Back to Journals » Clinical, Cosmetic and Investigational Dermatology » Volume 19
A Preliminary Study of Polycaprolactone Filler After Hyaluronidase for Facial Overfilled Syndrome
Received 7 April 2026
Accepted for publication 12 June 2026
Published 23 June 2026 Volume 2026:19 615095
DOI https://doi.org/10.2147/CCID.S615095
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Jeffrey Weinberg
Zhiqiang Xue, Changwon Kim, Dahee Hwang
Juvenate Beaucare Clinic, Beijing, People’s Republic of China
Correspondence: Zhiqiang Xue, Email [email protected]
Background: Hyaluronidase effectively degrades hyaluronic acid (HA) fillers in facial overfilled syndrome (FOS). However, the subsequent volume reduction may create soft tissue hollowing and contour irregularities.
Objective: To evaluate the aesthetic and structural changes following polycaprolactone (PCL) filler injection after hyaluronidase treatment in patients with FOS.
Methods: This single-arm, retrospective study enrolled patients with FOS who underwent hyaluronidase treatment followed by a PCL injection. Outcomes included Global Aesthetic Improvement Scale (GAIS), upper cheek fullness, temporal hollowing, 3D midfacial volume, and ultrasound-measured soft tissue–to-bone distance. Assessments were performed at baseline, after hyaluronidase, and at 3 and 6 months post-PCL treatment.
Results: 12 patients were enrolled. At 6 months after PCL injection, improvements were observed in GAIS (P < 0.001) and upper cheek fullness (P = 0.016). Using the pre-hyaluronidase state as baseline, the 3D midfacial filler volume decreased by 2.48 mL after hyaluronidase injection (P < 0.001), by 4.88 mL at 3 months after PCL treatment (P < 0.001), and by 5.14 mL at 6 months after PCL treatment (P < 0.001). Conversely, the ultrasound-assessed distance from soft tissue to bone surface was 1.21 mm greater than baseline after hyaluronidase treatment (P < 0.001), and 2.09 mm and 3.23 mm lower than baseline at 3 and 6 months after PCL injection, respectively (both P < 0.001). No adverse events were reported after hyaluronidase and PCL treatment.
Conclusion: In this preliminary study, aesthetic improvement and changes in soft tissue parameters were observed after PCL injection following hyaluronidase treatment.
Keywords: facial overfilled syndrome, hyaluronidase, polycaprolactone filler, hyaluronic acid
Introduction
Aesthetic medicine is a rapidly expanding field that integrates medical technology and pharmaceutical products to enhance physical appearance. This growth is driven by advances in medical science, demographic changes, increased life expectancy, and a cultural emphasis on youthful aesthetics.1 Non-invasive procedures such as fillers and laser treatments have become increasingly popular due to their short recovery time and lower risk.2 According to the International Society of Aesthetic Plastic Surgery (ISAPS) 2024 report, hyaluronic acid (HA) injections rank second among all non-surgical procedures performed globally, accounting for 30.9% of treatments, with a 56.4% increase from 2020 to 2024,3 highlighting the rising demand for soft-tissue fillers.
With the growing use of injectable fillers, complications have also become more frequent. Facial overfilled syndrome (FOS)—a condition caused by excessive soft-tissue filler accumulation—results in a heavy, swollen, or distorted facial appearance and may progress over time. FOS presents with various manifestations, including “flowerhorn forehead”, “sunset eyes”, “chipmunk cheeks”, “witch chin”, “pillow face”,4 and the recently described “Taurus Philtrum”.5 Its causes are multifactorial, including societal pursuit of exaggerated “ideal” fullness,4 profit-driven practices promoting high-volume injections, insufficient understanding of facial aesthetics,4,6 improper filler selection or technique, and repeated injections causing cumulative volume imbalance.7 Beyond aesthetic distortion, FOS may make patients appear older or disproportionate,8 disrupt facial harmony,9 cause dissatisfaction and psychological stress, and even trigger anxiety or depression.10 Overfilling can also lead to surface irregularities or nodules, sometimes with pain during facial movement.11 A recent MRI study showed HA fillers may persist in fat pads for up to 27 months,12 indicating the impact of FOS can be prolonged and clinically significant.
For FOS resulting from excessive HA, hyaluronidase remains one of the most effective corrective treatments.13,14 Hyaluronidase rapidly degrades HA, reducing excessive volume. However, because HA fillers often provide structural support within subcutaneous fat or fascial compartments, their rapid dissolution may cause sudden loss of support, leading to localized hollowing, contour irregularities, skin laxity, or sagging. Therefore, post-dissolution tightening treatments are recommended to stimulate collagen regeneration and restore tissue firmness.4
Recently, polycaprolactone (PCL)–based fillers have emerged as next-generation biostimulatory injectables with strong potential for volume restoration and structural lifting.15 PCL is a biocompatible, biodegradable polymer that stimulates type I collagen production, enabling long-lasting tissue support. Its immediate volumizing effect derives from the carboxymethyl cellulose (CMC) gel carrier, while its high elastic modulus (G′≈1000 Pa) provides mechanical stability and reduces the risk of migration or irregular distribution.16 Previous studies have investigated the use of PCL-based fillers across multiple facial regions—such as the forehead,17 midface,18 T-zone,19 and nasolabial folds20—and consistently demonstrated their combined benefits of immediate volumization and long-term collagen stimulation. Moreover, clinical evidence shows that PCL injection into the temporal region and its associated supporting structures can substantially improve facial laxity. At the same time, comprehensive full-face treatment further refines the lateral cheek contour and achieves overall facial tightening.21
Although post-dissolution hollowing, contour irregularities, skin laxity, and sagging may occur after hyaluronidase-mediated HA degradation, evidence regarding optimal post-dissolution management remains limited. In particular, few studies have investigated restorative strategies to rebuild soft-tissue support after hyaluronidase treatment, and the clinical benefit of adjunctive modalities, such as energy-based tightening procedures, remains uncertain in this setting. Given the collagen-stimulating and volume-restorative properties of PCL-based fillers, we hypothesized that PCL injection after hyaluronidase treatment may serve as a potential restorative approach for post-dissolution hollowing and facial contour irregularities in patients with FOS. Therefore, this exploratory study aims to evaluate the efficacy and safety of PCL as a post-dissolution treatment to restore firmness and lift in patients with FOS.
