Back to Journals » Patient Preference and Adherence » Volume 18
A Qualitative Study on Perspectives of Parkinson’s Disease Medications: Insights from Patient Focus Groups
Authors Richards K ![]() , Mantri S, Brown CM, Johnsrud M, Arcona S
, Mantri S, Brown CM, Johnsrud M, Arcona S ![]() , Sasané R
, Sasané R
Received 16 April 2024
Accepted for publication 10 September 2024
Published 18 September 2024 Volume 2024:18 Pages 1919—1928
DOI https://doi.org/10.2147/PPA.S473991
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Michael Ortiz
Kristin Richards,1 Sneha Mantri,2 Carolyn M Brown,1 Michael Johnsrud,1 Steve Arcona,3 Rahul Sasané3
1TxCORE, College of Pharmacy, The University of Texas at Austin, Austin, Texas, USA; 2Department of Neurology, Duke University, Durham, North Carolina, USA; 3Cerevel Therapeutics, LLC, Cambridge, Massachusetts, USA
Correspondence: Kristin Richards, Email [email protected]
Purpose: Medication is an important component of the management of Parkinson’s disease (PD), yet few studies investigate factors that inform medication decision-making from the perspective of those who use these therapies. This qualitative study aimed to better understand the medication experiences and perspectives of people with PD (PwPD).
Patients and Methods: Thirty-two PwPD recruited from five large movement disorder clinics from five US states participated in 1-hour on-line focus groups in 2022. Thematic analysis was used to analyze the data.
Results: Four primary themes (subthemes in parentheses) emerged concerning PD medications: (1) medication effectiveness (uncertainty, inconsistent effects, adjusting expectations); (2) medication burden (morning doses, timing challenges, constant reminder); (3) side effects (toleration, treatment, confusion with disease symptoms); and (4) preferences/requests (important attributes, therapy advancement).
Conclusion: This study identified four core dimensions associated with PD medications from the perspective of PwPD. Results indicate the need for enhanced communication between providers and patients regarding PD medication to reduce the uncertainties and burden associated with PD medication regimens and promote better health outcomes for PwPD.
Keywords: Parkinson’s disease, medication, patient perspective, patient experience
Introduction
Most people with Parkinson’s disease (PwPD) will eventually take multiple medications for the management of their motor and non-motor symptoms.1 Medication switching, dose adjustment, and frequent dosing are common challenges for PwPD as they work with their providers to balance symptom control and medication side effects.1,2 Resulting drug regimens can be complicated and difficult to manage. Medication adherence is crucial for symptom management; however, claims-based studies show that adherence is significantly suboptimal with only 33% to 54% of PwPD meeting an 80% adherence threshold.3–8 A recent systematic review of qualitative research regarding the treatment burden associated with PD found medications to be the most frequently raised issue by PwPD and their care partners.9
Medication use patterns and health outcomes in chronic disease are linked to patients’ beliefs and understandings about their medications.10,11 It is important to collect patient experience data related to medications to gain more comprehensive insight into chronic diseases as experienced in the real world. Patient experience literature in PD is growing with several studies focusing on areas related to PD medications. OFF periods—when medications wear off and PD symptoms return—are of significant concern to patients12 and have been a recent focus of patient experience research. Mantri et al reported patients’ descriptions of their OFF times, what triggers them, and how to cope with them.13 Armstrong et al have interviewed patients and care partners regarding the experience of and communication about OFF times and their impact on daily life.14–16 These studies demonstrate the need for more patient education regarding OFF periods and for improved communication between patients and providers in order to enhance PD medication management and patient quality of life. In fact, healthcare professionals supporting individuals with life-limiting illness have expressed a desire for better communication aids to help patients and family caregivers understand complex medication regimens.17
In addition to OFF times, researchers have engaged PwPD concerning other PD medication-related factors including medication initiation, adherence, and side effects.2,12,18–21 Shin et al detailed reasons for initiating or delaying PD medication at diagnosis18 and challenges with medication adherence,2 which included forgetfulness, high medication costs, and variable effectiveness. PwPD in Taiwan reported that PD medications helped to improve quality of life, but also had side effects that impacted their daily lives and required a readjustment of schedules and routine practices (eg, meal times, leaving the house).19 PwPD have been interviewed regarding specific dopaminergic medication side effects where they have described changes in their gambling urges and behaviors20 and episodes of sudden uncontrollable somnolence at inappropriate times such as while driving or speaking with friends.21 In a survey of PwPD from the US and from Japan regarding PD medications, US patients reported concerns about experiencing OFF times (55%) and dyskinesia (23%), while hallucinations (44%) were of primary concern to Japanese patients.12
To build on this burgeoning literature base, more comprehensive research on patients’ experiences with and perspectives concerning PD medications is needed.19 Specifically, while prior qualitative and mixed methods research provides growing evidence of treatment gaps and unmet needs, few studies have employed a focus group methodology which captures similar dynamics that PwPD often experience in support groups or other group-based discussions. Thus, we aimed to conduct focus groups in order to explore a broad set of issues related to PD medications with patients in the US who consume those therapies.
