Back to Journals » Clinical Ophthalmology » Volume 14
A Preliminary Comparative Study of Visual Performance Between Two Newly Commercially Available Monofocal Intraocular Lenses Implanted During Cataract Surgery
Authors Scorcia V ![]() , Soda M, Lucisano A
, Soda M, Lucisano A ![]() , Lanza M
, Lanza M ![]() , Giannaccare G
, Giannaccare G ![]()
Received 17 January 2020
Accepted for publication 27 February 2020
Published 16 March 2020 Volume 2020:14 Pages 831—835
DOI https://doi.org/10.2147/OPTH.S246319
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Vincenzo Scorcia,1 Mauro Soda,1 Andrea Lucisano,1 Michele Lanza,2 Giuseppe Giannaccare1
1Department of Ophthalmology, University Magna Græcia, Catanzaro, Italy; 2Multidisciplinary Department of Medical, Surgical and Dental Specialities, Università della Campania “Luigi Vanvitelli”, Naples, Italy
Correspondence: Vincenzo Scorcia
Department of Ophthalmology, University Magna Græcia, Viale Europa, Germaneto, Catanzaro 88100, Italy
Tel +39 3334800929
Fax +39 09613647094
Email [email protected]
Purpose: To compare visual outcomes of two newly developed monofocal intraocular lenses (IOLs) (I-Stream H and CT Lucia 211P) implanted in patients undergoing surgery for senile cataract.
Methods: This prospective, comparative, single-center, randomized study included 94 eyes of 94 patients undergoing cataract surgery. Patients were randomized to receive the implantation of I-Stream H IOL (Group 1) or CT Lucia 211P IOL (Group 2). Each patient underwent a complete ocular examination before (V0), 1 month (V1), 3 months (V2) and 6 months (V3) after surgery, including visual acuity testing, objective refraction, slit-lamp biomicroscopy, contrast sensitivity testing and visual function index questionnaire (VF-14).
Results: After surgery, a significant increase of best-corrected visual acuity (BCVA), CS and VF-14 and a significant decrease of SE were detected in both groups at each time point compared to baseline (always p< 0.01). No significant differences in the postoperative increase of BCVA (p=0.12), CS (p=0.21) and VF-14 (p=0.31) and decrease of SE (p=0.08) were detected comparing patients from Group 1 and Group 2 at V3. Mean and median prediction error, as well as absolute prediction error values, did not significantly differ between the two groups (p> 0.05). Eyes with an actual refraction within 0.25, 0.50 and 1 D were 53.1%, 85.1% and 100% for Group 1 and 55.3%, 87.2% and 100% for Group 2 (p> 0.05).
Conclusion: I-Stream H and CT Lucia 211P allowed a satisfied recovery of visual function after senile cataract surgery; both IOLs were shown to have similar outcomes of visual performance.
Keywords: intraocular lens, IOL, I-Stream H, CT Lucia 211P, cataract surgery
Introduction
Senile cataract is a progressive opacification of the crystalline lens occurring in the elderly and determining a significant decrease of vision.1 Nowadays, surgery is able to restore vision and improve quality of life. Significant advances have been developed in the last years in this field with the development of new phacoemulsification devices and intraocular lenses (IOLs) aiming at improving outcomes while reducing intra- and post-operative complications.2
With modern cataract surgery, the aim of IOL implantation is not only to reach the post-operative planus target but also to decrease spherical aberration and ultraviolet retinal toxicity and to improve contrast sensitivity (CS). Factors involved in the IOL selection are mainly related to patient’s characteristics, such as age, expectations, lifestyle, work and hobbies.3
In the European market, monofocal IOLs still represent the most used ones in the current surgical practice, mostly due to their lower cost compared to premium IOLs. Another reason is related to a lower rate of visual disturbances since neuroadaptation is rapid, and patients are almost immediately comfortable with their postoperative vision.4
I-Stream H (MD Tech, Casoria, Italy) and CT Lucia 211P (Carl Zeiss Meditech, Jena Germany) are two newly-commercially monofocal IOLs. The former IOL is hybrid since it consists of both acrylic hydrophilic (Benz IOL 25, Benz Research & Development, Sarasota, FL, USA) and hydrophobic co-polymers. The new polymer of 2-Hydroxyethylmethacrylate and 2-Ethoxyethylmethacrylate was specifically developed for IOL in order to obtain a combination of elasticity and tensile strength that allows the lens to return to its original shape and optical properties in an extremely short time. The lens geometry is aspheric biconvex with a 360° square edge.
