Back to Journals » Local and Regional Anesthesia » Volume 16
A Randomized Control Trial to Compare Hemodynamic Parameters of Patients Undergoing Percutaneous Nephrolithotomy Under Combined Spinal-Epidural and General Anesthesia in a Tertiary Hospital
Authors Sankar K ![]() , Anand K
, Anand K ![]() , Ramani S, Gayathri B
, Ramani S, Gayathri B ![]()
Received 16 March 2023
Accepted for publication 3 May 2023
Published 18 May 2023 Volume 2023:16 Pages 41—49
DOI https://doi.org/10.2147/LRA.S410510
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Stefan Wirz
Ksheerabdhi Sankar, Kuppusamy Anand, Swetha Ramani, Balasubramaniam Gayathri
Department of Anesthesiology, SRM Medical College Hospital and Research Centre, Potheri, 603203, India
Correspondence: Kuppusamy Anand, Department of Anesthesiology, SRM Medical College Hospital and Research Centre, Room No. 206, B Block, Second Floor, Potheri, 603203, India, Tel +91-98652 82288, Email [email protected]
Background and Aim: Percutaneous nephrolithotomy (PCNL) under epidural anesthesia has been reported to have few advantages over general anesthesia, like lower postoperative pain and less need for analgesics. There are limited studies on PCNL being performed under neuraxial anesthesia in supine position. Hence the present study was conceived to compare hemodynamic parameters in patients undergoing percutaneous nephrolithotomy (PCNL) in the supine position under combined spinal-epidural with general anesthesia (GA).
Material and Methods: A prospective, randomized control trial was conducted among 90 patients who were posted to undergo elective percutaneous nephrolithotomy in the the supine position, after obtaining Institutional Ethical Committee (IEC) approval and CTRI (Clinical Trial Registry - India) registration. Patients were randomly allotted to undergo surgery either under general anesthesia (group GA) or combined spinal epidural anesthesia (group CSE) by computer-generated random number method. Hemodynamic parameters, postoperative analgesic requirement and incidence of blood transfusion were recorded and analyzed.
Results: There was no significant difference between the two groups with respect to gender, ASA grade, surgery duration, calculus size and pulse rate. There was a statistically significant reduction in mean arterial pressure from 5 to 50 minutes of surgery and less incidence of blood transfusion in patients in the CSE group. Patients who underwent PCNL in the supine position under CSE required lesser analgesics postoperatively compared to those under general anesthesia.
Conclusion: Combined spinal epidural analgesia can be used as an alternative to general anesthesia for patients undergoing PCNL in the supine position in view of less MAP and reduced postoperative analgesic and blood transfusion requirement.
Keywords: pulse rate, mean arterial pressure, percutaneous nephrolithotomy, ureteroscopy, supine position
Introduction
The preferred method of treatment of large renal calculi, stag horn calculi and calculi that are resistant to extracorporeal shockwave lithotripsy and ureteroscopy is percutaneous nephrolithotomy (PCNL). General, regional or local anesthesia can be administered to perform PCNL.1 Nowadays, PCNL is also carried out in the supine position while the patient is administered general anesthesia for better respiratory control and increased patient comfort.2 However, general anesthesia has the risk of polypharmacy, atelectasis of the lungs and postoperative nausea and vomiting.3,4 The spinal anesthesia (SA) is a safe and well-tolerated treatment option, especially for older patients with pulmonary and cardiac comorbidities. However, during SA, if the process takes longer than expected or the anesthesia starts to wear off during the operation, it is challenging to convert to GA, especially in the prone position. This problem can be solved by placing an epidural catheter in addition to the SA, through which a local anesthetic top up can be given, if needed. On analysis of the literature, there is a paucity of information about the risks and benefits of neuraxial blockade in patients undergoing PCNL in a supine position.5,6 Hence we devised this study to compare hemodynamic parameters during combined epidural-spinal with general anesthesia in patients undergoing percutaneous nephrolithotomy in the supine position. The secondary objectives were to compare postoperative analgesic consumption and incidence of blood transfusion in both groups.
Material and Methods
A prospective, randomized control trial was conducted in patients posted for PCNL in the Department of Anesthesiology at a tertiary medical centre in India for the duration of one and half years (2021–22). The present study was conducted after getting Institutional Ethical Committee (IEC), SRM Medical College hospital and Clinical Trial Registry India (CTRI) approval (CTRI/2021/04/032655). This study adhered to ethical principles and good clinical practices set out in the Declaration of Helsinki.