Methods
The University of Texas Institutional Review Board (IRB) served as the IRB of record and approved the study, along with the IRBs of the five participating movement disorder clinics. Participants received information about study procedures, were informed regarding the potential publication of their responses, provided written informed consent before participating, and were provided compensation. The study complies with the Declaration of Helsinki and follows the Consolidated Criteria for Reporting Qualitative (COREQ) research framework.22
Study Design and Participants
Focus groups (FGs) were conducted in March and April of 2022 in order to examine key medication issues from the perspective of PwPD. Initially, semi-structured interviews (SSIs) with 20 participants were conducted to identify and explore concepts important to PwPD regarding their medications. FGs were then conducted to bring PwPD together to further explore and discuss medication issues in a group setting.
Five large movement disorder clinics located in Arizona (Barrow Neurological Institute—Phoenix, AZ), Colorado (University of Colorado—Aurora, CO), Florida (University of Florida—Gainesville, FL), North Carolina (Duke University—Durham, NC), and Oregon (Oregon Health & Science University—Portland, OR) served as recruitment centers for both SSIs and FGs. These clinics have been designated as Centers of Excellence by the Parkinson’s Foundation. Fellowship-trained movement disorder neurologists and their staff identified, obtained informed consent, and recruited patients who met the following criteria: (1) diagnosis of PD; (2) recorded modified Hoehn & Yahr (H&Y) score23 within the last 6 months; (3) 18 years of age or older; (4) prescribed antiparkinsonian medication; (5) fluent in English; (6) cognitively able to participate; and (7) had not participated in the SSIs associated with this study. Recruiters were asked to include patients at different stages of PD severity based on modified H&Y scores between 1 (unilateral involvement only) and 5 (wheelchair bound/bed confinement).
Focus Groups
All FGs were facilitated by a trained interviewer and FG moderator hired by the principal investigator (K.R). The moderator has expertise in market research and considerable experience in healthcare-related qualitative research. She has previously worked with two study investigators (C.B., K.R) on multiple qualitative research projects. The study team members are all researchers with qualitative and mixed methods experience and one is also a neurologist and movement disorder specialist (S.M).
Five recorded 1-hour online FGs were conducted via Zoom. Each FG consisted of a mix of patients with similar disease severity levels across the different recruiting clinics. The moderator began each FG by telling participants:
We want to explore aspects about the medications for Parkinson’s disease that you are taking now and that you have taken in the past. We’ll talk about how the medications work for you and any side effects you’ve experienced. I’ll ask you about your expectations regarding medication and how they might have changed throughout your journey with this disease.
FG sessions were professionally transcribed from recordings.
Analysis
Thematic analysis (TA) with an inductive approach was used to analyze FG transcripts. TA, with guidelines detailed by Braun and Clarke,24 is a widely used method for analyzing qualitative data in healthcare research.25 It is an appropriate and accessible method for reporting “experiences, meanings, and the reality of participants”.24 The analysis occurs in six phases (briefly listed): (1) data familiarization; (2) initial code generation; (3) theme identification; (4) theme review; (5) theme definitions and names; and (6) report production. Malkon et al have published a helpful and detailed description of qualitative TA in the supplementary material accompanying their study on patients’ views of antihypertensive medication.26
FG transcripts were qualitatively analyzed by the first author using NVivo 12 qualitative data analysis software. Line-by-line open coding and constant comparison techniques were utilized. A report of identified codes and supportive quotes was drafted and circulated to all study investigators who subsequently reviewed and discussed emerging themes and subthemes until consensus was reached. Stata v.17.0 was used to generate participant characteristic descriptive statistics.
Results
Thirty-two participants (16 females and 16 males) attended the FG online meetings (5–9 per FG). More than 60% (62.5%) had a recent modified H&Y score of 2.5 or less, indicating less severe PD. All 32 participants were currently taking levodopa and eight were also taking a dopamine agonist. Most (56.3%) were taking multiple PD medications. Characteristics of the FG members are presented in Table 1.