The latter IOL is made with ultra-high-purity hydrophobic acrylic material with a heparin-coated surface and the C-loop shape allows easy centering in the capsular bag. The optic design is monofocal spheric.
Since to date, no clinical data are available about the visual performance of both IOLs, the purpose of this study was to compare the visual outcomes of I-Stream H and CT Lucia 211P in the setting of senile cataract surgery.
Methods
Consecutive patients with senile cataract undergoing surgery at the Ophthalmology Unit of University Magna Græcia of Catanzaro (Italy) from January 2018 to January 2019 were enrolled in this comparative, randomized prospective study. The study was performed in accordance with the ethical standards stated in the 1964 Declaration of Helsinki and was approved by the local Ethics Committee (Comitato Etico Regione Calabria Sezione Area Centro). Informed consent was obtained from all subjects before the enrollment in the study.
Inclusion criteria were: good pupil dilatation (at least 6.5 mm), nuclear or cortico-nuclear cataract classified as grade 3 according to the Lens Opacities Classification System III scale and a range of IOL from 5 to 30 diopters (D).5 Exclusion criteria were: any ocular disease other than senile cataract potentially limiting post-operative full visual acuity, keratometric astigmatism >1.25 D and use of any type of ocular medications. Each patient underwent a complete ocular examination before (V0) and 1 month (V1), 3 months (V2) and 6 months (V3) after surgery, including the following procedure: visual acuity testing (LogMAR); objective refraction (Nidek AR-310, Tokyo, Japan) for the calculation of: actual refraction (spherical equivalent, SE), mean and median prediction error (calculated as the difference between the predicted postoperative refraction and the actual postoperative refraction), absolute prediction error (mean of the absolute values of prediction errors), and proportion of eyes with a actual refraction within 0.25, 0.5 and 1.0 D compared to predicted one; slit-lamp biomicroscopy; CS testing; the administration of visual function index questionnaire (VF-14).
Briefly, CS was measured using a Pelli-Robson Contrast Sensitivity Chart [M,N] (Precision Vision, Woodstock, IL, USA) in photopic conditions (85 cd/m2). This chart is designed to measure CS at low spatial frequencies and is known to be very reliable. Testing distance was 1 m with the patient’s best optical correction for this distance.6,7 The subject’s score was the logarithmic CS corresponding to the last triplet in which at least 2 out of 3 letters were correctly identified. The VF-14 is a questionnaire specifically designed to measure functional impairment due to cataract consisting of 18 questions covering 14 aspects of visual function. The questionnaire shows high internal consistency and is a reliable, valid instrument providing information not conveyed by visual acuity or general health status measures.8,9
IOL power and predicted postoperative refraction were calculated by using the Barrett Universal II formula preinstalled on the IOL-Master 700 (Software version 1.8, Carl Zeiss Meditech, Jena Germany). Company-labeled A-constant was 118.7 and 119.8 for I-Stream H and Lucia 221P, respectively.
Eyes of patients included in the study were randomly selected to be implanted with I-Stream H IOL (Group 1) or CT Lucia 211P one (Group 2). Surgical procedures were performed by one experienced high-volume surgeon (V.S.) using the same phacoemulsification device (Stellaris, Bausch&Lomb, Rochester, NY, USA) and the phaco-chop technique. IOL insertion was done using a standard injector through a clear corneal superior incision (2.5 mm).
Statistical analysis was run using SPSS software version 19.0 (SPSS Inc., Chicago, Illinois, USA). Continuous variables were examined for normal distribution using the Kolmogorov–Smirnov test. Analysis of changes in parametric variables before and after surgery in the same groups was performed using Student t test. Comparison of parametric variables of both groups was performed with nonparametric Mann–Whitney test. One-way ANOVA with Bonferroni post-hoc test and Cochran’s Q test were used to compare the two groups. A p value ≤0.05 was considered statistically significant.