Methods
Study Design and Participants
This retrospective single-arm study was conducted at Beijing Juvenate Beaucare Medical Cosmetic Clinic between July 1, 2023, and July 1, 2024. Adults (≥18 years) with a diagnosis of FOS confirmed by the treating physician were eligible. The diagnosis required a documented history of midfacial HA injection, visible midfacial overfilling, and ultrasonographic confirmation of residual material. All consecutive eligible patients who subsequently received PCL treatment at the study site were included. Individuals were excluded if complete pre- and post-treatment medical records were unavailable. The study was conducted in accordance with the Declaration of Helsinki, and the study protocol was approved by the Shanghai Ethics Committee for Clinical Research (Approval Letter No.: SECCR2024-181). The study met the criteria for a waiver of informed consent due to its retrospective data collection and the use of fully de-identified records. Written informed consent was obtained from one participant specifically for the publication of clinical photographs.
Treatment Procedures and Data Collection
Consecutive patients newly diagnosed with FOS were identified through the electronic medical record system. Detailed chart reviews were conducted to obtain demographic information, relevant clinical characteristics (overfilled regions and filler location), treatment parameters, and documented outcomes. Treatment-related variables included hyaluronidase injection technique, injection sites, and depths, as well as PCL dose, injection sites, and injection depths. Hyaluronidase (Jilin Aodong Taonan Pharmaceutical Co., Ltd., Taonan, China) was reconstituted to 1500 IU in 20 mL of normal saline, and routine skin testing was performed before administration using a 23-gauge needle. Ultrasound guidance was used to facilitate injection into residual filler deposits. Injection volume was determined based on the estimated filler volume, typically at approximately 1 mL per cm3 of filler. PCL (Sinclair Pharma Ltd., London, United Kingdom) was injected immediately following hyaluronidase treatment using a 23-gauge needle based on clinical judgment. A 23-gauge needle was selected to improve needle visualization and stability under ultrasound.
Efficacy was evaluated using documented aesthetic scales and imaging records. The Global Aesthetic Improvement Scale (GAIS) was used to assess overall aesthetic change, with scores ranging from 1 = worsened, 2 = no change, 3 = improved, 4 = much improved, to 5 = very much improved. The upper cheek fullness score reflected midfacial contour, ranging from 0 = no overfilling to 4 = overfilling. The temporal hollowing score assessed temple volume status, ranging from 0 = convex to 4 = severe hollowing. All assessments were performed independently by the treating physicians using a standardized evaluation protocol. Objective measures included standardized photographic analysis, three-dimensional (3D) midfacial filler volume, and ultrasound-measured soft tissue–to-bone distance. Quantitative 3D volume analysis was performed in the anteromedial cheek region, defined individually for each participant and varying in size.22 3D imaging was performed using the Meiji P2 3D scanner (Hangzhou Xiaofu Technology Co., Ltd., Hangzhou, China). All measurements and analyses were performed by trained investigators using a consistent protocol. Outcome measures were extracted from routine clinical assessments. GAIS, upper cheek fullness, and temporal hollowing scores were recorded after hyaluronidase treatment and at the 3- and 6-month follow-ups following PCL injection. PCL was administered on the same day as hyaluronidase treatment. For 3D midfacial volume and ultrasound-measured soft tissue–to-bone distance, measurements were available at four time points: pre-hyaluronidase, immediately post-hyaluronidase, and 3 and 6 months after PCL injection. Ultrasound measurements were performed independently by three trained physicians at the same anatomical locations. Each measurement was repeated three times, and the mean value was used for analysis. Safety data were obtained from chart-documented adverse events, including event type, onset, and severity. All data were fully anonymized before analysis, with removal of all direct and indirect identifiers to ensure that no participant could be re-identified.
Statistical Analysis
Data were presented as mean ± SD for continuous variables and as number (percentage) for categorical variables. Given the multiple follow-up time points, the McNemar test with Bonferroni correction was used to compare GAIS, upper cheek fullness, and temporal hollowing scores between baseline and each follow-up assessment. Generalized estimating equations (GEE) were applied to estimate mean differences between baseline and each time point, along with corresponding 95% confidence intervals, for 3D midfacial volume and ultrasound-measured soft–tissue–to–bone distance. A two-sided alpha level of 0.05 was considered statistically significant. All statistical analyses were performed using SAS software (version 9.4).
Results
Baseline Demographic and Clinical Characteristics
Twelve female participants with a mean age of 42 ± 5 years were included. The mean hyaluronidase dose was 6.3 ± 3.5 mL per patient. Table 1 summarizes the baseline characteristics of the participants and the treatment protocols used for FOS. Overfilled regions in this study were limited to the nasolabial fold and malar region, each accounting for 66.67% of cases. Filler materials were primarily located in the subcutaneous fat layer (50%), followed by the fibrous layer between superficial and deep fat (41.67%) and the deep fat layer above the periosteum (25%). Correspondingly, hyaluronidase was most frequently injected along the inferior malar border (75%) and nasolabial groove (50%), with injection depths spanning subcutaneous, inter-fat fibrous, and deep fat layers. Following hyaluronidase treatment, PCL was mainly injected into the temporal (58.33%) and preauricular (58.33%) regions, predominantly within the superficial layer of the deep temporal fascia and superficial masseteric–parotid fascia. The mean PCL volume administered was 1.88 ± 0.49 mL.
