Back to Journals » Medical Devices: Evidence and Research » Volume 18
A Prospective Clinical Study to Evaluate Safety and Performance of an Intra-Surgical Hydraulic Distractor During Spinal Surgeries
Authors Bornemann R ![]() , Himstedt J, Boszczyk B, Bowald S, Sander K, Mikulowski S, Farhoud HMS, Pflugmacher R
, Himstedt J, Boszczyk B, Bowald S, Sander K, Mikulowski S, Farhoud HMS, Pflugmacher R
Received 29 April 2025
Accepted for publication 13 October 2025
Published 24 October 2025 Volume 2025:18 Pages 525—536
DOI https://doi.org/10.2147/MDER.S537601
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Rahel Bornemann,1 Jens Himstedt,2 Bronek Boszczyk,3 Staffan Bowald,4 Kirsten Sander,5 Stan Mikulowski,4 Hesham Mohamed el Saady Farhoud,6 Robert Pflugmacher7
1Clinik Und Polyclinic for Orthopedics and Trauma, University Hospital, Bonn, Germany; 2Orthopedic Spine Surgery, Alfried Krupp Krankenhaus Steele, Essen, Germany; 3Orthopedic Children`s Clinic Aschau, Aschau i, Chiemgau, Germany; 4Ortoway-US Inc, Horsham, PA, USA; 5Aurevia Germany, Kassel, Germany; 6Orthopedic Surgery Department, Faculty of Medicine, Al-Azhar University, Cairo, Egypt; 7Clinic for Spinal Surgery, District Hospital Mechernich, Mechernich, Germany
Correspondence: Rahel Bornemann, Clinic and Polyclinic for Orthopedics and Trauma Surgery University Bonn, Bonn, 53127, Germany, Email [email protected]
Introduction: Spinal surgeries often require the manipulation of bone structures while at the same time protecting sensitive tissues. Existing surgical systems involve manual force, which has a high risk of damaging the vertebrae and instruments interfere with the visibility between the vertebrae, which complicates work. The OrtoWell® Distractor System, an intra-surgical hydraulic tool for vertebrae separation, offers incremental and stable force control and better visibility during distraction procedures in spinal surgeries. This study aims to fill the gap of still pending clinical trials using the device, by evaluating performance and safety of it across lumbar and thoracic surgeries.
Materials and Methods: This study is a prospective, single-arm, multi-center observational study and was conducted between April 2018 and April 2023 at 3 German sites in patients undergoing anterior or lateral spinal surgery requiring vertebral separation. The device’s safety and usability were assessed through surgeon-completed questionnaires on the device and its subcomponents, clinical outcomes and cardiovascular assessments. Assessments were conducted at four time points, at baseline, time of the index procedure, discharge and at a 30-day follow-up.
Results: 31 patients (13 males, mean age 62.33) were included. Single and multi-level treatments were performed using different accesses. The device facilitated spinal surgeries without any complications or device-related adverse events. Usability, stability and force control were evaluated as uniformly positive and all procedures proceeded as planned. Mean applied pressure was 147.69± 29.48 bar. There were no major delays in surgical time and a mean blood loss of 215.17± 113.57 cc. Cardiovascular parameters remained stable, with no significant changes between baseline and follow-up. Hospital stays averaged 16.39± 10.25 days. Surgeons unanimously reported that the distractor simplified surgery.
Discussion and Conclusions: The investigated device demonstrated high safety and performance, enabling precise force control and simplifying spinal surgeries. These findings suggest that hydraulic distractors could enhance surgical outcomes by improving intraoperative control and reducing procedural challenges.
Trial Registration: Registered at ClinicalTrials.gov (NCT03501810, 12 Mar 2018).
Keywords: spinal surgery, distractor, vertebral separation, hydraulic distraction
Introduction
During spinal surgeries, manipulation of bone structures requires a considerable amount of force, which is often applied over extensive durations, while simultaneously vulnerable nervous tissues have to be preserved. A precise control over the applied force and associated biodynamic response is necessary. Through external forces, a multitude of severe complications can arise, including neural damage or dural tear.1 Technical developments of surgical instruments facilitate surgical work and have led to safer procedures and improved quality of life for patients over the last decades.2
One relevant instrument group are distractors. These devices are applied during a multitude of interventions, for example to allow access or increase visibility during surgery,3 or to support insertion of implants into the intervertebral space.4 Also pedicle screw retractors, which are used to increase the distance between two connecting rods by rotating a distraction knob to drive the pedicle screws to distract the vertebral bodies are in use in lumbar interbody fusion.5 Despite their common use, distraction is associated with potential tissue damage caused by abrupt or step-wise distraction. Particularly during the first minutes of disc space distraction, stress on spinal structures is pronounced as viscoelastic relaxation only gradually sets in, and the stress varies as a function of the applied distraction force.6
To make intra-surgical distraction safer, development of instruments is constantly ongoing. However, most of the used distraction devices still rely on manual force control, eg paddle distractors7 or the Caspar distractor.8
Contemporary technical developments provide options for more nuanced control. This includes multifunctional systems that combine a vertebral distraction device with modules for retraction of soft tissues within the same system,9 tasks that are commonly performed by different devices.4,7 It also includes non-manual transmission of force,10,11 which should allow a more constant and nuanced pressure on vertebrae through improved force control, but prospective clinical trials evaluating their performance are still pending. As these devices are currently applied in the field, post-market clinical data for device performance is critical to track the real-world performance.12,13
The current study provides clinical real-world data on patients who underwent various spinal procedures using the OrtoWell® distractor. This hydraulically powered distractor is intended for inter-surgical separating and holding apart vertebral bodies. The hydraulic control of force has been developed in order to allow for a nuanced, incremental increase in force application to reduce the high risk of damaging the vertebrae and increase visibility between them for facilitating the safe and precise placement of implants or prostheses. Compared to other systems it does not require additional instruments like forceps to apply manual forces which need to sit in the space between the vertebra and requires no additional screws or lever which need to be turned. The OrtoWell® distractor shall generate a proper working area for insertion of cages or prostheses. The gentler hydraulic expansion compared to manual distractors could be also beneficial in cases of impaired bone structure (eg osteoporosis). Typical areas of application include discectomy and corpectomy requiring vertebral body replacement, spinal disc prostheses or interbody fusion cages.
