Back to Journals » International Journal of Women's Health » Volume 18
A Novel Nomogram for Predicting Gonadotropin-Releasing Hormone Analogue Treatment Outcome in Girls with Idiopathic Central Precocious Puberty
Authors Xu S, Guan L, Lin Q, Liu H
Received 29 September 2025
Accepted for publication 9 December 2025
Published 24 January 2026 Volume 2026:18 564053
DOI https://doi.org/10.2147/IJWH.S564053
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Matteo Frigerio
Shiyi Xu,1 Limei Guan,1,2 Qiuting Lin,1 Hui Liu1,2
1College of Clinical Medicine for Obstetrics and Gynecology and Pediatrics, Fujian Medical University, Fuzhou, 350000, People’s Republic of China; 2Department of Endocrinology and Inborn Metabolic Diseases, Fujian Children’s Hospital (Fujian Branch of Shanghai Children’s Medical Center), Fuzhou, 350014, People’s Republic of China
Correspondence: Hui Liu, College of Clinical Medicine for Obestetrics and Gynecology and Pediatrics, Fujian Medical University, No. 18 Daoshan Road, Gulou District, Fuzhou, 350000, People’s Republic of China, Email [email protected]
Objective: To explore the nomogram prediction model of long-acting gonadotropin-releasing hormone analogue (GnRHa) based on the clinical characteristics, bone metabolism and ovarian function of girls with idiopathic central precocious puberty (ICPP) and its clinical application value.
Methods: A total of 134 girls with ICPP who received long-term GnRHa treatment at our hospital from May 2021 to February 2024 were selected and randomly divided into a training set (n=94) and a validation set (n=40) in a 7:3 ratio. In the training set, univariate analysis and multivariate logistic regression analyses were used to identify factors influencing treatment efficacy, based on which a nomogram prediction model was constructed. The model’s predictive performance was evaluated using the receiver operating characteristic (ROC) curve and calibration curve, while its clinical application value was assessed by decision curve analysis (DCA).
Results: In the training set, 18 out of 94 children (19.15%) had a poor treatment response, compared to 7 out of 40 children (17.50%) in the validation set. Multivariate regression analysis showed that the higher degree of breast development, more pubic hair growth, higher level of N-MID, higher level of ALP, larger ovarian volume, more follicles, and higher levels of LH, FSH and E2 were the independent risk factors for poor curative effect of GnRHa (all P< 0.05). The constructed nomogram demonstrated good predictive performance in both sets: the area under the ROC curve (AUC) was 0.870 (95% CI: 0.814– 0.927) in the training set and 0.810 (95% CI: 0.711– 0.909) in the validation set. Calibration curves showed good agreement between predicted and observed outcomes. DCA indicated that the model provided net clinical benefit across a wide threshold probability range (approximately 0.1– 0.8).
Conclusion: Based on the clinical characteristics, bone metabolism and ovarian function of girls with idiopathic central precocious puberty, the nomogram prediction model of long-acting gonadotropin-releasing hormone analogues is helpful to predict the curative effect of GnRHa at an early stage, guide clinical decision-making and optimize the treatment plan.
Keywords: idiopathic central precocious puberty, girls, gonadotropin releasing hormone analogue, alignment chart, therapeutic effect prediction
Introduction
Idiopathic central precocious puberty (ICPP), as a common disease in the field of pediatric endocrinology, has a far-reaching impact on girls’ physical and mental health. Usually, if girls show signs of premature development of secondary sexual characteristics before the age of 8, such as abnormal breast bulge or premature growth of pubic hair, it is highly suggested that they may have ICPP.1 The root of this disease can be traced back to the premature and abnormal activation of hypothalamus-pituitary-gonad axis (HPGA) function, which broke the normal growth and development rhythm. Failure to effectively intervene in ICPP in time will lead to a series of serious consequences.2 From the perspective of height, the height of children in adulthood may be significantly damaged, and the normal genetic height potential cannot be achieved. In the field of psychological behavior, children may feel inferior and anxious because of their different physical development from their peers, which will affect their social skills and academic performance.3 More seriously, from the long-term health point of view, the risk of children suffering from chronic diseases such as metabolic syndrome and cardiovascular disease will also increase greatly in adulthood. At present, GnRHa was recommended as the first-line therapy for ICPP in the Clinical Practice Guidelines of the Pediatric Endocrine Society and played a dominant role in ICPP treatment, as it can effectively inhibit HPGA activation to delay sexual development and preserve adult height potential.4 Its main mechanism is to inhibit the functional activities of HPGA, so as to delay the sexual development process and create favorable conditions for improving the adult height of children.5 However, in practical clinical application, after receiving GnRHa treatment, the curative effect of ICPP girls shows significant differences among different individuals, and some children fail to achieve ideal therapeutic effect. In view of this, it is particularly critical to accurately predict the therapeutic effect of GnRHa as soon as possible. This treatment method not only provides a basis for doctors, so that they can accurately adjust the treatment plan according to the individual situation of children and select more appropriate drug dosage and course of treatment, but also can effectively reduce unnecessary side effects of drugs and minimize the treatment cost while improving the treatment effect, so as to finally realize individualized and accurate treatment of ICPP girls and ensure their healthy growth. Previous prediction models for GnRHa outcome in ICPP have primarily relied on clinical and basic hormonal parameters. While valuable, these models often overlook the significant role of bone metabolism in the disease progression and treatment response. Our novel nomogram incorporates key bone metabolism markers alongside comprehensive clinical characteristics and ovarian function indices, providing a more holistic predictive tool. This integration is the key novel aspect of our model, potentially offering improved accuracy for identifying patients at risk of poor treatment outcomes.