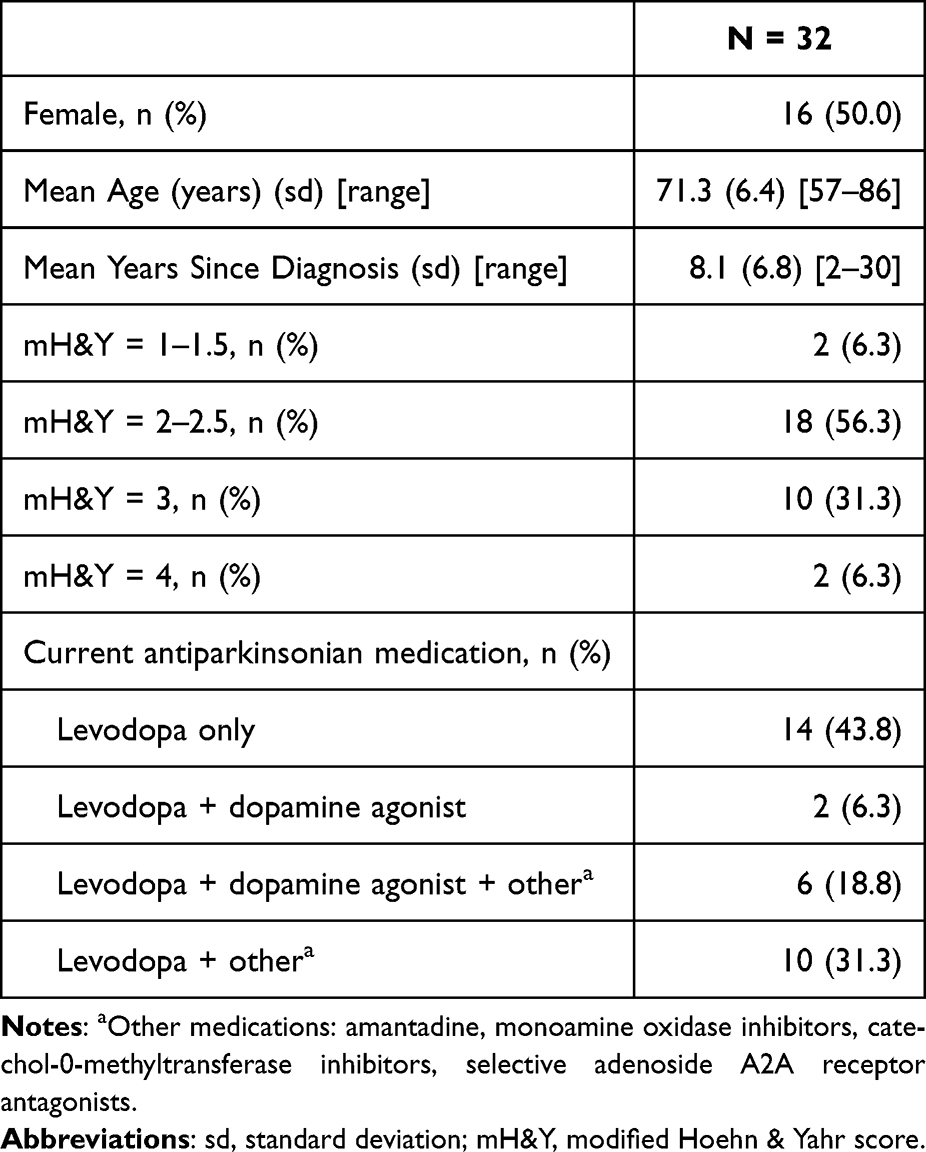 |
Table 1 Focus Group Participant Characteristics |
Four primary themes and 11 subthemes (Figure 1) emerged from the thematic analysis and are described below with supporting quotes.
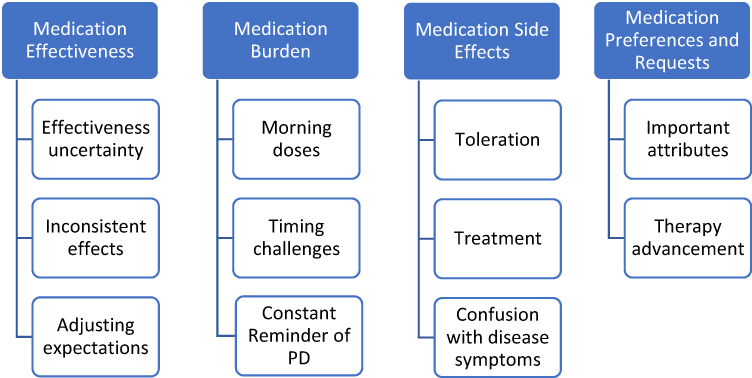 |
Figure 1 Themes and Subthemes Related to Patients’ Experiences with and Perspectives on Parkinson’s Disease Medications. |
Theme 1 – Medication Effectiveness: Uncertainty, Inconsistent Effects, and Adjusting Expectations
Some participants indicated that their PD medications worked well. However, even among participants who reported good medication effectiveness, many expressed uncertainties. They were unsure if their medications were as effective as they could be. They were unclear on the effects they should expect and wondered if they needed to switch to another medication. Respondents mentioned that they should ask their prescribers for help to clarify these matters.
I wonder if I should be feeling more symptom relief than I am currently feeling. I’m not discounting that I’m feeling any symptom relief … but I do wonder if I should be feeling more.
I was underwhelmed with the results I got from medications. I was wondering if the medicine could do me more good.
Participants also discussed inconsistencies in their medications’ effects. They believed the medications worked well on some days, but the effects could fluctuate, even on a day-to-day basis. Some also expressed their nervousness regarding medication changes due to the unknown effects.
I take the medication the same way, but I feel different every day. Sometimes I feel like my medicine is not working much at all. Sometimes I feel like it’s not working long enough.
Why can there be some days that it works so well, and other days, it doesn’t even feel like I took anything?
I hate changing my medications because I don’t know if I’m going to do well. I don’t know what will happen.
Participants emphasized that it is important as a patient to understand from the outset that PD medications do not cure the disease, nor subside all disease symptoms. Many discussed initially being under the impression that the medication would completely relieve the symptoms of PD, but later realized the need to realign their expectations.
The drugs don’t totally do what I thought they were going to do. I thought they were going to stop the tremor and stop the stiffness, and this slow moving … and they don’t do that, not with Parkinson’s.
My expectations of medication were very high. I believed you took medication to get rid of pain, and you got rid of it. Or you take medication to get well, and you get well. This is medication that doesn’t do either. It’s not going to get you well, and so your commitment to medication has to be for some other reason than getting well.
