Back to Journals » Journal of Pain Research » Volume 9
A novel paradigm to evaluate conditioned pain modulation in fibromyalgia
Authors Schoen C, Ablin J, Ichesco E, Bhavsar R, Kochlefl L, Harris R, Clauw D, Gracely R, Harte S
Received 17 June 2016
Accepted for publication 18 July 2016
Published 26 September 2016 Volume 2016:9 Pages 711—719
DOI https://doi.org/10.2147/JPR.S115193
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Michael Schatman
Cynthia J Schoen,1,* Jacob N Ablin,2,* Eric Ichesco,1 Rupal J Bhavsar,3 Laura Kochlefl,1 Richard E Harris,1 Daniel J Clauw,1 Richard H Gracely,4 Steven E Harte1
1Department of Anesthesiology, Chronic Pain and Fatigue Research Center, University of Michigan, Ann Arbor, MI, USA; 2Institute of Rheumatology, Tel Aviv Suorasky Medical Center, and Sackler Faculty of Medicine, Tel Aviv University, Tel Aviv, Israel; 3Department of Neurology, University of Pennsylvania, Philadelphia, PA, 4Department of Endodontics, University of North Carolina – Chapel Hill, Chapel Hill, NC, USA
*These authors contributed equally to this work
Introduction: Application of noxious stimulation to one body area reduces pain sensitivity in a remote body area through activation of an endogenous pain-inhibitory network, a behavioral phenomenon referred to as conditioned pain modulation (CPM). The efficiency of CPM is predictive of a variety of health outcomes, while impaired CPM has been associated with various chronic pain conditions. Current methods used to assess CPM vary widely, and interest in CPM method development remains strong. Here, we evaluated a novel method for assessing CPM in healthy controls and fibromyalgia (FM) patients using thumb pressure as both a test and conditioning stimulus.
Methods: Sixteen female FM patients and 14 matched healthy controls underwent CPM testing with thumbnail pressure as the test stimulus, and either cold water or noxious pressure as the conditioning stimulus. CPM magnitude was evaluated as the difference in pain rating of the test stimulus applied before and during the conditioning stimulus.
Results: In healthy controls, application of either pressure or cold water conditioning stimulation induced CPM as evidenced by a significant reduction in test stimulus pain rating during conditioning (P=0.007 and P=0.021, respectively). In contrast, in FM patients, neither conditioning stimulus induced a significant CPM effect P-values >0.274). There was a significant difference in CPM magnitude for FM patients compared to healthy controls with noxious pressure conditioning stimulation (P=0.023); however, no significant difference in CPM was found between groups using cold water as a conditioning stimulus (P=0.269).
Conclusion: The current study demonstrates that thumbnail pressure can be used as both a test and conditioning stimulus in the assessment of CPM. This study further confirms previous findings of attenuated CPM in FM patients compared with healthy controls.
Keywords: pressure pain, cold pressor test, diffuse noxious inhibitory controls, quantitative sensory testing
Introduction
In both healthy humans and animals, application of noxious stimulation activates one or more endogenous networks resulting in conditioned pain modulation (CPM). Many different methods have been used to evaluate CPM,1,2 but no standard experimental paradigm has emerged. Nearly all such paradigms, however, incorporate both a conditioning stimulus (a noxious stimulus that evokes CPM) and a test stimulus (a noxious stimulus used to evaluate the analgesic response to the conditioning stimulus).3,4 The magnitude of CPM is typically calculated as the difference in pain ratings of the test stimulus at baseline and during or immediately following application of the conditioning stimulus. A reduction in test stimulus rating as a result of application of the conditioning stimulus implies functional or intact (inhibitory) CPM, and the degree of reduction expresses the magnitude or “efficiency” of CPM. In contrast, an increase in test stimulus rating during conditioning implies pain facilitation.
It has been hypothesized that healthy individuals with inefficient CPM are more susceptible to developing chronic pain disorders than are those with efficient CPM.5–7 In addition, inefficient CPM has been shown to be associated with increased analgesia requirements and postsurgical pain,8,9 and it has also been consistently observed in fibromyalgia (FM) patients compared to healthy controls.10–16 Although the precise neurobiological determinants for CPM are unknown, it has been shown in animals to be mediated in part by supraspinal inhibition of second-order neurons that transmit nociceptive information from primary nociceptors to the brain.17–19
Here, we performed a proof-of-concept validation study of a novel CPM paradigm in FM patients and healthy controls in which pressure applied to the thumbnail bed was used as both a test stimulus and a conditioning stimulus. This paradigm was compared to a more established method using pressure as a test stimulus and cold water hand immersion (ie, cold pressor task) as a conditioning stimulus.20–24
Methods
Subjects
Sixteen right-handed female patients (mean ± standard deviation [SD], age 44.9±9.0 years, range: 24–57) satisfying 1990 American College of Rheumatology criteria for FM25 participated. A clinical pain score rated ≥40 on a 100 mm visual analog scale (with 0= no pain and 100= worst possible pain) was required for enrollment. Fourteen age-matched (40.3±12.0 years, range: 20–60) female healthy control subjects were also recruited. All subjects provided a medical history and underwent physical examination to screen for concurrent illnesses. Exclusion criteria consisted of significant medical and psychiatric comorbidities, including morbid obesity, substance abuse within 2 years (including cannabis), cardiovascular disease, lung disease, major depression, and schizophrenia, and current use of opioid analgesics. Other medications for depression, anxiety, and pain were permitted in the FM group as long as stable dosages were maintained during the course of the study. The protocol was approved by the University of Michigan Institutional Review Board, and all subjects gave written consent prior to participation.