Materials and Methods
Study Population
34 ICPP girls who received long-term treatment with GnRHa in our hospital from May 2021 to February 2024 were selected as the research objects. Inclusion criteria: (1) Meet the diagnostic criteria of ICPP;6 (2) The first treatment with GnRHa; (3) The clinical data were complete before and during the treatment. Exclusion criteria: (1) Combined with other endocrine diseases, such as hyperthyroidism; (2) Suffering from serious systemic diseases, such as hepatic and renal insufficiency and malignant tumor; (3) recent use of drugs that affect sexual development or bone metabolism; (4) unable to cooperate to complete the treatment and follow-up; (5) incomplete medical records or missing data The flow of patient selection and group allocation was summarized in Supplementary Figure 1. This study was approved by the Ethics Committee of the Fujian Children’s Hospital (approval number: 2024ETKLRK09007), and all parents of the affected children signed informed consent forms.
Clinical Data Collection
The clinical characteristics, bone metabolism and ovarian function indexes of the children were collected, including basic information such as age, height, weight, BMI and onset age. Evaluate the degree of breast development (according to Tanner stage) and pubic hair growth (according to Tanner stage); Bone metabolism indexes were detected, including N-MID, alkaline phosphatase (ALP) and so on. X-ray bone age of left wrist was measured regularly before and during treatment, and bone age was evaluated by G-P atlas. The ovarian volume, the size and number of follicles were measured by ultrasound. The levels of sex hormones such as luteinizing hormone (LH), follicle stimulating hormone (FSH) and estradiol (E2) were detected. Hormone levels (LH, FSH, E2) were measured using chemiluminescence immunoassay on a Cobas e801 analyzer (Roche Diagnostics, Germany). Bone metabolism markers N-MID and ALP were assessed by electrochemiluminescence immunoassay on the same platform. Ovarian volume and follicle count were measured by transabdominal ultrasound using a Voluson E8 system (GE Healthcare, USA) with a 4–8 MHz convex transducer, following a standardized protocol where the volume was calculated using the prolate ellipsoid formula (length × height × width × 0.523). Bone age was assessed independently by two experienced pediatric endocrinologists using the Greulich-Pyle atlas; discrepancies were resolved by consensus.