All patients were clearly explained to about the risks and benefits of intervention and informed consent was obtained before enrolment. The study included patients who were assessed under ASA PS I/II and underwent PCNL in the supine position under general anesthesia or combined spinal epidural anesthesia. Patients with a deformity in spine, infection at the injection site, coagulation disorders, neuromuscular or psychiatric disorder or chronic pain, hypertension, diabetes, hypersensitive to local anesthetics, substance abusers, patients with a solitary kidney and patients who were posted for a bilateral PCNL were excluded from the study.
Patients were randomly allocated into two groups general anesthesia (group GA) and combined spinal epidural anesthesia (group CSE) by computer generated random number code. The randomization code was hidden from the investigator by serially numbered opaque sealed envelope (SNOSE) method. After shifting to the operating room, patients were connected to standard monitors like an electrocardiogram and pulse oximeter, non-invasive blood pressure, temperature, capnography and baseline parameters were recorded.
Anesthesia Management
GA Group
General anesthesia was induced with Inj. propofol 2 mg/kg, fentanyl 2 mcg/kg and trachea was intubated with Inj. atracurium 0.5 mg/kg. Anesthesia was maintained with air-oxygen mixture and sevoflurane. Mechanical ventilation was set with a tidal volume of 8 mL/kg ideal body weight (IBW) and zero-positive end-expiratory pressure. Once the patient met the extubation criteria at the end of the procedure, the neuromuscular blockade was reversed and the trachea was extubated.
CSE Group
Epidural anesthesia was administered with the patient in a sitting position using 18G Tuohy needle in T9-10, T10-11 interspinous space. Epidural space was identified by loss of resistance to air and a catheter was introduced and secured with itstip at T8. Spinal anesthesia was performed at L3-L4 level with 15 mg of 0.5% hyperbaric bupivacaine using a 25G Quincke needle. Patients were monitored for 10 minutes for adequate sensory levels up to T6 before starting surgery. Epidural anesthesia was initiated with an incremental bolus of 8 mL of 0.25% levobupivacine when sensory level descended below T10. Mean arterial pressure below 80 mmHg or 20% from the baseline was treated by Inj. ephedrine 6 mg boluses and crystalloids and all pulse rate reductions below 60 were treated by intravenous atropine.
PCNL was performed on all patients in the supine position. Initially patients underwent cystoscopic ureteric catheterization in the lithotomy position. Under fluoroscopic direction, the tract was dilated using successive dilators up to 24 Fr–28 Fr after which an appropriate sized Amplatz sheath was deployed. A nephroscope was inserted into the collection system, and stones were shattered with a pneumatic lithotripter and fragments were retrieved with a grasper. At the end of the procedure, all patients received a double J (DJ) stent, and the insertion of a nephrostomy tube was optional, depending on the surgeon’s discretion. The epidural catheter was removed at the end of the procedure and postoperative analgesia was planned with intravenous paracetamol and tramadol.
Outcome Evaluation
Patients were monitored for hemodynamic changes (PR/MAP) every 5 minutes intraoperatively and every hour postoperatively for 24 hours. Blood loss was estimated clinically till “maximal allowable limit” was reached and confirmed by estimating point of care hemoglobin. A blood transfusion was then initiated as per institutional protocol. Post-operative pain was monitored with a visual analog score every 4 hours. Patients were administered Inj.paracetemol 1 gm IV thrice daily as a baseline analgesic and Inj. tramadol 100 mg IV bolus was given if VAS ≥ 4. Surgery time was measured from starting cystoscopy till PCNL was completed. Data were collected by a resident anesthesiologist using a structured proforma which contained patient name, age, gender, ASA PS classification, surgery time, calculus size, pulse rate and mean arterial pressure at various time lines, total post-op analgesic requirement and patients requiring blood transfusion.
Sample Size Estimation
Based on a pilot study in 10 patients (five from each group), we determined that a sample size of 43 in each group would be sufficient to detect significant differences between mean arterial pressure, with a power of 95% and a significance level of 5%. The sample size was increased to 45 patients in each group, to accommodate predicted drop-outs of around 10% from the study.
