Back to Journals » Infection and Drug Resistance » Volume 12
A Novel Detection of Enterococcus faecalis Using Multiple Cross Displacement Amplification Linked with Gold Nanoparticle Lateral Flow Biosensor
Authors Chen X, Ma K, Yi X, Xiao Z, Xiong L, Wang Y, Li S
Received 19 October 2019
Accepted for publication 22 November 2019
Published 4 December 2019 Volume 2019:12 Pages 3771—3781
DOI https://doi.org/10.2147/IDR.S235325
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Suresh Antony
Xu Chen,1,2 Kai Ma,3 Xu Yi,1 Ziyu Xiao,4 Lijuan Xiong,3 Yu Wang,5 Shijun Li2
1Central Laboratory of the Second Affiliated Hospital, Guizhou University of Traditional Chinese Medicine, Guiyang, Guizhou 550003, People’s Republic of China; 2Laboratory of Bacterial Infectious Disease of Experimental Centre, Guizhou Provincial Centre for Disease Control and Prevention, Guiyang, Guizhou 550004, People’s Republic of China; 3Clinical Laboratory Centre of the Second Affiliated Hospital, Guizhou University of Traditional Chinese Medicine, Guiyang, Guizhou 550003, People’s Republic of China; 4School of Public Health, Guizhou Medical University, Guiyang, Guizhou 550025, People’s Republic of China; 5Department of Clinical Laboratory Centre, The First People’s Hospital of Guiyang, Guiyang, Guizhou 550004, People’s Republic of China
Correspondence: Shijun Li
Experimental Centre, Guizhou Provincial Centre for Disease Control and Prevention, 115 Bageyan Road, Guiyang, Guizhou 550004, People’s Republic of China
Tel/Fax +86 851 86824290
Email [email protected]
Background: Enterococcus faecalis, an opportunistic bacterial pathogen, is one of the most frequently isolated bacterial species and cause of serious nosocomial infections in recent decades. A reliable and rapid assay for E. faecalis detection is significant for the diagnosis and follow-up treatment.
Methods: A novel assay method, named multiple cross displacement amplification linked with nanoparticle-based lateral flow biosensor (MCDA-LFB), was applied for detecting E. faecalis strains. A set of special 10 primers was designed according to E. faecalis-specific gene Ef0027. The MCDA amplification conditions, including the target DNA concentration, reaction temperature and time, were optimized. The sensitivity and specificity of MCDA method were tested in the current study, and then, the MCDA-LFB technology was applied to detect the E. faecalis strain from clinical samples.
Results: The E. faecalis specific primers were valid for the establishment of MCDA-LFB technology forthe detection of E. faecalis based on the Ef0027 gene. The MCDA amplification condition was optimized at 62°C for 35 min. The MCDA products were directly sensed and displayed with a biosensor. The full process, comprising genomic DNA template preparation (approximately 30 mins), amplification of MCDA (35 mins), and the product identification (approximately 2 mins), could be achieved in 70 mins. The MCDA technique could detect as little as 10 fg per reaction system of pure E. faecalis genomic DNA. The specificity of E. faecalis-MCDA-LFB method is 100%, with no cross-reactions to non-E. faecalis strains.
Conclusion: The MCDA-LFB technique established in the present study is a reliable, simple, rapid, sensitive and specific method to assay E. faecalis and can be applied for the detection of clinical samples.
Keywords: Enterococcus faecalis, limit of detection, multiple cross displacement amplification, gold nanoparticle, lateral flow biosensor, MCDA-LFB
Introduction
Enterococcus faecalis (E. faecalis), a Gram-positive enterococci, is widely distributed in the gastrointestinal tracts of humans, animals, and insects and natural environment.1,2 E. faecalis has emerged as a major opportunistic pathogen cause of outbreaks of nosocomial infections affecting various tissues, including human urinary tract infections, intraabdominal infections, infective endocarditis, neonatal sepsis, and bacteremia.3 Thus, to develop a reliable and rapid assay for E. faecalis, detection is significant for the diagnosis and follow-up treatment.
The traditional and gold standard for the detection of E. faecalis is cultivation on agar plates, while this detection method took more than 48 h of growth.4,5 Moreover, the sensitivity of cultivation-based techniques was significantly decreased if the clinical samples were collected after antimicrobial therapy.5 Polymerase chain reaction (PCR) and PCR-based technologies (real-time PCR and multiplex PCR) were applied to detect clinical pathogens because these detection methods are specific, rapid, and sensitive.6–9 Nevertheless, PCR-based methods need special experimental instruments and skilled personnel that may not be readily available in many resource-poor settings. Herein, advanced assays are urgently required for low-cost, reliable, sensitive, specific, and simple detection of target pathogens to ensure prompt treatment.
Multiple cross displacement amplification (MCDA) technique has been applied to detect a range of pathogens such as Shigella spp, Listeria monocytogenes, and Neisseria meningitides.10–12 MCDA method can amplify target gene sensitively and efficiently, using a water bath or sample heater at a constant temperature.13,14 In the MCDA amplification system, six primers for amplification (C1, D1, C2, D2, R1, and R2), two displacement primers (F1 and F2), and two cross primers (CP1 and CP2), designed according to target DNA sequence, were used for the amplification.15,16 MCDA method is able to yield amplicons from as little as three microbes. These amplification products can be rapidly, reliably, and visually detected with disposable gold nanoparticles-based lateral flow biosensors (LFB).17
In the present study, the MCDA-LFB detection was developed for the visual, rapid, highly specific, and sensitive detection of E. faecalis carrying the Ef0027 gene, which appeared to be uniquely present in E. faecalis as it showed no homology with other microbial genomes at GenBank by BLAST searches. The detection performance was analyzed with pure cultures and clinical samples.