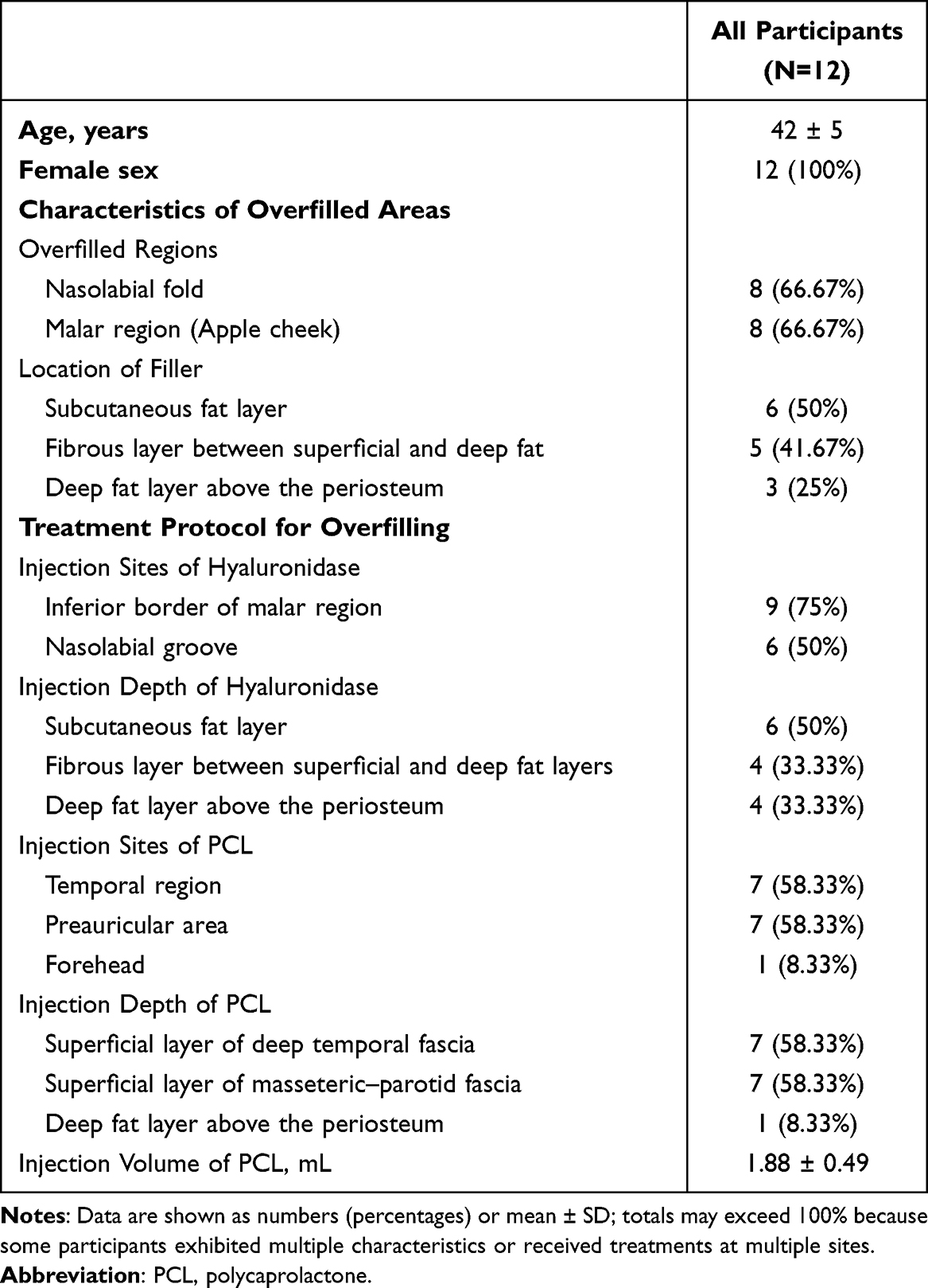 |
Table 1 Baseline Characteristics of Participants with Overfilling and Corresponding Treatment Protocols |
Clinical Evaluation Outcomes
All participants demonstrated aesthetic improvement following PCL treatment (Table 2). GAIS scores showed that all patients were rated as “significantly improved” (score 5) at both 3 and 6 months after PCL injection, compared with universal worsening (score 1) after hyaluronidase treatment (P = 0.0005 for both time points). Frontal and lateral photographs illustrated improvements in FOS from baseline to 6 months after PCL injection (Figure 1). Upper cheek fullness also improved significantly. Before PCL injection, only 41.67% of patients exhibited a score of 0 (no overfilling), whereas all patients (100%) achieved complete correction (score 0) at both 3 and 6 months post-treatment (P = 0.0156 for both comparisons). Temporal hollowing scores showed an improving trend but did not reach statistical significance. The proportion of participants with a fully contoured temple (score 0) increased from 41.67% pre-PCL to 58.33% at both 3 and 6 months. However, the overall distribution of scores did not differ significantly from baseline (P = 0.2500).
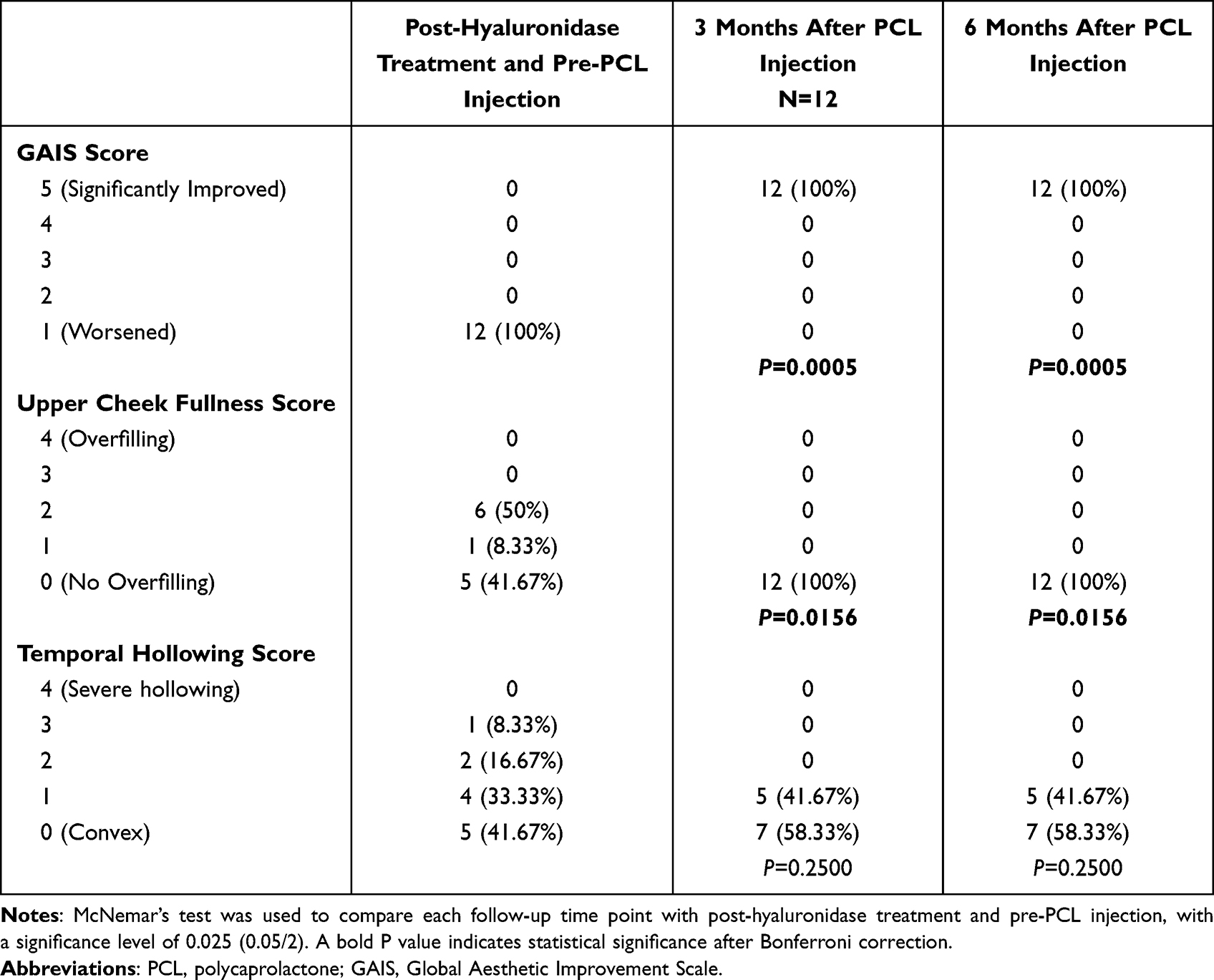 |
Table 2 Comparison of Clinical Evaluation Measures at Different Follow-up Time Points After Overfilling Treatment |
 |
Figure 1 Photographs of a 35-year-old female participant who previously received 1 mL of Juvéderm Voluma in each side of the midface. Hyaluronidase was administered at 300 U on the left side and 375 U on the right side. Polycaprolactone (PCL) was injected as 1 mL per site into the bilateral temporal and preauricular fascial regions. The images illustrate changes in facial overfilled syndrome from baseline to 6 months after PCL treatment, shown in frontal (A–D) and lateral (E–H) views. (A and E) The baseline image obtained before hyaluronidase