CPM assessment
We adapted the CPM paradigm of Granot et al, including their time parameters and method of stimulus presentation, for pressure stimuli as we have reported previously.26,27 Subjects underwent CPM testing with noxious pressure as the test stimulus, and either noxious pressure (n=15; eight FM patients and seven healthy controls) or noxious cold water (n=22; ten FM patients and twelve healthy controls) as the conditioning stimulus. Of the 30 subjects enrolled in this study, a subset of subjects (n=7; two FM patients and five healthy controls) participated in both pressure and cold water trials. Repeated visits were counterbalanced and separated by a minimum of 3 weeks to prevent potential carryover effects from the previous trial.
An initial psychophysical test identified the pressure intensity that would be used as the test stimulus and the conditioning pressure stimulus. Psychophysical testing was performed using methods previously validated by our group for the measurement of mechanical pain sensitivity.28–35 Instructions were scripted and subjects underwent a familiarization/training prior to testing. A series of discrete pressures was applied to the thumbnail bed with a 1 cm2 hard rubber circular probe attached to a hydraulic piston. The thumbnail was chosen in part because it represents a “neutral site” that is not associated with FM tender points, and it has been shown to be highly representative of overall pressure sensitivity throughout the body.36 The probe was positioned over the center of the subject’s dominant (right) thumbnail by a handheld plastic housing with a pistol-like grip, and the hydraulic system was activated by placing calibrated weights on a moveable platform and adjusting valves to control stimulus timing. The probe was lowered to apply pressure consistent with the weight on the moveable platform. The combination of valves and calibrated weights produced controlled and repeatable stimulation.
Each pressure application was 5 seconds in duration and delivered at 20 seconds intervals, beginning with 0.25 kg/cm2 and increasing in 0.25–0.50 kg/cm2 increments thereafter to either a maximum of 10 kg/cm2 or to tolerance (defined here as the first stimulus to elicit a rating of 80/100 or greater, or when subjects requested the test be stopped). Subjects used a 0–100 numerical rating scale (NRS) to verbally rate the intensity of the perceived pain sensation immediately following release of each pressure application. Zero was defined as “no pain”, and 100 was defined as “pain as bad as it could be”. From these ratings, regression analysis was used to interpolate the pressure value corresponding to a pain intensity rating of 60 on a 0–100 NRS (pain-60). The pain-60 pressure served as the test stimulus during both pressure and cold water CPM trials and as the conditioning stimulus during the pressure CPM trials.
Prior to conditioning stimulation, baseline pain elicited by the pain-60 test stimulus was rated three times on a 0–100 NRS after 10, 20, and 30 seconds of continuous pressure (Figure 1) applied to the nondominant (left) thumbnail using the device described above. Five minutes after baseline testing, CPM was induced by applying 60 seconds of continuous pain-60 pressure to the dominant thumbnail. Alternatively, CPM was induced by immersing the subjects’ dominant hand up to the wrist into a 12°C refrigerated circulating water bath (NESLAB Digital One RTE 7, Thermo Scientific, Newington, NH, USA) for 60 seconds. Pilot testing determined this temperature to be lowest tolerable by both FM patients and healthy controls. Subjects maintained their hand in an open, relaxed position for the duration. Parallel to the last 30 seconds of the pressure or cold water conditioning stimulus, the same test stimulus was reapplied to the nondominant thumbnail and rated every 10 seconds (at 40, 50, and 60 seconds). Subjects were also asked to rate the conditioning stimulus at the end of testing.