Evaluation of Curative Effect
All the children who participated in the study received GnRHa long-acting drug therapy, and the dose was adjusted according to the weight of the children, and was injected once every 4 weeks. The curative effect is good: after 6 months of treatment, the growth rate of children’s height reached or exceeded the 25th percentile of normal children of the same age and gender, and the growth rate of bone age slowed down obviously, which was close to that of normal children (the growth rate of bone age was less than 0.5 years after 6 months). According to Tanner staging standard, the development of children’s breasts showed signs of decline, while the growth of pubic hair showed an improvement trend, and LH and FSH promoted glands. On the contrary, it is poor curative effect.
Statistical Analysis
SPSS 26.0 and R 3.6.3 software were used for data analysis. For the comparative analysis of counting data, chi-square (χ2) test method is adopted; For the measurement data, if it conforms to the normal distribution, it is expressed in the form of mean standard deviation (S), and the differences between the two groups are compared by independent sample t-test. Only patients with complete data on all predictor variables and outcomes were included; therefore, there were no missing data in the final analytical cohort. In order to screen out the unfavorable factors affecting the curative effect, univariate analysis and multivariate Logistic regression analysis were carried out, and their odds ratios (OR) and 95% confidence intervals (CI) were calculated. The nomogram model was constructed by using the “rms” package of R software. The receiver operating characteristic (ROC) curve was plotted, and the area under the curve (AUC) value was calculated. The consistency index (C-index) of the model was calculated, and calibration curve was plotted and evaluated using the Hosmer-Lemeshow goodness-of-fit test. To mitigate risk of model overfitting, we employed bootstrap internal validation with 1000 resamples. The optimism-corrected performance metrics were reported alongside the apparent performance. Decision curve analysis (DCA) was used to evaluate the clinical application value of the nomogram by calculating the net benefit at different threshold probabilities. A P value < 0.05 was considered statistically significant.
Results
