Back to Journals » Clinical Optometry » Volume 18
A Predictive Model for Personalized Fitting of Peripheral Defocus Spectacles Based on Ocular Biometric Parameters
Authors Zhou P ![]() , Li Y, Chen S, Wang K, Li Y
, Li Y, Chen S, Wang K, Li Y
Received 25 October 2025
Accepted for publication 13 January 2026
Published 19 January 2026 Volume 2026:18 576749
DOI https://doi.org/10.2147/OPTO.S576749
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Chris Lievens
Peng Zhou,1,2,* Yingli Li,1,3– 6,* Sitong Chen,1,3– 6 Kai Wang,1,3– 6 Yan Li1,3– 6
1Optometry Center, Peking University People’s Hospital, Beijing, 100034, People’s Republic of China; 2Department of Ophthalmology, Parkway Gleneagles Medical and Surgical Center, Shanghai, 200003, People’s Republic of China; 3Department of Ophthalmology, Peking University People’s Hospital, Beijing, 100034, People’s Republic of China; 4Beijing Key Laboratory of Diagnosis and Therapy of Ocular Diseases and Optometry, Beijing, 100034, People’s Republic of China; 5School of Optometry and Ophthalmology, Peking University Health Science Center, Beijing, 100034, People’s Republic of China; 6Institute of Medical Technology, Peking University Health Science Center, Beijing, 100191, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Yan Li, Department of ophthalmology, Peking University People’s Hospital, 11 Xizhimen South Street, Beijing, 100044, People’s Republic of China, Email [email protected] Kai Wang, Department of ophthalmology, Peking University People’s Hospital, 11 Xizhimen South Street, Beijing, 100044, People’s Republic of China, Email [email protected]
Purpose: To construct a predictive model for personalized recommendation of peripheral defocus spectacle designs based on ocular biometric parameters.
Methods: This retrospective cohort study included 2824 myopic children who wore peripheral defocus spectacles at the Ophthalmology Center of Peking University People’s Hospital. Participants were divided into five groups according to the spectacle designs (Diversified Segmental Defocus Optimization [DSDO], Diffusion Optics Technology [DOT], Defocus Induced Multiple Segment [DIMS], Highly Aspherical Lenslets [HALT], Hexagon Optimized Reticular Integration [HORI]) and matched for gender, age, and baseline biometric parameters. The dataset was randomly split into training (80%) and validation (20%) sets for model evaluation. Separate multiple linear regression prediction models based on ocular biometric parameters were constructed for each designs. Finally, an R language function was developed for clinical personalized recommendation.
Results: After matching baseline parameters, no statistically significant difference was observed in axial elongation control efficacy among the five peripheral defocus spectacles designs (P = 0.28). The coefficient of determination (R2) ranged from 0.89 to 0.96 in the training set and from 0.88 to 0.97 in the validation set; the root mean square error (RMSE) ranged from 0.05 mm to 0.07 mm in the training set and from 0.04 mm to 0.07 mm in the validation set. Calibration plots showed good agreement between predicted and observed values.
Conclusion: Although no significant differences in average efficacy were observed among the five designs, this study successfully established predictive models based on ocular biometric parameters to guide personalized fitting of peripheral defocus spectacles.
Plain Language Summary: Defocus glasses have been proven to slow down the progression of myopia, but there is currently no method for selecting the type of defocus lenses on an individual basis. This study proposes a model for personalized selection of defocus lenses based on ocular biometric data. This model will offer guidance in clinical decisions for myopia management strategies.
Keywords: myopia control, defocus spectacle lenses, personalized selection, ocular biometry, predictive model
Corrigendum for this paper has been published.