Materials and Methods
Ethics Statement
The study was approved by the Human Ethics Committee of the Second Affiliated Hospital of Guizhou University of Traditional Chinese Medicine and complied with the Declaration of Helsinki. All data/isolates were analyzed anonymously.
Reagents and Materials
Reagents including DNA extraction kits (Qiagen, Hilden, Germany), visual detection reagent (Malachite Green, MG) and isothermal amplification kits (Beijing HaiTaiZhengYuan technology Co., Ltd., Beijing, China), streptavidin-immobilized 30-nm gold nanoparticles (SA-Gs) (Resenbio Co., Ltd., Xian, China), Antarctic thermal-sensitive uracil-DNA-glycosylase (AUDG), dNTP ((New England Biolabs, Inc, Beijing, China) rabbit anti-fluorescein antibody (anti-FITC Ab), and biotinylated bovine serum albumin (biotin-BSA) (Abcam Co., Ltd., Shanghai, China) were used in this study. Materials including the sample pad, membrane backing card, nitrocellulose membrane (NC), conjugate pad, and absorbent pad were acquired from the Jieyi Biotechnology Co., Ltd. (Shanghai, China).
Design of MCDA Assay Primers
Based on the reaction mechanism of MCDA, 5 pairs of special primers according to the Ef0027 gene (Genbank accession no. 1198935) of E. faecalis were devised by PRIMER PREMIER 5.0 and Primer Explorer V4 (Eiken Chemical, Japan).
Hybrids and hairpin structures of the primers were analyzed by the Integrated DNA Technologies design tools. The specificity of E. faecalis-MCDA primers was verified by Blast analysis tool. The C1 and D1 primers were labeled by biotin and fluorescein isothiocyanate (FITC) at their 5ʹ end, respectively. All of the primers were synthesized by TsingKe Biotech Co., Ltd (Beijing, China) with HPLC purification grade. The primer sequences are shown in Table 1, and the primer positions of the E. faecalis gene are displayed in Figure 1.
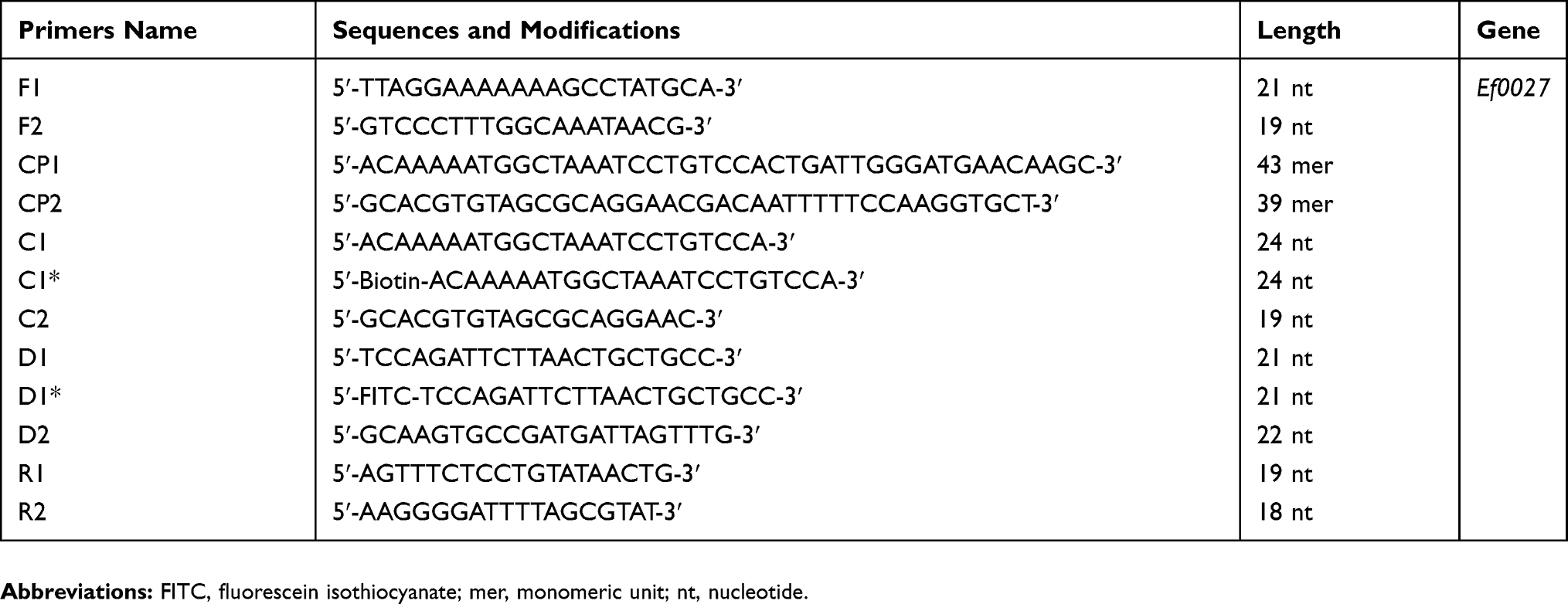 |