Comparison of Clinical Data Between Training Set and Validation Set
A total of 134 girls with ICPP who received long-term GnRHa treatment were selected, and randomly divided into a training set (n=94) and a validation set (n=40). There was no significant difference in clinical data between the training group and the validation group (P>0.05) (Table 1).
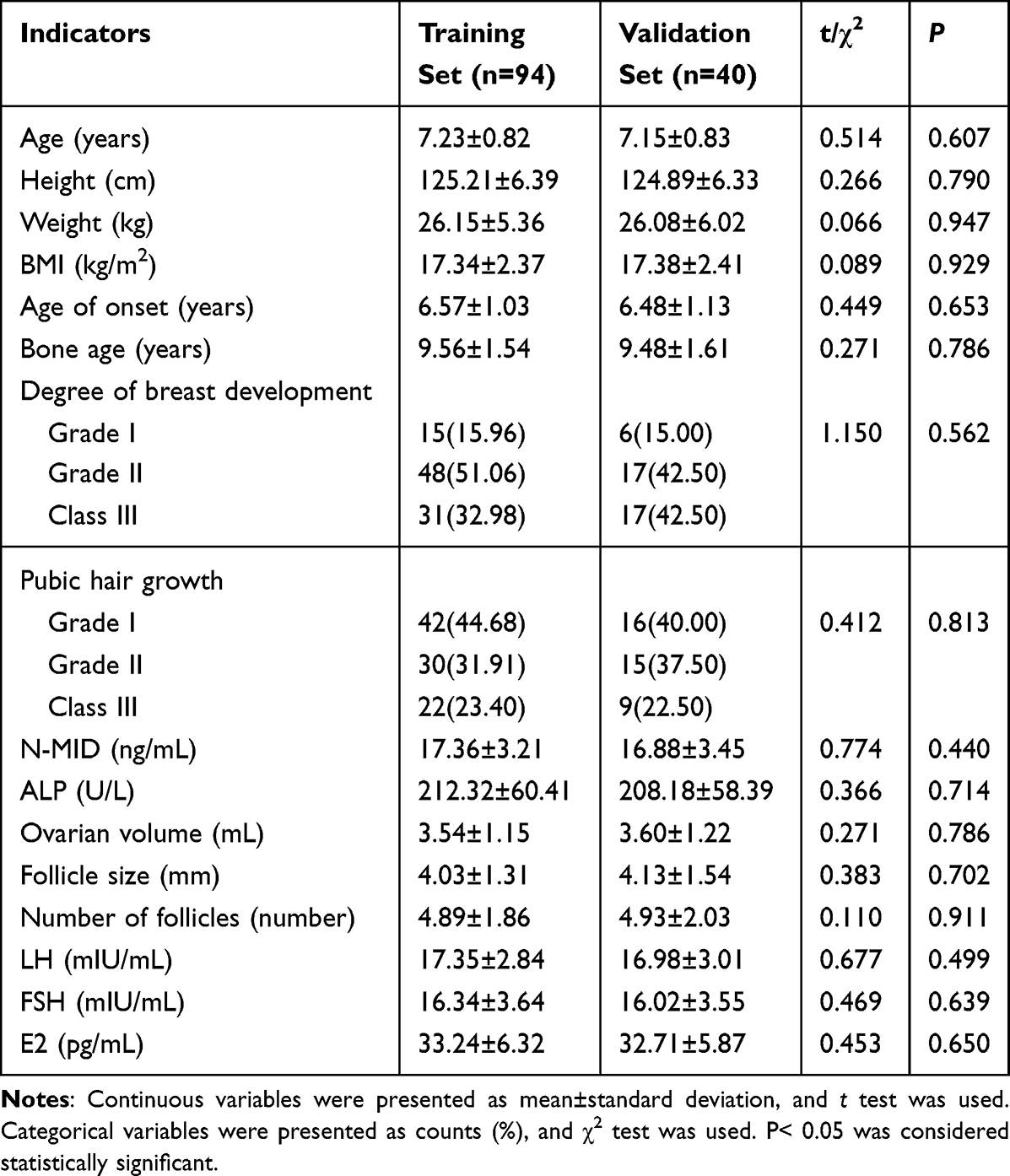 |
Table 1 Comparison of Clinical Data Between Training Set and Validation Set |
Analysis of Risk Factors of Poor Curative Effect of Training Set
18 cases (19.15%) of 94 children in the training set had poor curative effect, and 7 cases (17.50%) of 40 children in the validation set had poor curative effect. Univariate analysis showed that there were significant differences in breast development, pubic hair growth, N-MID, ALP, ovarian volume, number of follicles, LH, FSH and E2 levels among different therapeutic groups (all P<0.05) (Table 2). Taking the curative effect as the dependent variable (0= good curative effect, 1 = poor curative effect), and taking the factors in the univariate analysis as the covariate (Table 3), the multivariate Logistic regression analysis was further carried out. Greater breast development, more pubic hair growth, higher N-MID level, higher ALP level, larger ovarian volume, more follicles, and higher LH, FSH and E2 levels were independent risk factors for poor curative effect of GnRHa (all P<0.05) (Table 4). In the regression model, the tolerance of each variable, the VIF and the conditional index are all < 0.1.
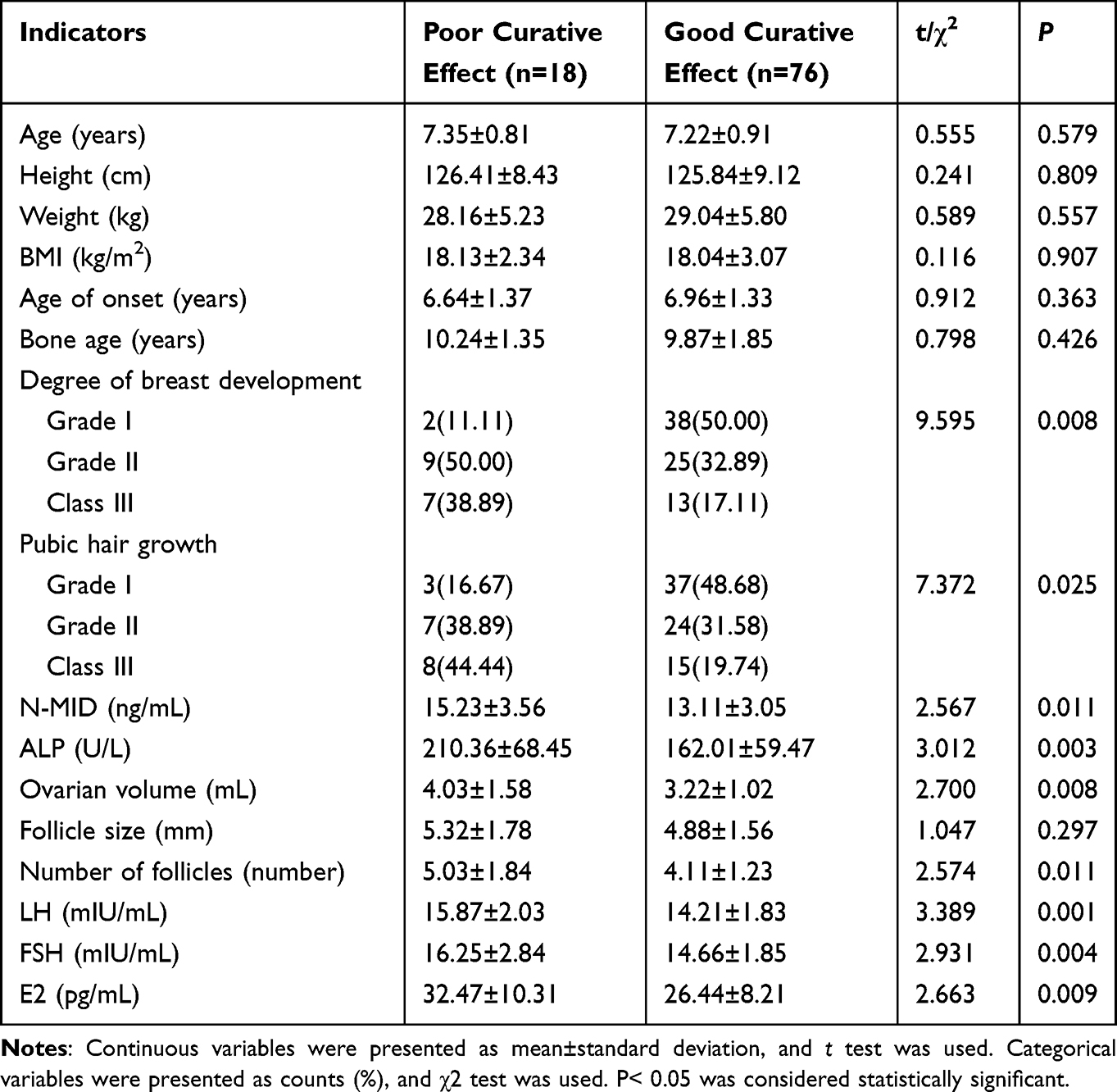 |
Table 2 Univariate Analysis of Poor Curative Effect in Training Group |
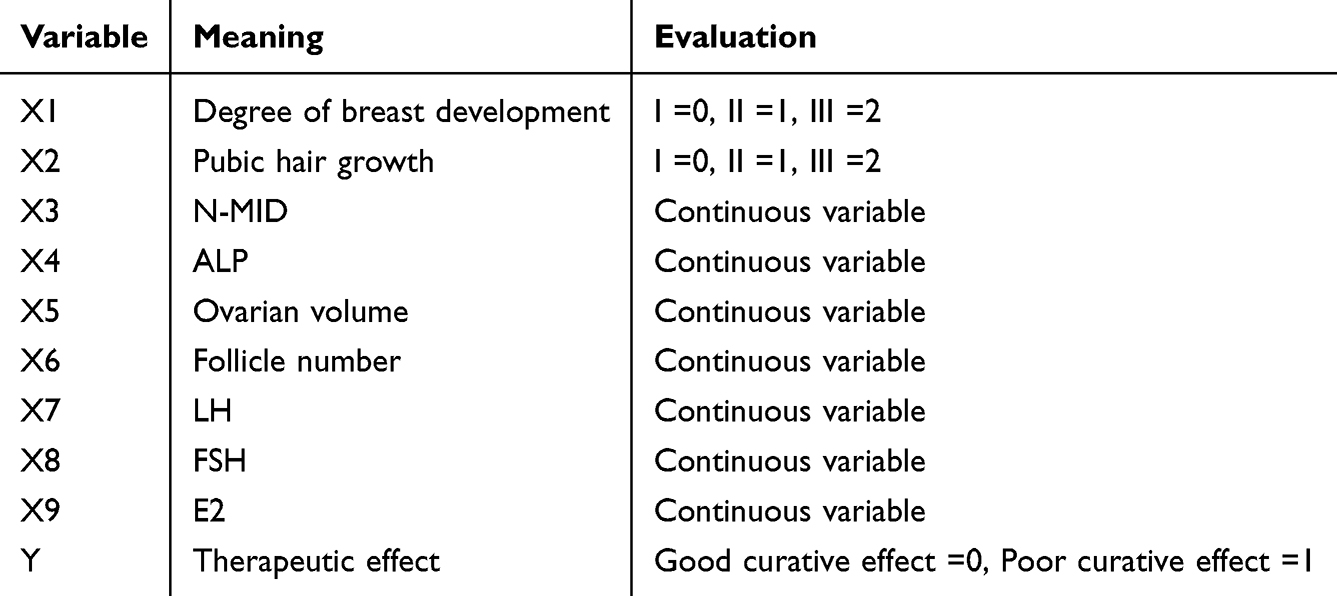 |
Table 3 Variable Assignment Method |
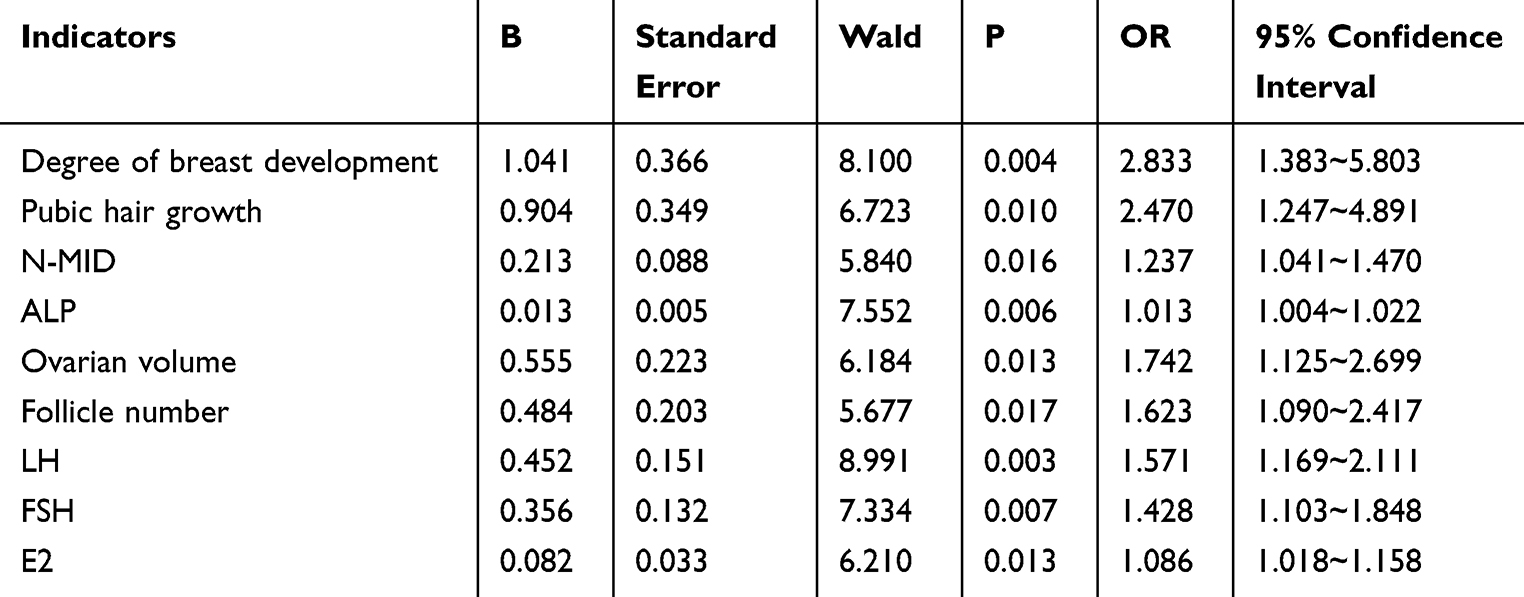 |
Table 4 Multivariate Logistic Regression Analysis of Poor Efficacy in Training Set |
Development of GnRHa Curative Effect Nomogram Prediction Model
According to the independent risk factors determined by multivariate Logistic regression analysis, a nomogram prediction model for the therapeutic effect of GnRHa is constructed, and each independent risk factor involved in the model is quantitatively assigned, and the total score for predicting the poor curative effect is calculated and reflected by the probability of predicting the poor curative effect. The higher the total score, the higher the accuracy of predicting the poor curative effect of GnRHa (Figure 1).