Statistical Analysis
The data were entered into Microsoft Office Excel 2013 and analyzed using SPSS 21 software. Continuous variables were expressed as mean and standard deviation while categorical variables were expressed as frequency and proportion. Independent sample t-test was used to compare two means. Chi square test was employed to compare the distribution of qualitative variables between the groups. All tests were two tailed and results were considered statistically significant if the p-value was <0.05.
Results
The flow of the patients in both groups is depicted in the CONsolidated Standards of Reporting Trials (CONSORT) diagram (Figure 1). A total of ninety four patients were assessed and enrolled into the trial. After exclusion of four patients for not fulfilling inclusion criteria, data from ninety patients were analyzed. On analysis of demographic data, we found no significant difference between both groups with respect to gender and ASA physical status, surgery time and calculus size. The demographic data are depicted in Table 1. There was no statistically significant difference between the groups with respect to pulse rate at various timelines up to 120 minutes (Figure 2). The results are summarized in Table 2. There was a significant reduction in MAP in the CSE group when compared with the GA group starting from 5 to 50 minutes (Figure 3). Comparisons of MAP between both groups are depicted in Table 3.
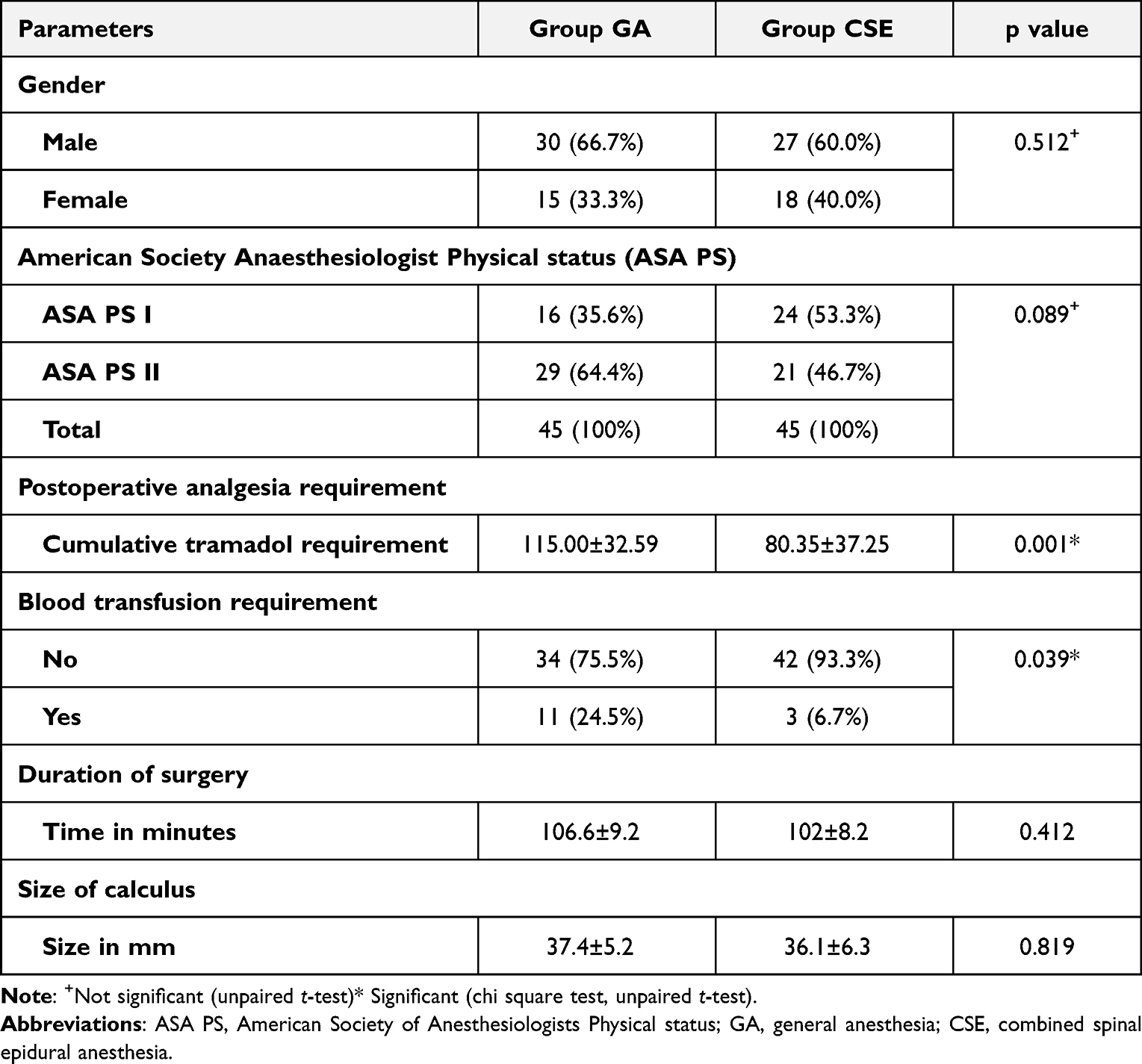 |
Table 1 Comparison of Demographic Characteristics, Blood Transfusion and Postoperative Analgesic Requirements |
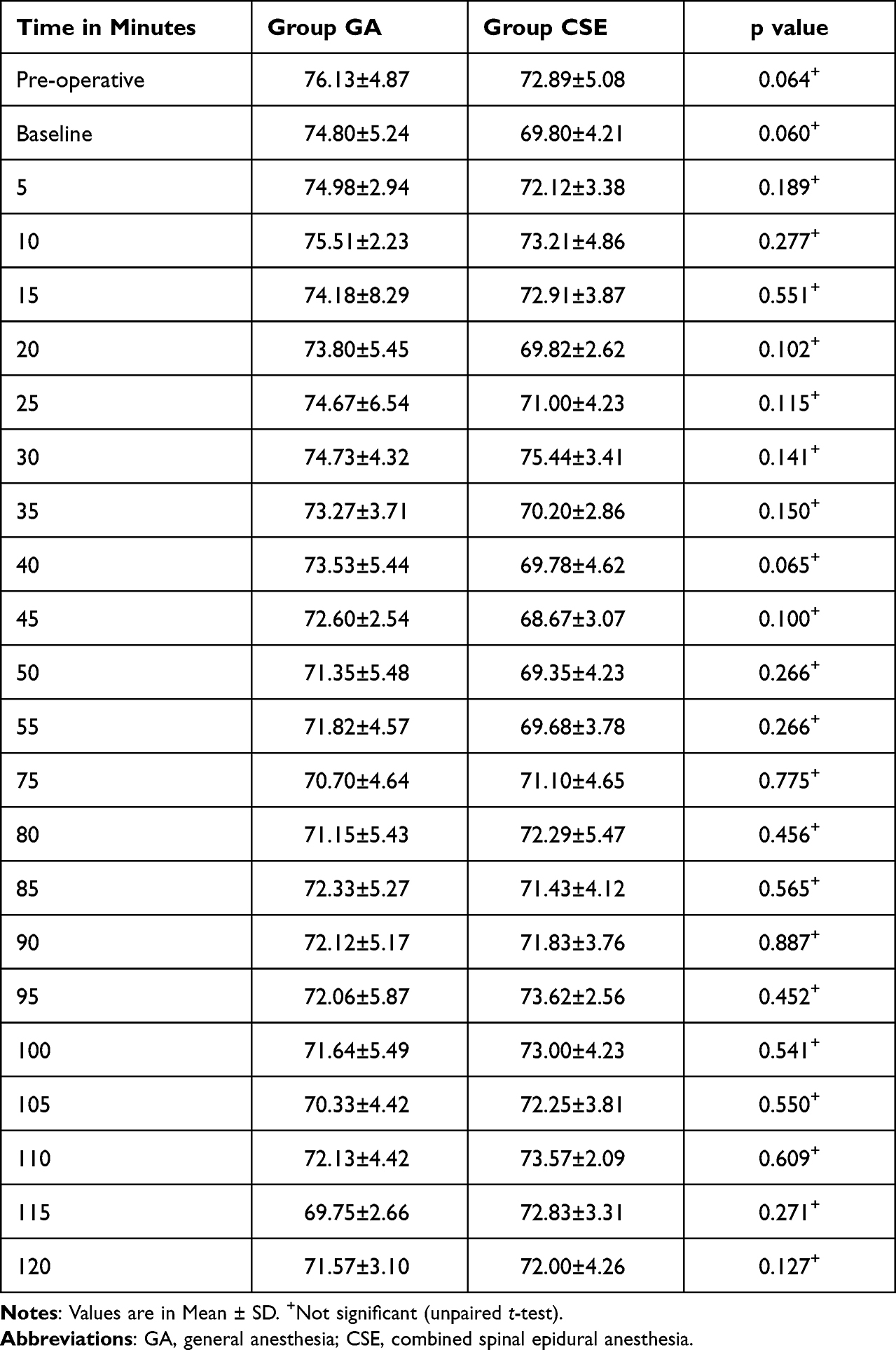 |
Table 2 Comparison of Pulse Rate Between Study Groups |
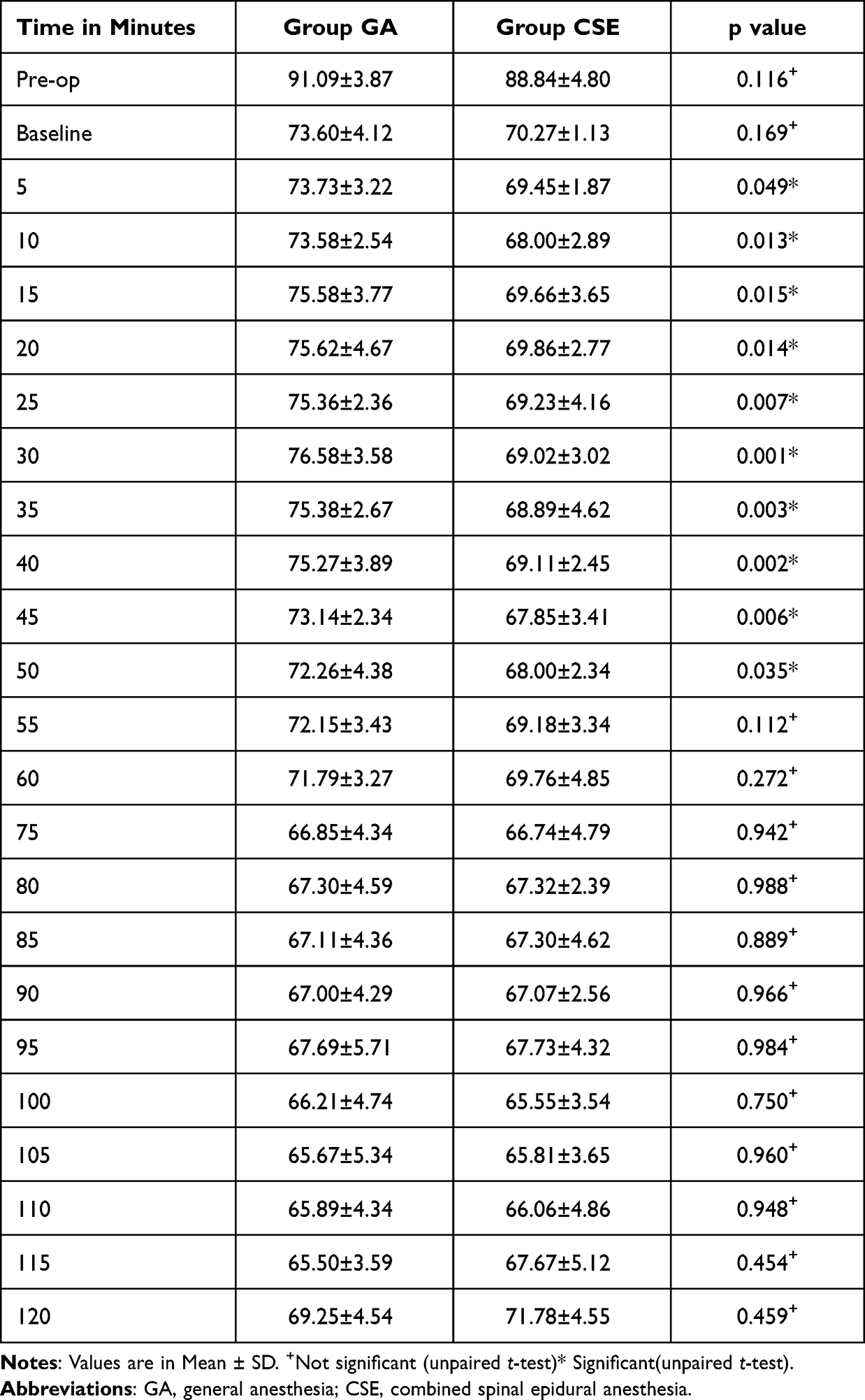 |
Table 3 Comparison of Mean Arterial Pressure Between Two Groups |
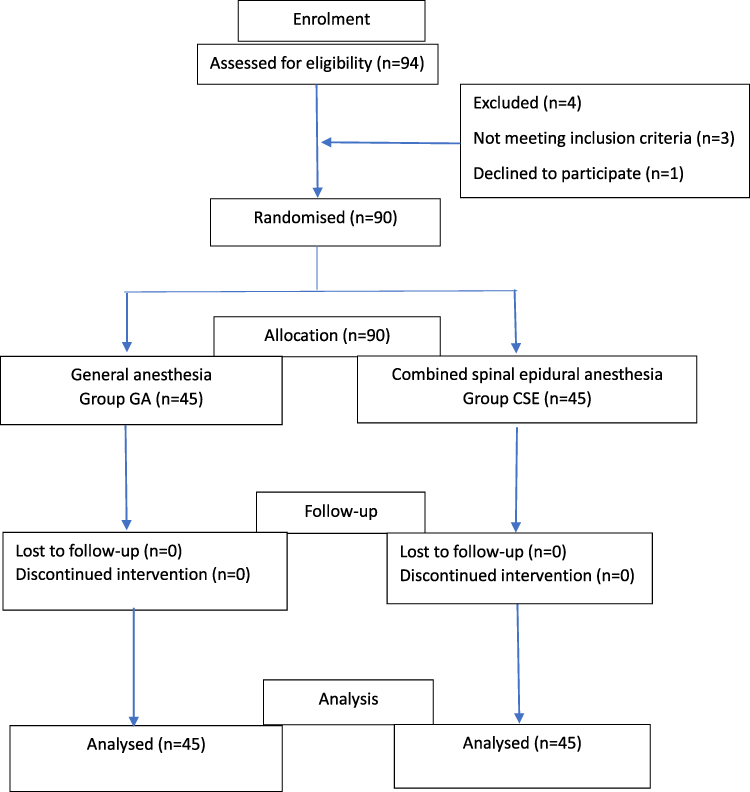 |
Figure 1 CONsolidated Standards Of Reporting Trials (CONSORT) flow chart. Notes: CONSORT figure adapted from Schulz KF, Altman DG, Moher D, CONSORT 2010 Statement: Updated Guidelines for Reporting Parallel Group Randomised Trials. PLoS Med. 2010;7(3): e1000251. Copyright: © 2010 Schulz et al.7 Creative Commons Attribution License. |
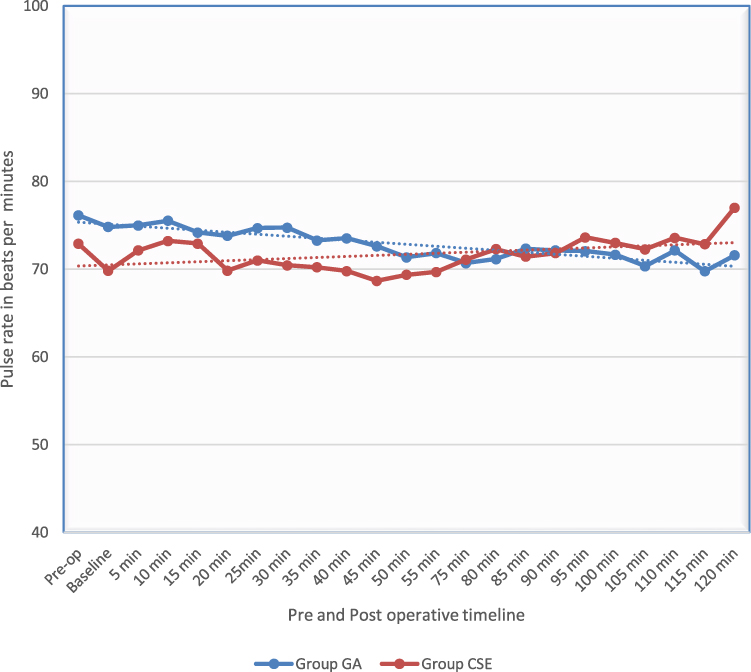 |
Figure 2 Line diagram showing mean pulse rate distribution over various times among study participants. |
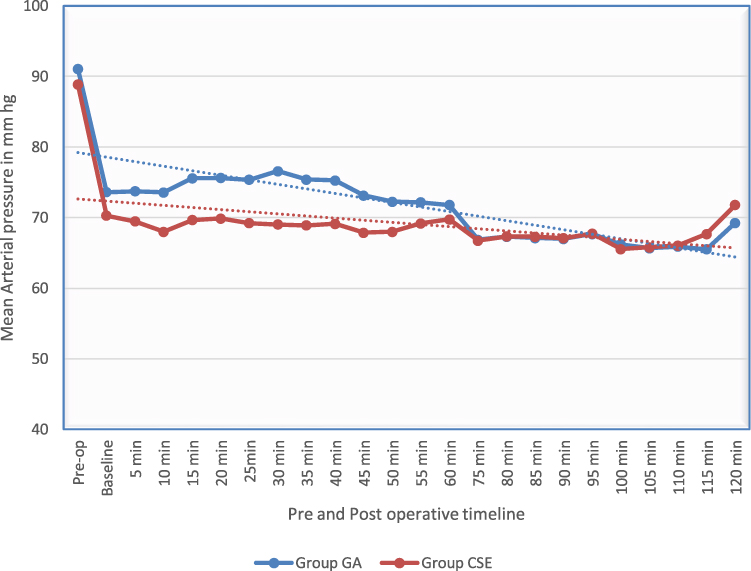 |
Figure 3 Line diagram showing a comparison of mean arterial pressure between two groups. |