administration showed facial overfilled syndrome. (B and F) Improvement in facial overfilled syndrome was observed 1 month after hyaluronidase treatment, prior to PCL treatment. (C and G) Skin tightening was observed 1 month after PCL filler injection. (D and H) The treatment effect persisted at 6 months after PCL filler injection. |
3D Volume and Ultrasound Assessments
Figures 2 and 3 display representative images showing changes in 3D midfacial filler volume and ultrasound-assessed soft tissue-to-bone distances, respectively. In Figure 3, the HA nodule (HA-N) and the corresponding measurement location are shown to illustrate the ultrasound-guided assessment of residual filler deposits. Quantitative analysis demonstrated significant improvements in 3D midfacial filler volume and ultrasound-measured soft tissue–to-bone distance after overfilling treatment (Table 3). Mean 3D midfacial filler volume decreased from 5.32 ± 1.06 mL at baseline to 2.85 ± 0.56 mL after hyaluronidase treatment, reflecting a mean change of –2.48 mL (95% CI: –2.93 to –2.02; P < 0.0001). At 3 months and 6 months after PCL injection, the mean volumes were 0.44 ± 0.50 mL and 0.18 ± 0.30 mL, corresponding to baseline differences of –4.88 mL and –5.14 mL, respectively (both P < 0.0001). Ultrasound measurements exhibited a distinct pattern. The soft tissue–to-bone distance increased from 3.78 ± 0.81 mm at baseline to 4.98 ± 1.11 mm after hyaluronidase treatment (+1.21 mm, 95% CI: 0.98 to 1.43; P < 0.0001). At 3 months and 6 months post-PCL injection, the distances decreased to 1.69 ± 0.81 mm and 0.55 ± 0.62 mm, corresponding to baseline differences of –2.09 mm and –3.23 mm, respectively (both P < 0.0001). These results indicate that hyaluronidase effectively reduced excessive filler volume, and that further changes in soft tissue contour were observed following PCL treatment over time, with a decrease in the soft tissue–to-bone distance on ultrasound.