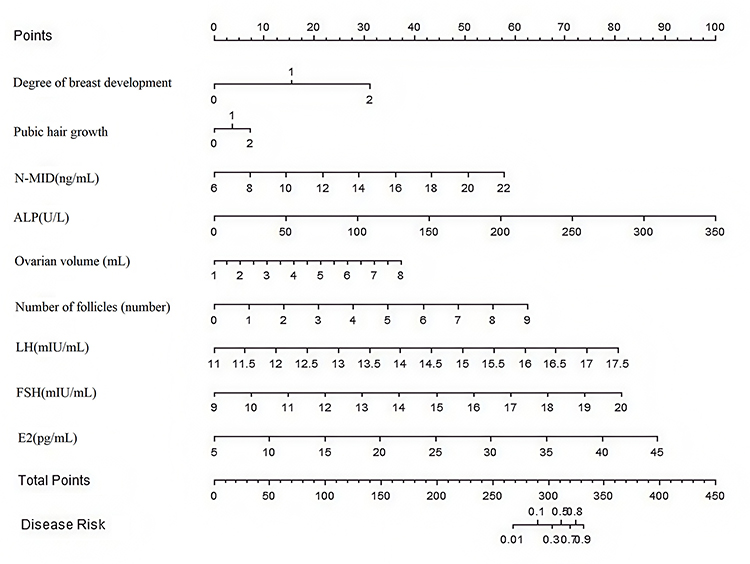 |
Figure 1 GnRHa curative effect nomogram prediction model. |
Evaluation and Validation of GnRHa Curative Effect Nomogram Prediction Model
In the training set and validation set, the apparent C-index of the nomogram model was 0.979 and 0.747, respectively. Bootstrap internal validation yielded bias-corrected C-index values of 0.872 for the training set and 0.812 for the validation set. The calibration curve showed a mean absolute error between predicted and actual values of 0.045 and 0.189, respectively. The Hosmer-Lemeshow test indicated good calibration in the training set (χ2=5.065, df=8, p=0.751) but suggested some miscalibration in the validation set (χ2=10.375, df=8, p =0.126) (Figure 2). The ROC curve analysis showed that the AUC for predicting poor GnRHa response was 0.870 (95% CI: 0.814–0.927) in the training set and 0.810 (95% CI: 0.711–0.909) in the validation set (Figure 3). At the optimal cutoff, sensitivity was 1.000 (95% CI: 0.82–1.00) and specificity was 0.889 (95% CI: 0.76–0.96) in the training set. In the validation set, sensitivity was 0.667 (95% CI: 0.30–0.93) and specificity was 0.773 (95% CI: 0.61–0.89). Internal validation using bootstrap resampling provided more realistic performance estimates, with bias-corrected C-index values of 0.872 and 0.812 for the training and validation sets, respectively.
 |
Figure 2 Calibration curves (A) training set, (B) validation set. |
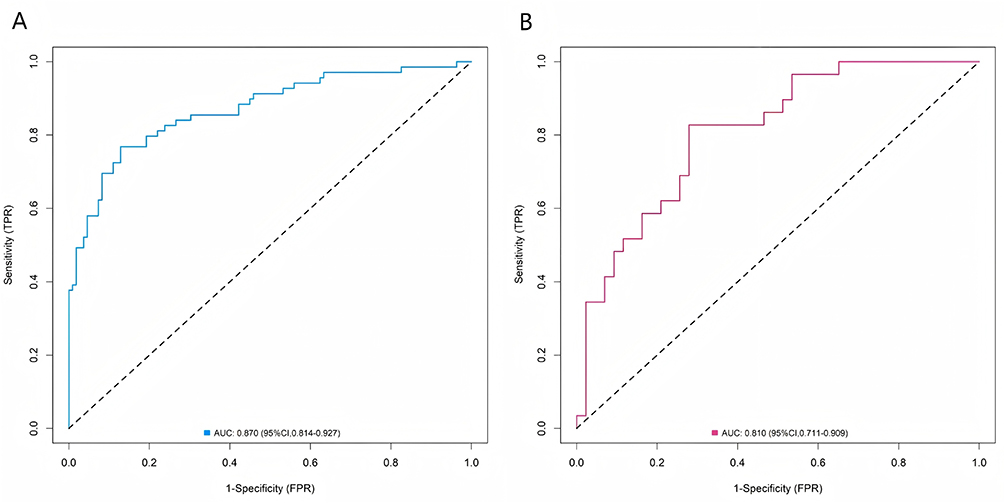 |
Figure 3 Receiver operating characteristic curves (A) training set, (B) validation set. |
Decision Curve Analysis of GnRHa Curative Effect Nomogram Prediction Model
The decision curve shows that when the threshold probability is about 0.1–0.8, the decision to predict the curative effect of GnRHa by using the nomogram model constructed in this study has more clinical benefits than the decision to think that all of them are effective or none of them are effective before operation (Figure 4).