Background
Myopia is an emerging public health concern worldwide, with its prevalence escalating at an alarming rate, especially in Asia. Projections for 2050 suggest that myopia will affect approximately 50% of the global population, establishing it as the foremost cause of irreversible vision impairment.1 A large-scale study in China, encompassing 5.09 million children and adolescents, highlights the acute severity of myopia among individuals aged 7–18 years.1 Although Europe experiences a lower prevalence than Asia, increasing trends in countries like Germany confirm the pervasive nature of myopia across diverse regions.2 The World Health Organization identifies uncorrected or inadequately corrected myopia as a significant contributor to blindness.3 High myopia, defined as refractive error exceeding −6 diopters, predisposes individuals to irreversible complications, including retinal detachment, glaucoma, and macular degeneration.4–6 The aging demographic is expected to exacerbate the burden of myopia-related complications, such as early-onset cataracts, on healthcare systems. Notably, the most rapid progression of myopia occurs during childhood, underscoring the necessity for early intervention strategies to mitigate its development.7,8
Effective control of pediatric myopia begins with a thorough understanding of its underlying mechanisms. Optical defocus is critical in the etiology of myopia. The retina can discern when an image is focused behind (hyperopic defocus) or in front of (myopic defocus) the eyeball and consequently adjusts axial growth to correct the focus.9 Studies indicate that the retina evaluates the defocus characteristics of natural images, such as contrast distribution, to identify defocus types, influencing scleral remodeling processes.9 Defocus signals may induce scleral thinning and axial elongation by altering the remodeling of the scleral extracellular matrix (ECM), including the reduction of type I collagen synthesis and increased degradation, which could constitute the core pathological process in myopia development.10 This mechanistic insight provides a theoretical foundation for optical interventions designed to control axial growth through the artificial introduction of myopic defocus signals.11
A prevalent optical technology utilized in the intervention of myopia progression is the multi-zone positive defocus strategy, as described in the literature.12 This class of corrective lenses encompasses varieties such as Defocus Incorporated Multiple Segments (DIMS), Diversified Segmental Defocus Optimization (DSDO), and the Asymmetric Multi-point Defocus Technique (AMDT). DIMS lenses achieve positive defocus by integrating multiple microlenses within the peripheral lens zones.11 The DSDO technology, sharing conceptual similarities with DIMS, may augment intervention effectiveness by offering a more adaptable defocus pattern through refined segmented defocus designs.13,14 Meanwhile, the AMDT approach seeks to mitigate myopia progression via an asymmetric multi-point defocus configuration.12 These methodologies are underpinned by the peripheral retinal defocus theory, employing optical design to establish a constant defocus signal anterior to the retina, thereby influencing axial elongation. Clinical studies have demonstrated that these lenses substantially decelerate myopia progression. Meta-analyses report that current peripheral defocus spectacles reduce myopia progression by approximately 30–60% over 1–2 years compared to single-vision lenses.15,16 However, a conclusive and effective approach for the individualized selection of defocus lenses for children remains unavailable.
Our previous investigations have identified a correlation between ocular biometric parameters and the progression of myopia. Specifically, reduced central corneal thickness may serve as a risk factor for advancing myopia in pediatric populations.17 Prior studies indicate that corneal curvature (K) and corneal radius (CR) contribute to myopia development by modulating refractive power. A flatter cornea (characterized by low curvature) is positively linked with axial myopia, whereas a steeper cornea might inhibit myopic progression through compensatory mechanisms.18 Additionally, dynamic alterations in anterior chamber depth (ACD) and lens thickness (LT) are implicated in refractive changes. Myopic children often exhibit a deeper anterior chamber paired with a thinner lens; this particular biometric profile may expedite the advancement of axial myopia.19 Moreover, ocular biometric parameters are integral to the selection of myopia management strategies. These parameters are utilized not only for assessing myopia risk but also for tailoring personalized intervention strategies. Notably, baseline axial length and corneal curvature are critical in determining the suitability of orthokeratology (OK) lenses. A longer axial length and certain corneal features (such as a flatter cornea) may augment the effectiveness of OK lenses in controlling myopia.15,20 Nonetheless, there is a lack of research examining the relationship between ocular biometric parameters and the efficacy of various defocus spectacle lenses for myopia control.
This study investigates the feasibility of utilizing ocular biometric parameters to predict the personalized fitting of defocus spectacle lenses. Initially, we analyzed the correlation between ocular biometric indicators and the efficacy of myopia control across various defocus lens brands. Subsequently, we developed a predictive model for myopia progression based on these biometric parameters. Finally, we examined the application of this model in selecting the most suitable defocus lens.
Materials and Methods
Study Design and Ethical Statement
This retrospective cohort study utilized clinical data from pediatric patients fitted with defocus spectacle lenses at the Ophthalmology and Optometry Center of Peking University People’s Hospital between January 1, 2022, and June 30, 2025. The study protocol received approval from the Ethics Review Committee of Peking University People’s Hospital (Approval No.: 2021PHB322-001). Written informed consent was obtained from a parent or legal guardian of each participant. All procedures conformed to the ethical principles outlined in the Declaration of Helsinki.
Study Subjects and Screening Criteria
The study enrolled myopic children aged 17 years or younger who were prescribed spectacles. Inclusion criteria comprised a spherical equivalent (SE) refraction greater than −1.00 D, use of defocus spectacle lenses, availability of comprehensive clinical data, provision of signed informed consent, and absence of alternative myopia control methods, including but not limited to low-concentration atropine. Exclusion criteria encompassed hereditary ocular diseases, follow-up duration of less than 12 months, concurrent use of other myopia control strategies, including but not limited to low-concentration atropine, or a missing data rate exceeding 20% for critical variables. All five defocus lens designs were available in spherical powers ranging from −0.50 D to −10.00 D, with cylindrical corrections up to −4.00 D, fully covering the refractive prescriptions of all participants in this cohort.
