Staudt M; Stranz M eds. The Research Methods Knowledge Base. 3rd ed. Mason, OH: Atomic Dog, Cengage Learning; 2008:100–124. | ||
Green CP, Porter CB, Bresnahan DR, Spertus JA. Development and evaluation of the Kansas city cardiomyopathy questionnaire: a new health status measure for heart failure. J Am Col Cardio. 2000;35(5):1245–1255. | ||
Radloff LS. The CES-D scale: a self-report depression scale for research in the general population. Appl Psychol Meas. 1977;1(3):385–401. | ||
Ware J Jr, Kosinski M, Keller SD. A 12-item short-form health survey: construction of scales and preliminary tests of reliability and validity. Med Care. 1996;34(3):220–233. | ||
Lohman TG, Roche AF, Martorell R. Anthropometric Standardization Reference Manual. Champaign, IL: Human Kinetic Books; 1988. | ||
Charlson ME, Pompei P, Ales KL, MacKenzie CR. A new method of classifying prognostic comorbidity in longitudinal studies: development and validation. J Chronic Dis. 1987;40(5):373–383. | ||
Kaholokula JK, Saito E, Shikuma C, Look M, Spencer-Tolentino K, Mau MK. Native and pacific health disparities research. Hawaii Med J. 2008;67(8):218–219, 222. | ||
Kaholokula JK, Saito E, Mau MK, Latimer R, Seto TB. Pacific Islanders’ perspectives on heart failure management. Patient Educ Couns. 2008;70(2):281–291. | ||
Luepker RV, Apple FS, Christenson RH, et al. Case definitions for acute coronary heart disease in epidemiology and clinical research studies: a statement from the AHA council on epidemiology and prevention; AHA statistics committee; world heart federation council on epidemiology and prevention; the European society of cardiology working group on epidemiology and prevention; centers for disease control and prevention; and the national heart, lung, and blood institute. Circulation. 2003;108(20):2543–2549. | ||
Adams HP Jr, Bendixen BH, Kappelle LJ, et al. Classification of subtype of acute ischemic stroke. Definitions for use in a multicenter clinical trial. TOAST. Trial of Org 10172 in acute stroke treatment. Stroke. 1993;24(1):35–41. | ||
Thabane L, Mbuagbaw L, Zhang S, et al. A tutorial on sensitivity analyses in clinical trials: the what, why, when and how. BMC Med Res Methodol. 2013;13:92. | ||
Bos-Touwen I, Jonkman N, Westland H, et al. Tailoring of self-management interventions in patients with heart failure. Curr Heart Fail Rep. 2015;12(3):223–235. | ||
Mokuau N, DeLeon PH, Kaholokula JK, Soares S, Tsark JU, Hala C. Challenges and Promise of Health Equity for Native Hawaiians. 2016; Discussion Paper. Available from: https://nam.edu/wp-content/uploads/2016/10/Challenges-and-Promise-of-Health-Equity-for-Native-Hawaiians.pdf. Accessed May 24, 2017. | ||