Theme 2 – Medication Burden: Morning Doses, Timing Challenges, and Constant Reminder
Medication burden was a topic of critical significance, logistically as well as psychologically. Participants commonly reflected upon their first dose of PD medication in the morning and discussed their morning medication routines to get out of bed more easily. A few relayed their practice of taking medication in the early morning hours (eg, 3am, 5am) so they could wake up ON with symptom control.
I take a pill in the morning and then I’m just waiting for it to kick in before I get up from bed and do anything. That’s just how I start my day.
I take a pill about 3:00 AM, or something like that, three or four in the morning, then I’m ready to go later when I get out of bed.
I don’t have many issues for getting up in the morning. I take the pill at 5:00 AM and then I go back to sleep for a little while.
Participants also expressed frustration with the number of medications they take and having to take medication several times each day. They discussed the challenges of scheduling meals around taking their medications. Those who took medication fewer times per day expressed concerns about their future medication needs and the timing challenges they could expect.
I constantly take medication, because my dose is spread out. I take my meds at 6:00, 9:00, 12:00, 3:00, 6:00, and bedtime.
You would not believe how fast two hours goes. I take my pill, and then two hours later, the alarm goes off again. I’m like, “What? Two hours has gone by? It felt like it was 10 minutes”.
The other thing too is that you’re supposed to take it at least a half hour to an hour away from any meals, and I’m supposed to take it three times a day. Trying to do that and juggle the pill taking with my meals and my schedule with the rest of my life, it’s just a pain.
Many shared that PD medication has become a prominent focus of their lives that limits their freedom, even with everyday activities (eg, meals, leaving the house). The number of medications they take and the increasing dosing frequency serve as incessant reminders of their disease.
It gives no flexibility. Because, as I said, it dictates when we eat, and we’re going to go out, then I need to take my pill before we go out to meet some people for dinner or whatever.
I have to take some medication six times a day and I’m reminded of my Parkinson’s six times a day. I would just like for it to not be such an important part of my life.
I feel like I’m being tied to that pillbox.
It’s being chained to a lot of medicine. We have to make sure if we’re out and about, we have the medicine with us. I take it every three hours. We’ve turned into clock-watchers.
Theme 3 – Side Effects: Toleration, Treatment, and Confusion with Disease Symptoms
Some participants reported no bothersome side effects from PD medications, but most mentioned that they have experienced or are currently struggling with medication side effects. They indicated that all PD medications have side effects and people have different reactions to therapies. One participant said, “We are all, what I call in terms of differences, we are all snowflakes”. They discussed making decisions on whether to keep taking a PD medication and tolerate the accompanying side effects or switch to another medication.
I wish we could figure out how to get around the side effects. I have to take mine with food to combat the nausea. But I’m thinking I’m not getting the best effect because of the food. It’s better if you take it on an empty stomach, but then you feel queasy all the time and then you kind of get used to feeling bad.
That medication made me feel like I was just in a fog. I tried it for a while, but I went off of it because I didn’t see the benefits outweighed the side effects.
I had a lot of nightmares with it, but it was so disconcerting that I had them so consistently. I decided I just couldn’t tolerate it, and after I came off of that medication, the nightmares slowly stopped and went away. That was a relief.
Participants discussed being prescribed additional medications to treat PD medication side effects. This added to medication burden and created frustration.
I was on [carbidopa/levodopa], which worked pretty good for a while. Then, the doctor started prescribing all kinds of— I had patches, and I had this stuff and that stuff – stuff for the side effects, too. He just kept piling them on top of each other to where it got to where I was taking nine different medications or something like that.
Finally, participants explained the difficulty of determining if a symptom they experienced was a medication side effect or a sign of PD progression. This was another topic that several indicated they would like to further discuss with their healthcare providers.
It’s hard to tell because all these drugs’ side effects, all of them have the same symptoms, potential, as what Parkinson’s presents with. It’s hard to differentiate. Is it a side effect or is it your disease? It’s really hard to tell the chicken from the egg for me.
How do all these medications work together? I’m on a lot of medication. You don’t know whether something is causing the symptoms or whether it’s just part of the disease process.
Theme 4 – Medication Preferences and Requests: Important Attributes and Therapy Advancement
Participants welcomed the opportunity to discuss medication attributes that were of most importance to them. They certainly desired curative therapies, but understood the limitations of currently-available medications. Slowing disease progression and lessening medication burden were top-of-mind issues. Many indicated that they would like a longer medication effect and something that did not interact with meals.
I don’t want this to get worse, and the medications don’t help with that. I know that there won’t be a cure for it in my lifetime realistically, but I would like to have something that will halt it or slow the progression.
I’d like to have medication that would last longer. You wouldn’t have to take it four times a day. It would be nice if you could take it once or maybe twice.
There needs to be something that is more efficient and continuous than taking a pill that is as effective as the vagaries of the diet that you have that day.
Participants also called on researchers to push boundaries and advance the frontiers of PD therapies. They recognize therapeutic progress and breakthroughs associated with other disease states and desire the same for PD.