Results
Overall, 94 patients (94 eyes) were included in the study: of these, 47 patients (22 M and 25 F; mean age 74.94 ± 7.68 years [range from 50 to 88 years]) were randomized to Group 1, while the remaining 47 (24 M and 23 F; mean age 72.89 ± 8.86 years [range from 50 to 95 years]) were randomized to Group 2. Demographic and clinical data of both groups are summarized in Table 1.
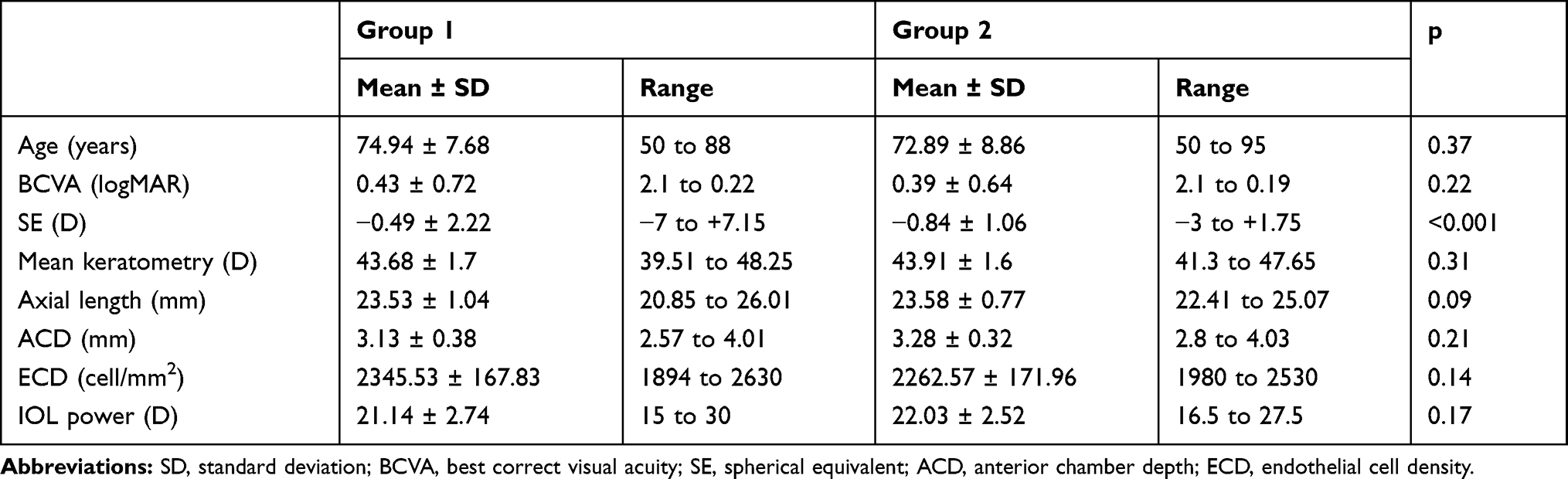 |
Table 1 Clinical Characteristics of Patients at Baseline and Surgical Parameters |
After surgery, a significant increase of BCVA (Group 1: 0.43±0.72 LogMAR at V0 vs 0.10±0.62 at V3; Group 2: 0.39±0.64 at V0 vs 0.15±0.62 at V3), CS (Group 1: 1.08±0.23 at V0 vs 1.56±0.33 at V3; Group 2: 1.12±0.35 at V0 vs 1.53±0.41 at V3) and VF-14 (Group 1: 83.31±1.02 at V0 vs 94.51±1.97 at V3; Group 2: 81.54±2.78 at V0 vs 93.29±2.08 at V3) and a significant decrease of SE (Group 1: −0.49±2.22 D at V0 vs −0.31±0.71 at V3; Group 2: −0.84±1.06 at V0 vs −0.44±0.54 at V3) were detected in both groups at each time point compared to baseline (always p<0.01). No significant differences in the post-operative increase of BCVA (p=0.12), CS (p=0.21) and VF-14 (p=0.31) and decrease of SE (p=0.08) were detected comparing patients from Group 1 and Group 2 at V3 (Table 2). Mean and median prediction error values were, respectively, 0.3±0.6 D and −0.4 for Group 1 and 0.2±0.5 and −0.3 for Group 2 (p>0.05). Similarly, absolute prediction error was 0.6±0.5 and 0.5 for Group 1 and 0.7±0.5 and 0.6 for Group 2 (p>0.05). Eyes with an actual refraction within 0.25, 0.50 and 1.00 D were 53.1%, 85.1% and 100%, respectively, in Group 1; in Group 2 percentage was 55.3%, 87.2% and 100%, respectively. No significant difference was recorded between the two groups (p>0.05). During the entire follow-up period, none of the following complications (intraocular pressure spikes, IOL tilting or dislocation, posterior capsule opacification, long-lasting corneal edema, inflammatory or infective events) have been recorded in both groups.
