Back to Journals » Clinical Optometry » Volume 18
A Pilot Study of Retinal Vessel Calibre and Its Potential Link to Cardiovascular Risk in HIV
Authors Buthelezi LM ![]() , Munsamy AJ
, Munsamy AJ ![]() , Mashige KP
, Mashige KP ![]()
Received 30 May 2025
Accepted for publication 15 November 2025
Published 14 February 2026 Volume 2026:18 541786
DOI https://doi.org/10.2147/OPTO.S541786
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Mr Simon Berry
Lungile M Buthelezi, Alvin J Munsamy, Khathutshelo P Mashige
Department of Optometry, University of Kwazulu-Natal, Durban, KwaZulu-Natal, South Africa
Correspondence: Lungile M Buthelezi, Email [email protected]
Background: This pilot study investigates the effects of HIV and antiretroviral therapy (ART) on retinal vessel calibre in immunocompetent people living with HIV (PLHIV). Changes in vessel calibre in HIV-positive individuals may serve as biomarkers of iBRB integrity and endothelial dysfunction.
Methods: This was a cross-sectional study. Fundus photography was conducted in three groups: HIV-positive individuals on ART (HIV-ART, n=62 eyes), HIV-positive ART-naïve individuals (HIV-NART, n=20 eyes), and a comparison group of HIV-negative controls (n=82 eyes). We evaluated retinal vessel calibres (Arteriolar widths, venular widths, central retinal artery equivalent (CRAE), central retinal vein equivalent (CRVE), arteriole-venule ratio (AVR) using VAMPIRE software. Association models included Multivariable regression, generalized estimated equations, and mixed effects models.
Results: The mean venular width was significantly greater among PLHIV compared to HIV-negative controls (p=0.003). Longer ART duration was associated with the narrowing of venules in the HIV-ART group, particularly affecting mean venular width (β=− 1.40 μm, p=0.02) and CRVE (β=− 4.44 μm, p=0.05). The generalized model showed longer ART duration was positively associated with wider arteriolar calibre (β=7.09 μm for CRAE, p=0.001). The HIV-NART group had a significantly higher odds of abnormal CRAE (OR=3.00; p=0.033) compared to controls.
Conclusion: This study provides a novel perspective on the probable link between retinal vessel calibre and systemic HIV factors, suggesting a possible relationship to systemic vascular health. All health clinicians should be aware of the potential for ART to influence retinal microvasculature. Future research should focus on larger cohorts and longitudinal studies to track changes in vessel calibre over time.
Keywords: antiretroviral therapy, human immunodeficiency virus, retina, vessel calibre, cardiovascular
Background
The human immunodeficiency virus (HIV) continues to affect millions of people globally, posing a threat to global health. Antiretroviral therapy (ART) has made great progress in controlling the infection in people living with HIV (PLHIV); however, despite viral suppression with ART, HIV continues to exert systemic effects, including on the ocular vasculature.1 The impact of HIV and ART on vascular function and endothelial integrity is an active area of research, with particular interest in identifying biomarkers that may signal increased cardiovascular risk.
Ocular complications in PLHIV often reflect both systemic and local inflammation, which can influence retinal structure and function. The retina’s vascular network, particularly the blood vessels’ calibre, may serve as a valuable marker of systemic health because of its direct interaction with blood flow and sensitivity to immune and inflammatory changes. Changes in blood flow regulation and vessel calibre have been linked to endothelial dysfunction, which is characterised by the poor function of the endothelial cells lining blood vessels. The relationship of retinal calibre modification (narrower retinal arterioles and wider retinal venules) has been accepted as an indication of long-term risk of cardiovascular mortality and is correlated with cardiovascular risk factors. As a result, vessel calibre may be a valuable biomarker of inflammation and inner blood retina barrier (iBRB) integrity when used to analyse the retinal vascular structure. Studies such as the Beaver Dam Eye Study,1 Rotterdam Study,2 and the Atherosclerosis Risk in Communities (ARIC) study3 have all indicated a relationship between blood vessel endothelial dysfunction and vessel calibre. In HIV research using semi-automated software applied to digital fundus photographs, increasing HIV viral loads are associated with decreased retinal arteriolar calibre.4,5 There is also a positive correlation of narrowing of retinal arterioles with commencement and duration of ART, in which blood vessels narrowed with increasing years on therapy.5,6 Arteriolar calibre is thought to reflect endothelial and smooth muscle dysfunction, often linked to immune activation and oxidative stress, whereas venular dilation is more closely related to systemic inflammation and impaired venous drainage.5,6 These distinct physiological responses may explain why arteriolar and venular calibres respond differently to HIV-related immune suppression and ART exposure.
However, it remains unclear how clinically applicable these previous findings are, especially considering the diversity in study populations and methodologies. Few studies have included ART-naïve individuals as a comparative group, making it difficult to separate the direct effects of HIV on retinal health from those associated with ART exposure. This study includes a small ART-naïve group to explore this gap, possibly offering a clearer perspective on how ART, viral load, and other HIV-related factors contribute to retinal vessel changes. By exploring these factors in ART-naïve and ART-receiving PLHIV, this study seeks to provide direction for a more nuanced understanding of the relationship between HIV, ART, and retinal health. Although exploratory in nature, this pilot study hypothesizes that retinal vessel calibre differs between ART-treated, ART-naïve, and HIV-negative individuals. Therefore, this pilot study aims to investigate structural changes in retinal vessel calibre in PLHIV and assess how these changes relate to immunological factors and ART exposure, with a particular focus on the inclusion of an ART-naïve subgroup.