Data Extraction and Variable Definitions
The study extracted the following variables from the electronic medical record system: sex, age at initial spectacle wear (AGEofONSET), spherical power (Sphere), cylindrical power (Cylinder), axis of astigmatism (Axis), flat corneal curvature (K1), steep corneal curvature (K2), corneal astigmatism (AST), pupillary distance (PD), corneal diameter (white-to-white, WTW), axial length (AL), central corneal thickness (CCT), anterior chamber depth (ACD), lens thickness (LT), and vitreous length (VT). The annual axial elongation rate (RateofAL) was defined as the annualized change in axial length over the follow-up period. Data collection was limited to the right eye only for this investigation to avoid inter-eye correlation.
Sample Matching and Grouping
Clinical data were extracted, and subjects were matched based on sex, age, and fundamental ocular biometric parameters, excluding those relevant to axial elongation rate calculation. Participants were categorized into five groups according to the brand of defocus lenses worn: Diversified Segmental Defocus Optimization (DSDO), Diffusion Optics Technology (DOT), Defocus Incorporated Multiple Segments (DIMS), Highly Aspherical Lenslets (HALT), and Hexagon Optimized Reticular Integration (HORI).
Statistical Modeling and Analysis
To assess the predictive efficacy of each defocus lens brand on axial elongation rate, separate multiple linear regression models were developed for the five glasses brands. The response variable was the Rate of Axial Length (RateofAL), with 15 clinical indicators serving as predictor variables. Each group’s data were randomly divided into a training set and a validation set in an 8:2 ratio. The training set was employed to fit the models, and the goodness-of-fit was evaluated using the coefficient of determination (R2) and root mean square error (RMSE). The models were validated with the validation set, and the regression coefficients along with the final equations were documented. Source code is available in Supplementary Material 1.
Model Application and Implementation
For the purpose of clinical personalized recommendations, each model for different brands was preserved in.rds format. An R function titled recommend_brand() was developed. This function accepts the 15 clinical variables of a new patient as input and outputs the predicted axial elongation rate for each lens brand. It subsequently suggests the optimal brand by ranking in ascending order of the predicted rate. Source code is available in Supplementary Material 1.
Statistics
Data analyses were conducted utilizing R software (version 4.3.0), with the significance threshold established at α = 0.05.
Results
Baseline Characteristics of Patients