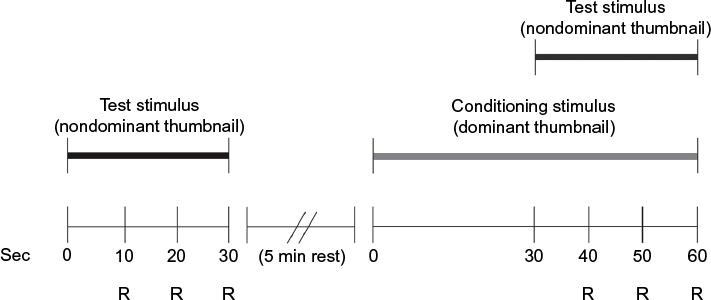 | Figure 1 CPM paradigm. Notes: Individually predetermined pain-60 test pressure was applied to the nondominant thumbnail for 30 seconds at baseline. After a 5 minute rest, the conditioning stimulus (either a pain-60 pressure to the dominant thumbnail or immersion of the dominant hand in a 12°C water bath) was applied for 60 seconds. For the last 30 seconds of the conditioning stimulus, the original test stimulus was reapplied to the nondominant thumbnail. Abbreviations: CPM, conditioned pain modulation; min, minutes; R, time point at which subjects rated the test stimulus; Sec, seconds. |
Data analysis
Group ages were compared by independent samples t-test. Within each group (healthy controls and FM patients), differences in test stimulus ratings before and during pressure and cold water conditioning were assessed separately with paired samples t-tests. These analyses were conducted to determine whether each paradigm produced a CPM effect. To compare the magnitude of the CPM effect between groups, a difference score was calculated for each subject by subtracting baseline ratings of the test stimulus from ratings of the test stimulus obtained during conditioning stimulation (Testconditioning − Testbaseline). Thus negative values reflect pain inhibition, whereas positive values reflect pain facilitation.3 Differences in CPM magnitude between groups and between conditioning stimuli (pressure and cold water) were assessed by independent samples t-tests. Results are presented as mean NRS pain ratings ± SD. Analyses were conducted with SPSS 22 (IBM, Armonk, NY, USA). A P-value of <0.05 was considered statistically significant.
Results
There was no significant difference in age between FM patients and healthy controls (t=−1.21, df=28, P=0.236). FM patients reported an average clinical pain score of 61.47±14.36 (range: 41–97) visual analog scale units, and reported using the following medications: pregabalin (n=6), bupropion (n=3), nonsteroidal anti-inflammatory drugs (n=3), amidrine (n=1), amitriptyline (n=1), escitalopram (n=1), lorazepam (n=1), and zolpidem (n=1).
In healthy controls, intact inhibitory CPM was identified by significant differences in means of test stimulus pain ratings taken at baseline and during thumbnail pressure pain conditioning stimulation (54.62±13.01 vs 40.76±19.93, respectively; t=4.06, df=6, P=0.007) and during cold water conditioning stimulation (50.97±22.13 vs 32.50±19.04; t=2.69, df=11, P=0.021) (Figure 2). In contrast, FM patients exhibited no significant change in mean pain ratings of the test stimulus obtained before and during pressure (47.58±24.69 vs 51.88±25.14; t=−0.73, df=7, P=0.487) or cold water (54.90±18.80 vs 47.33±24.64; t=1.16, df=9, P=0.274) conditioning stimulation (Figure 2). Both pressure and cold water conditioning stimuli were perceived as painful; healthy controls rated the cold water conditioning stimulus as 56.67±19.23 and the pressure conditioning stimulus as 47.00±10.95, while FM patients rated the cold water as 80.00±18.71 and the pressure as 51.25±14.36.