Methods
This cross-sectional pilot study was conducted at a tertiary care hospital between 2022 and 2024 using convenience sampling from outpatient clinics. The study only included adults (all genders and ethnicities) who were aged 18 to 65 years. HIV immunocompetence was regarded as CD4 > 350 cells/mm3 and viral load (VL) less than 1000 copies/mL. Participants were stratified into three groups: HIV immunocompetent on ART (31 participants, n = 62 eyes, HIV-ART), immunocompetent not on ART (10 participants, n = 20 eyes, HIV-NART), and a HIV-negative comparison group (41 participants, n = 82 eyes, HIV control). Exclusion criteria included a history of diabetes mellitus, hypertension, current tobacco use, and ocular or retinal pathology (eg, diabetic retinopathy, hypertensive retinopathy, glaucoma). All participants underwent a clinical review, including medical history and chart review, to confirm eligibility.
Sampling
A purposive sampling technique was employed. The sample size was calculated using two population mean formula:
where Z represents the critical values from the standard normal distribution corresponding to the chosen significance level (α) and power (1−β), with α as the Type I error rate and β as the Type II error rate. The standard deviations of VF for the experimental and control groups are denoted by σ1 and σ2, which are 1.68 and 1.46, respectively, based on previous studies. The group means for VF are ( )1 = −1.34 (experimental) and (
)1 = −1.34 (experimental) and ( )2 = −0.33 (control).22 Using these values, the required sample size to achieve 92% power is calculated to be 141 eyes (71 per group). To account for potential dropouts and non-responses, a 10% increase is recommended, resulting in a final target sample size of 156 eyes (79 experimental group and 79 control group) to ensure statistical robustness.
)2 = −0.33 (control).22 Using these values, the required sample size to achieve 92% power is calculated to be 141 eyes (71 per group). To account for potential dropouts and non-responses, a 10% increase is recommended, resulting in a final target sample size of 156 eyes (79 experimental group and 79 control group) to ensure statistical robustness.
Blood Laboratory Investigations
Demographic data (age, sex) and HIV-related clinical information (CD4 count, CD4%, viral load, and ART duration) were extracted from patient records and verified against the National Health Laboratory Service (NHLS) online system. Blood work was conducted as part of the routine primary health care protocol at the data collection site.
The CD4 count measures the absolute number of CD4 cells in a microliter of blood, indicating the strength of the immune system. In contrast, the CD4% represents the percentage of total lymphocytes that are CD4 cells. While the CD4 count shows the overall immune cell quantity, CD4% provides a relative measure that can be more stable over time, especially when overall white blood cell counts fluctuate. Both metrics are routinely used to assess immune health in PLHIV.
The duration of ART use was self-reported and cross-verified with the NHLS database, based on the date of first HIV diagnosis. Although the exact date of ART initiation is not recorded, in South Africa, ART is typically initiated immediately following a positive test result.
Measurement of Blood Vessel Integrity
All patients underwent a complete ophthalmological examination, including visual acuity evaluation using Snellen chart, slit lamp biomicroscopy and fundus photography.
Fundus Photography for Retinal Vessel Imaging
Non-mydriatic digital fundus images were obtained from both eyes of each patient. To account for narrow pupils, the examination was performed in a darkened room. Fundus images were obtained, at a 30° camera angle with the optic nerve head (ONH) centered using the Zeiss Visucam non-mydriatic fundus camera (Carl Zeiss, Germany).
Vessel Calibre Measurement
The Vascular Assessment and Measurement Platform for Images of the Retina (VAMPIRE) software (VAMPIRE; VAMPIRE group, University of Dundee, Dundee, Scotland) was used to obtain vessel calibres.7 VAMPIRE computes measurements per image including basic statistics: central retinal artery equivalent (CRAE), central retinal vein equivalent (CRVE), and arteriole-venule ratio (AVR).
Vessels are subsequently detected and labelled as arterioles or venules automatically. The six largest arterioles and six largest venules in a ring-shaped area located between 0.5- and 1.0-disc diameters from the edge of the optic nerve (B-zone) are identified and then combined into two summary measures: CRAE and CRVE (Figure 1). Summarised retinal vessel calibre of CRAE and CRVE is calculated according to a standard protocol developed by Hubbard et al.8 These are then expressed as an AVR. Raw measurements of CRAE and CRVE are computed in pixels by VAMPIRE. Raw CRAE and CRVE measurements were computed in pixels by the VAMPIRE software. These were converted to micrometres (μm) using a pixel-to-micron conversion factor derived from the Zeiss Visucam 500 calibration data. For 30° field-of-view (FOV) Visucam images with a resolution of 2124 × 2056 pixels, the conversion factor was calculated as 4.07 μm per pixel, based on an assumed average optic disc diameter of 1850 μm.
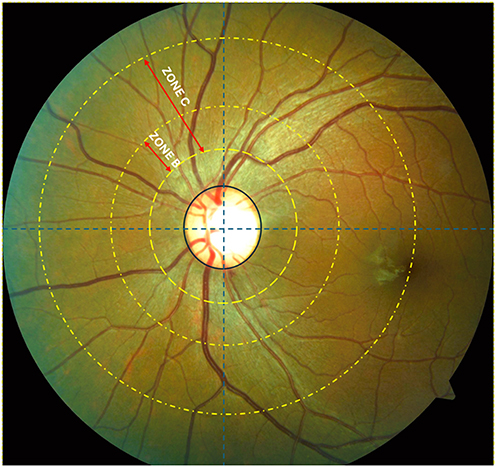 |
Figure 1 Retinal fundus image zones using VAMPIRE software. |
Data Analysis
Both eyes of each patient were analysed. Data was analysed using Statistical Product and Service Solutions (SPSS), version 27 (IBM Corp). The Schapiro–Wilk test was used to check normality. All data were normally distributed; therefore, parametric tests were used. Descriptive and inferential statistics were calculated. Descriptive statistics were provided as means with standard deviations. All the tests were two-tailed, and the criterion for statistical significance was set at 5% level. Multivariable analysis investigated associations between HIV factors (CD4 count, viral load, ART duration) with vessel calibres, adjusting for age and sex.