A cohort of 2824 eligible subjects was included in the analysis, consisting of 1551 males and 1273 females. Participants were stratified into five groups according to the brand of prescribed spectacle lenses: DSDO (n = 632), DOT (n = 596), DIMS (n = 551), HORI (n = 538), and HALT (n = 507). The average age at myopia onset was 8.90 ± 2.45 years, with a range from 2.04 to 16.47 years and a mode of 7.47 years. The median follow-up duration was 18.3 months (interquartile range: 12.1–30.7 months), supporting the reliability of annualized axial elongation rates. Post hoc power analysis indicated >99% power to detect a clinically meaningful difference of 0.05 mm/year in axial elongation across groups (α = 0.05). Comprehensive characteristics of each group are detailed in Table 1.
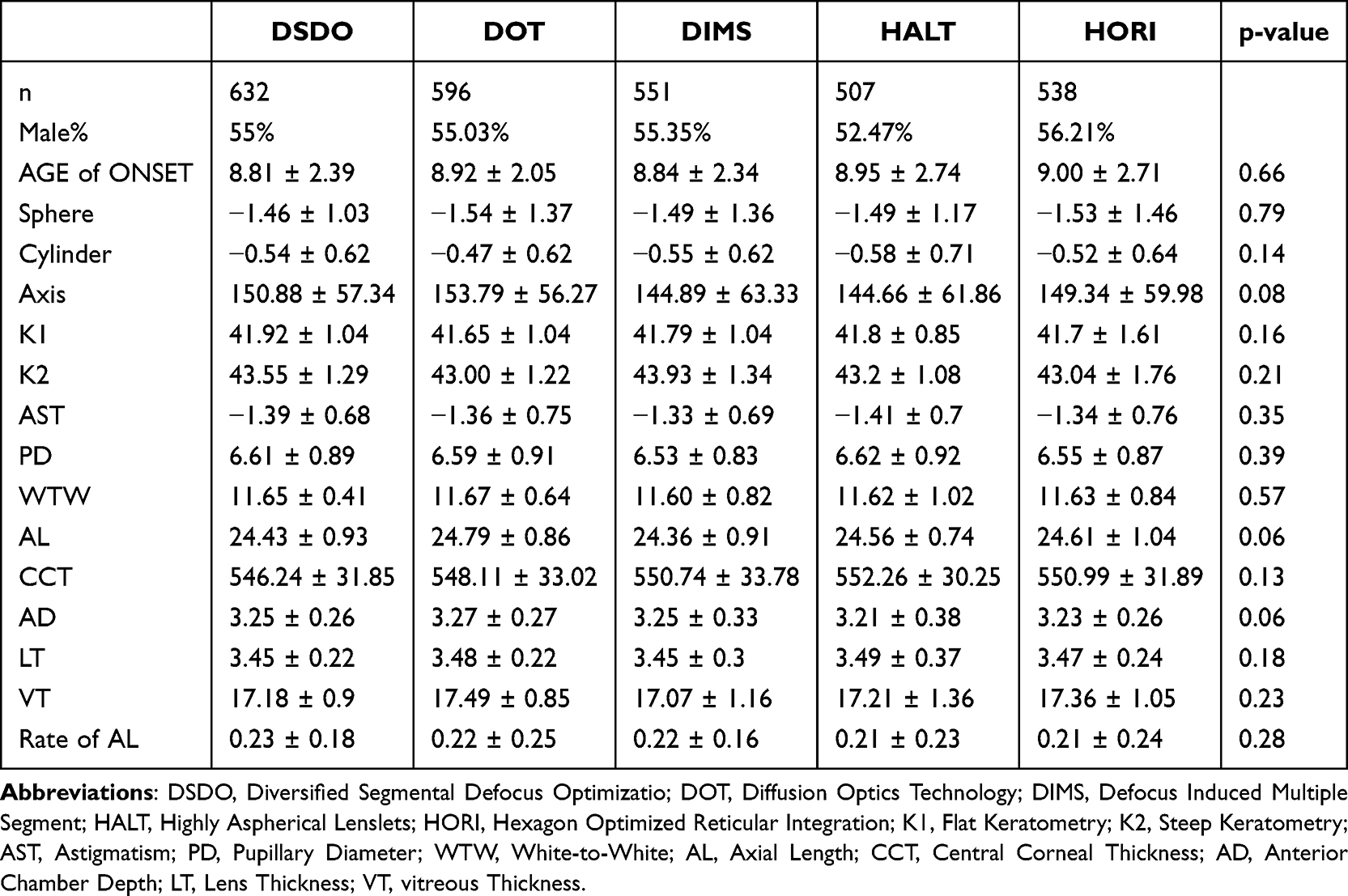 |
Table 1 Comparison of Five Peripheral Defocus Spectacle Designs |
Comparison of Five Defocus Spectacle Lenses
The study aimed to construct a personalized prediction model for selecting defocus spectacle lenses based on specific ocular biometric parameters. For this purpose, data were adjusted for sex, age, and baseline ocular biometric parameters, excluding axial length growth velocity from the matching criteria. Post-adjustment, the average axial elongation rate varied between 0.21 mm/year and 0.23 mm/year among the five defocus lens groups. Statistical analysis revealed no significant differences in myopia progression control across the various lens types (F = 1.28, P = 0.28; Table 1, Figure 1).
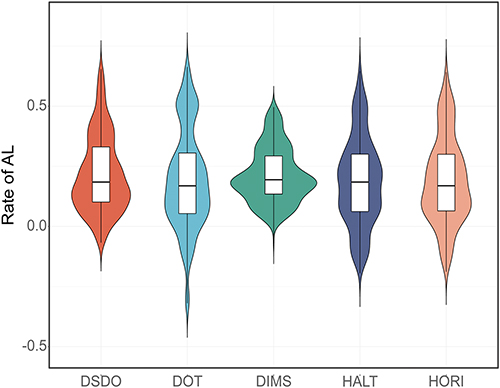 |
Figure 1 Violin plots illustrating the efficacy of various peripheral defocus spectacle designs in controlling axial elongation. No statistically significant differences were observed among the five designs after matching for gender, age, and baseline biometric parameters (P = 0.28). Abbreviations: DSDO, Diversified Segmental Defocus Optimization; DOT, Diffusion Optics Technology; DIMS, Defocus Induced Multiple Segment; HALT, Highly Aspherical Lenslets; HORI, Hexagon Optimized Reticular Integration; AL, axial length. |
Construction and Validation of Models
For each of the five lenses (DSDO, DOT, DIMS, HORI, and HALT), distinct multiple linear regression models were developed. These models exhibited robust fitting across both the training and validation datasets (refer to Figure 2A). The coefficient of determination (R2) served as the metric for evaluating model fit, with values approaching 1 denoting enhanced explanatory power and superior fit of the models to the data. Specifically, for the defocus lens models, R2 values spanned from 0.89 to 0.96 in the training datasets and from 0.88 to 0.97 in the validation datasets (Table 2). To assess the level of prediction error, the Root Mean Square Error (RMSE) was calculated, representing the mean deviation between predicted and actual observed values. The RMSE values ranged from 0.05 mm to 0.07 mm in the training datasets, and from 0.04 mm to 0.07 mm in the validation datasets (Table 2). Calibration plots, depicting the relationship between observed and predicted axial elongation rates, indicated strong concordance (see Figure 2B). The regression equations for estimating the annual rate of axial elongation are delineated in Table 2.