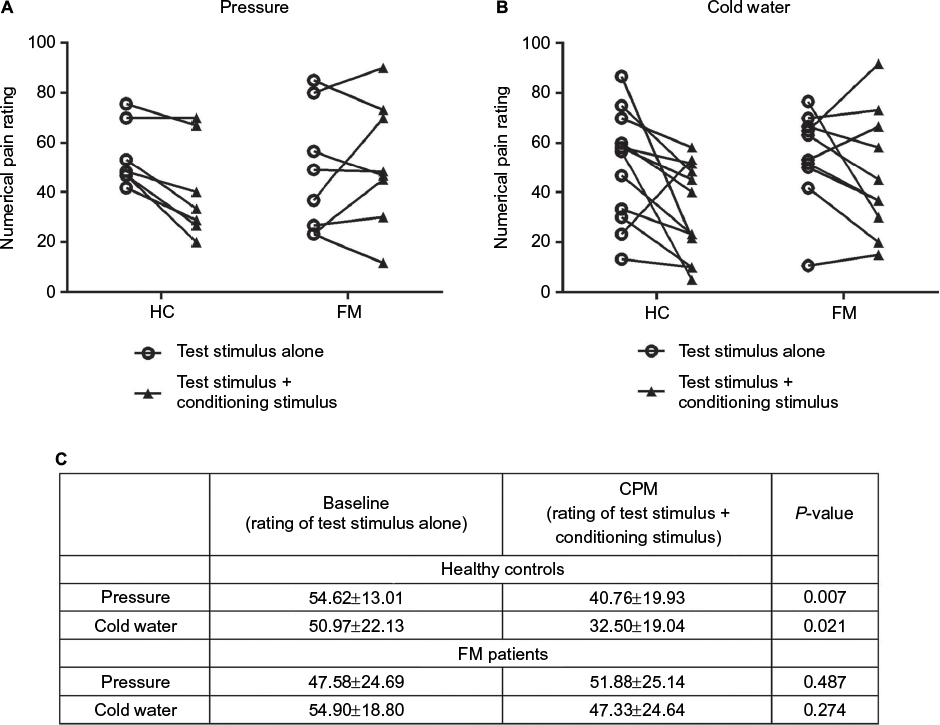 | Figure 2 Changes in pain ratings in HC and FM patients during a CPM paradigm. Notes: CPM was assessed by using pressure pain applied to the nondominant left thumbnail as the test stimulus and either pressure pain to the contralateral thumbnail (A) or cold water immersion of the contralateral hand (B) as the conditioning stimulus. Decreases in test stimulus pain ratings during conditioning stimulation are an indication of intact CPM. Note that not all healthy controls exhibited CPM and not all FM patients exhibited a lack of CPM. (C) Pain ratings (mean ± SD) at baseline and during CPM are shown by group and stimulus. Differences in test stimulus ratings before and during CPM were assessed with paired-samples t-tests. In healthy controls, the mean pain rating of the test stimulus significantly decreased when either pressure pain (n=7) or cold water (n=12) was used as the conditioning stimulus. In FM patients, the mean pain rating did not significantly change regardless of conditioning stimulus used (pressure pain, n=8; cold water, n=10). A subset of subjects (n=7) underwent both test stimuli on separate visits. Abbreviations: CPM, conditioned pain modulation; FM, fibromyalgia; HC, healthy control; SD, standard deviation. |
We further compared the CPM magnitude between healthy controls and FM patients for each conditioning stimulus using independent samples t-tests. For pressure conditioning, there was a significant difference in the CPM magnitude between groups (–13.86±9.03 for healthy controls vs 4.29±16.55 for FM patients; t=−2.58, df=13, P=0.023). For cold water conditioning, the difference between groups was not significant (−18.47±23.79 for healthy controls vs −7.57±20.55 for FM patients; t=−1.14, df=20, P=0.269).
Within each group of subjects, the effect of type of conditioning stimulus on CPM magnitude was not significant. For healthy controls, CPM magnitude was −18.47±23.79 as a result of cold water conditioning stimulation and was −13.86±9.03 as a result of pressure conditioning stimulation (t=−0.488, df=17, P=0.632). For FM patients, the CPM magnitude was −7.57±20.55 as a result of cold water conditioning stimulation and was 4.29±16.55 as a result of pressure conditioning stimulation (t=−1.32, df=16, P=0.205).
Discussion
To the best of our knowledge, this is the first study to evaluate CPM in healthy controls and FM patients using discrete thumbnail pressure as both a test and conditioning stimulus. We demonstrated that pressure pain conditioning stimulation applied to the thumbnail is at least as effective as cold water immersion of the hand for inducing CPM when pressure pain to the contralateral thumbnail is used as a test stimulus.
Few studies have compared different conditioning stimuli in CPM paradigms. Arendt-Nielsen et al used either deep muscle pain (hypertonic saline injection into tibialis anterior) or cold water immersion of the hand to evaluate magnitude of CPM in young, healthy subjects.21 They concluded that saline injections were effective at increasing pressure pain thresholds in males but not in females, while cold water was able to increase pressure pain thresholds in both sexes. Granot et al also evaluated CPM magnitude in young, healthy subjects and used either hot water or cold water as a conditioning stimulus and heat pain as a test stimulus; they found that both conditioning stimuli were able to induce CPM in their subjects.26 Our study evaluated only females, both with and without FM, and each of the two conditioning stimuli induced CPM in healthy controls.