Previously, a case study documented the successful use of the device in a 2-level corpectomy with vertebral body replacement and fusion,10 but data from prospective clinical trials on this device are still pending. The current study aims to fill this gap.
Besides evaluating the basic safety of the OrtoWell® distractor through assessments of complications and handling, this study provides more details on whether the device facilitates surgical procedures. Focus was put on the surgeons’ experience with the device, because such clinical insights are of high importance to evaluate the practical value of medical devices14 and for creating future health technology assessments in surgery.15 To assess a more detailed understanding of distractor handling, evaluations of general device performance were conducted as well as evaluations of device subcomponents. Besides assessments of intra-operative and postoperative adverse events, cardiovascular markers were used as additional indicators for potential complications.
Materials and Methods
Study Design and Patient Selection
This study was a prospective, single-arm, multi-center, observational, post-market clinical follow-up study. Based on a normal estimated enrollment rate per site and taking in account the participation of 3 sites during a 3 months enrollment period, a total of 30 patients was expected to be satisfactory, since the validity of theoretical assumptions for asymptotic methods would be fulfilled in most of the cases. Study duration was from April 2018 to April 2023. All patients gave their written informed consent before participation. When inclusion criteria were fulfilled and none of the exclusion criteria applied, the first measurements were conducted.
Criteria for Inclusion Were
- The OrtoWell® Distractor System is indicated, ie, patients who are indicated to underwent anterior or lateral spinal surgery with required separation of vertebrae
- Patients are between 18 and 75 years old
Exclusion Criteria Were
- Pregnancy at the time of spinal surgery
- Known osteoporosis
- Obstacles to perform radioscopy (primarily lateral), such as obesity (Body Mass Index [BMI] ≥ 30 kg/m2)
Subsequently, the respective surgical procedure was conducted with use of the OrtoWell® Distractor System. Overall, assessments were performed at four visits: screening/baseline, at the time or directly after the index procedure, before discharge and at 30 days follow-up. During study participation, all unscheduled visits and subsequent spinal surgical interventions were recorded, if relevant. A detailed overview of assessment points and parameters is given in Table 1.
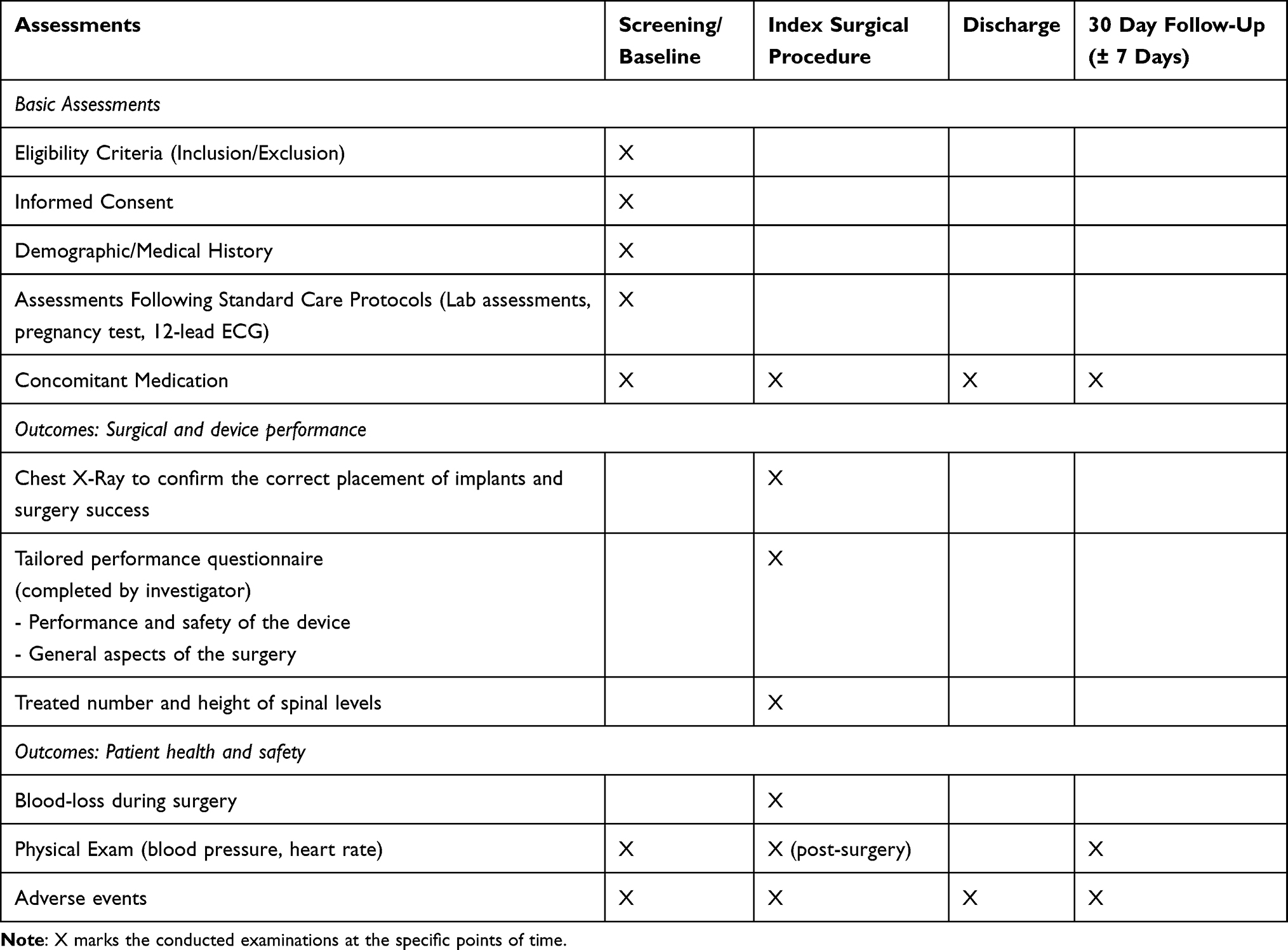 |
Table 1 Schedule of Assessments |
Investigational Device
The OrtoWell® Distractor System (OrtoWay Inc., Horsham, PA, USA) is a surgical hydraulic system for separating, holding apart or repositioning vertebrae during surgery (Figure 1). It is intended to facilitate removal of spinal structures as during corpectomies, implantation of disc prostheses and fusion procedures with spinal cages. It offers adequate holding strength and freedom of movement and precise calibrations with altering forces during surgery in a gentle way to create the greatest required room to work during surgery with the least risk. The purpose of the system is to provide precise control of the applied force through hydraulic force transmission as compared to other common distractor devices which are based on the application of manual force, or applied eg via screw reversal that likely may increase over-distraction. Ha et al 2013 discussed in cervical usage that for the manual Casper retractor that uses a screw-mechanism, surgeons habitually turn the lever without considering how much excessive force is being applied to the vertebra in cases where the intervertebral disc space is insufficiently exposed after initial distraction. Results of that study highlight the clinical relevance of distraction force in the immediate postoperative period showing that distraction force affects the surgical outcome and controlling the distraction force is essential.16 This could be also valid for thoracic and lumbar spine.