Table 1 The Primers Used in the Present Study |
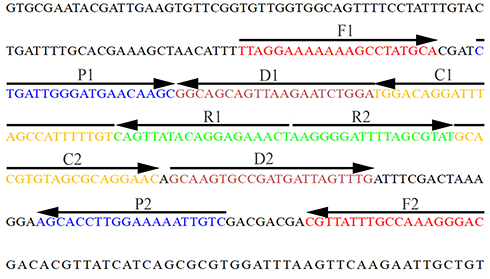 |
Figure 1 Location and sequence of the Enterococcus faecalis specific gene Ef0027 applied for the MCDA primer design. The nucleotide sequence of the sense strand of the E. faecalis gene Ef0027 is shown in the diagram. Right arrows and left arrows indicate sense and complementary sequences which were used in the current study, respectively. Abbreviation: MCDA, multiple cross displacement amplification. |
Bacterial Strains and Genomic DNA Template Preparation
In the present study, forty-nine bacterial strains, including standard strain of E. faecalis (ATCC 29212), twelve clinical E. faecalis-positive isolates, and thirty-six non-E. faecalis strains, were used in this study (Table 2). The E. faecalis standard strain (ATCC 29212) was applied for the optimization of the target method. The DNA templates were prepared by extracting the genomic DNA from the bacterial isolates using QIAamp DNA Mini Kit in accordance with the instructions from the manufacturer and measured with a Nanodrop ND-2000 (Beijing, China) at A260/280.
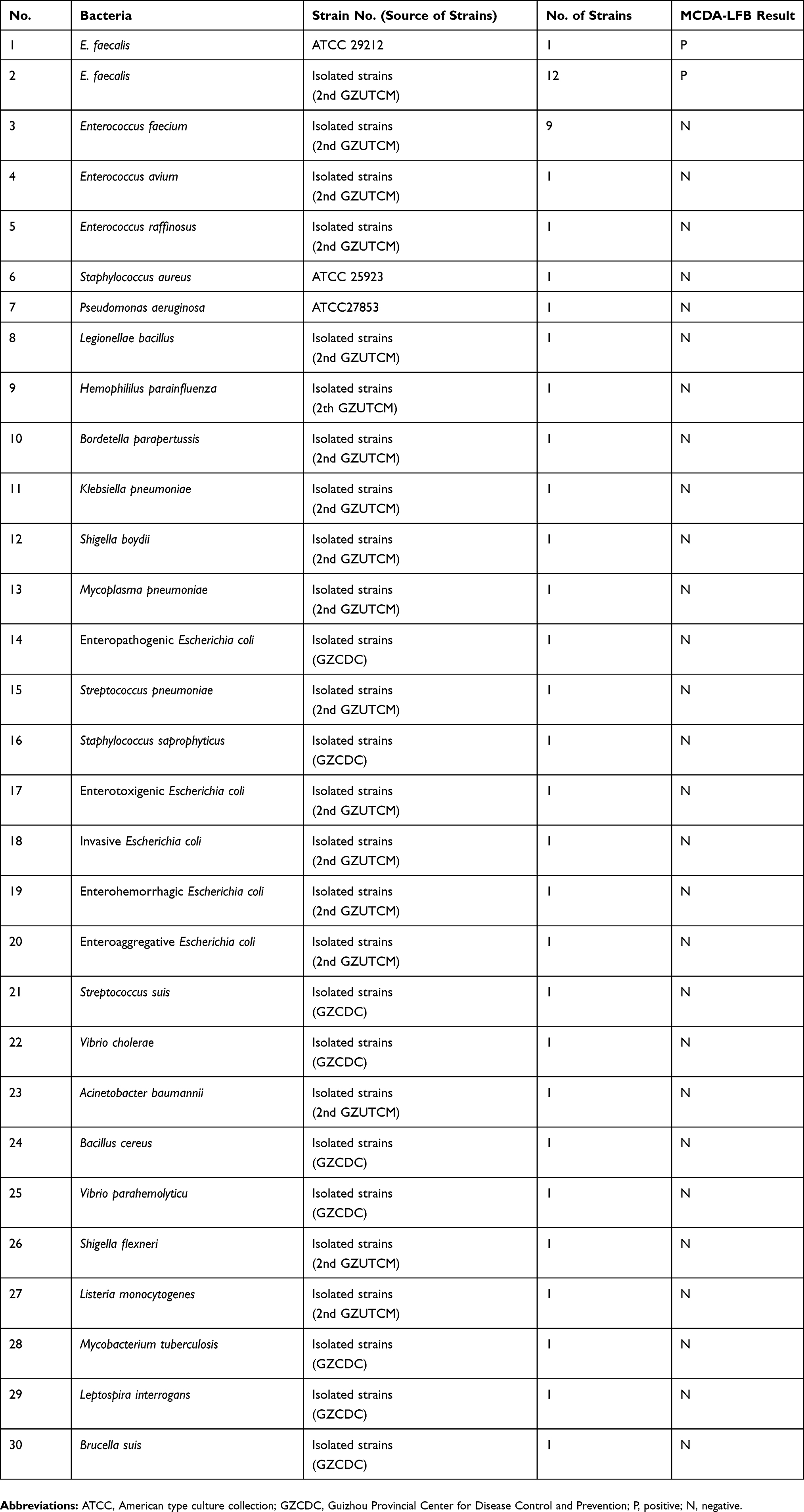 |
Table 2 Bacterial Strains Used in the Current Study |
Gold Nanoparticle-Based Lateral Flow Biosensor Preparation
The LFB (4mm×60 mm) was constructed according to the previous reports.18,19 In brief, a plastic adhesive backing card was laminated with NC membrane, sample pad, absorbent pad, and conjugate pad, followed by spraying with biotin-BSA (2.5 mg/mL) and anti-FITC Ab (0.15 mg/mL) conjugates onto the NC membrane to produce the line for control sample (CL) and test sample (TL).Each line was separated with 5 mm. And the conjugate pad of the strip was deposited with SA-G in 0.01M PBS (PH 7.4). The 4-mm-wide strips were prepared by cutting the assembled cards. The prepared biosensors were preserved in a plastic box with a desiccant gel at room temperature.