A number of previous studies have identified attenuated CPM in the majority of FM patients,10–13,15,16 and this was corroborated by a meta-analysis that concluded that CPM is impaired in many chronic pain disorders.7 Some have suggested that CPM dysfunction is a pathogenic factor in the development of chronic pain.5–7 An alternative explanation for absent or reduced CPM in FM and similar chronic pain conditions is that CPM systems are already activated at baseline and cannot be increased further by noxious conditioning stimulation.28 Accordingly, FM may not be the result of dysfunctional CPM, but rather the cause of an overwhelmed CPM system operating at maximal output. In this study, we demonstrated that evaluating CPM by using pressure pain as both a conditioning and test stimulus can identify intact CPM in healthy subjects, as well as attenuated CPM in FM patients. It is important to note, however, that not every healthy control subject exhibited intact CPM, and not every FM patient exhibited attenuated CPM (Figure 2). Findings of both pain inhibition and pain facilitation within groups of individuals are not uncommon in studies of CPM,37,38 and reflect significant interindividual variability in endogenous pain control mechanisms.39
Interestingly, although there was no statistically significant difference in CPM magnitude between conditioning stimuli within the group of FM patients, CPM was numerically more efficient (ie, greater inhibition) with cold water conditioning. Cold water conditioning produced a net pain inhibitory effect (−7.57 NRS units), whereas pressure pain conditioning produced a net pain facilitatory effect (4.29 NRS units). This might be explained by the fact that FM patients in our study experienced the cold water as more painful than the pressure pain conditioning stimulus, and indeed several studies have suggested that more painful conditioning stimuli result in more robust endogenous pain inhibition.40–42 Additional evidence, however, suggests that increasing the intensity or perceived painfulness of conditioning stimulation (as long as it is initially perceived as painful) does not affect CPM magnitude, which may represent a ceiling effect,26,43,44 and these studies support our finding that the differences in CPM between conditioning stimuli in our study are not statistically significant. Nevertheless, it is worth noting that a group difference in CPM magnitude was only observed in this study with pressure pain conditioning. The reason for this is unknown but it may be related to small sample size, the potential influence of anxiety on pressure-based CPM testing,45 and/or the greater inhibitory effect of cold water conditioning in this group of FM patients relative to the controls.
Another intriguing aspect of this issue relates to the evolving understanding regarding mechanisms governing cold and cold pain sensation, such as the activation of the transient receptor potential cation channel, subfamily M, member 8 (TRPM8) and transient receptor potential cation channel, subfamily A, member 1 (TRPA1), respectively.46 These receptors, which play a complex role in the mediation of both cold-related pain and analgesia, are potential targets of pharmacological manipulation by various agonists and antagonists.47 Thus, the role played by medications used by FM patients in the current study, including pregabalin, must be kept in mind when evaluating the differences between the groups. Additional studies with larger sample sizes and measures of psychological factors will be necessary to more fully characterize the effect of conditioning stimulus type on detecting CPM differences between healthy controls and FM patients.
As previously described by Yarnitsky et al, assessing CPM may have clinical utility in patients suffering from chronic pain.9 Thus, in patients suffering from painful diabetic neuropathy, impaired CPM was shown to correlate with an improved clinical response to duloxetine, a serotonin–norepinephrine reuptake inhibitor (SNRI). This finding was interpreted as indicating that treatment with an SNRI could restore more efficient CPM, thus being particularly useful for patients with a baseline CPM impairment. Further elaborating on this notion, it has subsequently been proposed that experimental methods can be used to establish a pain modulation profile, based on the measurement of CPM as well as temporal summation, thus establishing a pain inhibitory/facilitatory balance; the assumption being that this pain phenotype may be used to position individuals on a pronociceptive/antinociceptive spectrum.39 While the link between impaired CPM and response to SNRIs has yet to be shown in FM, which is also frequently treated with this class of medication, a similar response would appear to be predictable, based on the frequency of CPM impairment among FM patients. In view of the notorious sensitivity of FM patients to side effects of medications (including SNRIs) and the less-than-optimal response to pharmacological treatments in general,48 it would be particularly useful to develop practical and simple methods for performing longitudinal CPM assessment among FM patients. Ideally, such methods implemented in the clinical setting might serve to guide patient-tailored treatment and reduce the rates of treatment failure, which are so typical of the trial-and-error strategy.49,50
The pressure paradigm presented in the current study does not require sophisticated and cumbersome equipment (eg, thermodes, hot/cold water vessels) and thus provides an easy-to-use standardized CPM-assessment method to be introduced into clinical practice. Additionally, the equipment utilized in the current study can easily be adapted for use in a magnetic resonance imaging (MRI) environment, thus facilitating neuroimaging research into the neurobiological correlates of CPM. Indeed, using a pneumatic piston controlled by a computerized system, we have been able to perform preliminary assessments of CPM during functional MRI (fMRI) (unpublished data). Such methods can be used both for evaluating brain responses to phasic pain stimuli,28,51 as well as identifying areas activated during CPM, and can be used for comparing patterns of brain activation during CPM among patients with chronic pain compared with healthy controls (see Figure S1 for examples of fMRI scanning performed during pressure-based CPM).