 |
Figure 1 Investigational device, OrtoWell® Distractor System, lateral distractor unit. |
The OrtoWell® Distractor System is used by positioning four or two screws (for bilateral or unilateral application, respectively) near the vertebral endplates. For marking the target position of screws, an awl is used to create notches in the vertebrae. Subsequently, the screws are applied and the distractor unit(s) are mounted onto these screws. For unilateral application, one distractor unit is mounted and for bilateral application two units. Surgeons can incrementally increase the pressure of the hydraulic mechanism through handles and thereby gradually extend the pistons. This increases the space between vertebrae, allowing the surgeon to perform the desired surgical procedure with precise control over vertebral spacing. The angle between the screws and the distractor unit can then be adapted to alter the direction of the applied force.
The system can be used with different approaches, including lateral approach. To our knowledge, this is not possible with other distractors currently on the market.
After the procedure has been performed, the pressure is gradually released and the device is removed.
Outcome Measures
Across the different measurement time-points, assessments of safety and patient characteristics were conducted and after the surgical procedure, device performance was assessed (Table 1).
The primary outcome measures were the questionnaires on device performance and safety which were completed by the investigators to evaluate performance, safety and usability of the distractor.
Four items assessed how the distractor system affected surgery (“Simplified”, “Neither simplified nor made surgery more difficult”, “Made surgery more difficult”), its position accuracy (“Not good”, “Good”, “Very good”), its holding capacity (“Not good”, “Good”, “Very good”) and in case of multiple spinal levels treated it was noted whether device problems occurred with two or more spinal levels. Additionally, functionality of the following subcomponents was rated on a three-point scale (“Not good”, “Good”, “Very good”): spacers for distractor height, measurement rods for choice of piston rods, tools for attachment of the distractor, use of the marker for the screws (awl), hydraulic application of the force, screws, general stability of the system.
Furthermore, issues regarding correct usage were assessed, ie, whether correct usage was performed according to the instructions for use (IFU, yes/no) and whether instructions were sufficient (yes/no). Furthermore, investigators indicated whether surgery went according to plan (yes/no) and whether any delay was related to the device. At follow-up, medical personal evaluated whether overall daily functioning of patients changed (“better”, “worse” with description, “same”).
Secondary outcome variables included the duration of the surgical procedure and any reasons for surgical delays, evaluation of complications, duration of hospital stay, causes of mortality, and re-operations, re-hospitalization.
Analysis
The study population was defined according to the Intention-to-Treat principle. All enrolled patients were considered in the analysis of all parameters, without any planned exclusion. In case of missing data, no interpolations were made. Statistical analysis was performed with Microsoft® Excel® 2016 (version 16.0.5469.1000, 32-bit). For all measures, descriptive statistics was performed. For continuous variables, mean values and standard deviations are provided, as well as minimal and maximal values. For qualitative variables, case counts are provided and for device ratings percentage values were calculated.
Results
Patient Characteristics
In total 31 patients were recruited (Table 2). All patients signed the informed consent form before participation in the study and fulfilled the inclusion and none of the exclusion criteria. 3 sites in Germany participated in the study with a patient distribution of: n=24 Bonn, n=5 Essen, n=2 Tutzing. One patient withdrew their consent directly after surgery and the data was excluded, resulting in an available sample size of n = 30.