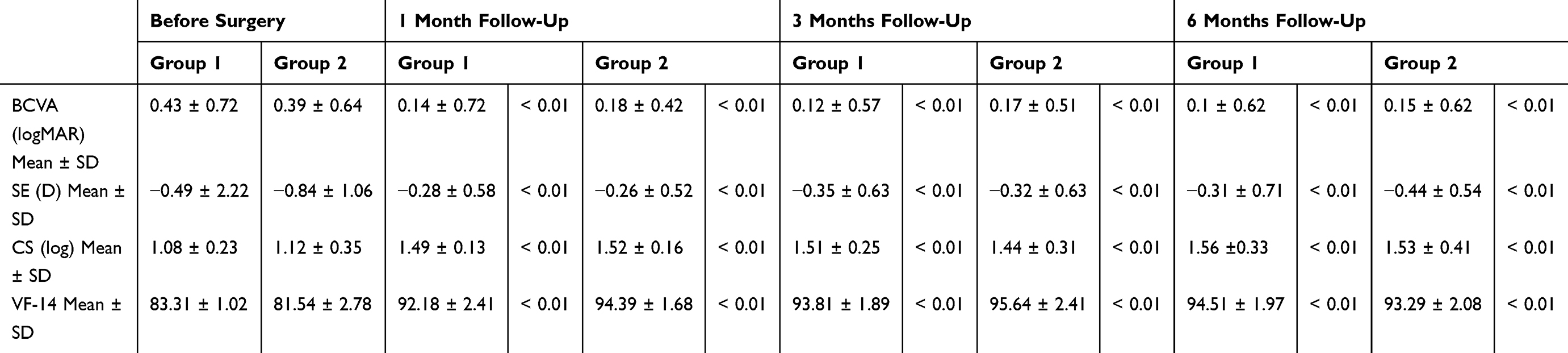 |
Table 2 Changes of Best Correct Visual Acuity (BCVA), Refraction Measured as Spherical Equivalent (SE), Contrast Sensitivity (CS) Measured with Pelli-Robson Chart and Visual Function Index (VF-14) Score Before and at 1, 3 and 6 Months Follow Up in Group 1 and Group 2 Eyes. Statistical Test Have Been Performed Using Student t Test for Paired Data |
Discussion
Visual impairment due to cataract still remains the leading cause of blindness in middle- and low-income countries, accounting for half cases of blindness.10–12 On the contrary, in developed countries where cataract surgery is the most performed surgical procedure, this type of visual impairment is responsible for only 5% of blindness cases.13,14
The choice of the type of IOL implanted during cataract surgery depends upon patient’s characteristics and expectations, surgeon preferences and settings (private Clinic vs Public Hospital). Overall, monofocal IOLs still represent the most implanted ones due to economic issues, good tolerability and poor/null contraindications.4
The present study aimed at comparing the visual performance of two newly-developed monofocal IOLs (I Stream H and CT Lucia 211P) implanted in patients with senile cataract. Visual performance was evaluated in the study through the testing of visual acuity, post-operative actual refraction, prediction error, CS and VF-14, a questionnaire specific for functional impairment secondary to cataract. Overall, all parameters improved significantly 1 month after surgery and this trend was maintained approximately unchanged over the entire study duration. Almost the totality of patients achieved a refractive outcome with half diopter, regardless of the type of IOL implanted. Furthermore, no significant differences in the evaluated parameters were recorded between patients who were implanted with the two different IOLs. When comparing our results with those ones from other studies with other widely used monofocal IOLs, we found comparable values about CS and VF-14.15,16
This preliminary study validates the visual performance of either I-Stream H and CT Lucia 211P, and highlights their good profile of safety. This is a crucial aspect to consider when evaluating a new medical device introduced into the market.