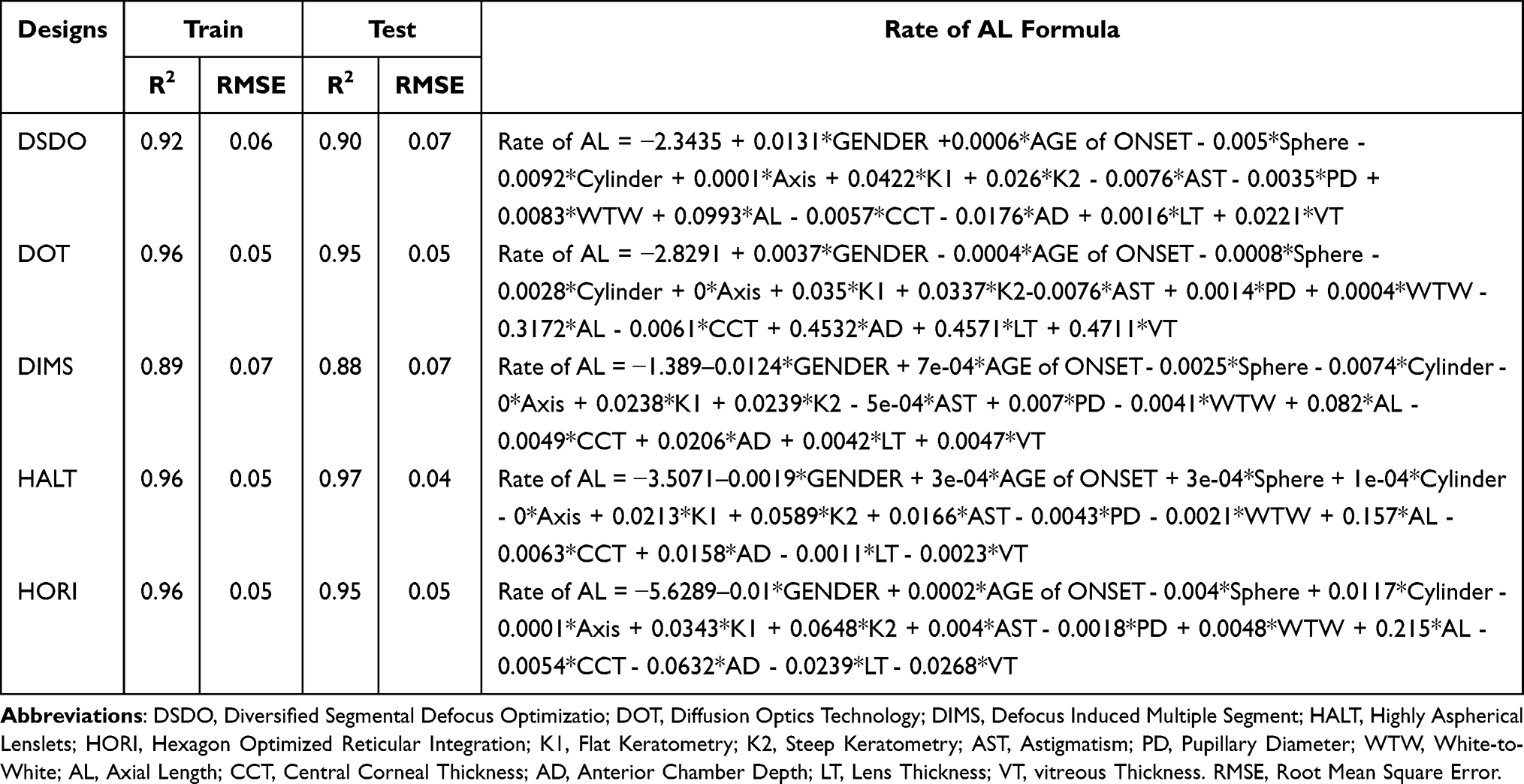 |
Table 2 Models to Predict the Axial Elongation Rate for Personalized Fitting of Peripheral Defocus Spectacles |
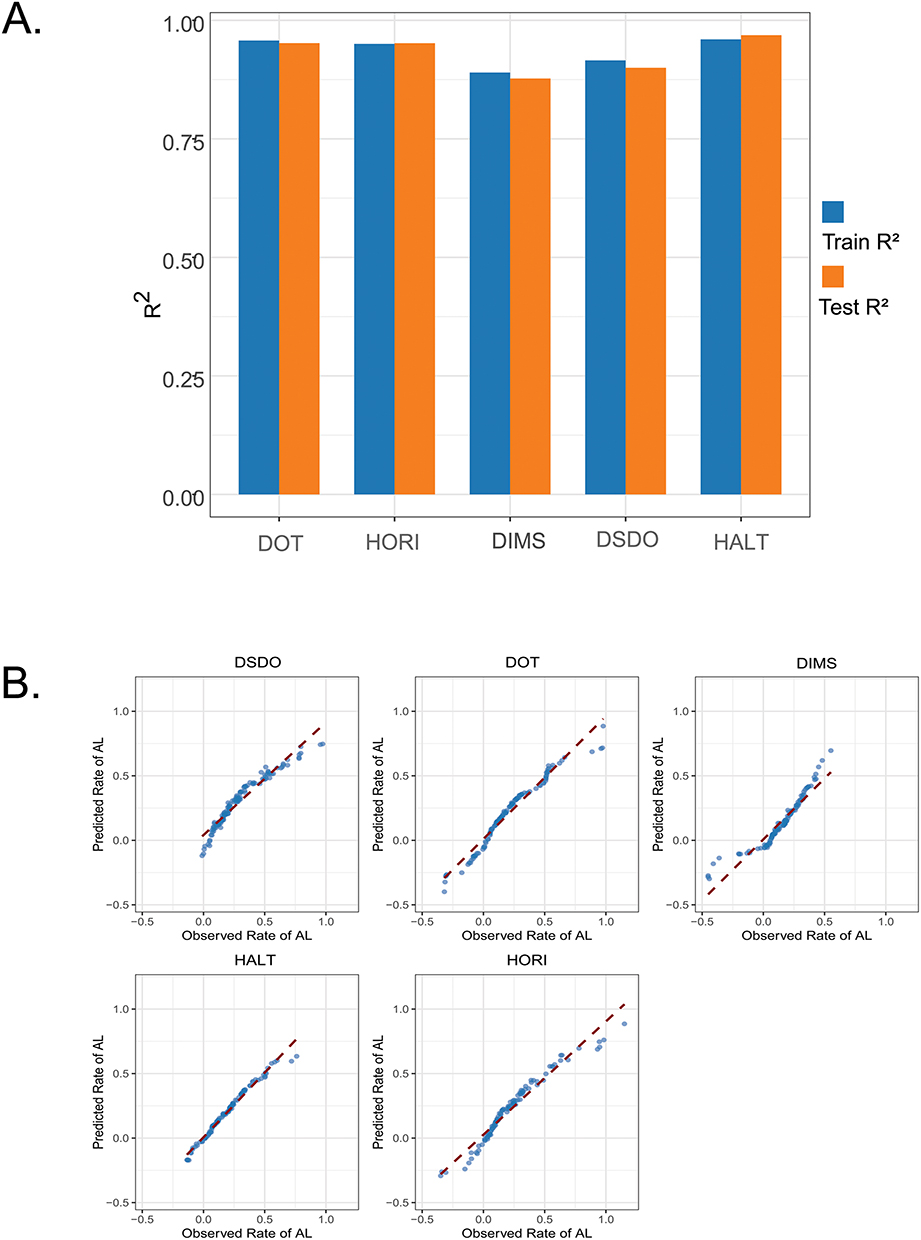 |
Figure 2 Model Performance Evaluation. The prediction models for each spectacle design demonstrated excellent goodness-of-fit and predictive accuracy. (A) High R2 values (Training: 0.89–0.96; Validation: 0.88–0.97) and low RMSE values (Training: 0.05–0.07 mm; Validation: 0.04–0.07 mm) were observed across all models. (B) Calibration plots showed strong agreement between the predicted and observed values. |
Discussion
This study identified no statistically significant differences in the efficacy of the five defocus spectacle lenses (DSDO, DOT, DIMS, HORI, and HALT) after controlling for sex, age, and baseline ocular biometric parameters. Additionally, predictive models for myopia progression were developed for each lens type using these biometric parameters, offering a basis for personalized selection of defocus spectacle lenses.
Ocular biometric parameters were selected for predictive purposes due to their practical advantages and clinical relevance in myopia management. While genetic sequencing could theoretically facilitate personalized defocus lens fitting—analogous to its application in forecasting Orthokeratology success—this method entails substantial costs associated with genetic testing. Genotypic characteristics manifest through phenotypic traits, with ocular biometric parameters, such as corneal thickness and pupil diameter, serving as key phenotypic indicators in myopia research. In our clinical practice, we routinely employ the IOLmaster for axial length measurements among pediatric patients to track myopia progression. This procedure also yields other ocular biometric data concurrently, furnishing a comprehensive dataset. Consequently, we explored the feasibility of leveraging these accessible biometric indicators to forecast outcomes in the customization of defocus lenses.