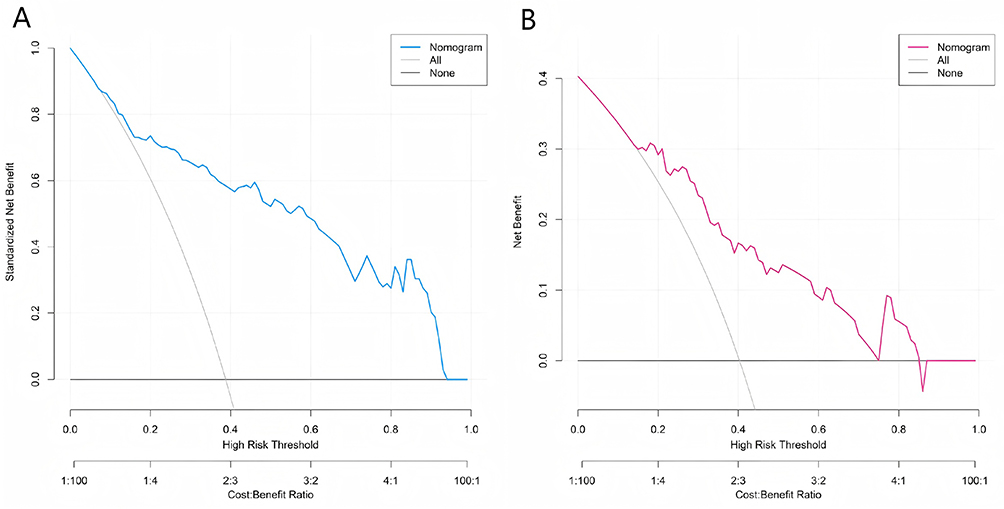 |
Figure 4 Decision curves (A) training set, (B) validation set. |
Discussion
In this study, the results showed that the model has high prediction performance in both training data sets and validation data sets, and provides a powerful tool for early prediction of the curative effect of GnRHa, guiding clinical decision-making and optimizing treatment plans.
Correlation of Predictors with GnRHa Efficacy
As an important manifestation of the clinical characteristics of girls with precocious puberty, the degree of breast development and pubic hair growth have been proved to be independent risk factors for poor curative effect of GnRHa in this study. The development of breast and pubic hair is serious, which reflects the strong role of sex hormones in children, and the shafting activation from hypothalamus to pituitary gland to gonad shows a high level. This may make GnRHa face greater challenges in inhibiting the function of this axis, because it needs to fight against the already active endocrine environment.7 For example, in a girl whose breast development reaches TannerIII stage, the estrogen content in her body is maintained at a high level, which continuously stimulates the breast tissue. Even if GnRHa is used for treatment, the regression of breast development may be slow, thus affecting the overall treatment effect.8 The higher levels of N-MID and ALP are closely related to the poor curative effect of GnRHa. N-MID is a metabolite of osteocalcin, which is mainly synthesized by osteoblasts. The increase of concentration often means the improvement of osteoblast activity and the acceleration of bone turnover rate.9 ALP is also a key index to evaluate osteoblast function and bone metabolism activity. In the group of female children with precocious puberty, abnormal bone metabolism activity accelerates the process of bone maturation, which not only leads to the early development of bone age, but also makes it more difficult for GnRHa to control the progress of bone age.10 For example, high ALP level may mean too fast bone renewal. Even if GnRHa inhibits some effects of sex hormones on bones, the overactivity of osteoblasts may still promote the growth of bone age and affect the final height improvement.11 The related indexes of ovarian function, such as larger ovarian volume, more follicles and higher levels of LH, FSH and E2, are all risk factors for poor curative effect. Ovary is an important organ for producing sex hormones, and its premature activation plays a key role in ICPP. The larger ovarian volume and more follicles indicate that the ovary is in a relatively active state and continuously secretes more sex hormones.12 The increase of LH and FSH directly stimulates the ovary to secrete sex hormones such as E2, and the high level of E2 further promotes the development of secondary sexual characteristics and bone maturation. For example, a higher E2 level will accelerate epiphyseal closure, shorten the time window of height growth, and make it difficult to effectively control the development of sexual characteristics under GnRHa treatment, thus affecting the treatment effect.13
Performance of the Model
Based on the above factors, this study is committed to building a nomogram prediction model for the therapeutic effect of GnRHa. ROC curve analysis showed that the AUC of the nomogram model for predicting poor GnRHa efficacy was 0.870 (95% CI: 0.814–0.927) in the training set and 0.810 (95% CI: 0.711–0.909) in the validation set. Internal validation using bootstrap resampling provided more realistic performance estimates, with bias-corrected C-index values of 0.872 and 0.812 for the training and validation sets, respectively. The model demonstrated excellent calibration in the training set (Hosmer-Lemeshow p=0.751), though some miscalibration was observed in the validation set (p=0.126), which may reflect the limited sample size and should be addressed in future external validation studies. DCA showed that when the high-risk threshold was approximately 0.1–0.8, the decision to predict the curative effect of GnRHa using the nomogram model constructed in this study provided more clinical benefit than the strategies of treating all patients or none. Given the limited number of events, the precision of coefficient estimates should be interpreted with caution. Bootstrap resampling (n=1000) indicated generally stable distributions for the included variables, supporting the model’s internal validity despite the low EPV. This discovery emphasizes the key role of nomogram prediction model in clinical decision-making, which provides valuable reference information for doctors, so that doctors can predict the therapeutic effect of GnRHa in the early stage of the disease, and then optimize the treatment strategy and improve the overall curative effect.