MCDA-LFB Detection
MCDA was performed in a 25 μL reaction system as described by previously reported.20 In brief, 0.4 μM of d F1 and F2 (displacement primers), 1.2 μM of R1, R2, D1* and D2, 0.8 μM of C1* and C2, 1.2 μM of CP1 and CP2 (cross primers), 1.25 μL of Bst DNA polymerase (10 U), and 12.5 μL of 2×reaction mix, and 1 μL prepared DNA.
Colorimetric indicator (Malachite Green, MG) and lateral flow biosensor (LFB) methods were applied for the determination and verification of the E. faecalis-MCDA products, respectively. The color of effectively amplified products could change from colorless to light green by using MG method. However, the color of negative and blank controls kept colorless. For the LFB assay, two visible red lines (the CL and TL) could display for the positive results but only the line (CL) appeared for the negative and blank control samples.
Temperature Optimization of the E. faecalis-MCDA-LFB Assay
The E. faecalis-MCDA reaction temperature used for optimization was from 60°C to 67°C for 60 mins with 10 pg Enterococcus faecium DNA template. In addition, DNA of Staphylococcus aureus (ATCC 25923) and double-distilled water (DW) were used as negative control and a blank control, respectively. The MCDA amplifications were monitored through the turbidity of products. The curves of DNA concentrations of each amplified products were exhibited in the graph. Turbidity >0.1 was considered as positive.
Analytical Sensitivity of E. faecalis-MCDA-LFB Assay
The sensitivity of E. faecalis-MCDA-LFB method was determined using 1μL of the serial dilution (10 ng, 10 pg, 1 pg, 100 fg, 10 fg, 1fg and 100 atto gram per microliter) of the genomic DNA extracted from E. faecalis. The amplification was carried out at the optimized temperature to measure the limit of detection (LoD) of E. faecalis-MCDA-LFB. Three replicates of each dilution were tested.
Optimization of the Amplification Time for E. faecalis-MCDA-LFB Assay
The E. faecalis-MCDA reaction system was amplified at the optimized temperature for diverse amplification times (from 15 to 45 mins, 10 mins of the interval). And then, the products were determined using LFB, and each amplification time was tested at least three times.
Specificity Analysis of E. faecalis-MCDA-LFB Detection
Genomic DNA templates from 49 different bacterial strains (Table 2) were used to verify the specificity of E. faecalis-MCDA-LFB method. The 49 bacterial strains included the standard strain of E. faecalis (ATCC 29212), 12 E. faecalis isolates, and 36 non-E. faecalis strains. DW was used as a blank control. All of the MCDA results were tested with LFB and confirmed at least three times.
Application of E. faecalis-MCDA-LFB Method for the Detection of Clinical Samples
Fifty-three urine samples of patients, 30 hospital surface samples, and 35 urine samples of healthy volunteers were collected from the Second Affiliated Hospital of Guizhou University of Traditional Chinese Medicine. All of the samples were detected for E. faecalis using traditional culture, PCR, and DCDA-LFB techniques, respectively. Traditional culture methods including colony morphology, Gram stain, and biochemical identification were used for identification of the E. faecalis isolates. PCR detections of all the genomic DNA templates were conducted by using E. faecalis specific primers.8 The MCDA-LFB detection results were compared with that of traditional culture and PCR assay.