Our previous investigations have established ocular biometry as a reliable tool for predicting the onset and progression risk of myopia. Notably, reduced central corneal thickness (CCT) has emerged as a potential risk factor for accelerated myopic progression in children, with adolescents presenting thinner corneas exhibiting a higher progression rate.17 Recent advances include the development of a predictive nomogram incorporating age, female sex, and ocular biometric parameters to estimate myopia risk.21 Additionally, biometric characteristics such as anterior chamber depth (ACD), axial length (AL), and CCT have been identified as significant predictors of myopia.22 These findings collectively underscore the utility of ocular biometric measurements in risk assessment strategies, offering support for their application in personalizing defocus lens prescriptions to address myopia progression effectively.
The significant outcome of this study is the development of formulas that predict the effects of various defocusing lenses based on ocular biometry.In this investigation, we constructed and validated personalized multiple linear regression models aimed at predicting defocus lens selection. These models exhibited favorable performance metrics, including the coefficient of determination (R2) which signifies the model fit, and the root mean square error (RMSE), representing the average prediction error. Upon inputting precise ocular biometric parameters, the models can accurately forecast the axial elongation rate associated with a specific defocus spectacle lens.
Several noteworthy findings were identified. Firstly, the DSDO lens design resembles an astigmatic chart.12 The model coefficient for astigmatism in the DSDO group was negative and relatively larger in magnitude, suggesting a potential association between higher baseline astigmatism and reduced axial elongation—a pattern that warrants formal testing in future prospective trials. The DOT lens functions predominantly on the peripheral defocus principle, theoretically minimizing the impact of unfocused peripheral light on the retina.23–25 Its enhanced performance in children with smaller pupils may be due to reduced peripheral light entry. In contrast, the HALT lens, which utilizes a concentric ring-based defocus design,16 showed improved outcomes in children with larger pupils, potentially because these pupils allow more utilization of the defocused signal.
This study is limited by its retrospective design. To develop more reliable models for defocus lens selection, future research should focus on prospective clinical trials that expand on these results. Furthermore, while our models demonstrate promising internal consistency and biological plausibility, they require prospective external validation in geographically and demographically distinct populations before clinical implementation. Although our models identify associations between baseline ocular biometrics and individual responses to specific lens designs, these findings are exploratory and should not be interpreted as evidence of superior efficacy for any lens type. The predictive formulas are intended to generate testable hypotheses for personalized fitting, not to establish comparative effectiveness.
Conclusion
This study found no statistically significant differences in average efficacy across the five defocus lens types when matched for baseline characteristics. However, ocular biometric parameters can be leveraged to predict individual responses, enabling personalized lens selection.
Data Sharing Statement
The datasets used and analyzed during the current study are available from the corresponding author on reasonable request.
Ethics Approval and Consent to Participate
The study protocol received approval from the Ethics Review Committee of Peking University People’s Hospital (Approval No: 2021PHB322-001). All procedures conformed to the ethical principles outlined in the Declaration of Helsinki.
Consent for Publication
All authors consent to be co-authors of this paper.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
Disclosure
The authors have no competing interests to disclose for this work.
References
1. Pan Z, Xian H, Li F, et al. Myopia and high myopia trends in Chinese children and adolescents over 25 years: a nationwide study with projections to 2050. Lancet Reg Health West Pac. 2025;59:101577. doi:10.1016/j.lanwpc.2025.101577
2. Moreira-Rosario A, Lanca C, Grzybowski A. Prevalence of myopia in Europe: a systematic review and meta-analysis of data from 14 countries. Lancet Reg Health Eur. 2025;54:101319. doi:10.1016/j.lanepe.2025.101319
3. Kido A, Miyake M, Watanabe N. Interventions to increase time spent outdoors for preventing incidence and progression of myopia in children. Cochrane Database Syst Rev. 2024;6(6):CD013549. doi:10.1002/14651858.CD013549.pub2