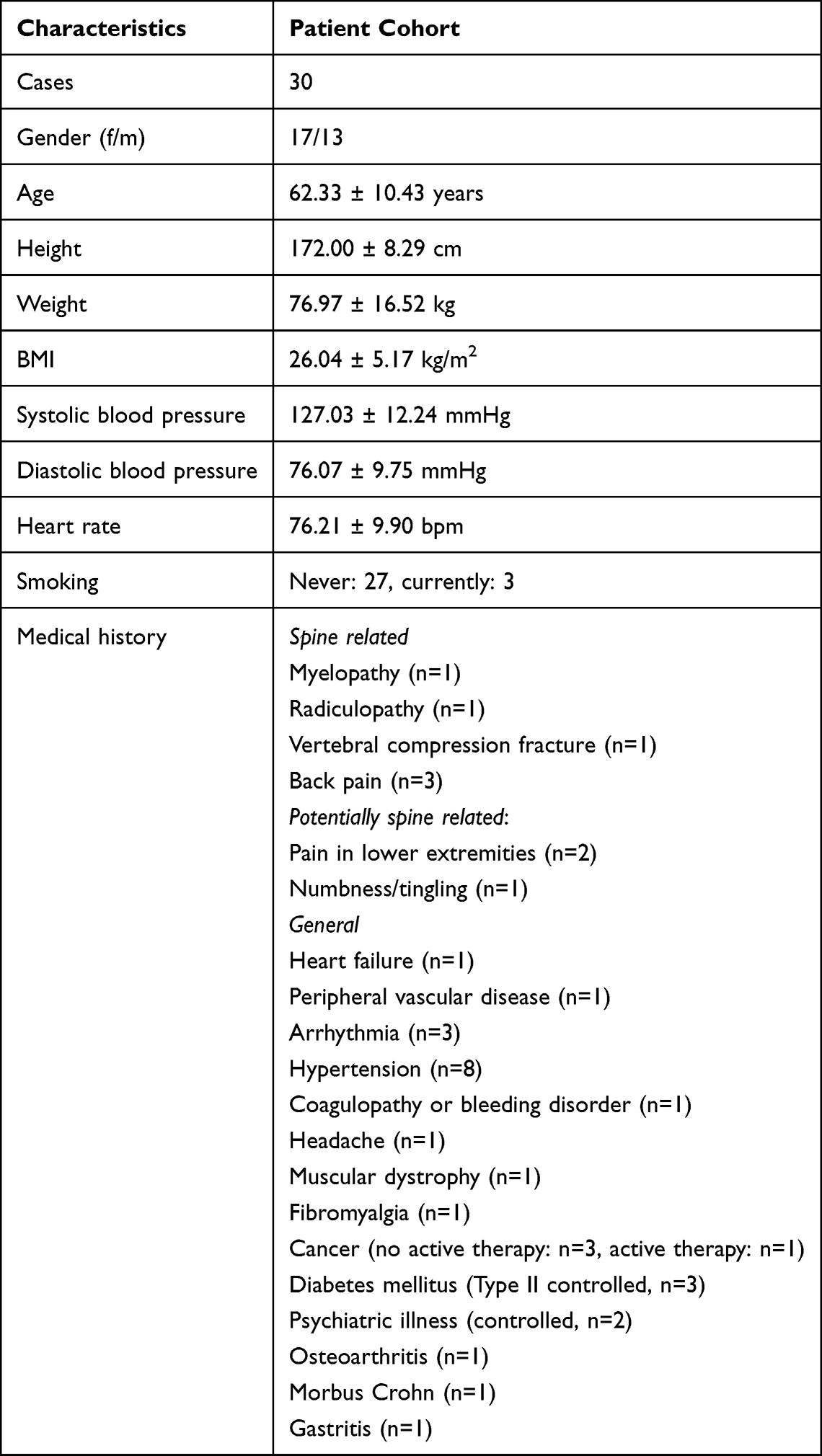 |
Table 2 Patient Characteristics at Baseline |
In 19 patients, the total duration of conservative treatment for the painful discs was between 6 and 12 months, in 9 patients > 12 months and 1 patient < 6 months (1 patient unknown). Patients underwent multiple types of conservative treatments, including narcotic medication (n=16), non-narcotic medication (n=19), other pharmacologic therapy (n=1), bed rest (n=11), physical therapy (n=15), training on safe movement/safe weight-bearing exercise (n=1), spinal bracing (n=5), n=2 (Transcutaneous Electrical Nerve Stimulation [TENS]/Electrical Muscle Stimulation [EMS], infiltration). Medical history is listed in Table 2. Laboratory results at inclusion showed no abnormalities. 15 patients had a history of prior spinal surgery for painful degenerative disc disease (DDD, several types are possible per patient).
Surgical Procedures
The mean time for the procedure (first incision – skin closed) was 2:43 h ± 1:14 h (range: 1:02 h–5:49 h). The mean time of anesthesia (start – stop) was 3:59 h ± 1:18 h (range: 1:50 h–6:32 h; n=26).
The treated spinal level(s) ranged between T9 and S1. 13 patients had prior spinal surgeries (fusion n=8; corpectomy, discectomy, fusion n=1; transforaminal lumbar interbody fusion (TLIF) n=1; total disc replacement n=1; discectomy n=1) at one or multiple spinal levels, see Table 3. In two cases. the surgeon did only provide data on the number of treated levels and did not record the actual height.
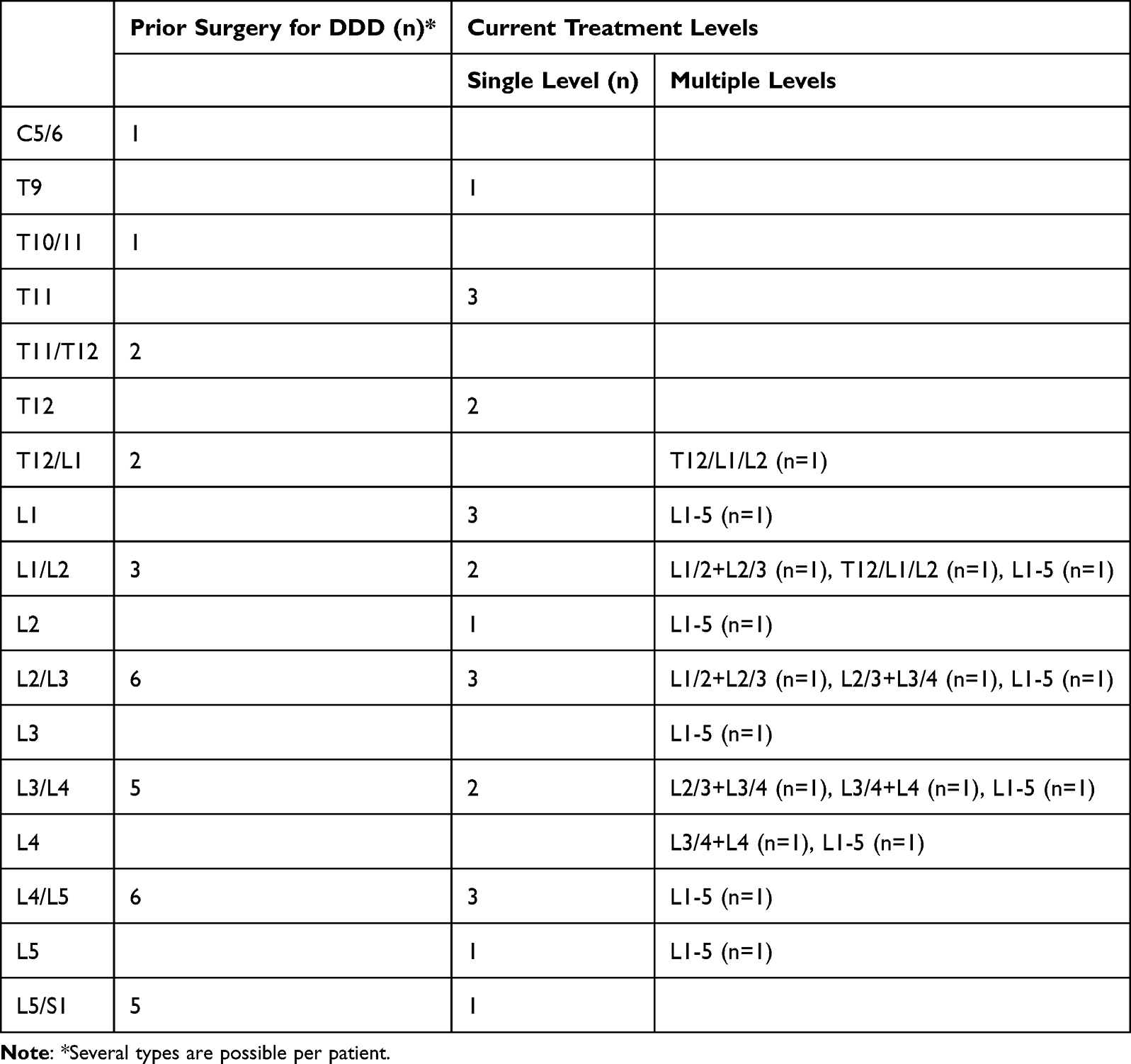 |
Table 3 Prior History of Surgery and Current Spinal Levels Treated |
The following surgical approaches were used: TLIF (n=2), anterior lumbar interbody fusion (ALIF, n=17), lateral lumbar interbody fusion (LLIF, n=2), oblique lumbar interbody fusion (OLIF n=2), fusion of T10-L2, (n=1), ventral retroperitoneal approach (n=5). The following surgical access was used: Open (n=18), Mini-open (n=10), minimally invasive (n=1).