We’ve got gene therapies and DNA things that we are using in other areas. I don’t think it’s a stretch to go that direction.
I’m in the “go big or go home” camp. Stem cell and other research has all kinds of possibilities out there.
As many people in the world who have this disease, I can’t believe how little the drugs have changed to treat the course of the disease. There are tons of studies out there going on about all sorts of different things in mice and skin fibroblasts and stem cells and all this stuff.
Discussion
As with most disease states, pharmacological therapy is a fundamental aspect of the management of PD motor and non-motor symptoms. Given the need for more therapies and the escalating dosage frequency with disease progression, this is especially true in PD. This study explored issues related to PD medications from the perspective of PwPD across disease stages who are currently taking these medications. Effectiveness, medication burden, side effects, and preferences/requests were the four core themes identified in our qualitative study, not uncommon among medication experience research.12,19,26,27 The subthemes that emerged, discussed below, are all issues that should be better understood from the patient perspective in order to improve health outcomes.
While participants reported feeling PD symptom relief, they felt unsure about the nature and extent of medication effectiveness they should expect and if their expectations warranted adjustments. They had questions about the inconsistencies in symptom control they experienced and expressed the need to speak with their providers for clarification. No participants mentioned that they had discussed these concerns with a provider, however. Open communication between PwPD and their providers should be encouraged and fostered, with a focus on level-setting expectations regarding medications.
Consistent with findings from other studies,28–30 participants believed they needed more information regarding the role of medications in managing PD as well as their variable effectiveness, particularly at the time of diagnosis. “Satisfaction with the explanation of the condition at diagnosis” has been found to significantly impact quality of life in PwPD, even years after being diagnosed with the condition.31 Providers should actively engage with patients regarding what they can reasonably expect from their PD medications and urge them to promptly and regularly communicate their experiences, questions, and concerns. A patient-centered approach to healthcare empowers patients and their care partners to be dynamic participants in their care, and has positive effects on quality of life, satisfaction, and medication adherence.28,32
Medication burden was a universal concern among study participants despite their current stage of PD severity. The number of medications required to manage PD symptoms and the frequency with which they must be taken are challenges for all patients, not only those who are still working or have very active lifestyles. The medication burden associated with PD becomes oppressive to patients, exemplified in the participants’ expressions on this matter: “tied to that pill box”, “chained to a lot of medicine”, “we have turned into clock-watchers”. It is well-documented that the increasing complexity of a medication regimen negatively affects therapy adherence and persistence in chronic disease,33–36 and this complexity is likely reflected in the poor adherence rates in PD as well.3–8 Prescribers are encouraged to understand that reducing medication burden is important to all people living with PD and to tailor medication regimens to individual needs.17 Pharmacists can assist PwPD and their care partners by providing clear instructions and medication packaging and organization suggestions to make medication consumption less taxing.17,33
Sleep disturbances (eg, insomnia, restless leg syndrome, rapid eye movement sleep disorder syndrome, excessive daytime sleepiness) are common in PD and can seriously compromise sleep quality, daytime functioning, clinical outcomes, and quality of life.37,38 In our study, some participants reported that they intentionally interrupt their nighttime sleep to take medication in order to wake up ON. Providers should inquire about their patients’ morning medication routines and, alongside patients, seek solutions for waking challenges that do not require sleep interruptions.
Medication side effects was a prominent theme, with most participants reporting having experienced various adverse effects associated with PD medications. These findings are consistent with other patient experience studies in PD.12,19 Patients are sometimes prescribed additional medication to manage a side effect, contributing to the burden of already complex medication regimens. As previously mentioned, effective patient-provider communication and solution-driven medication strategies would benefit PwPD who regularly encounter side effects and are also often uncertain whether an experienced symptom is a medication side effect or sign of disease progression.
Coping with medication side effects and accepting the reality that complete avoidance of side effects is nearly impossible with PD therapies were evident among participants. Some could manage or get used to the experienced adverse effect, while others discontinued and/or switched to a different PD therapy because of a side effect. Discussions indicated that PwPD have to make trade-off decisions regarding medication: they want PD symptom relief, but are they able and willing to tolerate bothersome side effects? PwPD and care partners face a daunting and complex decision process regarding therapies and their positive and negative effects. This is an area in PD ripe for exploration in future studies. Shared decision making among providers, patients, and care partners—a process that considers medical evidence, clinician expertise, and patient values and preferences—is encouraged to help support more informed and effective decision-making.28,39,40
Concerning the theme of medication preferences and requests, participants prioritized medications with a lower burden profile regarding dosing frequency and drug-food interactions. They valued a medication with a fast onset of action that could also provide a longer-lasting effect to limit OFF times. A discrete choice experiment conducted in 2019 found the former attribute (quick onset) was, in fact, more important to PwPD than the latter (longer effect).41 Participants wanted to take medications less often and hoped for the development of curative therapies, or for those which could halt or slow disease progression. They expressed frustration with limitations of currently-available treatment options and the perceived lack of therapeutic advancement over the years. They wanted research into PD treatments to be conducted with a greater sense of urgency.