Results
Verification of E. faecalis-MCDA Productions
In order to confirm the validity of primers (Table 1) for the E. faecalis-MCDA assay, genomic DNA from pure E. faecalis cultures were amplified at 64°C for 60 mins. The products were identified using MG and LFB methods. The results showed that amplification appeared with genomic DNA from E. faecalis (ATCC 29212), but not with E. faecium, S. aureus, and the blank control (Figure 2A and B). Therefore, the E. faecalis-MCDA primers used in the current study were valid for the development of E. faecalis-MCDA-LFB.
 |
Figure 2 Confirmation and verification of E. faecalis-MCDA products. (A) The E. faecalis-MCDA amplification products were detected by the MG method through visual observation of the color change. (B) LFB was applied for the visual detection of E. faecalis-MCDA products. Tube 1/Biosensor 1: positive amplification of E. faecalis strain 29212; Tube 2/Biosensor 2: negative amplification of Enterococcus faecium (2nd GZUTCM); Tube 3/Biosensor 3: negative amplification of Staphylococcus aureus (ATCC25923); Tube 4/Biosensor 4: blank control (DW). |
Optimal Temperature for E. faecalis-MCDA-LFB Detection
To certify the optimum amplification temperature, 10 pg of genomic DNA of E. faecalis strain was utilized as the target template in each reaction mixture. The results showed that 62°C was the faster amplification as indicated by the kinetics graphs of real-time turbidity (Figure 3). Therefore, the most suitable temperature for E. faecalis-MCDA-LFB was determined as 62°C, which was applied to the rest of the assays in the current study.
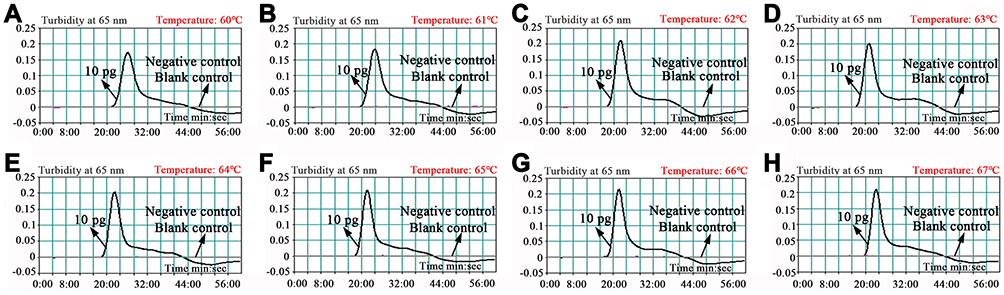 |
Figure 3 (A–H) Optimization of reaction temperature for E. faecalis-MCDA primers. The MCDA amplifications for the detection of E. faecalis were monitored through real-time turbidity, and the corresponding curves of DNA concentrations were displayed in the graph. The threshold value was 0.1 and a turbidity>0.1 was considered as positive. Mixtures with 10-pg genomic templates of Enterococcus faecium (isolated strain) and Staphylococcus aureus (ATCC 25923) were used as negative controls (NCs), and 1 μL of double-distilled water (DW) was used as a blank control (BC). Eight kinetic graphs were obtained at different temperatures (60–67°C, 1°C intervals) with 10-pg target genomic DNA per reaction. The graphs from C to H showed robust amplification. |
Sensitivity of MCDA-LFB Method for E. faecalis Assay
The sensitivity of E. faecalis-MCDA-LFB was tested by serially diluted DNA sample from E. faecalis strain (ATCC29212) and determined by visual inspection of reaction productions with MG reagents and lateral flow biosensors, respectively. Both of the two methods demonstrated that the LoD of E. faecalis-MCDA-LFB was 10 fg DNA template (Figure 4A and B).
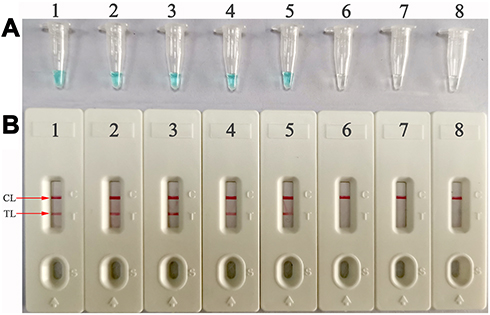 |
Figure 4 Sensitivity analysis of the MCDA-LFB detection by serial dilutions of genomic DNA extracted from E. faecalis strain. Two detection methods, colorimetric indicator (MG; A) and lateral flow biosensor (B), were used to analyze the amplification productions. The serial dilutions of E. faecalis genomic DNA (10 ng, 10 pg, 1 pg, 100 fg, 10 fg, 1fg, and 100 atto gram per microliter) were subjected to standard MCDA amplifications. Tubes (A)/Biosensors (B) 1–8 represent the DNA levels of 10 ng, 10 pg, 1 pg, 100 fg, 10 fg, 1 fg, and 100 atto gram per reaction of target templates and blank control (DW), respectively. The target gene levels of 10 ng, 10 pg, 1 pg, 100 fg, 10 fg per reaction showed positive amplifications. |
Optimized Amplification Time for E. faecalis-MCDA-LFB Detection
In order to confirm the optimum amplification time for the E. faecalis-MCDA-LFB detection during amplification phases, 15-, 25-, 35-, and 45-min amplification times were selected and compared at 62°C, respectively. The detection limit level of DNA (10 fg of E. faecalis genomic templates per reaction) showed both TLand CL when the reaction proceeded for 35 and 45 mins (Figure 5). Therefore, 35 mins was deemed as an appropriate amplification time for E. faecalis-MCDA-LFB detection.