Davidson PM, Newton PJ, Tankumpuan T, Paull G, Dennison-Himmelfarb C. Multidisciplinary management of chronic heart failure: principles and future trends. Clin Ther. 2015;37(10):2225–2233. | ||
DeWalt DA, Malone RM, Bryant ME, et al. A heart failure self-management program for patients of all literacy levels: a randomized, controlled trial [ISRCTN11535170]. BMC Health Serv Res. 2006;6:30. | ||
Slim AM, Thomas H, Parish R, Mansi I. Comparison of outcomes of illicit drug users and nonusers hospitalized with heart failure. Am J Cardiol. 2012;110(4):558–561. | ||
Katz AM. The “modern” view of heart failure: how did we get here? Circ Heart Fail. 2008;1(1):63–71. | ||
Sharma A, Colvin-Adams M, Yancy CW. Heart failure in African Americans: disparities can be overcome. Cleve Clin J Med. 2014;81(5):301–311. | ||
Boyde M, Turner C, Thompson DR, Stewart S. Educational interventions for patients with heart failure: a systematic review of randomized controlled trials. J Cardiovasc Nurs. 2011;26(4):E27–E35. | ||
Adib-Hajbaghery M, Maghaminejad F, Abbasi A. The role of continuous care in reducing readmission for patients with heart failure. J Caring Sci. 2013;2(4):255–267. | ||
Sperry BW, Ruiz G, Najjar SS. Hospital readmission in heart failure, a novel analysis of a longstanding problem. Heart Fail Rev. 2015;20(3):251–258. | ||
Vasilevskis EE, Kripalani S, Ong MK, et al. Variability in implementation of interventions aimed at reducing readmissions among patients with heart failure: a survey of teaching hospitals. Acad Med. 2016;91(4):522–529. | ||
Brady TJ, Kruger J, Helmick CG, Callahan LF, Boutaugh ML. Intervention programs for arthritis and other rheumatic diseases. Health Educ Behav. 2003;30(1):44–63. | ||
Parthasarathy S, Subramanian S, Quan SF. A multicenter prospective comparative effectiveness study of the effect of physician certification and center accreditation on patient-centered outcomes in obstructive sleep apnea. J Clin Sleep Med. 2014;10(3):243–249. | ||
Bevans M, Wehrlen L, Castro K, et al. A problem-solving education intervention in caregivers and patients during allogeneic hematopoietic stem cell transplantation. J Health Psychol. 2014;19(5):602–617. | ||
Sisk JE, Hebert PL, Horowitz CR, McLaughlin MA, Wang JJ, Chassin MR. Effects of nurse management on the quality of heart failure care in minority communities: a randomized trial. Ann Intern Med. 2006;145(4):273–283. |
Supplementary material
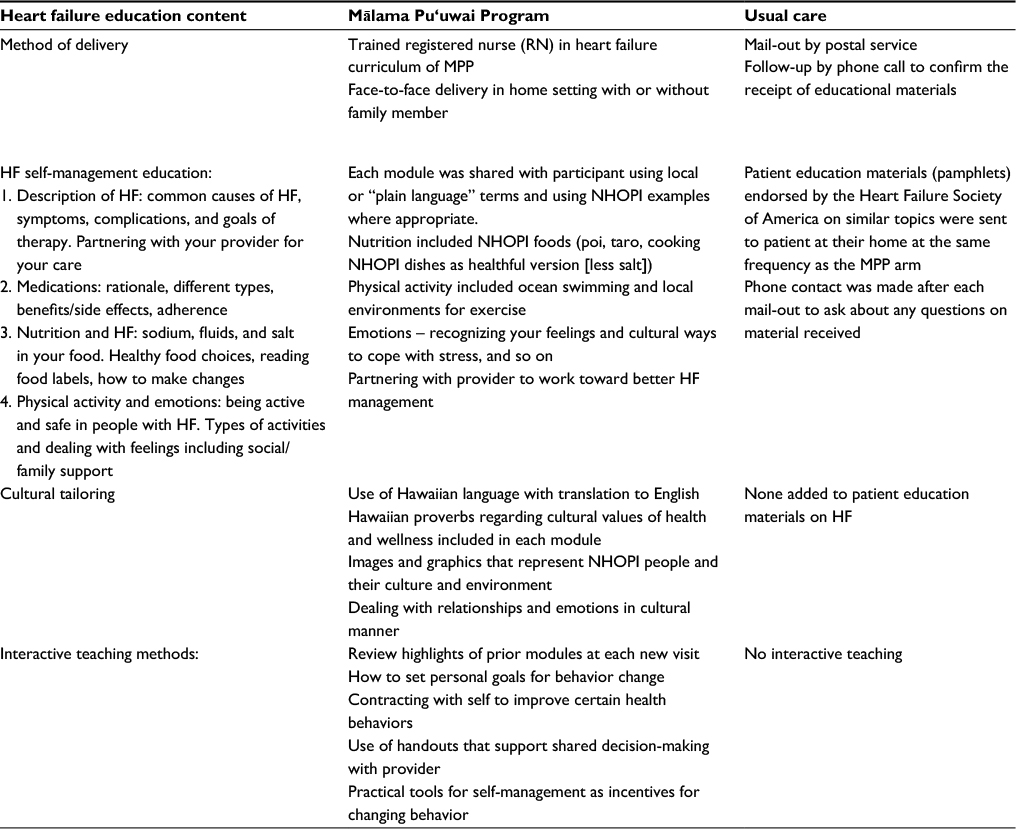 | Comparison of Mālama Pu‘uwai Program and Usual Care Interventions (the Mālama Pu‘uwai Study) Abbreviations: HF, heart failure; MPP, Mālama Pu‘uwai Program; RN, registered nurse; NHOPI, Native Hawaiian and other Pacific Islander. |
 © 2017 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2017 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.