The total post-operative analgesic (Inj. tramadol) requirement of patients in group GA was 115±32.59 mg, whereas in group CSE it was 80.35 ± 37.25 mg. Patients in the CSE group required less post-op analgesia than the GA group and the difference between groups was statistically significant (p =< 0.001). In the present study, the total number of patients requiring blood transfusion in group GA was 11 (24.5%) whereas in group CSE, only three patients needed transfusion (6.7%). The difference in number of patients requiring blood transfusion between both groups was found to be statistically significant (p = 0.039).
Discussion
PCNL is a minimally invasive procedure done to remove large renal stones and upper ureteric calculus under general anesthesia in the prone position under fluoroscopy guidance.8 A neuraxial block is not routinely administered to patients undergoing PCNL in a prone position due to possible hemodynamic disturbances after positioning, inability to prolong anesthesia and loss of airway control. However neuraxial anesthesia can be administered to patients who undergo PCNL in the supine position due to the absence of position related complications and ability to secure the airway, if needed. There was no RCT to compare general anesthesia with neuraxial anesthesia in patients undergoing PCNL in the supine position. Hence we conceptualized this study to compare hemodynamic parameters in patients undergoing percutaneous nephrolithotomy (PCNL) in the supine position under combined spinal-epidural with general anesthesia (GA).