Ethics Statement
This study was conducted in accordance with the ethical standards of the Declaration of Helsinki and approved by the University of KwaZulu-Natal Biomedical Research Ethics Council (ref: BREC/00002911/2021). Written informed consent was obtained from all participants prior to their inclusion in the study.
Results
Participant Characteristics
The study’s demographic characteristics and HIV-related factors, shown in Table 1, provide an overview of the three groups. The average age for HIV on ART (HIV-ART) was 43.61±9.89 years, while HIV not on ART (HIV-NART) had a mean age of 40.60±11.27 years. The HIV-negative controls were 42.6±12.14 years old on average. The non-significant age distributions across groups help to control for age-related differences in the analysis. The average duration of ART (Dolutegravir) intake among HIV-ART was 8.57±4.59 years. Immune status, indicated by CD4 count and percentage, varied between the two HIV-positive groups. The mean CD4 count for the HIV-ART group was 624.53±209.86 cells/mm3, higher than the 405±60 cells/mm3 observed in HIV-NART. Similarly, the CD4 percentage was higher in HIV-ART, with an average of 26.97%±8.19%, compared to 21.35%±7.04% in HIV-NART group.
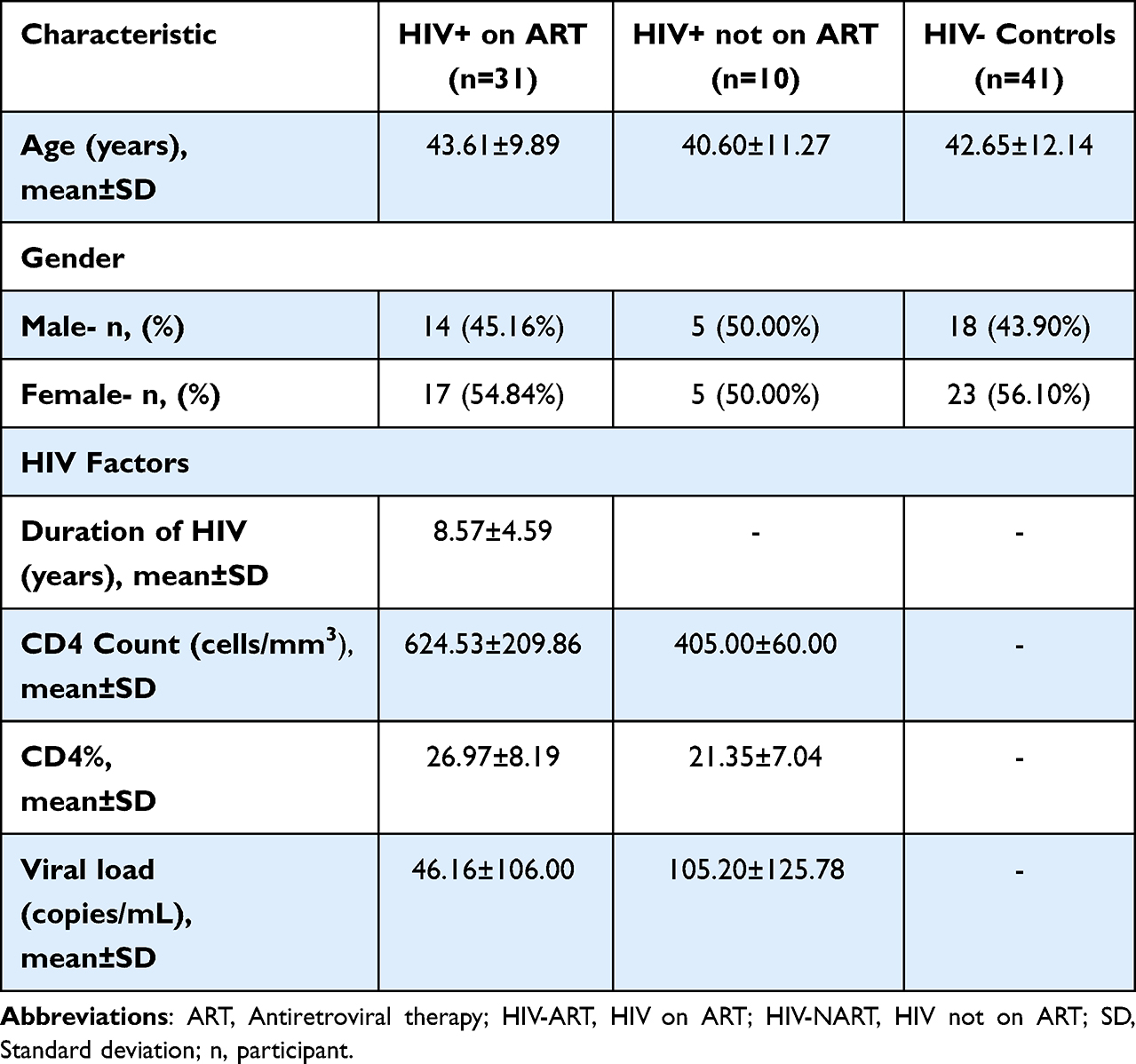 |
Table 1 Demographic Characteristics and HIV Factors |
Retinal Vessel Calibre Measurements
The analysis of vascular calibre measurements revealed several significant findings across the three groups (Table 2). Individuals with HIV, whether on ART or not, exhibited narrower arterioles and wider venules compared to HIV-negative controls, suggesting early microvascular alterations associated with HIV infection.