The neurobiological correlates of CPM in humans have begun to be explored by functional neuroimaging. A recent fMRI study in healthy individuals using a different CPM paradigm (electrical stimulation of the sural nerve as a test stimulus and cold water immersion of the contralateral foot as a conditioning stimulus) showed decreased activity during CPM in brain regions involved in pain processing, including the anterior cingulate cortex, supplementary motor area, primary somatosensory cortex, and insula.52 In a separate fMRI study, the right leg was surrounded on three sides by bags of ice water as a tonic conditioning stimulus while a fixed-temperature heat thermode (47.5°C) was applied to the left forearm as a phasic test stimulus.53 The authors observed significantly decreased activity in the insula, anterior cingulate cortex, thalamus, amygdala, and medulla during CPM. Subsequently, individual differences in CPM have been shown to be related to different levels of prefrontal cortical activation during the early part of the CPM stimulus, possibly due to different levels of anxiety.38 Interestingly, while performing CPM during fMRI scanning, we observed increased activation at the red nucleus area of the midbrain among healthy controls, but not among FM patients (Figure S1). Further research is necessary in order to elucidate the role of the midbrain as well as other areas involved in CPM and to distinguish between normal and pathological patterns of activation.
Conclusion
In summary, we have shown that noxious pressure applied to the thumbnail bed can be used as both a conditioning and test stimulus to evaluate CPM in FM patients and healthy controls. This paradigm was as effective at inducing CPM as a more established method using cold water hand immersion as a conditioning stimulus and pressure as a test stimulus. In contrast to other CPM paradigms that use either sophisticated and/or cumbersome test stimuli or very noxious conditioning stimuli that individuals – particularly those suffering from chronic pain – may be reluctant to undergo repeatedly, this paradigm to evaluate CPM can be performed longitudinally in nearly any setting with minimal participant burden.
Acknowledgments
The authors thank Dr Bradley Foerster for his neuroimaging expertise. We also thank Rachel K. Harrison for technical assistance, and Drs Daniel Harper and Andrew Schrepf for critical comments. This work was supported by Cooperative Agreement DAMD 17-002-0018.
Author contributions
CJS and JNA drafted the manuscript. CJS, LK, and SEH analyzed the psychophysical data. RB analyzed the fMRI data. EI collected behavioral data and helped to analyze the fMRI data. REH helped to analyze the fMRI data. DJC participated in the conception and design of the study. RHG and SEH conceived of and designed the study. All authors contributed toward data analysis, drafting and revising the paper and agree to be accountable for all aspects of the work.
Disclosure
The authors would like to disclose that REH and SEH have received consulting fees from Pfizer Inc. SEH has also worked as a consultant for Analgesic Solutions, Aptinyx, and deCode Genetics, received research funding from Cerephex, Eli Lily, Forest Laboratories, and Merck, and is a member of Arbor Medical Innovations, LLC (Ann Arbor, MI). The authors report no further conflicts of interest in this work.
References
Pud D, Granovsky Y, Yarnitsky D. The methodology of experimentally induced diffuse noxious inhibitory control (DNIC)-like effect in humans. Pain. 2009;144(1–2):16–19. | ||
Nir RR, Yarnitsky D. Conditioned pain modulation. Curr Opin Support Palliat Care. 2015;9(2):131–137. | ||
Yarnitsky D, Arendt-Nielsen L, Bouhassira D, et al. Recommendations on terminology and practice of psychophysical DNIC testing. Eur J Pain. 2010;14(4):339. | ||
Yarnitsky D, Bouhassira D, Drewes AM, et al. Recommendations on practice of conditioned pain modulation (CPM) testing. Eur J Pain. 2015;19(6):805–806. | ||
Edwards RR. Individual differences in endogenous pain modulation as a risk factor for chronic pain. Neurology. 2005;65(3):437–443. | ||
Yarnitsky D. Conditioned pain modulation (the diffuse noxious inhibitory control-like effect): its relevance for acute and chronic pain states. Curr Opin Anaesthesiol. 2010;23(5):611–615. | ||
Lewis GN, Rice DA, McNair PJ. Conditioned pain modulation in populations with chronic pain: a systematic review and meta-analysis. J Pain. 2012;13(10):936–944. | ||