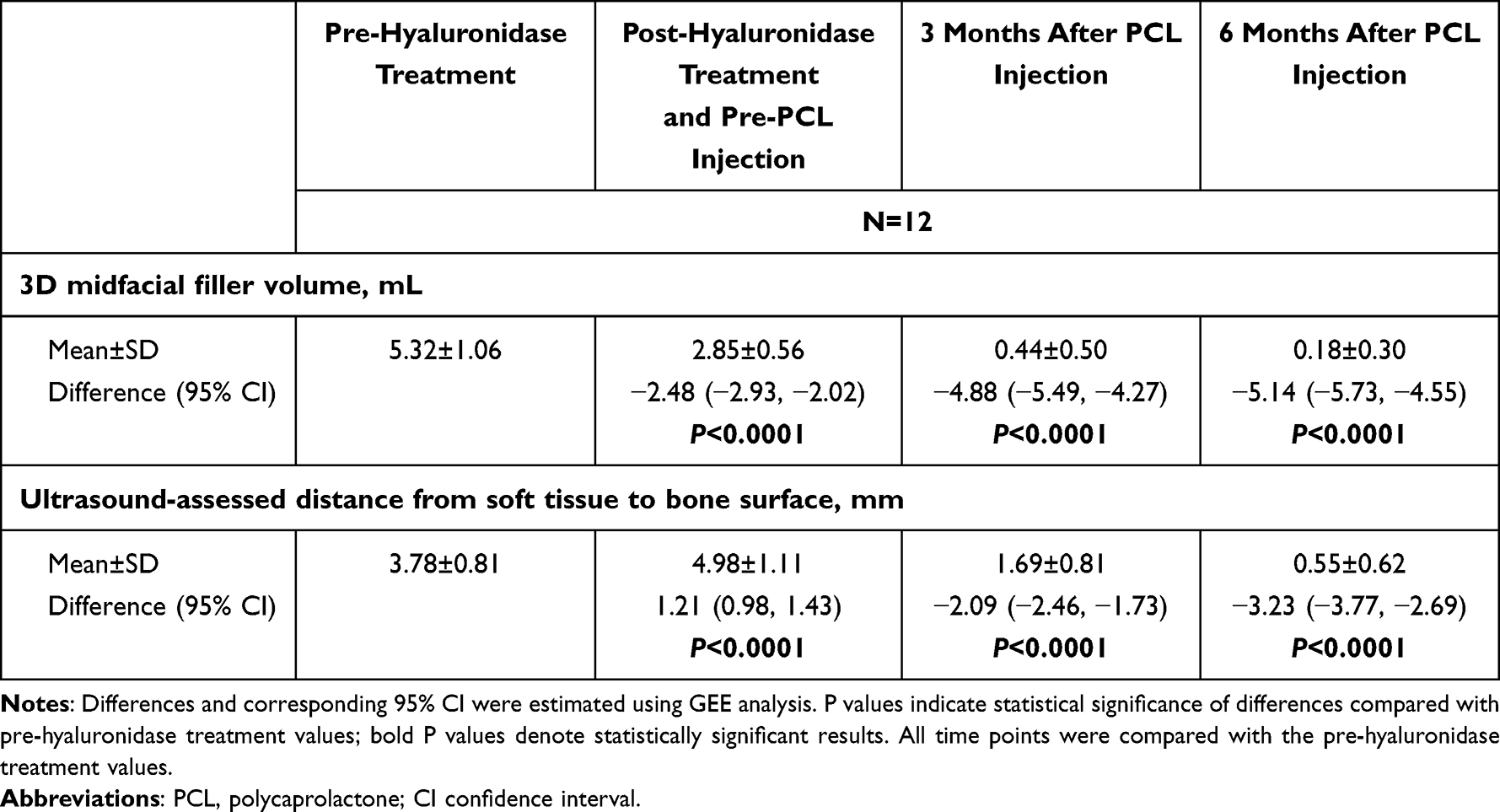 |
Table 3 Effects of Hyaluronidase Treatment and PCL Injection on Midface Correction |
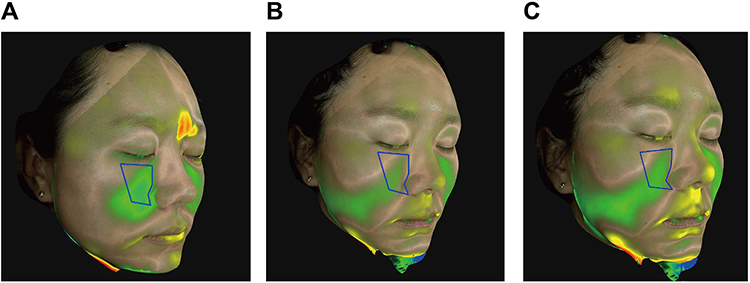 |
Figure 2 Representative 3D topographic images of a 35-year-old female participant showing the anteromedial cheek region. (A) Before PCL injection, (B) 3 months after PCL injection, (C) 6 months after PCL injection. The blue polygon outlines the predefined midfacial region used for volumetric assessment. The superior boundary corresponds to the Frankfurt horizontal plane, the medial boundary to the nasofacial junction, the inferior boundary to the alar base plane, and the lateral boundary to a vertical line extending from the lateral canthus. Green shading indicates regions of volume reduction, whereas yellow and red shading indicate mild and greater volume increases, respectively. Areas showing volume increase outside the defined midfacial region were associated with additional aesthetic treatments unrelated to the present study. |
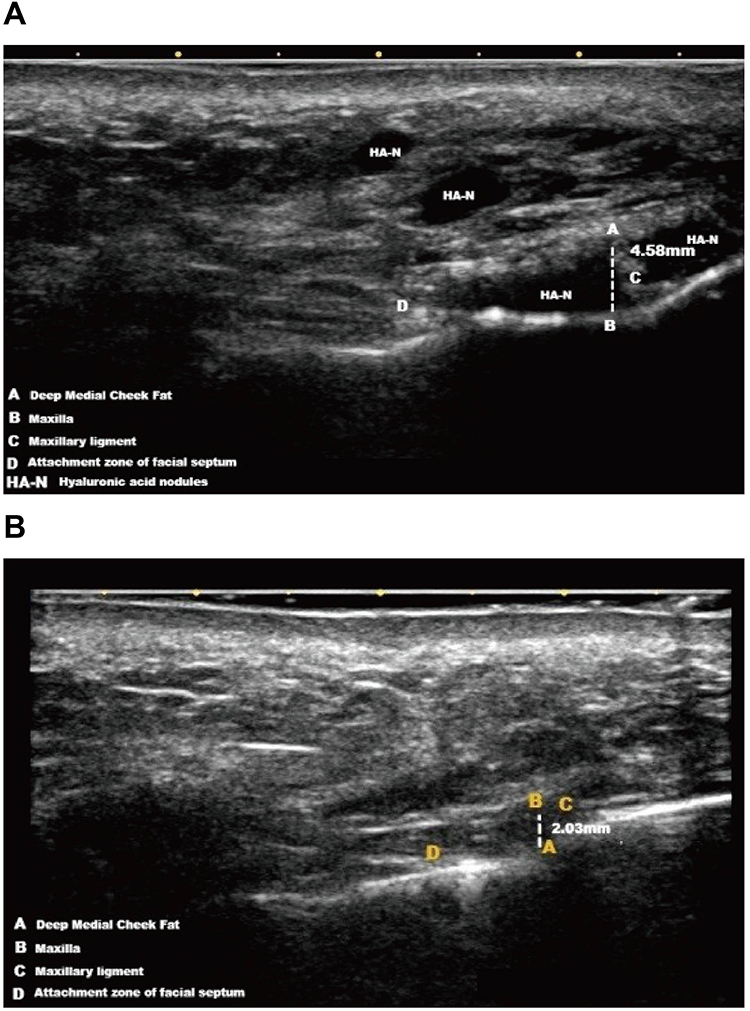 |
Figure 3 Representative ultrasound images. The distance between the deep medial cheek fat (point A) and the maxilla (point B) measured 4.58 mm at baseline (A) and decreased to 2.03 mm at 6 months post-PCL injection (B). |
Safety Outcomes
Throughout the entire treatment course—from hyaluronidase administration to the 6-month follow-up after PCL injection—no adverse events were documented. No cases of local pruritus, allergic reactions, inflammatory reactions, nodules, infection, vascular complications, or other treatment-related sequelae were observed. However, these findings should be interpreted cautiously, as the limited sample size may be insufficient to detect uncommon or delayed complications, and retrospective data collection may underestimate minor adverse events.