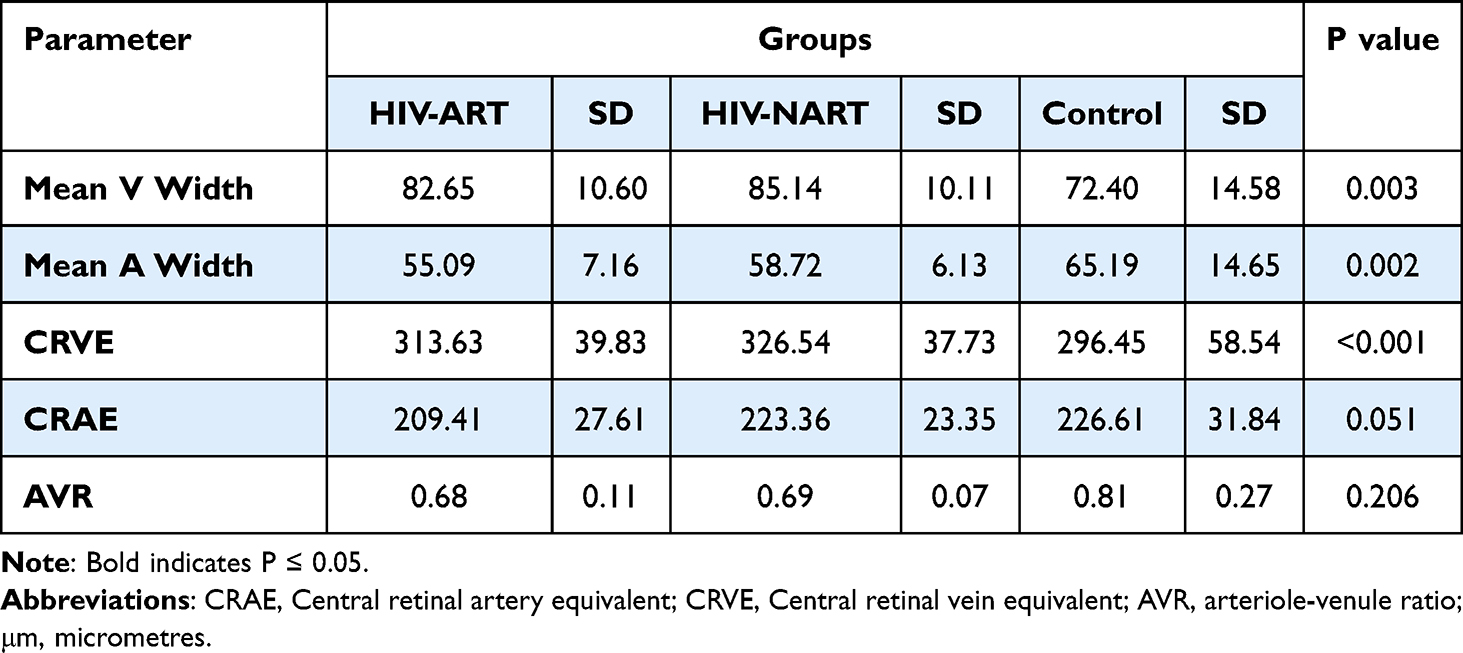 |
Table 2 Retinal Vessel Calibre Measurements |
The mean arteriolar width for the HIV-ART group was 55.09±7.16 μm, while the HIV-NART group had a mean of 58.72±6.13 μm, and the HIV-negative controls measured 65.19±14.65 μm (p = 0.002). The CRAE measurements showed a similar trend, with the HIV-ART group averaging 209.41±27.61 μm, the HIV-NART group 223.36±23.35 μm, and the HIV-negative controls 226.61±31.84 μm (p = 0.051).
The mean venular width was significantly greater among PLHIV compared to HIV-negative controls, with the HIV-ART group averaging 82.65±10.60 μm, the HIV-NART group 85.14±10.11 μm, and the controls 72.40±14.58 μm (p = 0.003). Similarly, CRVE values were higher in the HIV groups compared to controls (HIV-ART: 313.63±39.83 μm; HIV-NART: 326.54±37.73 μm; control: 296.45±58.54 μm; p < 0.001). Cohen’s d effect sizes in the HIV-NART group showed notable differences in mean venular width (Cohen’s d = 0.73, CI: 0.23–1.22) and the CRVE (Cohen’s d = 0.88, CI: 0.38–1.39) of larger vessel calibres in HIV-NART.
The AVR values were slightly lower among PLHIV compared to controls (HIV-ART: 0.68±0.11; HIV-NART: 0.69±0.07; control: 0.81±0.27), although this difference did not reach statistical significance (p = 0.206).
Multivariable Regression Analysis of Vessel Calibre Associations with HIV Factors
This analysis examined the relationship between HIV-related factors (CD4 count, CD4 percentage, viral load, and ART duration) and retinal vessel calibre. Findings indicate that higher CD4 counts and CD4% are associated with wider retinal arteriolar vessels, particularly in HIV-NART, while increased ART duration is linked to the narrowing of venular calibre. The analysis is detailed in Supplementary Table 1.
CD4 Count
Higher CD4 counts in the HIV-NART group were linked to notable increases in both arteriolar and venular widths. In contrast, the associations in the HIV-ART group were weaker. In the HIV-NART group, higher CD4 counts were linked to increases in mean venular width (β = 0.27, 95% CI: 0.21–0.33, p < 0.001), mean arteriolar width (β = 0.15, CI: 0.12–0.19, p < 0.001), CRVE (β = 1.06, CI: 0.82–1.29, p < 0.001), and CRAE (β = 0.57, CI: 0.45–0.69, p < 0.001). For the HIV-ART group, a significant association was observed with mean venular width (r = 0.02, CI: 0.00–0.05, p = 0.02) and CRAE (β = 0.09, CI: 0.01–0.17, p = 0.03), indicating a smaller but still meaningful impact of CD4 count on retinal vessel measurements.