The present study is preliminary and suffers from some limitations, including the small number of patients and the relatively short period of follow-up. However, an implementation of present data with a larger sample size and a longer follow-up is currently ongoing at our Institution to try to provide further evidence in this field.
In conclusion, I-Stream H and CT Lucia 211P allowed a satisfied recovery of visual function after senile cataract surgery with a good profile of safety. In addition, both IOLs were shown to have similar outcomes of visual performance.
Disclosure
The authors report no funding and no conflicts of interest in this work.
References
1. Liu YC, Wilkins M, Kim T, Malyugin B, Mehta JS. Cataracts. Lancet. 2017;390(10094):600–612. doi:10.1016/S0140-6736(17)30544-5
2. Olson RJ. Cataract surgery from 1918 to the present and future-just imagine! Am J Ophthalmol. 2018;185:10–13. doi:10.1016/j.ajo.2017.08.020
3. Wang SY, Stem MS, Oren G, Shtein R, Lichter PR. Patient-centered and visual quality outcomes of premium cataract surgery: a systematic review. Eur J Ophthalmol. 2017;27(4):387–401. doi:10.5301/ejo.5000978
4. de Silva SR, Evans JR, Kirthi V, Ziaei M, Leyland M. Multifocal versus monofocal intraocular lenses after cataract extraction. Cochrane Database Syst Rev. 2016;12:CD003169. doi:10.1002/14651858.CD003169.pub4
5. Chylack LT
6. Elliott DB, Sanderson K, Conkey A. The reliability of the Pelli-Robson contrast sensitivity chart. Ophthalmic Physiol Opt. 1990;10(1):21–24. doi:10.1111/opo.1990.10.issue-1
7. Pelli DG, Robson JG, Wilkins AJ. The design of a new chart for measuring contrast sensitivity. Clin Vis Sci. 1988;2:187–199.
8. Alonso J, Espallargues M, Andersen TF, et al. International applicability of the VF-14. An index of visual function in patients with cataracts. Ophthalmology. 1997;104(5):799–807. doi:10.1016/S0161-6420(97)30230-9
9. Steinberg EP, Tielsch JM, Schein OD, et al. The VF-14, An index of functional impairment in patients with cataract. Arch Ophthalmol. 1994;112:630–638. doi:10.1001/archopht.1994.01090170074026
10. Song P, Wang H, Theodoratou E, Chan KY, Rudan I. The national and subnational prevalence of cataract and cataract blindness in China: a systematic review and meta-analysis. J Glob Health. 2018;8(1):010804. doi:10.7189/jogh.08-010804
11. Batlle JF, Lansingh VC, Silva JC, Eckert KA, Resnikoff S. The cataract situation in Latin America: barriers to cataract surgery. Am J Ophthalmol. 2014;158:242–250. doi:10.1016/j.ajo.2014.04.019
12. Khanna R, Pujari S, Sangwan V. Cataract surgery in developing countries. Curr Opin Ophthalmol. 2011;22:10–14. doi:10.1097/ICU.0b013e3283414f50
13. Lee CM, Afshari NA. The global state of cataract blindness. Curr Opin Ophthalmol. 2017;28(1):98–103. doi:10.1097/ICU.0000000000000340
14. Mundy KM, Nichols E, Lindsey J. Socioeconomic disparities in cataract prevalence, characteristics, and management. Semin Ophthalmol. 2016;31(4):358–363. doi:10.3109/08820538.2016.1154178
15. Lasta M, Mihaltz K, Kovacs I, et al. Effect of spherical aberration on the optical quality after implantation of two different aspherical intraocular lenses. J Ophthalmol. 2017:8039719. doi:10.1155/2017/8039719
16. Tarfah M, Samah M, Ahmed A. Corneal spherical aberration and its impact on choosing an intraocular lens for cataract surgery. Saudi J Ophthalmol. 2014;28:274–280. doi:10.1016/j.sjopt.2014.06.005
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.