Clinical Application of the Model
In practical clinical application, doctors can make personalized treatment plans for ICPP girls according to the output of nomogram prediction model. For those girls whose predicted curative effect is ideal, the existing GnRHa treatment scheme can be maintained unchanged, and the changes of the condition can be closely monitored; For girls with poor predicted curative effect, it is necessary to consider adjusting the treatment plan, such as increasing drug dosage, prolonging treatment time or adopting other treatment methods, in order to achieve better therapeutic effect.14 Many previous studies have also paid attention to the influencing factors of the therapeutic effect of GnRHa in ICPP girls, which is consistent with the results of this study. Some studies have also found that breast development, bone metabolism and ovarian function are related to the curative effect. For example, it has been reported that the height growth of girls with higher stages of breast development may be limited after GnRHa treatment, which is consistent with the conclusion that the degree of breast development is a risk factor for poor curative effect in this study. In the aspect of bone metabolism, other studies have also confirmed that the abnormal bone turnover index is closely related to the bone development and therapeutic effect of children with precocious puberty, and the results of N-MID and ALP in this study further support this view.15 As for ovarian function, previous studies have also shown that premature ovarian activation and abnormal sex hormone levels have adverse effects on the treatment outcome, which is consistent with the findings of ovarian volume, follicle number and sex hormone level in this study. However, compared with previous studies, the nomogram model constructed in this study may be different in specific variable selection and model performance. Factors such as case characteristics, sample size, detection methods and model construction methods included in different studies.Can lead to different results. For example, some studies may include more clinical indicators or adopt different statistical analysis methods, thus constructing slightly different prediction models.
Clinical Management Implications
The proposed nomogram has the potential to influence clinical management by enabling early identification of ICPP girls at high risk for a poor response to GnRHa. For such patients, clinicians might consider more intensive monitoring, dose adjustment of GnRHa within the approved range, or earlier initiation of combination therapy (eg, with growth hormone) if indicated, to optimize growth outcomes. Conversely, for patients predicted to have a good response, the model could reinforce confidence in the standard treatment protocol, potentially reducing unnecessary interventions or anxieties.
In addition, the model can also be used to evaluate the curative effect regularly during the treatment, and adjust the treatment strategy in time according to the actual situation to achieve the best treatment effect. From the point of view of clinical research, this model provides new ideas and methods for further study on the pathogenesis and treatment strategy of ICPP. By identifying the risk factors of poor curative effect, we can carry out basic and clinical research and explore new therapeutic targets and drugs. In the aspect of medical resource allocation, the model is helpful to allocate medical resources reasonably. For children with good curative effect prediction, standardized treatment and follow-up can be carried out in primary medical institutions, while for children with high risk of complex or poor curative effect, they can be referred to higher medical institutions in time for further evaluation and treatment, so as to improve the utilization efficiency of medical resources.16
Strengths and Limitations
The advantage of this study lies in the comprehensive consideration of clinical characteristics, bone metabolism and ovarian function, and the constructed model shows good predictive ability in both the training set and the validation set, especially the high C-index index and good calibration of the training set, which provides a reliable basis for clinical application. The nomogram prediction model constructed in this study provides a powerful tool for individualized treatment of ICPP girls. Clinicians can calculate the probability of poor curative effect of GnRHa through the model according to various indicators of children before treatment, such as breast development, bone metabolism and ovarian function. For children with high risk of poor prognosis, doctors can monitor their growth and development more closely and adjust the treatment plan in time.17 For example, it may be considered to combine other drugs to enhance the therapeutic effect, or to adjust the dose and treatment cycle of GnRHa. On the contrary, for children with better predicted curative effect, they can be treated according to the conventional scheme, reducing unnecessary medical intervention and expenses, and improving the treatment compliance of children and parents.18 Early and accurate prediction of the curative effect of GnRHa is helpful for early intervention of ICPP girls. By identifying those children who may benefit from early intensive treatment, more active measures can be taken at the early stage of disease progression to improve the prognosis of children to the greatest extent. For example, for children with abnormal bone metabolism and obvious premature activation of ovarian function, early intervention may help to slow down the progress of bone age, prolong the time of height growth, reduce the risk of height damage at the end of the year, and may also alleviate the adverse effects of precocious puberty on children’s psychological and social adaptability.19
This study has several limitations. First, the sample size of this study is relatively small and it is a single-center study. Although strict statistical processing was carried out in the data analysis, the small sample size may not fully cover all the clinical characteristics and variations of girls with ICPP, resulting in a certain selection bias in the research results. Single-center research may also be influenced by local medical level, patient group characteristics and other factors, which limits the universal applicability and representativeness of the research results to some extent. Second, the statistical power was constrained by the relatively small sample size from a single center and the low number of outcome events (poor response). This resulted in a low EPV ratio, increasing the risk of model overfitting, as suggested by the performance drop from the training to the validation set. Although internal bootstrap validation was employed to provide optimism-corrected estimates, the model requires external validation in larger, multi-center cohorts before it can be considered for routine clinical application.20,21 Third, the follow-up period was limited to 6 months for evaluating treatment response. The long-term efficacy and the impact of potential combination therapies (eg, with rhGH) remain unclear and warrant further investigation. Fourth, despite including a range of clinical, bone metabolism, and ovarian function indicators, other potentially influential factors, such as genetic predispositions or lifestyle elements, were not considered and could be integrated into future models. Finally, despite standardized protocols, measurement variations (eg, in bone age assessment or biochemical assays) could have introduced some error, highlighting the need for strict quality control in subsequent studies.22
Conclusion
In this study, a GnRHa therapeutic effect nomogram model of ICPP girls was constructed. It was found that the risk factors of poor therapeutic effect were the heavier breast development, more pubic hair growth, higher N-MID level, higher ALP level, larger ovarian volume, more follicles, and higher LH, FSH and E2 levels. The model has good prediction efficiency in training set and validation set, and has clinical decision-making value, which can help doctors make individualized plans. The model performance should be interpreted with caution due to potential overfitting, and external validation is needed before clinical application.
Data Sharing Statement
The datasets used and analysed during the current study available from the corresponding author on reasonable request.
Ethics Approval and Consent to Participate
This study was approved by the Ethics Committee of the Fujian Children’s Hospital (approval number: 2024ETKLRK09007), and all parents of the affected children signed informed consent forms. All methods were carried out in accordance with Declaration of Helsinki.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This study was Supported by the Fujian Medical University Sailing Fund Project (2021QH1196).