CD4 Percentage
In the HIV-NART group, higher CD4 percentages were linked to substantial increases in arteriolar and venular widths, as well as CRVE and CRAE. Higher CD4% were linked to increases in mean venular width (β = 2.14, CI: 0.93–3.36, p < 0.001), mean arteriolar width (β = 1.50, CI: 0.88–2.13, p < 0.001), CRVE (β = 8.52, CI: 3.88–13.16, p < 0.001), and CRAE (β = 5.34, CI: 3.03–7.64, p < 0.001). In the HIV-ART group, significant findings included positive associations with mean venular width (β = 1.00, CI: 0.02–1.97, p = 0.05), mean arteriole width (β = 0.92, CI: 0.36–1.47, p < 0.001), CRVE (β = 3.72, CI: 0.09–7.35, p = 0.05), and CRAE (β = 3.40, CI: 1.30–5.51, p < 0.001), though the magnitude of the effects was generally lower than in the HIV-NART group.
Viral Load
Viral load has a distinct impact on retinal vessel measurements, with opposite effects observed between HIV-ART and HIV-NART. In the HIV-NART group, viral load was a negative association showing a decrease in mean venular width (β = −23.17, CI: −45.60 to −0.73, p = 0.04) and CRVE (β = −92.52, CI: −178.45 to −6.60, p = 0.04) with higher viral loads. For the HIV-ART group, higher viral load was significantly linked to an increase in CRVE (β = 81.87, CI: 1.55–162.19, p = 0.05). The wide confidence intervals for these associations, particularly in the ART-naïve subgroup, suggest a high degree of imprecision in the estimated effect, emphasizing the exploratory nature of this finding.
ART Duration
Longer ART duration was associated with the narrowing of retinal arteriolar calibres in individuals on HIV-ART, particularly affecting mean arteriolar width and CRAE. The most prominent effects were observed in mean arteriolar width (β = −1.40, CI: −2.57 to −0.23, p = 0.02) and CRAE (β = −4.44, CI: −8.87 to −0.01, p = 0.05), indicating a narrowing of these vessels with longer ART duration. The effects on other retinal vessel parameters were not statistically significant, suggesting a more localised impact of ART duration on venular dimensions.
Generalized Estimating Equation (GEE) on the Pooled HIV-Positive Cohort (HIV-ART and HIV-NART)
Further multivariable analysis using a Generalized Estimating Equation (GEE) on the pooled HIV-positive cohort (HIV-ART and HIV-NART), adjusted for age and sex, revealed significant associations with demographic and ART factors (details in Supplementary Table 1). Male participants exhibited significantly wider venular calibre than females. This was observed for both the Mean Venular Width (β=11.92μm, CI: 4.01μm to 19.82μm, p=0.003) and the CRVE (β=44.83μm, CI: 15.20μm to 74.45μm, p=0.003).
The duration of ART was positively associated with wider venular calibre in the pooled model. Each additional year on ART was associated with an increase of 2.06μm in Mean Venular Width (β=2.06μm, CI: 0.92μm to 3.20μm, p<0.001) and an increase of 7.09μm in CRVE (β=7.09μm, CI: 2.97μm to 11.21μm, p=0.001). Additionally, in the pooled multivariable model, a higher CD4% was associated with a small, but statistically significant, narrowing of venular vessels: Mean Venular Width (β=−0.52μm, CI: −1.02μm to −0.02μm, p=0.042) and CRVE (β=−1.88μm, CI: −3.68μm to −0.07μm, p=0.042).
Linear Mixed Effects Model Sensitivity Analysis on the Pooled HIV-Positive Cohort
A Linear Mixed Effects Model (LMM) was employed as a sensitivity analysis on the pooled HIV-positive cohort to assess the independent effects of HIV-related factors on retinal vessel calibres, while explicitly controlling for the correlation between eyes within the same participant. All models were adjusted for age and sex. The LMM confirmed and strengthened several findings observed in the GEE analysis and the subgroup linear regressions. The analysis is detailed in Supplementary Table 1.
Males were significantly associated with wider Mean Venular Width (β=11.92 μm; CI: 4.49,19.34; p=0.002) and wider CRVE (β=44.83 μm; CI: 17.19,72.47; p=0.002) compared to female sex. This suggests a systemic difference in venular calibre between the sexes in this cohort.
A longer duration of ART was significantly associated with a wider CRVE (β=7.09 μm per year of ART; CI: 2.97,11.21; p=0.001). This finding suggests that longer ART exposure may be protective or related to better preserved venular integrity, an association that requires further investigation.
Risk Factors for Vessel Calibre Morphological Alterations
To evaluate whether HIV-positive status, stratified by ART use, was independently associated with an increased risk of abnormal retinal vessel calibres, a logistic regression was performed, using the HIV-negative control group as the reference. All models were adjusted for age and sex (Table 3).