A chest x-ray was performed in 28 of 30 patients. The screws were evaluated as being placed with correct distance in 25 patients, not correctly in 3 patients (n=28; 2 unknown), no problems with intraoperative placement of the screws were noted. In 20 patients (n=29; 1 unknown) the bilateral distractor units were mounted, in 9 an unilateral unit. In none of the patients problems with the use of the distractor were noted.
Distractor Performance
In 27 patients, handles to control pressure and extend pistons in the distractor unit were noted and ranged from 80 to 170 bar (147.69 ± 29.48 bar, documented in 13 patients), for the other interventions the devices were used pre-calibrated. No problems with the use of the handles occurred. The OrtoWell® System was used as intended without any difficulties.
The mean blood loss was 215.17 ± 113.57 cc (range 50–500 cc). The mean hospital stay was 16.39 ± 10.25 days (range 4–38 days) (n=23).
Ratings on performance and usability for each surgery (Figure 2) showed maximally positive evaluations across all questions. Only in 2 surgeries, the duration of procedure was experienced as minor increased and rated as “slightly longer than expected”. The delay was caused by special anatomy with a high iliac crest and severe fibrosis anterior to the index level including severe osteochondrosis of the index level.
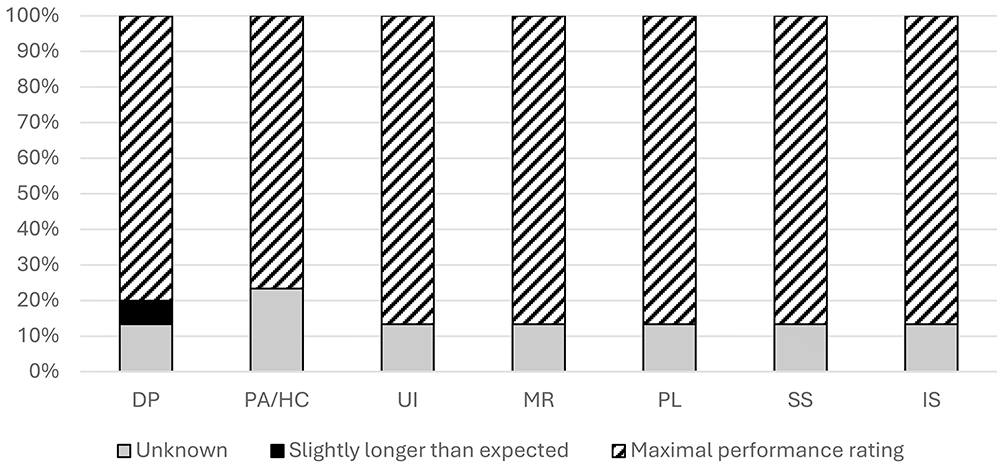 |
Figure 2 Investigator ratings of distractor performance and usability. DP: duration of procedure, PA/HC: positioning. |
In all cases, the OrtoWell® Distractor was rated to simplify the surgery in relation to other systems that were used by the surgeons (n=26; 4 unknown). Additional comments by investigators, were: “keeps disc space open, easier to take out disc tissue” and “significantly helped surgery”. Surgeons noted no problems with the OrtoWell® Distractor related to the treatment of two or more levels.
The positioning accuracy and holding capacity of the device was rated as “very good” in all cases (n=23; 4 unknown). The surgical operation proceeded as planned in all cases (n=26; 4 unknown).