Disclosure
The authors declared that they have no conflicts of interest regarding this work.
References
1. Toutoudaki K, Paltoglou G, Papadimitriou DT, et al. The role of SNPs in the pathogenesis of idiopathic central precocious puberty in girls. Children. 2023;10(3):450. doi:10.3390/children10030450
2. Maqdasy S, Barres B, Salaun G, et al. Idiopathic central precocious puberty in a klinefelter patient: highlights on gonadotropin levels and pathophysiology. Basic Clin Androl. 2020;30(1):19. doi:10.1186/s12610-020-00117-1
3. Knific T, Lazarevič M, Žibert J, et al. Final adult height in children with central precocious puberty - a retrospective study. Front Endocrinol. 2022;13:1008474. doi:10.3389/fendo.2022.1008474
4. Oktay K, Harvey BE, Partridge AH, et al. Fertility preservation in patients with cancer: ASCO clinical practice guideline update. J Clin Oncol. 2018;36(19):1994–11. doi:10.1200/JCO.2018.78.1914
5. Shi Y, Ma Z, Yang X, et al. Gonadotropin-releasing hormone analogue and recombinant human growth hormone treatment for idiopathic central precocious puberty in girls. Front Endocrinol. 2022;13:1085385. doi:10.3389/fendo.2022.1085385
6. He J, Kang Y, Zheng L. Correlation of serum levels of LH, IGF-1 and leptin in girls with the development of idiopathic central precocious puberty. Minerva Pediatr. 2023;75(3):381–386. doi:10.23736/S2724-5276.18.05069-7
7. Chen T, Yu W, Xie X, et al. Influence of gonadotropin hormone releasing hormone agonists on interhemispheric functional connectivity in girls with idiopathic central precocious puberty. Front Neurol. 2020;11:17. doi:10.3389/fneur.2020.00017
8. Jin W, Gu C, Fei Z, et al. Mayer-rokitansky-küster-hauser syndrome with idiopathic central precocious puberty: a case report. Transl Pediatr. 2023;12(5):1053–1058. doi:10.21037/tp-23-181
9. Zhang J, Gao R, Jiang Y, et al. Novel serological biomarker models composed of bone turnover markers, vitamin D, and estradiol and their auxiliary diagnostic value in girls with idiopathic central precocious puberty. Bone. 2022;154:116221. doi:10.1016/j.bone.2021.116221
10. Nieminen-Pihala V, Tarkkonen K, Laine J, et al. Early B-cell factor1 (Ebf1) promotes early osteoblast differentiation but suppresses osteoblast function. Bone. 2021;146:115884. doi:10.1016/j.bone.2021.115884
11. Zhu S, Long L, Hu Y, et al. GnRHa/Stanozolol combined therapy maintains normal bone growth in central precocious puberty. Front Endocrinol. 2021;12:678797. doi:10.3389/fendo.2021.678797
12. Yuan B, Pi YL, Zhang YN, et al. A diagnostic model of idiopathic central precocious puberty based on transrectal pelvic ultrasound and basal gonadotropin levels. J Int Med Res. 2020;48(8):300060520935278. doi:10.1177/0300060520935278
13. Zhang Y, Zhao W, Han Y, et al. The follicular-phase depot GnRH agonist protocol results in a higher live birth rate without discernible differences in luteal function and child health versus the daily mid-luteal GnRH agonist protocol: a single-centre, retrospective, propensity score matched cohort study. Reprod Biol Endocrinol. 2022;20(1):140. doi:10.1186/s12958-022-01014-0
14. Huang S, Zhang L, Gao C, et al. Efficacy and safety of leuprorelin 3-month depot (11.25 mg) for idiopathic central precocious puberty treatment of Chinese girls: a single-center retrospective study. J Pediatr Endocrinol Metab. 2023;37(1):15–20. doi:10.1515/jpem-2023-0410
15. Thom K, Patsch JM, Haufler F, et al. Evaluation of bone mineral density and bone turnover in children on anticoagulation. Front Endocrinol. 2023;14:1192670. doi:10.3389/fendo.2023.1192670
16. Vuralli D, Ozon ZA, Gonc EN, Alikasifoglu A, Kandemir N, Gonc EN, et.al. Long-term effects of GnRH agonist treatment on body mass index in girls with idiopathic central precocious puberty. J Pediatr Endocrinol Metab. 2020;33(1):99–105. doi:10.1515/jpem-2019-0214
17. Wu W, Zhu X, Chen Y, et al. Development and validation of a model for predicting the adult height of girls with idiopathic central precocious puberty. Eur J Pediatr. 2023;182(4):1627–1635. doi:10.1007/s00431-023-04842-3
18. Zou P, Zhang L, Zhang R, et al. Development and validation of a combined mri radiomics, imaging and clinical parameter-based machine learning model for identifying idiopathic central precocious puberty in girls. J Magn Reson Imaging. 2023;58(6):1977–1987. doi:10.1002/jmri.28709
19. Aiello F, Palumbo S, Cirillo G, et al. MKRN3 circulating levels in girls with central precocious puberty caused by MKRN3 gene mutations. J Endocrinol Invest. 2024;47(6):1477–1485. doi:10.1007/s40618-023-02255-5
20. Cleemann Wang A, Hagen CP, Johannsen TH, et al. Differentiation of idiopathic central precocious puberty from premature thelarche using principal component analysis. J Clin Endocrinol Metab. 2024;109(2):370–379. doi:10.1210/clinem/dgad535
21. Haijing C, Xia W, Xinguang L, et al. Analysis of influencing factors and strategies for premature breast development in female children based on logistic regression analysis: a rand omized double-blind controlled clinical trial. Altern Ther Health Med. 2024;10:AT10315.
22. He Z, Yuan B. Diagnostic value of combined detection of pelvic ultrasound and serum LH, FSH, and E2 levels in children with idiopathic central precocious puberty. Evid Based Complement Alternat Med. 2022;8:7928344.
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.