Yarnitsky D, Crispel Y, Eisenberg E, et al. Prediction of chronic post-operative pain: pre-operative DNIC testing identifies patients at risk. Pain. 2008;138(1):22–28. | ||
Yarnitsky D, Granot M, Nahman-Averbuch H, Khamaisi M, Granovsky Y. Conditioned pain modulation predicts duloxetine efficacy in painful diabetic neuropathy. Pain. 2012;153(6):1193–1198. | ||
Lautenbacher S, Rollman GB. Possible deficiencies of pain modulation in fibromyalgia. Clin J Pain. 1997;13(3):189–196. | ||
Potvin S, Larouche A, Normand E, et al. No relationship between the ins del polymorphism of the serotonin transporter promoter and pain perception in fibromyalgia patients and healthy controls. Eur J Pain. 2010;14(7):742–746. | ||
Kosek E, Hansson P. Modulatory influence on somatosensory perception from vibration and heterotopic noxious conditioning stimulation (HNCS) in fibromyalgia patients and healthy subjects. Pain. 1997;70(1):41–51. | ||
Normand E, Potvin S, Gaumond I, Cloutier G, Corbin JF, Marchand S. Pain inhibition is deficient in chronic widespread pain but normal in major depressive disorder. J Clin Psychiatry. 2011;72(2):219–224. | ||
Ge HY, Nie H, Graven-Nielsen T, Danneskiold-Samsoe B, Arendt-Nielsen L. Descending pain modulation and its interaction with peripheral sensitization following sustained isometric muscle contraction in fibromyalgia. Eur J Pain. 2012;16(2):196–203. | ||
Jensen KB, Kosek E, Petzke F, et al. Evidence of dysfunctional pain inhibition in fibromyalgia reflected in rACC during provoked pain. Pain. 2009;144(1–2):95–100. | ||
Julien N, Goffaux P, Arsenault P, Marchand S. Widespread pain in fibromyalgia is related to a deficit of endogenous pain inhibition. Pain. 2005;114(1–2):295–302. | ||
Le Bars D. The whole body receptive field of dorsal horn multireceptive neurones. Brain Res Brain Res Rev. 2002;40(1–3):29–44. | ||
Le Bars D, Dickenson AH, Besson JM. Diffuse noxious inhibitory controls (DNIC). I. Effects on dorsal horn convergent neurones in the rat. Pain. 1979;6(3):283–304. | ||
Le Bars D, Dickenson AH, Besson JM. Diffuse noxious inhibitory controls (DNIC). II. Lack of effect on non-convergent neurones, supraspinal involvement and theoretical implications. Pain. 1979;6(3):305–327. | ||
Graven-Nielsen T, Babenko V, Svensson P, Arendt-Nielsen L. Experimentally induced muscle pain induces hypoalgesia in heterotopic deep tissues, but not in homotopic deep tissues. Brain Res. 1998;787(2):203–210. | ||
Arendt-Nielsen L, Sluka KA, Nie HL. Experimental muscle pain impairs descending inhibition. Pain. 2008;140(3):465–471. | ||
Edwards RR, Grace E, Peterson S, Klick B, Haythornthwaite JA, Smith MT. Sleep continuity and architecture: associations with pain-inhibitory processes in patients with temporomandibular joint disorder. Eur J Pain. 2009;13(10):1043–1047. | ||
Goodin BR, McGuire L, Allshouse M, et al. Associations between catastrophizing and endogenous pain-inhibitory processes: sex differences. J Pain. 2009;10(2):180–190. | ||
Locke D, Gibson W, Moss P, Munyard K, Mamotte C, Wright A. Analysis of meaningful conditioned pain modulation effect in a pain-free adult population. J Pain. 2014;15(11):1190–1198. | ||
Wolfe F, Smythe HA, Yunus MB, et al. The American College of Rheumatology 1990 criteria for the classification of fibromyalgia. Report of the Multicenter Criteria Committee. Arthritis Rheum. 1990;33(2):160–172. | ||
Granot M, Weissman-Fogel I, Crispel Y, et al. Determinants of endogenous analgesia magnitude in a diffuse noxious inhibitory control (DNIC) paradigm: do conditioning stimulus painfulness, gender and personality variables matter? Pain. 2008;136(1–2):142–149. | ||
Henry NL, Conlon A, Kidwell KM, et al. Effect of estrogen depletion on pain sensitivity in aromatase inhibitor-treated women with early-stage breast cancer. J Pain. 2014;15(5):468–475. | ||
Gracely RH, Petzke F, Wolf JM, Clauw DJ. Functional magnetic resonance imaging evidence of augmented pain processing in fibromyalgia. Arthritis Rheum. 2002;46(5):1333–1343. | ||
Giesecke T, Williams DA, Harris RE, et al. Subgrouping of fibromyalgia patients on the basis of pressure-pain thresholds and psychological factors. Arthritis Rheum. 2003;48(10):2916–2922. | ||
Petzke F, Harris RE, Williams DA, Clauw DJ, Gracely RH. Differences in unpleasantness induced by experimental pressure pain between patients with fibromyalgia and healthy controls. Eur J Pain. 2005;9(3):325–335. | ||
Giesecke J, Reed BD, Haefner HK, Giesecke T, Clauw DJ, Gracely RH. Quantitative sensory testing in vulvodynia patients and increased peripheral pressure pain sensitivity. Obstet Gynecol. 2004;104(1):126–133. | ||