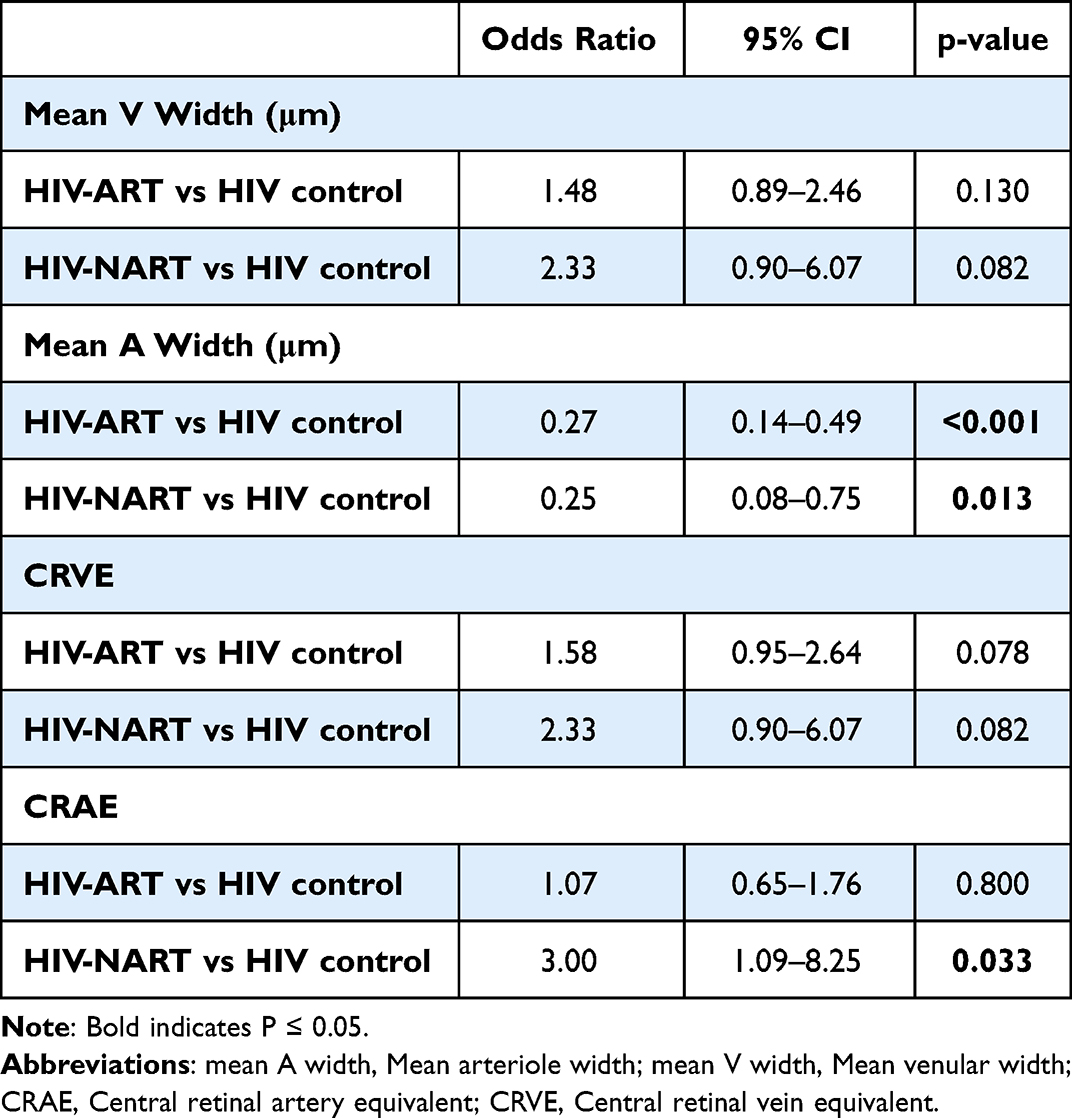 |
Table 3 Logistic Regression for Vessel Calibre Alterations |
Both HIV subgroups had significantly lower odds of having an abnormal Mean Arteriolar Width outcome compared to the HIV-negative control group. The HIV-ART group had significantly reduced odds (OR=0.27; CI: 0.14,0.49; p<0.001). The HIV-NART group also showed significantly reduced odds (OR=0.25; CI: 0.08,0.75; p=0.013). Since the Odds Ratios are less than 1, this indicates that both HIV subgroups are less likely to have the abnormal arteriolar width outcome compared to the control group.
The HIV-NART group showed a significantly increased odds of having an abnormal CRAE compared to the HIV-negative control group (OR=3.00; CI: 1.09,8.25; p=0.033). This suggests that the ART-naïve state is independently associated with a threefold greater risk of an abnormal overall arteriolar calibre.
No significant difference was found between either HIV subgroup or the control group for the venular measures.
Discussion
This pilot study examined the relationship between HIV, ART exposure, and retinal vessel calibre alterations, with an emphasis on the integrity of iBRB and potential implications for cardiovascular health. While preliminary, the findings suggest that HIV infection, regardless of ART status, may be associated with structural differences in retinal vasculature compared to HIV-negative controls. Individuals living with HIV, both those on ART and those who were ART-naïve, exhibited significantly narrower arterioles and wider venules compared to HIV-negative controls, suggesting early microvascular alterations associated with HIV infection.
HIV-related endothelial dysfunction is further supported by our findings of variations in retinal vessel calibre among PLHIV compared to controls. Although the arteriole-to-venule ratio (AVR) is commonly used as a summary metric, it may mask important vessel-specific differences. In our study, AVR did not differ significantly between groups. However, this may be because AVR does not adequately reflect isolated changes in arteriolar or venular calibre.9 For instance, a smaller AVR may result from both broader venules and narrower arterioles. Therefore, a lower AVR is unable to distinguish between alterations in venular and arteriolar calibre. This current study’s approach allowed for the detection of these distinct vessel-specific alterations.
Arteriolar narrowing and venular widening are hallmarks of microvascular remodelling and early signs of vascular stress and inflammation, features commonly seen in systemic conditions with elevated cardiovascular risk. The study further explored the relationship between HIV-related factors and vessel calibre. The HIV-NART group demonstrated strong associations between immune parameters (CD4 count and percentage) and retinal vessel calibre, suggesting that immune health directly affects the retinal vasculature in untreated individuals. Higher CD4 counts in this group were linked to notable increases in both arteriolar and venular widths. Similarly, higher CD4 percentages were linked to substantial increases in arteriolar and venular widths. These findings support the hypothesis that retinal vessel calibre is dynamic and responds to immune status.