Discussion
Hyaluronidase remains the primary therapeutic modality for HA-related FOS, as it can rapidly reduce excessive volume in overfilled regions. Both the present findings and the previous literature suggest that excessive HA filler accumulation may alter facial soft-tissue tension and contour dynamics.4 Consequently, rapid enzymatic dissolution of HA may lead to an abrupt loss of support, resulting in skin laxity, deepened wrinkles, or midfacial descent. In this study, improvements in facial aesthetic appearance and ultrasound-measured tissue parameters were observed following PCL injection after hyaluronidase treatment, suggesting a potential role in reducing post-dissolution hollowing and contour irregularities. Although this exploratory study has limited generalizability, evidence regarding the management of FOS after hyaluronidase treatment remains scarce, and our findings may help address this knowledge gap and provide preliminary guidance for the future development of standardized FOS management strategies.
In subjective assessments, we employed validated aesthetic rating scales commonly used in previous research.23–25 Following hyaluronidase treatment, all patients were rated as “worsened” on GAIS (score 1), indicating that the structural alterations resulting from HA dissolution adversely affected overall aesthetics. In contrast, after PCL injection, improvements in GAIS scores were observed at both 3 and 6 months, suggesting an overall improvement in aesthetic appearance over time. A similar trend was observed in upper cheek fullness: only 41.67% of patients achieved a score of 0 (no overfilling) after hyaluronidase, whereas 100% achieved complete correction after PCL treatment, substantiating PCL’s efficacy in midfacial contour restoration. Temporal hollowing showed an improving trend, but the change did not reach statistical significance. Although this mechanism was not directly evaluated in the present study, we speculate, based on anatomical considerations, that this finding may be influenced by the characteristics of the superficial layer of the deep temporal fascia, a dense inter-fascial plane with limited capacity for true volumetric augmentation. Unlike supraperiosteal injections, which benefit from direct bony support,26,27 this plane primarily acts through fascial tension modulation, which inherently limits its ability to fully correct temporal hollowing.
Objective measurements further supported these clinical findings. 3D volumetric analysis demonstrated that hyaluronidase effectively reduced excessive midfacial filler volume (−2.48 mL). Significantly, PCL did not induce “secondary overfilling”; instead, its biostimulatory properties led to continued volume refinement at 3 and 6 months, reflecting gradual collagen deposition and a shift toward a naturally tightened tissue profile. Based on findings from previous studies, we speculate that this may be related to the temporary nature of the CMC carrier, which provides initial volume but is metabolized within 2–3 months, allowing the subsequent collagen maturation phase to contract and stabilize the soft tissues,16,28,29 thereby potentially contributing to an additive restorative effect in FOS. Conversely, ultrasound imaging showed that the soft tissue–to-bone distance increased significantly immediately after hyaluronidase treatment. Although the underlying mechanism was not directly assessed in this study, this finding may be related to previous observations suggesting that excessive midfacial filler can alter the function of the transverse facial septum (TFS) and compromise soft-tissue support.6,30 In addition, HA filler, being denser than native adipose tissue, may be subject to compressive and shear forces within superficial layers.7 Following hyaluronidase-induced volume reduction, the release of these mechanical influences may contribute to changes in soft tissue position. At 3 and 6 months post-PCL injection, this distance decreased markedly (−2.09 mm and −3.23 mm, respectively), indicating a reduction in the measured soft tissue–to-bone distance over time. These findings suggest that PCL may contribute to structural tissue remodeling rather than merely providing superficial camouflage. Additionally, injections in the midface were not intended to provide volumization but were used in the context of post-hyaluronidase tissue changes. In contrast, injections along the outer facial contours may alter overall facial appearance. These observations may reflect different effects depending on injection location, although the underlying mechanisms cannot be determined from this study.
Beyond the intrinsic biostimulatory properties of PCL, the outer-contour lifting technique used in this study further contributed to midfacial tightening and lifting. Previous research has demonstrated that augmenting certain facial regions can influence adjacent areas, meaning that localized volume enhancement may reposition soft tissues in neighboring zones.31,32 Suwanchinda et al33 reported that subdermal injections in the posterior–superior temporal region can induce repositioning of the midface and lower-face soft tissues. The layered fascial architecture and the retinacula cutis serve as conduits that transmit the local (temporal) volumizing effect into a pan-facial lifting response. Similarly, studies by Claudia et al34 showed that temporal volumization can reduce midfacial volume and enhance jawline contouring, likely by cranially repositioning lateral facial soft tissues. In addition to the temporal region, the preauricular area has recently gained attention as an injection site for fillers, particularly for creating a more angular and defined lateral facial contour.35 In Asian patients—who typically present with high, full zygomatic bones but a retruded medial maxilla36—midfacial rejuvenation focuses on enhancing medial cheek projection rather than widening the malar area. Augmenting the medial cheek shifts the upper-cheek light-reflection point inward, producing the visual impression of a smaller and narrower midface. When volume deficiency and shadowing in the temporal and preauricular regions are corrected, and the midline facial structures receive adequate support, this “visual narrowing” effect becomes further amplified.37 Therefore, in addition to the temporal region, our study primarily used PCL injections in the preauricular area to achieve midfacial elevation and enhance 3D form through outer-contour support.