Limitations
Study findings should be interpreted in light of several limitations, including the small sample size (n=32). Research including more participants with varied characteristics and experiences is needed to further explore the heterogeneity of PwPD’s perspectives on their medications. Study enrollment was limited to patients with access to Parkinson’s Foundation Centers of Excellence, which impacts the generalizability of the results. Thus, issues related to PD medications identified in this study may not represent the universe of relevant medication-related issues in all PwPD. A recent study reported that approximately 50% of Medicare beneficiaries with PD had a visit with a general neurologist in 2019, while fewer than 10% saw a movement disorder specialist.42 The remainder had a visit with their primary care provider (29%) or had no physician visits (11%) during the year. Future research should aim to include those who are less likely to access neurologists and movement disorder specialists for treatment. Additionally, not all stages of PD were represented as only two participants were rated at modified H&Y stage 1–1.5, two at stage 4, and none at stage 5. However, with most participants rated at modified H&Y stages 2–3, the results emphasize the complexity of medication adherence even in the earlier stages of the disease; presumably those with more advanced PD would be even more impacted by their medication frequency and side effects, particularly given the effects of cognitive impairment on treatment adherence.43,44 Due to the nature of this study, participants had to be cognitively able to use a computer and articulate their thoughts in English; perspectives may differ for more cognitively impaired PwPD, those without computer or internet access, and those with limited English fluency.45,46 We did attempt to improve the generalizability of the findings by recruiting participants at different stages of PD and recruiting from five geographically diverse movement disorder clinics (though not all geographic areas of the US were represented), but additional study is needed to understand the broader range of patient perspectives. Furthermore, we did not collect culturally-related information such as race/ethnicity, rural/urban residence, education, and attitude; such information could enhance the understanding of differences in patient experiences and assist with culturally sensitive management approaches. Finally, the research team’s experience in qualitative research and in PD influences our interpretations of the FG data to some degree, but we sought to minimize bias in data collection by the use of a trained independent FG moderator.
Conclusion
This study exploring the perspectives and experiences of people living with PD regarding their medications found that many PwPD have questions and want more information about PD medication effectiveness and side effects. They are frustrated by burdensome PD medication regimens and strongly desire innovation in PD therapies. Understanding patients’ views is a critical component in the delivery of patient-centric care and development of treatment plans that meet patients’ individual needs. Patient-provider communication and shared decision making processes should be encouraged in order to promote improved health outcomes among those who are diagnosed with PD both now and in the future. Additional research in diverse populations of PwPD is needed to better and more fully understand their experiences with and perspectives on PD medications.
Acknowledgments
We would like to acknowledge the staff at the participating movement disorder clinics who facilitated recruitment and were integral to the launch of this study. We especially thank all of the participants who generously gave of their time and provided such valuable insight into their Parkinson’s disease journeys. Interim findings were presented in a poster at 2023 American Academy of Neurology annual meeting in Boston, MA. The poster’s abstract was published in the April 25, 2023 issue of Neurology (https://doi.org/10.1212/WNL.0000000000202791).
Disclosure
Kristin Richards, Carolyn Brown, and Michael Johnsrud are employees of The University of Texas at Austin and conducted the research through a grant from Cerevel Therapeutics. Sneha Mantri is an employee of Duke University and conducted the research through a grant from Cerevel Therapeutics; non-financial support from Michael J Fox Foundation, Parkinson’s Foundation; personal fees from Modality.ai, outside the submitted work. Steve Arcona and Rahul Sasané are employees of Cerevel Therapeutics. The authors report no other conflicts of interest in this work.
References
1. Armstrong MJ, Okun MS. Diagnosis and treatment of Parkinson disease: a review. JAMA. 2020;323(6):548–560. doi:10.1001/jama.2019.22360
2. Shin JY, Habermann B, Pretzer-Aboff I. Challenges and strategies of medication adherence in Parkinson’s disease: a qualitative study. Geriatr Nurs. 2015;36(3):192–196. doi:10.1016/j.gerinurse.2015.01.003