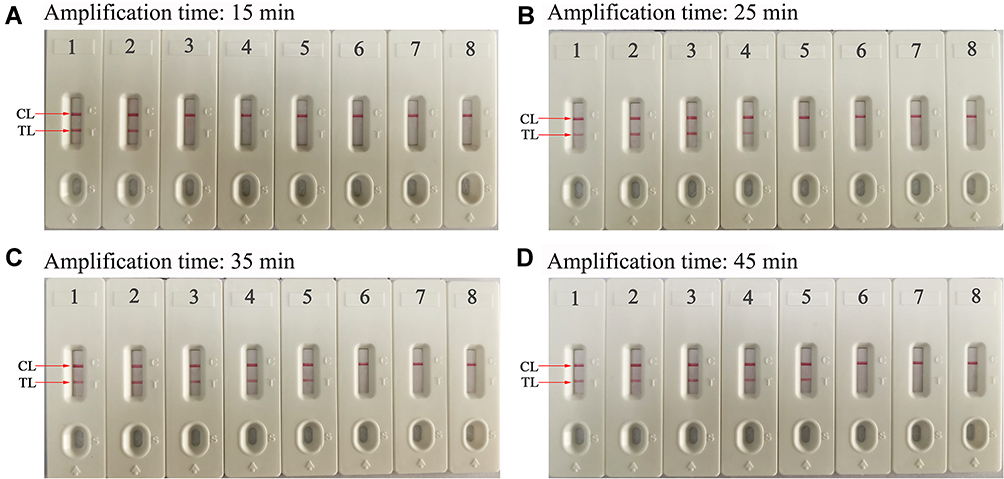 |
Figure 5 Optimization of amplification time for E. faecalis-MCDA-LFB detection method. Different amplification times (A, 15mins; B, 25 mins; C, 35 mins; D, 45 mins) were tested at 62°C, respectively. Biosensors 1, 2, 3, 4, 5, 6, 7, and 8 represent genomic DNA levels of 10 ng, 10 pg, 1 pg, 100 fg, 10 fg, 1 fg, and 100 atto gram per reaction of target templates and blank control (DW). The best sensitivity was observed when the amplification lasted for 35 mins (C). |
Specificity of MCDA-LFB Method for E. faecalis Assay
The genomic DNA from all of the bacterial strains (Table 1) were used for E. faecalis-MCDA-LFB specificity determination. The results showed that only the genomic DNA from E. faecalis strains showed positive results, while other non-E. faecalis isolates and blank control showed negative results (Figure 6).
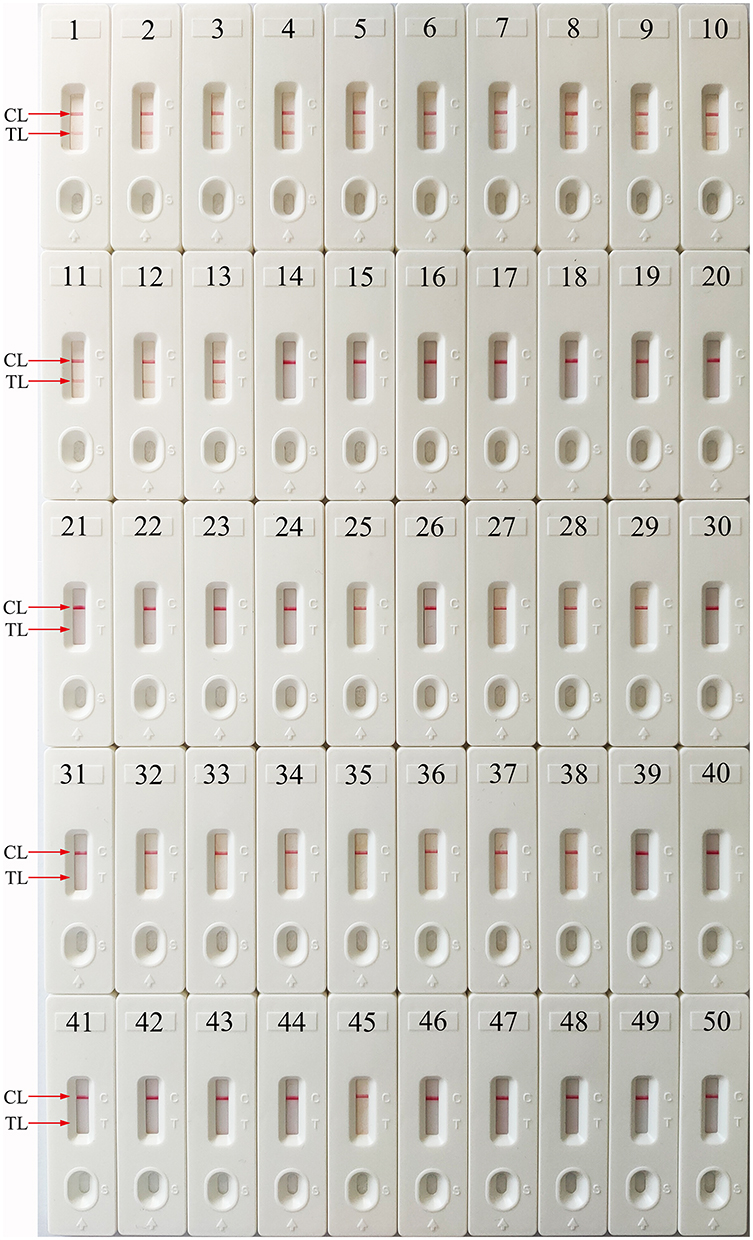 |
Figure 6 Specificity analysis of the E. faecalis-MCDA-LFB detection for different strains. The MCDA amplifications were carried out using different strain genomic DNA as templates and determined by means of visual LFB method. Biosensor 1, E. faecalis strain (ATCC 29212); biosensor 2–13, twelve isolated strain of E. faecalis from the Second Affiliated Hospital, Guizhou University of Traditional Chinese Medicine; biosensor 14–22, nine isolated Enterococcus faecium strains, biosensor 23–49, Enterococcus avium, Enterococcus raffinosus, Staphylococcus aureus, Pseudomonas aeruginosa, Legionellae bacillus, Hemophililus parainfluenza, Bordetella parapertussis, Klebsiella pneumonia, Shigella boydii, Mycoplasma pneumonia, Enteropathogenic Escherichia coli, Streptococcus pneumonia, Staphylococcus saprophyticus, Enterotoxigenic Escherichia coli, Invasive Escherichia coli, Enterohemorrhagic Escherichia coli, Enteroaggregative Escherichia coli, Streptococcus suis, Vibrio cholera, Acinetobacter baumannii, Bacillus cereus, Vibrio parahemolyticu, Shigella flexneri, Listeria monocytogenes, Mycobacterium tuberculosis, Leptospira interrogans, Brucella suis; biosensor 50, blank control (DW). |
Detection Results of E. faecalis-MCDA-LFB for Clinical Samples
In order to demonstrate that the MCDA-LFB method is a reliable and rapid tool for E. faecalis detection in clinical samples, 53 urine samples of patients, 30 hospital surface samples, and 35 urine samples of healthy volunteers collected from the Second Affiliated Hospital of Guizhou University of Traditional Chinese Medicine were used for the application of E. faecalis-MCDA-LFB established in the current study. The results showed that 23 of 118 samples had been verified as E. faecalis-positive results through traditional culture technique, and the other 95 samples showed E. faecalis-negative outcome. The MCDA-LFB assay results were consistent with traditional cultivation detection results. However, only 15 urine samples showed positive results when using conventional Ef0027 gene-based PCR, and all of the 15 positive urine samples were covered by the E. faecalis positive samples detected by traditional culture and MCDA-LFB methods (Table 3).