Arteriolar dilatation may reflect responses to local hypoxia or metabolic demand, while venular widening is linked to systemic inflammation and metabolic dysfunction.10 This effect appears to diminish in the HIV-ART group, where longer ART duration was significantly associated with the narrowing of retinal arteriolar calibres, particularly affecting mean arteriolar width and CRAE. This narrowing with longer ART duration aligns with prior studies that found retinal arterioles narrow with increasing duration of ART.6 However, the GEE on the pooled HIV-positive cohort (HIV-ART and HIV-NART) revealed a different effect, showing that the duration of ART was positively associated with wider venular calibre. Specifically, each additional year on ART was associated with an increase of 2.06 μm in Mean Venular Width and an increase of 7.09 μm in CRVE. This complex picture, where ART is linked to arteriolar narrowing in the HIV-ART subgroup and venular widening in the pooled model, highlights the need to consider both immune recovery and potential ART-induced vascular effects. The finding of wider CRVE with longer ART duration suggests that prolonged ART may be protective or related to better preserved venular integrity, an association requiring further investigation.
Few studies have characterised retinal vasculature in immunocompetent HIV cohorts. In our study, CRAE and arteriolar calibre were wider in HIV-ART participants compared to controls, with longer ART duration associated with narrowing venules. Pathai et al6 discovered that retinal arteriolar diameters narrowed with increasing duration of ART, independent of age, where those who were on three years of ART showed reduced arteriolar diameters. These findings were later confirmed by Tan et al4 who found that higher viral loads whilst on ART were found to be associated with narrower arterioles and thought to be secondary to inflammation. Both these studies support the current study’s findings. Furthermore, all studies reinforce the link between ART duration, viral load, and remodeling of retinal arterioles in PLHIV. Notably, both studies did not find any significant associations between CD4 counts and retinal vascular parameters, which our study was able to show. This is possibly due to the inclusion of an immunocompetent treatment-naïve cohort. Li et al11 however, refuted all these findings by reporting that ART improved retinal venular health and was predictive of immune restoration in PLHIV who had been on ART for at least nine months. It must be noted that the study population in Li et al had CD4 counts lower than 200 cells/mm3 at the beginning of their study.
The current study carefully controlled potential confounders such as age, smoking, hypertension, and diabetes. All participants were African and of comparable age, allowing clearer attribution of findings to HIV status and ART exposure. The observed alteration of calibres in the HIV-ART group may be related to ART’s impact on systemic inflammation and endothelial cell function. ART has known metabolic and endothelial effects, and our findings support a hypothesis that prolonged ART may paradoxically contribute to subclinical vascular stiffening, despite controlling viral replication.12 These findings highlight the importance of considering both immune recovery and potential ART-induced vascular effects when assessing ocular health in HIV-positive individuals.
The integrity of the iBRB is crucial for maintaining retinal health, and disruptions can lead to retinal damage and vision impairment. Our study’s findings of altered vessel calibre in HIV-positive individuals point to a potential compromise of the iBRB. The re-modelling of arterioles and venules raises concerns about the impact of untreated HIV infection on endothelial health and iBRB function. Since endothelial dysfunction is a shared mechanism in both retinal and cardiovascular disease, our retinal findings may represent ocular correlates of systemic vascular injury in PLHIV.
We propose that retinal imaging serves as a non-invasive proxy for systemic vascular health, reflecting cumulative effects of HIV, immune recovery, and ART. A single layer of endothelial cells makes up the vascular endothelium, which lines the inside of blood vessels and acts as a semipermeable barrier between tissues and circulating blood, controlling vascular permeability, remodeling, and blood flow.10 In PLHIV, there is evidence of increased arterial stiffness linked to increased immune activation, which may reflect coronary artery disease (CAD).13,14 Patients on ART exhibited increased arterial stiffness, indicating that ART use does not improve endothelial function, even though patients with high viral loads were more likely to have it. According to a study that compared PLHIV with and without CAD with demographically matched negative controls with and without CAD, coronary endothelial function was significantly compromised in the PLHIV without CAD, comparable to coronary endothelial function in subjects with established CAD.15 Lorenz et al16 found that PLHIV who had been on ART for one year or less showed signs of sub-clinical atherosclerosis compared to those treatment-naive PLHIV. A comparative study of PLHIV on ART, healthy negative controls with no CAD, and negative controls with established CAD showed that PLHIV had increased thickness of the carotid artery compared to healthy controls. Lekakis et al17 compared HIV-negative CAD patients and PLHIV on ART (without clinical CAD) and found that PLHIV subjects and HIV-negative individuals with CAD had a similar increased thickness of carotid artery values.17 These findings demonstrated that PLHIV without CAD have considerable coronary endothelial dysfunction and demonstrated that such endothelial dysfunction can be as severe as in clinical CAD patients. We can propose that the ocular changes observed, alterations in retinal vessel calibre, are therefore not isolated findings but may serve as early indicators of systemic vascular and cardiovascular health.
Chronic low-grade inflammation, an established risk factor for cardiovascular disease, may be the fundamental process causing the ocular alterations seen in HIV-positive people.15 These ocular alterations, noted in our study, align with an increased cardiovascular risk profile, which has been linked to both lower CD4 counts and prolonged ART duration.15,17 This highlights the need for thorough cardiovascular evaluations in this cohort and raises the possibility that ocular health may mirror or indicate preclinical systemic reactions to ART. These results highlight how closely related cardiovascular and ocular health are, with endothelial dysfunction being a major factor in both. The ocular alterations reported in this investigation might indicate generalised cardiovascular concerns in addition to localised changes in the retinal and choroidal vasculature. Future studies must include the measurement of other systemic markers of CAD and linked diseases (cholesterol and obesity) to correlate with the vessel calibre findings. These include the measurement of Body mass index (BMI) and blood pressure, and blood markers (cholesterol profile and blood glucose).
Changes in these parameters could provide early indications of ocular or systemic vascular alterations, guiding clinical decisions regarding ART management and cardiovascular risk reduction strategies. Furthermore, the study emphasizes the need for an adapted approach to ART, taking into consideration individual variations in immune recovery and potential vascular side effects. Clinicians should be aware of the potential for ART to influence retinal microvasculature and should include regular ophthalmological evaluations as part of routine care for PLHIV, especially those on long-term ART. Future research should focus on longitudinal studies to track changes in vessel calibre over time.