3. Johnsrud M, Richards K, Arcona S, Sasané R, Leoni M. An assessment of Parkinson’s disease medication treatment patterns in the Medicaid population. Clin Park Relat Disord. 2021;5:100109. doi:10.1016/j.prdoa.2021.100109
4. Richy FF, Pietri G, Moran KA, Senior E, Makaroff LE. Compliance with pharmacotherapy and direct healthcare costs in patients with Parkinson’s disease: a retrospective claims database analysis. Appl Health Econ Health Policy. 2013;11(4):395–406. doi:10.1007/s40258-013-0033-1
5. Delea TE, Thomas SK, Hagiwara M. The association between adherence to levodopa/carbidopa/entacapone therapy and healthcare utilization and costs among patients with Parkinson’s disease: a retrospective claims-based analysis. CNS Drugs. 2011;25(1):53–66. doi:10.2165/11538970-000000000-00000
6. Davis KL, Edin HM, Allen JK. Prevalence and cost of medication nonadherence in Parkinson’s disease: evidence from administrative claims data. Mov Disord. 2010;25(4):474–480. doi:10.1002/mds.22999
7. Tarrants ML, Denarié MF, Castelli-Haley J, Millard J, Zhang D. Drug therapies for Parkinson’s disease: a database analysis of patent compliance and persistence. Am J Geriatr Pharmacother. 2010;8(4):374–383. doi:10.1016/j.amjopharm.2010.08.001
8. Kulkarni AS, Balkrishnan R, Anderson RT, Edin HM, Kirsch J, Stacy MA. Medication adherence and associated outcomes in medicare health maintenance organization-enrolled older adults with Parkinson’s disease. Mov Disord. 2008;23(3):359–365. doi:10.1002/mds.21831
9. Tan QY, Cox NJ, Lim SER, et al. The experiences of treatment burden in people with Parkinson’s disease and their caregivers: a systematic review of qualitative studies. J Parkinson's Dis. 2021;11(4):1597–1617. doi:10.3233/JPD-212612
10. Cea-Calvo L, Marín-Jimémez I, de Toro J, et al. Different associations of intentional and non-intentional non-adherence behaviors with patient experience with healthcare and patient beliefs in medications: a survey of patients with chronic conditions. Patient Prefer Adher. 2020;14:2439–2450. doi:10.2147/PPA.S281985
11. Kvarnström K, Westerholm A, Airaksinen M, Liira H. Factors contributing to medication adherence in patients with a chronic condition: a scoping review of qualitative research. Pharmaceutics. 2021;13(7):1100. doi:10.3390/pharmaceutics13071100
12. Hattori N, Fujimoto K, Kondo T, Murata M, Stacy M. Patient perspectives on Parkinson’s disease therapy in Japan and the United States: results of two patient surveys. Patient Relat Outcome Meas. 2012;3:31–38. doi:10.2147/PROM.S29443
13. Mantri S, Lepore M, Edison B, et al. The experience of OFF periods in Parkinson’s disease: descriptions, triggers, and alleviating factors. J Patient Cent Res Rev. 2021;8(3):232–238. doi:10.17294/2330-0698.1836
14. Armstrong MJ, Rastgardani T, Gagliardi AR, Marras C. The experience of off periods: qualitative analysis of interviews with persons with Parkinson’s and carepartners. Clin Park Relat Disord. 2019;1:31–36. doi:10.1016/j.prdoa.2019.07.008
15. Armstrong MJ, Rastgardani T, Gagliardi AR, Marras C. Barriers and facilitators of communication about off periods in Parkinson’s disease: qualitative analysis of patient, carepartner, and physician interviews. PLoS One. 2019;14(4):e0215384. doi:10.1371/journal.pone.0215384
16. Armstrong MJ, Rastgardani T, Gagliardi AR, Marras C. Impact of off periods on persons with Parkinson disease and care partners: a qualitative study. Neurol Clin Pract. 2021;11(3):e232–e238. doi:10.1212/CPJ.0000000000000921
17. Wilson E, Caswell G, Latif A, Anderson C, Faull C, Pollock K. An exploration of the experiences of professionals supporting patients approaching the end of life in medicines management at home. A qualitative study. BMC Palliat Care. 2020;19(1):66. doi:10.1186/s12904-020-0537-z
18. Shin JY, Habermann B. Initiation of medications for Parkinson’s disease: a qualitative description. J Clin Nurs. 2016;25(1–2):127–133. doi:10.1111/jocn.13009
19. Chen Y-W, Huang C-Y, Chen J-H, et al. Living with Parkinson’s disease: disease and medication experiences of patients and caregivers. Int J Qual Stud Health Well-Being. 2022;17(1):2018769. doi:10.1080/17482631.2021.2018769
20. Olley J, Blaszczynski A, Lewis S. Dopaminergic medication in Parkinson’s disease and problem gambling. J Gambl Stud. 2015;31(3):1085–1106. doi:10.1007/s10899-014-9503-0
21. Avorn J, Schneeweiss S, Sudarsky LR, et al. Sudden uncontrollable somnolence and medication use in Parkinson disease. Arch Neurol. 2005;62(8):1242–1248. doi:10.1001/archneur.62.8.1242
22. Tong A, Sainsbury P, Craig J. Consolidated criteria for reporting qualitative research (COREQ): a 32-item checklist for interviews and focus groups. Int J Qual Health Care. 2007;19(6):349–357. doi:10.1093/intqhc/mzm042
23. Hoehn MM, Yahr MD. Parkinsonism: onset, progression, and mortality. Neurology. 1967;17(5):427–442. doi:10.1212/WNL.17.5.427
24. Braun V, Clarke V. Using thematic analysis in psychology. Qual Res Psychol. 2006;3(2):77–101. doi:10.1191/1478088706qp063oa
25. Braun V, Clarke V. What can “thematic analysis” offer health and wellbeing researchers? Int J Qual Stud Health Well-Being. 2014;9(1):26152. doi:10.3402/qhw.v9.26152