 |
Table 3 Comparison of Conventional Culture, PCR. and MCDA-LFB Methods for the Assay of E. Faecalis in Clinical Samples |
Discussion
E. faecalis is becoming increasingly important for causing bacteremia, endocarditis, and other nosocomial infections in recent decades.21,22 Moreover, more and more E. faecalis isolates build up antibiotic resistance.2,23,24 Thus, developing a reliable, rapid, specific, and sensitive detection method for E. faecalis is essential for the disease diagnosis and its therapy. Our study showed that the newly established E. faecalis-MCDA-LFB is a rapid, sensitive, and specific method to detect E. faecalis.
The specificity of MCDA was powerfully confirmed with genomic DNA from E. faecalis pure cultures. All of the E. faecalis isolates showed positive results, but all the non-E. faecalis strains displayed a negative outcome (Figure 6). Thus, the E. faecalis-MCDA-LFB method has a high level of specificity for the identification of E. faecalis species. The high degree of specificity of the MCDA-LFB established in the present study seems due to using the Ef0027 gene, which encodes a putative phosphosugar-binding transcriptional regulator. This gene appeared to be uniquely present in E. faecalis as it showed no homology with other microbial genomes at GenBank by BLAST searches, and the Ef0027 gene also applied to develop some advanced methods for detecting E. faecalis species.8,25 Another reason to explain the high degree of specificity of E. faecalis-MCDA-LFB is because we designed ten primers targeting the different regions of the Ef0027 gene sequence.
Compared with conventional culture and PCR-based methods, the MCDA-LFB developed in this study is more time-saving and economical.10,12,26 The E. faecalis-MCDA-LFB reaction just requires a simple incubation at 62°C for 35 mins. There are various portable user-friendly instruments for MCDA reaction. For example, the dry block heater (Labnet, USA) is one of the suitable instruments, which is a portable, battery-powered equipment supporting 96-channel MCDA reactions per detection. Moreover, the universal isothermal amplification kits such as NEB Warmstart and Eiken Loopamp kits can be commercially obtained and applied for MCDA amplification, and the cost of MCDA reaction is estimated to be $3.5 USD, the LFB detection merely costs approximately $2 USD, which is cheaper than the common PCR-based methods.15,16 Additionally, this method can decrease labor costs because performing the MCDA-LFB assay does not need skilled technical personnel. The entire detection process, including template preparation (approximately 30 mins), isothermal amplification (35 mins), and LFB reading (approximately 2 mins), could be accomplished within 70 mins. Thus, this method can save precious time and cost of detection compared with the traditional methods.