Functionality of subcomponents (Figure 3) was dominantly assessed with maximal performance ratings across all items (n = 26; 4 unknown).
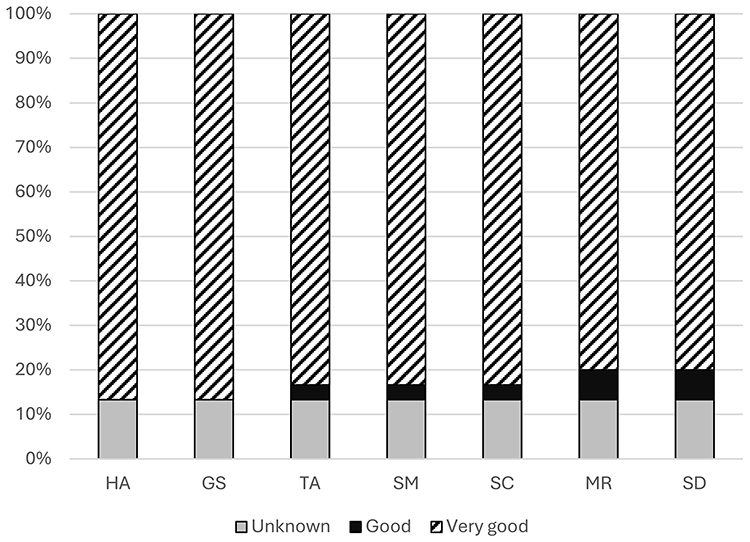 |
Figure 3 Investigator ratings for distractor subcomponent functionality. HA: The hydraulic application of the force, GS: The general stability of the system, TA: Tools for attachment of Distractor, SM: The use of the marker for the screw, SC: The screws, MR: Measurement rods for choice of piston rods, SD: Spacer of Distractor height. No ratings in four cases. |
Patient Health and Life Factors After Surgery
All patients performed an ECG before surgery with a normal result. Post-surgical cardiovascular function was within normal ranges. Mean systolic blood pressure post procedure was 125.85 ± 6.40 mmHg (range 113–137 mmHg) and the diastolic blood pressure was 75.96 ± 7.67 mmHg (range 60–95 mmHg) (n=27; unknown). At discharge, the mean heart rate was 72.67 ± 7.35 bpm (range 57–96 bpm) (n=27; unknown). At 30 days follow-up, the mean systolic blood pressure was 126.48 ± 5.09 mmHg (range 115–130 mmHg; n=25), mean diastolic blood pressure was 75.40 ± 4.55 mmHg (range 65–80 mmHg; n=25) and the mean heart rate was 74.38 ± 6.45 bpm (range 67–98 bpm; n=24) (Figure 4A–C). None of the cardiovascular measures showed pronounced differences between baseline and follow-up.
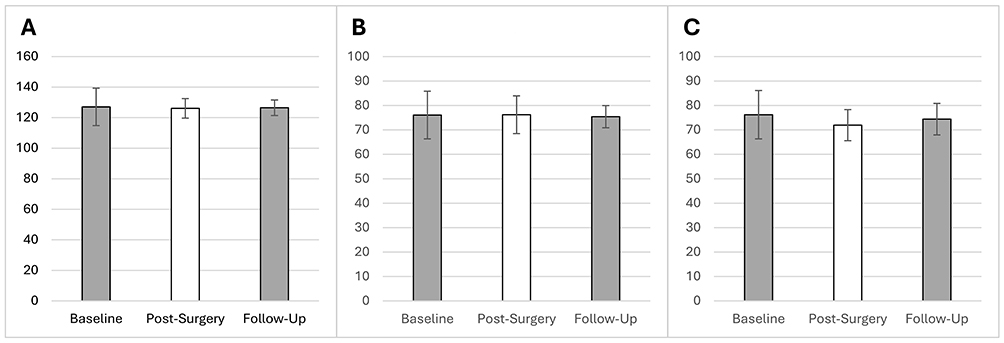 |
Figure 4 Cardiovascular measures across time. (A). Systolic blood pressure [mmHg]. (B). Diastolic blood pressure [mmHg]. (C). Heart rate [bpm]. |
Compared to baseline, overall daily functioning of patients was rated as “Better” in all cases (n=28; 2 unknown). At discharge, the mean weight was 78.47±16.62 kg (range 43–130 kg) and the BMI 26.3±5.1 and at follow-up 25.75±5.2. After discharge, appropriate medication (narcotic: n=2, non-narcotic: n=20) was administered depending on the indication, along with stabilization using orthoses (n=7) and mobilization through physiotherapy (n=17).
Adverse Events
There were no unplanned procedures or adverse events during surgery. 1 adverse event, which was not related to the use of the device, occurred prior to discharge. The affected patient underwent re-operation (decompression) at the treated segment.
Discussion
When developing novel surgical devices, data has to be collected that can verify the safety, efficacy and usability of the given device. A range of such data can be gathered through premarket clinical studies but critical information on safety and performance has to be retrieved from applications in real-world settings.16 Particularly, effects on surgical performance in a more diverse patient group should be evaluated with samples that are gathered under the demands and constraints of everyday clinical work. The current study provided such data, including outcome data of 30 patients undergoing lumbar and thoracic spinal surgeries with application of the hydraulic distractor (OrtoWell® Distractor System, OrtoWay Inc.) for separating vertebrae during surgery. The interventions in which the distractor was applied were performed between T9 and L5, with multiple access strategies, mainly open or minimally open, and in one case minimally invasive access. Variability was also present in the chosen surgical approaches of the current procedures. Whereas dominantly ALIF approaches were documented (54.84% of cases), nearly half of the sample data reflects distractor use with other approaches, including TLIF, LLIF, OLIF and ventral retroperitoneal approaches. Safe usage in different approaches offers a wider range of applications, which enables the surgeons to use the system with their preferred approach considering the patient and implant characteristics.