4. Jiravarnsirikul A, Belghith A, Rezapour J, et al. Evaluating glaucoma in myopic eyes: challenges and opportunities. Surv Ophthalmol. 2025;70(3):563–9. doi:10.1016/j.survophthal.2024.12.003
5. Cheong KX, Xu L, Ohno-Matsui K, Sabanayagam C, Saw SM, Hoang QV. An evidence-based review of the epidemiology of myopic traction maculopathy. Surv Ophthalmol. 2022;67(6):1603–1630. doi:10.1016/j.survophthal.2022.03.007
6. Wang -D-D, Zhou P. Myopia: pathogenesis and Intervention. Nat Cell Sci. 2025;3(1):62–76. doi:10.61474/ncs.2024.00049
7. Zhao J, Yu Y, Li Y, et al. Development and validation of predictive models for myopia onset and progression using extensive 15-year refractive data in children and adolescents. J Transl Med. 2024;22(1):289. doi:10.1186/s12967-024-05075-0
8. Modjtahedi BS, Abbott RL, Fong DS, Lum F, Tan D, Task Force on M. Reducing the global burden of myopia by delaying the onset of myopia and reducing myopic progression in children: the academy’s task force on myopia. Ophthalmology. 2021;128(6):816–826. doi:10.1016/j.ophtha.2020.10.040
9. Goethals S, Louboutin A, Hamlaoui S, et al. Nonlinear spatial integration allows the retina to detect the sign of defocus in natural scenes. Sci Adv. 2025;11(32):eadq6320. doi:10.1126/sciadv.adq6320
10. Zhang L, Yi K, Sun Q, et al. Palladium nanocrystals regulates scleral extracellular matrix remodeling in myopic progression by modulating the hypoxia signaling pathway Nrf-2/Ho-1. J Control Release. 2024;373:293–305. doi:10.1016/j.jconrel.2024.07.031
11. Liu J, Lu Y, Huang D, et al. The efficacy of defocus incorporated multiple segments lenses in slowing myopia progression: results from diverse clinical circumstances. Ophthalmology. 2023;130(5):542–550. doi:10.1016/j.ophtha.2023.01.007
12. Wang M, Ma R, Kuang L, et al. Myopia control efficacy of asymmetric multipoint defocus technique spectacle lenses: one-year double-masked randomized controlled trial. Ophthalmology. 2025;132(9):972–979. doi:10.1016/j.ophtha.2025.04.022
13. Lu Y, Yang X, Zhou J, et al. Diversified segmental defocus optimization lenses with and without atropine for myopia prevention: a randomized clinical trial. JAMA Ophthalmol. 2025;143(8):684–691. doi:10.1001/jamaophthalmol.2025.2072
14. Zhou P, Wang D. Comparing the efficacy of low-dose atropine eye drops, orthokeratology, and combined treatment for myopia progression control. Nat Cell Sci. 2025;3(1):1–6. doi:10.61474/ncs.2024.00048
15. Sarkar S, Khuu S, Kang P. A systematic review and meta-analysis of the efficacy of different optical interventions on the control of myopia in children. Acta Ophthalmol. 2024;102(3):e229–e244. doi:10.1111/aos.15746
16. Yu J, Guo Y, Zhou Y. Comparison of the effects of orthokeratology and highly aspherical lenselets in achieving myopia control and defocus in adolescents. Eye Contact Lens. 2024;50(10):445–454. doi:10.1097/ICL.0000000000001124
17. Zhou P, Wang DD, Fan L, Yang L, Zhao MW. Thin central corneal thickness may be a risk factor for myopia progression in children. J Ophthalmol. 2023;2023:3815863. doi:10.1155/2023/3815863
18. Yuan XL, Zhang R, Zheng Y, et al. Corneal curvature-associated MTOR variant differentiates mild myopia from high myopia in Han Chinese population. Ophthalmic Genet. 2021;42(4):446–457. doi:10.1080/13816810.2021.1923035
19. Ganesh S, Lusobya RC, Uduman MS, et al. Ocular biometric parameters in South-Indian children with myopia - A hospital-based retrospective descriptive analysis. Indian J Ophthalmol. 2025;73(2):292–296. doi:10.4103/IJO.IJO_546_24
20. Shao H, Zhu Q, Zhang L, et al. Corneal biomechanical properties in myopic anisometropia measured by corneal visualization scheimpflug technology. Am J Transl Res. 2025;17(4):2817–2825. doi:10.62347/EPRI9798
21. Mu J, Zhong H, Jiang M, Wang J, Zhang S. Development of a nomogram for predicting myopia risk among school-age children: a case-control study. Ann Med. 2024;56(1):2331056. doi:10.1080/07853890.2024.2331056
22. Hu T, Wu R, Wang W, Li H, Peng X. Analysis of factors related to the development of ocular biometric parameters in Chinese children aged 6-10 years: a cross-sectional study. BMJ Open. 2024;14(2):e080066. doi:10.1136/bmjopen-2023-080066
23. Gawne TJ, Khanal S, Norton TT. An alternative mechanism for the anti-myopia effectiveness of diffusion optics technology (DOT) lenses. Transl Vis Sci Technol. 2025;14(1):15. doi:10.1167/tvst.14.1.15
24. Neitz J, Neitz M. Diffusion optics technology (DOT): a myopia control spectacle lens based on contrast theory. Transl Vis Sci Technol. 2024;13(10):42. doi:10.1167/tvst.13.10.42
25. Jabeen A, Luensmann D, Woods J, Hill JS, Jones L. Evaluation of lag of accommodation with full-field diffusion optics technology (DOT) contrast management spectacle lenses in emmetropic children. Clin Ophthalmol. 2024;18:1181–1190. doi:10.2147/OPTH.S453790
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.