Petzke F, Clauw DJ, Ambrose K, Khine A, Gracely RH. Increased pain sensitivity in fibromyalgia: effects of stimulus type and mode of presentation. Pain. 2003;105(3):403–413. | ||
Harris RE, Gracely RH, McLean SA, et al. Comparison of clinical and evoked pain measures in fibromyalgia. J Pain. 2006;7(7):521–527. | ||
Geisser ME, Glass JM, Rajcevska LD, et al. A psychophysical study of auditory and pressure sensitivity in patients with fibromyalgia and healthy controls. J Pain. 2008;9(5):417–422. | ||
As-Sanie S, Harris RE, Harte SE, Tu FF, Neshewat G, Clauw DJ. Increased pressure pain sensitivity in women with chronic pelvic pain. Obstet Gynecol. 2013;122(5):1047–1055. | ||
Petzke F, Khine A, Williams D, Groner K, Clauw DJ, Gracely RH. Dolorimetry performed at 3 paired tender points highly predicts overall tenderness. J Rheumatol. 2001;28(11):2568–2569. | ||
Potvin S, Marchand S. Pain facilitation and pain inhibition during conditioned pain modulation in fibromyalgia. Pain. 2016;157(8):1704–1710. | ||
Bogdanov VB, Vigano A, Noirhomme Q, et al. Cerebral responses and role of the prefrontal cortex in conditioned pain modulation: an fMRI study in healthy subjects. Behav Brain Res. 2015;281:187–198. | ||
Yarnitsky D, Granot M, Granovsky Y. Pain modulation profile and pain therapy: between pro- and antinociception. Pain. 2014;155(4):663–665. | ||
Le Bars D, Chitour D, Clot AM. The encoding of thermal stimuli by diffuse noxious inhibitory controls (DNIC). Brain Res. 1981;230(1–2):394–399. | ||
Willer JC, Roby A, Le Bars D. Psychophysical and electrophysiological approaches to the pain-relieving effects of heterotopic nociceptive stimuli. Brain. 1984;107(Pt 4):1095–1112. | ||
Willer JC, De Broucker T, Le Bars D. Encoding of nociceptive thermal stimuli by diffuse noxious inhibitory controls in humans. J Neurophysiol. 1989;62(5):1028–1038. | ||
Nir RR, Granovsky Y, Yarnitsky D, Sprecher E, Granot M. A psychophysical study of endogenous analgesia: the role of the conditioning pain in the induction and magnitude of conditioned pain modulation. Eur J Pain. 2011;15(5):491–497. | ||
Nir RR, Yarnitsky D, Honigman L, Granot M. Cognitive manipulation targeted at decreasing the conditioning pain perception reduces the efficacy of conditioned pain modulation. Pain. 2012;153(1):170–176. | ||
Nahman-Averbuch H, Nir RR, Sprecher E, Yarnitsky D. Psychological factors and conditioned pain modulation: a meta-analysis. Clin J Pain. 2016;32(6):541–554. | ||
Olsen RV, Andersen HH, Møller HG, Eskelund PW, Arendt-Nielsen L. Somatosensory and vasomotor manifestations of individual and combined stimulation of TRPM8 and TRPA1 using topical L-menthol and trans-cinnamaldehyde in healthy volunteers. Eur J Pain. 2014;18(9):1333–1342. | ||
McKemy DD. Therapeutic potential of TRPM8 modulators. Open Drug Discov J. 2010;2(1):81–88. | ||
Hauser W, Walitt B, Fitzcharles MA, Sommer C. Review of pharmacological therapies in fibromyalgia syndrome. Arthritis Res Ther. 2014;16(1):201. | ||
Ablin JN, Buskila D. Personalized treatment of pain. Curr Rheumatol Rep. 2013;15(1):298. | ||
Cruz-Almeida Y, Fillingim RB. Can quantitative sensory testing move us closer to mechanism-based pain management? Pain Med. 2014;15(1):61–72. | ||
Ichesco E, Puiu T, Hampson JP, et al. Altered fMRI resting-state connectivity in individuals with fibromyalgia on acute pain stimulation. Eur J Pain. 2016;20(7):1079–1089. | ||
Piche M, Arsenault M, Rainville P. Cerebral and cerebrospinal processes underlying counterirritation analgesia. J Neurosci. 2009;29(45):14236–14246. | ||
Sprenger C, Bingel U, Buchel C. Treating pain with pain: supraspinal mechanisms of endogenous analgesia elicited by heterotopic noxious conditioning stimulation. Pain. 2011;152(2):428–439. |
Supplementary material
 | Figure S1 Pressure-based CPM during functional magnetic resonance imaging. Notes: A comparison of BOLD signal pattern during a CPM scan (moderately painful pressure test stimulus and conditioning stimulus applied concurrently to both thumbnails) to that obtained during a baseline scan (test stimulus alone applied to one thumbnail), revealed a significant effect of conditioning stimulation in female healthy controls (n=10) in the left red nucleus (x=−5, y=−14, Z=4.27, corrected, P<0.01), contralateral to the conditioning stimulus. Abbreviations: CPM, conditioned pain modulation; min, minutes; sec, seconds. |
 © 2016 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2016 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.