A key focus of the current study was to test the controllability of the distractor by operating surgeons. This was considered crucial, as there is a significant relationship between applied distraction force and tissue stress6 and controlled reversion of applied distraction is essential for incidence management.17 Consistently positive ratings were given by the surgeons on items that assessed the device as a whole, ie, on the possibility to control the device as intended, its positioning accuracy and holding capacity. Evaluations of subcomponents were aligned with these results and showed maximally positive ratings for hydraulic application of force and general stability. All surgeons evaluated the different aspects of the device with “good” or “very good” and no problems with specific subcomponents were evident.
This shows that the OrtoWell® is well accepted by the surgeons and easy to handle. Compared to commonly used distraction devices which rely on manual force control, eg paddle distractors7 or distraction systems like Caspar distractor,8 the subjective evaluation of the surgeons supports a more widely spread use of the system in clinical practice. However, besides intra-surgical safety and performance and clinical usability data supportive clinical patient-relevant outcome data from a larger patient group are required to fully show the clinical benefit of the OrtoWell® itself and in comparison to other systems.
Measures assessing the progress of overall procedures and the device’s role in them supported these notions. Procedures could be conducted as planned and daily functioning of all patients improved after surgery. Regarding the device’s effect on the index procedure, surgeons noted that the distractor simplified surgery, with minor increases in surgical time in two cases. However, considering the low occurrence rate and minor extend, this cannot be considered a significant device effect. Safety of the device was rated as good and no adverse events occurred during placement or use of the distractor system. One adverse event occurred prior to a patients’ discharge and required reoperation, but this was not related to the distractor or the related procedure. Blood loss was assessed as 215.17 ± 113.57 cc. As cardiac complications have been related to spinal surgery even with long-term assessments,18 cardiovascular parameters were tracked until follow-up but did not suggest any postoperative cardiovascular complications. The average duration of hospital stays amounted to 16.39 ± 10.25 days, a value within the ranges of larger datasets on lumbar fusion that included a similar variety of approaches.19,20
In addition to an assessment of the current intervention, previous spinal procedures were tracked. In a sample that can provide representative data on the real-world target population, medical history of previous spinal interventions was expected. Vulnerabilities caused by previous procedures could in these cases affect intervention outcomes and complicate surgery.21–23 In the recruited sample, all patients had received prior surgery for painful DDD across a range of spinal levels that overlapped with the levels treated in the current study. However, no complications or obstacles in conducting surgeries occurred, which shows that the distractor can also be used safe and effective at levels already treated beforehand. This confirms also the first data from successful usage of the device in a previously performed case-study.
Limitations
This study has an observational design with descriptive statistics. It focused on the surgeons’ experience with the investigated device and associated procedures. Although all patients improved with regard to their daily functioning after surgery, patient-centered measures, like pain or mobility ratings, could offer an additional perspective on device performance. However, the distractor was only one of many surgical tools applied and given the variability of approaches, it is unlikely that these measures would have yielded results directly traceable to the distractor. The conducted study evaluated safety, usability and early postoperative outcomes. Investigating the longer-term clinical impact, extended follow-ups will be necessary in larger scale studies to consider patient-centered outcome measures. Additional investigations that directly compare the system with other distractors would strengthen the evidence of this study, which was partially based on a subjective rating of the surgeons to evaluate the advantages of the system.
Conclusions
The current study described the application of a hydraulic distractor system across a range of surgical approaches in the lumbar and thoracic spine. Senior spine surgeons indicated based on their experience with other systems, first, that distraction could be performed with a good level of controllability and second, it facilitated surgical procedures. Increases in surgical time were minor and no complications or adverse events occurred in relation to the index procedures. Further studies could extend on these findings by focusing on patient rated outcomes and comparisons to other distraction devices. Due to the hydraulic pressure, there may be a reduced risk of over-distraction and a more precious application leading to less risks and better clinical outcome compared with other devices. In conclusion, the subjective rating of the surgeons revealed that the novel investigated distractor facilitated surgical work and enabled more perceived control during surgery when compared to other systems the surgeon had used before. Standard application of hydraulic distractors in spinal surgery could in the future help surgeons to focus more effectively on other critical aspects of the procedures and to reduce risks of vertebra damage.
Abbreviations
ALIF, anterior lumbar interbody fusion; BMI, body mass index; bpm, beats per minute; DDD, degenerative disc disease; DP, duration of procedure; EMS, electrical muscle stimulation; GS, the general stability of the system; HA, the hydraulic application of the force;. h, hours; IFU, instructions for use; IS, IFU sufficient; kg, kilogram; LLIF, lateral lumbar interbody fusion; m², square meter; mmHg, millimeters of mercury; MR, measurement rods for choice of piston rods; MR, mobilization and removal; OLIF, oblique lumbar interbody fusion; PA/HC, positioning accuracy/holding capacity; PL, surgical operation proceeded as planned; SC, the screws; SD, spacer of Distractor height; SM, the use of the marker for the screw; SS, device simplified surgery; TA, tools for attachment of Distractor; ENS, transcutaneous electrical nerve stimulation; TLIF, transforaminal lumbar interbody fusion; UI, usable according to the instructions for use.
Data Sharing Statement
The datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request.
Ethics Approval and Informed Consent
The study was submitted to the Ethics committee of the Medical faculty of the Rheinische Friedrich-Wilhelm’s-University Bonn, Germany (Medizinische Fakultät der Rheinischen Friedrich-Wilhelm’s-Universität Bonn), which is the responsible Ethics committee for the Clinic and Polyclinic for orthopedics and trauma surgery university Bonn, and accepted (EC file number: 353/17). The study was conducted in accordance with the ethical principles of the Declaration of Helsinki, and the written informed consent was obtained from each patient before participating in the study.
Funding
The sponsor of the study was OrtoWay-US Inc.
Disclosure
Stan Mikulowski represents the manufacturer of the device, which acted as sponsor. Stan Mikulowski also reports pending patents US 12,023017 B1, US 10,952,714 B1 and US 351461-2013. Staffan Bowald is affiliated with the manufacturer/sponsor. The other authors report no conflicts of interest in this work.