We found no statistically significant difference with respect to sex, ASA physical status, surgery time and calculus size in patients between the two groups.There was no statistically significant difference in heart rate while mean arterial pressure was significantly lower in patients who underwent surgery under the combined spinal-epidural anesthesia (CSE) from 5–50 minutes of surgery compared to those who were administered general anesthesia. The fall in blood pressure in the CSE group could be due to a neuraxial blockade induced venous pooling in the lower limbs. These conclusions were partly similar to the findings of research done by Moawad et al9 where a significant reduction in heart rate and mean arterial pressure were noted till 90 minutes after starting PCNL in the prone position. Since PCNL in the supine position does not require a change in position, we experienced better hemodynamic stability in both groups. In contrast, a study conducted by Karacalar et al10 showed increased incidence of bradycardia in both the GA and CSE groups.
Eleven patients who underwent surgery under GA (24.5%) required blood transfusions in the post-operative period whereas only three patients (6.7%) in the CSE group. In view of reduced blood pressure and heart rate under CSE, patients lose less blood during surgery, thereby obviating the need for blood transfusion. These findings were similar to research done by Movasseghi et al,11 where one patient (3.3%) in their GA group had a blood transfusion but none of the patients in the SA group had any transfusion. Similarly, Gonen et al had observed that none of the patients who underwent PCNL under spinal anesthesia required a blood transfusion. In the current study, postoperative analgesic requirements were lesser in patients in the CSE group compared to that of the GA group (P < 0.0001) in the first 24 hrs. The results observed in this study was similar to the study done by Tangpaitoon et al who concluded that the mean analgesic requirement within 24 hours was lower in the CSE group when compared with the GA group (P < 0.0001).12 Similarly, Singh et al inferred that the mean requirement of analgesic in the first 2 hours of the postoperative period was higher in the GA group than in the CSE group (P <0.0001).13 Patients who undergo surgery under CSE do not experience puncture site pain till the regression of sensory level in the neuraxial block. Hence total analgesic consumption is significantly lower in the CSE group.