26. Malkon S, Wettermark B, Kahan T, Bastholm-Rahmner P, Hasselström J, Qvarnström M. A qualitative study on patients’ views on hypertension and antihypertensive medications. Patient Prefer Adher. 2023;17:3331–3339. doi:10.2147/PPA.S429638
27. van der Elst K, Meyfroidt S, De Cock D, et al. Unraveling patient-preferred heath and treatment outcomes in early rheumatoid arthritis: a longitudinal qualitative study. Arthritis Care Res. 2016;68(9):1278–1287. doi:10.1002/acr.22824
28. van der Eijk M, Nijhuis FAP, Faber MJ, Bloem BR. Moving from physician-centered care towards patient-centered care for Parkinson’s disease patients. Parkinsonism Relat Disord. 2013;19(11):923–927. doi:10.1016/j.parkreldis.2013.04.022
29. van der Eijk M, Faber MJ, Al Shamma S, Munneke M, Bloem BR. Moving towards patient-centered healthcare for patients with Parkinson’s disease. Parkinsonism Relat Disord. 2011;17(5):360–364. doi:10.1016/j.parkreldis.2011.02.012
30. van der Eijk M, Faber MJ, Ummels I, Aarts JWM, Munneke M, Bloem BR. Patient-centeredness in PD care: development and validation of a patient experience questionnaire. Parkinsonism Relat Disord. 2012;18(9):1011–1016. doi:10.1016/j.parkreldis.2012.05.017
31. Global Parkinson’s Disease Survey (GPDS) Steering Committee. Factors impacting on quality of life in Parkinson’s disease: results from an international survey. Mov Disord. 2002;17(1):60–67. doi:10.1002/mds.10010
32. Rastgardani T, Armstrong MJ, Marras C, Gagliardi AR. Improving patient-centred care for persons with Parkinson’s: qualitative interviews with care partners about their engagement in discussion of “off” periods. Health Expect. 2019;22(3):555–564. doi:10.1111/hex.12884
33. Lauffenburger JC, Haff N, McDonnell ME, et al. Exploring patient experiences coping with using multiple medications: a qualitative interview study. BMJ Open. 2021;11(11):e046860. doi:10.1136/bmjopen-2020-046860
34. Tesfaye WH, McKercher C, Peterson GM, et al. Medication adherence, burden and health-related quality of life in adults with predialysis chronic kidney disease: a prospective cohort study. Int J Environ Res Public Health. 2020;17(1):371. doi:10.3390/ijerph17010371
35. Ab Rahman N, Lim MT, Thevendran S, Hamdi NA, Sivasampu S. Medication regimen complexity and medication burden among patients with type 2 diabetes mellitus: a retrospective analysis. Front Pharmacol. 2022;13:808190. doi:10.3389/fphar.2022.808190
36. Zheng C, Meng J, Xiao X, Xie Y, Zhao D, Wang H. Polypharmacy, medication-related burden and antiretroviral therapy adherence in people living with HIV aged 50 and above: a cross-section study in Hunan, China. Patient Prefer Adher. 2022;16:41–49. doi:10.2147/PPA.S340621
37. Maggi G, Vitale C, Cerciello F, Santagelo G. Sleep and wakefulness disturbances in Parkinson’s disease: a meta-analysis on prevalence and clinical aspects of REM sleep behavior disorder, excessive daytime sleepiness and insomnia. Sleep Med Rev. 2023;68:101759. doi:10.1016/j.smrv.2023.101759
38. Schütz L, Sixel-Doring F, Hermann W. Management of sleep disturbances in Parkinson’s disease. J Parkinson's Dis. 2022;12(7):2029–2058.
39. Ward J, Kalsi D, Barnett N, Fulford BK, Handa A. Shared decision making in chronic medication use: scenarios depicting exemplary care. Res Social Adm Pharm. 2020;16(1):108–110. doi:10.1016/j.sapharm.2019.04.047
40. Hirsch MA, Simpson AM. Why bother with shared decision-making in Parkinson’s disease? Parkinsonism Relat Disord. 2013;19(11):928–929. doi:10.1016/j.parkreldis.2013.06.021
41. Thach A, Sutphin J, Coulter J, Leach C, Pappert E, Mansfield C. Patient preference for treating “OFF” episodes in Parkinson’s disease; a discrete choice experiment. Patient Prefer Adher. 2021;15:1187–1196. doi:10.2147/PPA.S301644
42. Pearson C, Hartzman A, Munevar D, et al. Care access and utilization among medicare beneficiaries living with Parkinson’s disease. NPJ Parkinson's Dis. 2023;9(1):108. doi:10.1038/s41531-023-00523-y
43. Sumbul-Sekerci B, Hanagasi HA, Bilgic B, Tufekcioglu Z, Gurvit H, Emre M. Medication management and treatment adherence in Parkinson’s disease patients with mild cognitive impairment. Acta Neurol Belg. 2023;123(3):823–829. doi:10.1007/s13760-022-01916-1
44. Castro GS, Aguilar-Alvarado CM, Zúñiga-Ramírez C, et al. Adherence to treatment in Parkinson’s disease: a multicenter exploratory study with patients from six Latin American countries. Parkinsonism Relat Disord. 2021;93:1–7. doi:10.1016/j.parkreldis.2021.10.028
45. Chen Y-R, Tan C-H, Su H-C, et al. Investigating the interaction between neuropsychiatry features and daily activities on social function in patients with Parkinson’s disease with mild cognitive impairment. BJPsych Open. 2022;8(6):e205. doi:10.1192/bjo.2022.611
46. Yu R-L, Wu R-M. Mild cognitive impairment in patients with Parkinson’s disease: an updated mini-review and future outlook. Front Aging Neurosci. 2022;14:943438. doi:10.3389/fnagi.2022.943438
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.