References
1. Loubresse C. Neurological risks in scheduled spinal surgery. Orthop Traumatol Surg Res. 2014;100(Suppl 1):S85–S90. doi:10.1016/j.otsr.2013.11.001
2. Byvaltsev VA, Kalinin AA, Konovalov NA. Minimally invasive spinal surgery: stages of development. Burdenko’s J Neurosurg. 2019;83(5):92–101. doi:10.17116/neiro20198305192
3. Denaro V, Denaro L, Martino AD, Longo UG, Maffulli N. Degenerative disk disease. In: Pitfalls in Cervical Spine Surgery: Avoidance and Management of Complications. London: Academic; 2010:121–163.
4. Tender GC, Serban D. Minimally invasive transforaminal lumbar interbody fusion: comparison of two techniques. Chirurgia. 2014;109(6):812–821.
5. Xie H, Ouyang Z, Zhang H. radiographic analysis of pedicle screw retractor-assisted transforaminal lumbar interbody fusion for single-segment spondylolisthesis in adults: a retrospective study and technical note. Orthop Surg. 2022;14(9):2219–2229. doi:10.1111/os.13441
6. Havey RM, Voronov LI, Tsitsopoulos PP, et al. Relaxation response of lumbar segments undergoing disc-space distraction: implications to the stability of anterior lumbar interbody implants. Spine. 2012;37(9):733–740. doi:10.1097/BRS.0b013e3182323adc
7. Lindley TE, Viljoen SV, Dahdaleh NS. Effect of steerable cage placement during minimally invasive transforaminal lumbar interbody fusion on lumbar lordosis. J Clin Neurosci. 2014;21(4):441–444. doi:10.1016/j.jocn.2013.06.006
8. Tippets RH, Apfelbaum RI. Anterior cervical fusion with the Caspar instrumentation system. Neurosurgery. 1988;22(6P1–P2):1008–1013. doi:10.1227/00006123-198806010-00006
9. Nordmann N, Weber MW, Nie JZ, Graves CM. Minimally invasive transforaminal lumbar interbody fusion with the Space-D access system. J Minim Invasive Spine Surg Tech. 2024;9(Suppl 1):S41–S48. doi:10.21182/jmisst.2023.01018
10. Desai B. Introduction to using a novel hydraulically powered system – ortoWell® Distractor – to separate vertebral bodies during anterior surgery: case report of a spine inflammation with need for 2-level corpectomy, vertebral body replacement, and fusion.
11. Leader BST, Moran C, Schmitt M, Ciha BD. Inflatable vertebral distractor. BME 300/200 Project Report. University of Wisconsin-Madison; 2014. Available from: https://bmedesign.engr.wisc.edu/projects/f14/vertebral_body_distractor/file/view/26255031-1379-44c1-993e-39574bcae017/Final_Report-Inflatable_Vertebral_Distractor.pdf.
12. Zippel C, Bohnet-Joschko S. Post-market surveillance in the German medical device sector – current state and future perspectives. Health Policy. 2017;121(8):880–886. doi:10.1016/j.healthpol.2017.06.005
13. Badnjevic A, Gurbeta Pokvic L, Deumic A, Spahic Becirovic L. Post-market surveillance of medical devices: a review. Technol Health Care. 2022;30:1315–1329. doi:10.3233/THC-220284
14. Sawant S, Joshi P, Sawant S. Usability testing of healthcare devices: a review of the current UX methods used for usability testing of healthcare devices. Proc Hum Factors Ergon Soc Ann Meet. 2023;67(1):1078–1083. doi:10.1177/21695067231192409
15. Erskine J, Abrishami P, Charter R, et al. Best practice considerations on the assessment of robotic-assisted surgical systems: results from an international consensus expert panel. Int J Technol Assess Health Care. 2023;39(1):e39. doi:10.1017/S0266462323000314
16. Hoogervorst LA, Geurkink TH, Lübbeke A, et al. Quality and utility of European cardiovascular and orthopedic registries for the regulatory evaluation of medical device safety and performance across the implant lifecycle: a systematic review. Int J Health Policy Manag. 2023;12:7648. doi:10.34172/ijhpm.2023.7648
17. Hejrati N, Srikandarajah N, Alvi MA, et al. The management of intraoperative spinal cord injury - a scoping review. Global Spine J. 2024;14(3 Suppl):150S–165S. doi:10.1177/21925682231196505
18. Guyot JP, Cizik A, Bransford R, Bellabarba C, Lee MJ. Risk factors for cardiac complications after spine surgery. Evid Based Spine Care J. 2010;1(2):18–25. doi:10.1055/s-0028-1100910
19. Kobayashi K, Imagama S, Ito Z, et al. Predictors of prolonged length of stay after lumbar interbody fusion: a multicenter study. Spine J. 2019;19(4):650–656.
20. Pokorny G, Amaral R, Marcelino F, et al. Minimally invasive versus open surgery for degenerative lumbar pathologies: a systematic review and meta-analysis. Eur Spine J. 2022;31:2502–2526. doi:10.1007/s00586-022-07327-3
21. Zehnder P, Aghayev E, Fekete TF, Haschtmann D, Pigott T, Mannion AF. Influence of previous surgery on patient-rated outcome after surgery for degenerative disorders of the lumbar spine. Eur Spine J. 2016;25(8):2553–2562. doi:10.1007/s00586-016-4383-x
22. Riksaasen AS, Kaur S, Solberg TK, et al. Impact of the number of previous lumbar operations on patient-reported outcomes after surgery for lumbar spinal stenosis or lumbar disc herniation: a population-based cohort study from the Norwegian Registry for Spine Surgery. Bone Joint J. 2023;105(B4):422–430. doi:10.1302/0301-620X.105B4.BJJ-2022-0704.R1
23. Roiha M, Marjamaa J, Siironen J, Koski-Palkén A. Inferior long-term outcomes after surgery for lumbar disc herniation in patients with prior lumbar spine surgery. Acta Neurochir. 2024;166:32–40. doi:10.1007/s00701-024-05932-3
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.