This study provides the preliminary clinical evidence supporting the use of PCL as a tightening strategy following hyaluronidase treatment; however, several limitations should be acknowledged. First, this retrospective study relied on photographic assessment, which may introduce potential selection bias and limit causal inference. The observed improvement may be partially attributable to the spontaneous resolution of overfilling over time. Therefore, prospective controlled studies are needed to more clearly establish the treatment effect. In addition, as this was an exploratory study conducted in a clinical setting with limited prior evidence, certain treatment decisions, including injection sites and volumes, were individualized based on the degree of volume loss, physician assessment, and anatomical considerations. Second, the small sample size (N=12) reduces statistical power and may have prevented specific trends from reaching significance. Third, as a single-center study involving a relatively homogeneous patient population, the generalizability of the findings may be limited. Future investigations with larger sample sizes and multi-center participation are necessary to more robustly validate the efficacy and safety of this approach. From a procedural standpoint, although injection points and planes followed consistent anatomical principles, real-world clinical practice makes it difficult to entirely eliminate operator-dependent variability (eg, needle angle, speed, or tension assessment), which may subtly influence lifting outcomes or collagen responses. In addition, although ultrasound measurements were performed by multiple investigators and averaged to improve consistency, measurement variability cannot be completely excluded. Lastly, the 6-month follow-up reflects only mid-term performance. Given PCL’s sustained collagen-stimulating properties,17,38 longer follow-up periods (12–24 months) are required to validate its long-term stability and durability.
Conclusion
This preliminary study evaluated the use of PCL following hyaluronidase treatment in patients with FOS using both subjective and objective outcome measures. We observed improvements in aesthetic appearance and reductions in ultrasound-measured soft tissue–to-bone distance following PCL treatment after hyaluronidase administration. Although these findings are exploratory and hypothesis-generating, they may provide preliminary insight into post-hyaluronidase management in FOS. Larger prospective controlled studies are needed to further validate these observations.
Abbreviations
FOS, facial overfilled syndrome; HA, hyaluronic acid; PCL, polycaprolactone; GAIS, Global Aesthetic Improvement Scale; 3D, three-dimensional; CMC, carboxymethyl cellulose; GEE, generalized estimating equations; TFS, transverse facial septum.
Data Sharing Statement
The data supporting this study’s findings are not publicly available due to patient privacy and institutional restrictions. De-identified data may be made available from the corresponding author upon reasonable request and with permission from the relevant ethics committee.
Ethics Approval and Informed Consent
This study was conducted in accordance with the principles of the Declaration of Helsinki and was approved by the Shanghai Ethics Committee for Clinical Research (Approval No.: SECCR2024-181).
Consent for Publication
Written informed consent for publication of clinical images was obtained from the participant. The participant was informed of the manuscript’s content and consented to the publication of the images and associated clinical information.
Author Contributions
All authors made a significant contribution to the work reported, whether in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising, or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This research received no external funding.
Disclosure
The authors declare that they have no competing interests, including any financial or non-financial interests that could have influenced the work reported in this manuscript.
References
1. Kurtti A, Charles C, Jagdeo J, Nguyen J. Combination facial aesthetic treatment in millennials. J Drugs Dermatol. 2022;21(1):37–12. doi:10.36849/JDD.2022.6425
2. Fabi S, Alexiades M, Chatrath V, et al. Facial aesthetic priorities and concerns: a physician and patient perception global survey. Aesthet Surg J. 2022;42(4):NP218–NP229. doi:10.1093/asj/sjab358
3. International Society of Aesthetic Plastic Surgery (ISAPS). ISAPS international survey on aesthetic/cosmetic procedures. 2025. Available from: https://www.isaps.org/media/oogpzodr/isaps-global-survey_2024.pdf.
4. Lim T. Facial overfilled syndrome. Dermatol Clin. 2024;42(1):121–128. doi:10.1016/j.det.2023.06.007
5. Wong IKJ, Sydorchuk O, Yi KH. Taurus philtrum: a newly identified phenomenon in overfilled syndrome. Aesthetic Plast Surg. 2025;49(21):6215–6218. doi:10.1007/s00266-025-04951-4
6. Cotofana S, Gotkin RH, Frank K, Lachman N, Schenck TL. Anatomy behind the facial overfilled syndrome: the transverse facial septum. Dermatol Surg. 2020;46(8):e16–e22. doi:10.1097/DSS.0000000000002236
7. Lim TS, Wanitphakdeedecha R, Yi KH. Exploring facial overfilled syndrome from the perspective of anatomy and the mismatched delivery of fillers. J Cosmet Dermatol. 2024;23(6):1964–1968. doi:10.1111/jocd.16244
8. Buhren BA, Schrumpf H, Bolke E, Kammers K, Gerber PA. Standardized in vitro analysis of the degradability of hyaluronic acid fillers by hyaluronidase. Eur J Med Res. 2018;23(1):37. doi:10.1186/s40001-018-0334-9
9. Boey JJJ, Boey JJE, Cao T, Ng ZY. Conventional high-dose vs low-dose hyaluronidase for skin necrosis after hyaluronic acid fillers: a systematic review and pilot meta-analysis. Aesthetic Plast Surg. 2024;48(19):3971–3978. doi:10.1007/s00266-024-04334-1
10. Michon A, Hassan H. Is more better? Benefits of hyaluronic acid soft tissue filler on the psychological- and social-related quality of life dimensions. Aesthet Surg J Open Forum. 2022;4:ojac086. doi:10.1093/asjof/ojac086
11. Murray G, Convery C, Walker L, Davies E. Guideline for the safe use of hyaluronidase in aesthetic medicine, including modified high-dose protocol. J Clin Aesthet Dermatol. 2021;14(8):E69–E75.