This pilot study demonstrates the potential utility of retinal imaging as a non-invasive biomarker for vascular alterations in PLHIV, however, the study had some limitations. The study’s pilot nature and small sample size, particularly in the HIV-NART subgroup, limit statistical power to generalize findings. Additionally, magnification-related variables such as axial length, refractive error, and corneal curvature, known confounders of retinal vessel calibre, were not available for adjustment and should be considered in future studies. The unreported assessment of multicollinearity among the independent variables can lead to inflated standard errors and unstable regression coefficients (high Variance Inflation Factors); these should be assessed in future studies. There is also a need to comprehensively adjust for key systemic CVD risk factors (blood pressure, BMI, and cholesterol profile).
Conclusion
This study explored the impact of HIV infection and ART on retinal vessel calibre to better understand their relationship with iBRB structural integrity and systemic vascular health. Retinal vessel changes were associated with immune status and ART duration, suggesting that retinal imaging could provide early signals of systemic vascular stress. These findings highlight the potential for inclusion into ophthalmic evaluations in PLHIV on long-term ART and may support the role of retinal imaging as a window into cardiovascular health.
Abbreviations:
AVR, Arteriole-venule ratio; ART, Antiretroviral therapy; CRVE, Central Retinal Vein Equivalent; CAD, Coronary Artery Disease; HIV, Human Immunodeficiency Virus; iBRB, Inner Blood Retina Barrier; ONH, Optic Nerve Head; PLHIV, People Living with HIV.
Funding
There was no funder or sponsor for this study.
Disclosure
The authors report no competing interests in this work.
References
1. Klein R, Klein BEK, Knudtson MD, Wong TY, Tsai MY. Are inflammatory factors related to retinal vessel caliber? The beaver dam eye study. Arch Ophthalmol. 2006;124(1):87–11. doi:10.1001/ARCHOPHT.124.1.87
2. Ikram MK, De Jong FJ, Vingerling JR, et al. Are retinal arteriolar or venular diameters associated with markers for cardiovascular disorders? The Rotterdam Study. Invest Ophthalmol Vis Sci. 2004;45(7):2129–2134. doi:10.1167/IOVS.03-1390
3. Klein R, Sharrett AR, Klein BEK, et al. Are retinal arteriolar abnormalities related to atherosclerosis? The atherosclerosis risk in communities study. Arterioscler Thromb Vasc Biol. 2000;20(6):1644–1650. doi:10.1161/01.ATV.20.6.1644
4. Tan PB, Hee OK, Cheung C, et al. Retinal vascular parameter variations in patients with human immunodeficiency virus. Invest Ophthalmol Vis Sci. 2013;54(13):7962–7967. doi:10.1167/IOVS.13-13081
5. Edwar L, Karim B, Wijaya IP, et al. Factors affecting the health of retinal vessels in human immunodeficiency virus patients beginning anti-retroviral therapy. AIDS Res Hum Retroviruses. 2019;35(6):529–535. doi:10.1089/AID.2018.0251
6. Pathai S, Weiss HA, Lawn SD, et al. Retinal arterioles narrow with increasing duration of anti-retroviral therapy in hiv infection: a novel estimator of vascular risk in HIV? PLoS One. 2012;7(12):e51405. doi:10.1371/JOURNAL.PONE.0051405
7. Vampire. Available from: https://vampire.computing.dundee.ac.uk/.
8. Knudtson MD, Lee KE, Hubbard LD, Wong TY, Klein R, Klein BEK. Revised formulas for summarizing retinal vessel diameters. Curr Eye Res. 2003;27(3):143–149. doi:10.1076/CEYR.27.3.143.16049
9. Sun C, Wang JJ, Mackey DA, Wong TY. Retinal vascular caliber: systemic, environmental, and genetic associations. Surv Ophthalmol. 2009;54(1):74–95. doi:10.1016/J.SURVOPHTHAL.2008.10.003
10. Segal SS. Regulation of blood flow in the microcirculation. Microcirculation. 2005;12(1):33–45. doi:10.1080/10739680590895028
11. Li LJ, Cheung CY, Tan P, et al. Retinal vascular changes and immune restoration in a cohort of HIV/AIDS patients on highly active antiretroviral therapy. The Lancet. 2013:
12. Zanoli L, Briet M, Empana JP, et al. Vascular consequences of inflammation: a position statement from the ESH working group on vascular structure and function and the artery society. J Hypertens. 2020;38(9):1682. doi:10.1097/HJH.0000000000002508
13. Balsam P, Mikuła T, Peller M, et al. Evaluation of endothelial function and arterial stiffness in HIV-infected patients: a pilot study. Polish Heart J. 2015;73(5):344–351. doi:10.5603/KP.a2014.0231
14. Kaluba L, Goma F, Guure C, et al. Immune activation and arterial stiffness in lean adults with HIV on antiretroviral therapy. Southern African J HIV Med. 2021;22(1). doi:10.4102/sajhivmed.v22i1.1190
15. Iantorno M, Schär M, Soleimanifard S, et al. Coronary artery endothelial dysfunction is present in HIV-positive individuals without significant coronary artery disease. AIDS. 2017;31(9):1281–1289. doi:10.1097/QAD.0000000000001469
16. Lorenz MW, Stephan C, Harmjanz A, et al. Both long-term HIV infection and highly active antiretroviral therapy are independent risk factors for early carotid atherosclerosis. Atherosclerosis. 2008;196(2):720–726. doi:10.1016/J.ATHEROSCLEROSIS.2006.12.022
17. Lekakis J, Tsiodras S, Ikonomidis I, et al. HIV-positive patients treated with protease inhibitors have vascular changes resembling those observed in atherosclerotic cardiovascular disease. Clin Sci. 2008;115(5–6):189–196. doi:10.1042/CS20070353
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.