Limitations
One of the limitations of this study was the inability to blind participants and observers. Another limitation was that a successful CSE anesthesia requires a high level of expertise and experience.
Conclusion
Patients who underwent percutaneous nephrolithotomy under combined spinal epidural analgesia had less mean arterial pressure, comparable heart rate, required less blood transfusion and postoperative analgesic compared to a group under general anesthesia.
Data Sharing Statement
The data used to support findings of the study can be obtained from the corresponding author upon written request.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Li H, Xu K, Li B, et al. Percutaneous nephrolithotomy under local infiltration anesthesia: a single-center experience of 2000 Chinese cases. Urology. 2013;82(5):1020–1025. doi:10.1016/j.urology.2013.07.007
2. Malik I, Wadhwa R. Percutaneous nephrolithotomy: current clinical opinions and anesthesiologists perspective. Anesthesiol Res Pract. 2016;2016:9036872. doi:10.1155/2016/9036872
3. Shaikh SI, Nagarekha D, Hegade G, et al. Postoperative nausea and vomiting: a simple yet complex problem. Anesth Essays Res. 2016;10(3):388–396. doi:10.4103/0259-1162.179310
4. Ozdedeli K, Cek M. Residual fragments after percutaneous nephrolithotomy. Balkan Med J. 2012;29(3):230–235. doi:10.5152/balkanmedj.2012.082
5. Kamal M, Sharma P, Singariya G, et al. Feasibility and complications of spinal anaesthesia in percutaneous nephrolithotomy: our experience. J Clin Diagn Res. 2017;11(6):UC08–UC11. doi:10.7860/JCDR/2017/26425.10111
6. Ranjan R, Malviya D, Misra S, et al. To compare the changes in hemodynamic parameters and blood loss during percutaneous nephrolithotomy - general anesthesia versus subarachnoid block. Anesth Essays Res. 2020;14(1):72–74. doi:10.4103/aer.AER_14_20
7. Schulz KF, Altman DG, Moher D. CONSORT Statement: Updated Guidelines for Reporting Parallel Group Randomised Trials. PLoS Med. 2010;7(3):e1000251.
8. Carrion DM, Cansino JR, Quintana LM, et al. Prone percutaneous nephrolithotomy: its advantages and our technique for puncture. TranslAndrol Urol. 2018;7(6):950–959. doi:10.21037/tau.2018.10.04
9. Moawad HE, El Hefnawy AS. Spinal vs. general anesthesia for percutaneous nephrolithotomy: a prospective randomized trial. Egypt J Anaesthesia. 2015;31:71–75. doi:10.1016/j.egja.2014.08.004
10. Karacalar S, Bilen CY, Sarihasan B, et al. Spinal-epidural anesthesia versus general anesthesia in the management of percutaneous nephrolithotripsy. J Endourol. 2009;23(10):1591–1597. doi:10.1089/end.2009.0224
11. Movasseghi G, Hassani V, Mohaghegh MR, et al. Comparison between spinal and general anesthesia in percutaneous nephrolithotomy. Anesth Pain Med. 2013;4(1):e13871. doi:10.5812/aapm.13871
12. Tangpaitoon T, Nisoog C, Lojanapiwat B. Efficacy and safety of percutaneous nephrolithotomy (PCNL): a prospective and randomized study comparing regional epidural anesthesia with general anesthesia. Int Braz J Urol. 2012;38(4):504–511. doi:10.1590/s1677-55382012000400010
13. Singh V, Sinha RJ, Sankhwar SN, et al. A prospective randomized study comparing percutaneous nephrolithotomy under combined spinal-epidural anesthesia with percutaneous nephrolithotomy under general anesthesia. Urol Int. 2011;87(3):293–298. doi:10.1159/000329796
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Innovations in Kidney Stone Removal
Tzelves L, Geraghty RM, Hughes T, Juliebø-Jones P, Somani BK
Research and Reports in Urology 2023, 15:131-139
Published Date: 11 April 2023
Cystine Stones: Developments in Minimally Invasive Surgery and Their Impact on Morbidity and Stone Clearance
Hughes T, Tzelves L, Somani BK
Research and Reports in Urology 2023, 15:175-185
Published Date: 5 June 2023