12. Master M, Roberts S. Long-term MRI follow-up of hyaluronic acid dermal filler. Plast Reconstr Surg Glob Open. 2022;10(4):e4252. doi:10.1097/GOX.0000000000004252
13. Wu GT, Kam J, Bloom JD. Hyaluronic acid basics and rheology. Facial Plast Surg Clin North Am. 2022;30(3):301–308. doi:10.1016/j.fsc.2022.03.004
14. Jung H. Hyaluronidase: an overview of its properties, applications, and side effects. Arch Plast Surg. 2020;47(4):297–300. doi:10.5999/aps.2020.00752
15. Haddad S, Galadari H, Patil A, Goldust M, Al Salam S, Guida S. Evaluation of the biostimulatory effects and the level of neocollagenesis of dermal fillers: a review. Int J Dermatol. 2022;61(10):1284–1288. doi:10.1111/ijd.16229
16. Christen MO, Vercesi F. Polycaprolactone: how a well-known and futuristic polymer has become an innovative collagen-stimulator in esthetics. Clin Cosmet Invest Dermatol. 2020;13:31–48. doi:10.2147/CCID.S229054
17. Bae B, Lee G, Oh S, Hong K. Safety and long-term efficacy of forehead contouring with a polycaprolactone-based dermal filler. Dermatol Surg. 2016;42(11):1256–1260. doi:10.1097/DSS.0000000000000913
18. Angelo-Khattar M. Objective assessment of the long-term volumizing action of a polycaprolactone-based filler. Clin Cosmet Invest Dermatol. 2022;15:2895–2901. doi:10.2147/CCID.S385202
19. Chen Q, Wang Y. Ellanse: advanced technology and advantageous selection of new collagen stimulating agents for face rejuvenation. Aesthetic Plast Surg. 2024;48(10):1977–1984. doi:10.1007/s00266-023-03761-w
20. Zhao H, Ren R, Bao S, et al. Efficacy and safety of polycaprolactone in treating nasolabial folds: a prospective, multicenter, and randomized controlled trial. Facial Plast Surg. 2023;39(3):300–306. doi:10.1055/a-1954-3986
21. Lin SL. Polycaprolactone facial volume restoration of a 46-year-old Asian women: a case report. J Cosmet Dermatol. 2018;17(3):328–332. doi:10.1111/jocd.12482
22. Few J, Cox SE, Paradkar-Mitragotri D, Murphy DK. A multicenter, single-blind randomized, controlled study of a volumizing hyaluronic acid filler for midface volume deficit: patient-reported outcomes at 2 years. Aesthet Surg J. 2015;35(5):589–599. doi:10.1093/asj/sjv050
23. Carruthers A, Carruthers J. A validated facial grading scale: the future of facial ageing measurement tools? J Cosmet Laser Ther. 2010;12(5):235–241. doi:10.3109/14764172.2010.514920
24. Carruthers J, Jones D, Hardas B, et al. Development and validation of a photonumeric scale for evaluation of volume deficit of the temple. Dermatol Surg. 2016;42 Suppl 1(Suppl 1):S203–S210. doi:10.1097/DSS.0000000000000848
25. Carruthers J, Flynn TC, Geister TL, et al. Validated assessment scales for the mid face. Dermatol Surg. 2012;38(2 Spec No):320–332. doi:10.1111/j.1524-4725.2011.02251.x
26. Casabona G, Frank K, Moellhoff N, et al. Full-face effects of temporal volumizing and temporal lifting techniques. J Cosmet Dermatol. 2020;19(11):2830–2837. doi:10.1111/jocd.13728
27. Cotofana S, Lachman N. Anatomy of the facial fat compartments and their relevance in aesthetic surgery. J Dtsch Dermatol Ges. 2019;17(4):399–413. doi:10.1111/ddg.13737
28. Woodruff MA, Hutmacher DW. The return of a forgotten polymer—polycaprolactone in the 21st century. Prog Polym Sci. 2010;35(10):1217–1256. doi:10.1016/j.progpolymsci.2010.04.002
29. Kim JS. Changes in dermal thickness in biopsy study of histologic findings after a single injection of polycaprolactone-based filler into the dermis. Aesthet Surg J. 2019;39(12):NP484–NP494. doi:10.1093/asj/sjz050
30. Schelke L, Harris S, Cartier H, et al. Treating facial overfilled syndrome with impaired facial expression-Presenting clinical experience with ultrasound imaging. J Cosmet Dermatol. 2023;22(12):3252–3260. doi:10.1111/jocd.16013
31. Casabona G, Bernardini FP, Skippen B, et al. How to best utilize the line of ligaments and the surface volume coefficient in facial soft tissue filler injections. J Cosmet Dermatol. 2020;19(2):303–311. doi:10.1111/jocd.13245
32. Casabona G, Frank K, Koban KC, et al. Lifting vs volumizing-The difference in facial minimally invasive procedures when respecting the line of ligaments. J Cosmet Dermatol. 2019;18(5):1237–1243. doi:10.1111/jocd.13089
33. Suwanchinda A, Webb KL, Rudolph C, et al. The posterior temporal supraSMAS minimally invasive lifting technique using soft-tissue fillers. J Cosmet Dermatol. 2018;17(4):617–624. doi:10.1111/jocd.12722
34. Hernandez CA, Freytag DL, Gold MH, et al. Clinical validation of the temporal lifting technique using soft tissue fillers. J Cosmet Dermatol. 2020;19(10):2529–2535. doi:10.1111/jocd.13621
35. Vasconcelos-Berg R, Desyatnikova S, Bonavia P, Chammas MC, Navarini A, Sigrist R. Best practices for the use of high-frequency ultrasound to guide aesthetic filler injections-part 2: middle third of the face, nose, and tear troughs. Diagnostics. 2024;14(22):2544. doi:10.3390/diagnostics14222544
36. Wu WT, Liew S, Chan HH, et al. Consensus on current injectable treatment strategies in the Asian face. Aesthetic Plast Surg. 2016;40(2):202–214. doi:10.1007/s00266-016-0608-y
37. Ho WWS. Achieving the attractive Asian midface profile with hyaluronic acid-based fillers. Dermatol Clin. 2024;42(1):113–120. doi:10.1016/j.det.2023.06.013
38. Moers-Carpi MM, Sherwood S. Polycaprolactone for the correction of nasolabial folds: a 24-month, prospective, randomized, controlled clinical trial. Dermatol Surg. 2013;39(3 Pt 1):457–463. doi:10.1111/dsu.12054
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Elucidations on the Performance and Reversibility of Treatment with Hyaluronic Acid Based Dermal Fillers: In vivo and in vitro Approaches
Scrima M, Merola F, Vito N, Pacchioni D, Vecchi G, Melito C, Iorio A, Giori AM, Ferravante A
Clinical, Cosmetic and Investigational Dermatology 2022, 15:2629-2640
Published Date: 8 December 2022
A Review: Causes, Consequences, and Management Strategies of Facial Overfilling

Peng CX, Xv W, Ao YJ
Clinical, Cosmetic and Investigational Dermatology 2025, 18:1857-1864
Published Date: 4 August 2025