In addition, the advanced E. faecalis-MCDA-LFB technique was more sensitive than normal PCR and loop-mediated isothermal amplification (LAMP) methods. The newly developed E. faecalis-MCDA-LFB method was capable of assaying 10 fg of E. faecalis genomic DNA (Figure 4), which was more sensitive than E. faecalis-LAMP-LFB detection (250 fg per reaction) reported by the previous study.25 Although the amplification products could be detected equally with the MG method used in the present study, the LFB was deemed as the preferred method as observing the amplification results is more objective and does not need any apparatus.19,27 In conclusion, the newly E. faecalis-MCDA-LFB assay in this study is a valuable method for the convenient, rapid, sensitive, specific, visual, reliable, and low-cost detection of E. faecalis in clinical and environmental samples, especially in resource-constrained settings. However, the E. faecalis-MCDA-LFB method has some limitations when compared with some methods which can be applied for E. faecalis antimicrobial resistance detection. Later, we will study on the rapid and reliable assay of drug resistance genes of E. faecalis based on the E. faecalis MCDA-LFB method created in the current study.
Conclusion
In this study, a reliable and rapid E. faecalis-MCDA-LFB method was developed for detecting E. faecalis, causing nosocomial infection, including urinary tract infection, bloodstream infection, and surgical site infection in human. This method could rapidly, sensitively, specifically, and reliably detect the E. faecalis agent in the urine sample and did not rely on expensive instruments and reagents. Using LFB detection could help to obtain a rapid, objective, and easily interpretable result. Hence, the E. faecalis-MCDA-LFB assay could be considered as a useful method for reliable and rapid detection of E. faecalis in clinical and environmental samples, particularly in resource-limited regions of the world.
Acknowledgments
This study was funded by the Program of the High-Level Creative Talents Cultivation in Guizhou Province (Qian Ke He (2016)4021), the Program of Scientific and Technological Innovation Team of Guizhou Province (Grant No. Qian Ke He Platform talent [2018]5606), the Guizhou Provincial Special Funds for Science and Technology Supporting Program ([2019]1186 and [2018]5767), and the Program of Science and Technology of Guizhou Provincial Health Commission (gzwjkj2018-1-012).
Disclosure
All of the authors declared that there are no competing interests in this article.
References
1. Beganovic M, Luther MK, Rice LB, et al. A review of combination antimicrobial therapy for Enterococcus faecalis bloodstream infections and infective endocarditis. Clin Infect Dis. 2018;67(2):303–309. doi:10.1093/cid/ciy064
2. Jabbari Shiadeh SM, Pormohammad A, Hashemi A, et al. Global prevalence of antibiotic resistance in blood-isolated Enterococcus faecalis and Enterococcus faecium: a systematic review and meta-analysis. Infect Drug Resist. 2019;12:2713–2725. doi:10.2147/IDR.S206084
3. Janani M, Jafari F, Samiei M, et al. Evaluation of antibacterial efficacy of photodynamic therapy vs. 2.5% NaOCl against E. faecalis-infected root canals using real-time PCR technique. J Clin Exp Dent. 2017;9(4):e539–e544. doi:10.4317/jced.53526
4. Pongsachareonnont P, Honglertnapakul W, Chatsuwan T. Comparison of methods for identifying causative bacterial microorganisms in presumed acute endophthalmitis: conventional culture, blood culture, and PCR. BMC Infect Dis. 2017;17(1):165. doi:10.1186/s12879-017-2264-5
5. Okui A, Soga Y, Kokeguchi S, et al. Detection of identical isolates of Enterococcus faecalis from the blood and oral mucosa in a patient with infective endocarditis. Internal Med. 2015;54(14):1809–1814. doi:10.2169/internalmedicine.54.3223
6. Mirnejad R, Sajjadi N, Masoumi Zavaryani S, et al. Identification of aminoglycoside resistance genes by triplex PCR in Enterococcus spp. isolated from ICUs. Infez Med. 2016;24(3):222–229.
7. Medeiros AW, Pereira RI, Oliveira DV, et al. Molecular detection of virulence factors among food and clinical Enterococcus faecalis strains in South Brazil. Braz J Microbiol. 2014;45(1):327–332. doi:10.1590/S1517-83822014005000031
8. Liu D, Wang C, Swiatlo EJ, et al. PCR amplification of a species-specific putative transcriptional regulator gene reveals the identity of Enterococcus faecalis. Res Microbiol. 2005;156(9):944–948. doi:10.1016/j.resmic.2005.05.004
9. Farrell JJ, Tsung AJ, Flier L, et al. PCR and electrospray ionization mass spectrometry for detection of persistent Enterococcus faecalis in cerebrospinal fluid following treatment of postoperative ventriculitis. J Clin Microbiol. 2013;51(10):3464–3466. doi:10.1128/JCM.01343-13
10. Wang Y, Wang Y, Xu J, et al. Development of multiple cross displacement amplification label-based gold nanoparticles lateral flow biosensor for detection of Shigella spp. Front Microbiol. 2016;7:1834.
11. Wang Y, Li H, Wang Y, et al. Development of multiple cross displacement amplification label-based gold nanoparticles lateral flow biosensor for detection of Listeria monocytogenes. Int J Nanomedicine. 2017;12:473–486.
12. Li S, Liu C, Liu Y, et al. Development of a multiple cross displacement amplification combined with nanoparticles-based biosensor assay to detect Neisseria meningitidis. Infect Drug Resist. 2019;12:2077–2087. doi:10.2147/IDR.S210735
13. Zhao F, Niu L, Yan L, et al. Establishment and application of multiple cross displacement amplification coupled with lateral flow biosensor (MCDA-LFB) for visual and rapid detection of Candida albicans in clinical samples. Front Cell Infect Microbiol. 2019;9:102. doi:10.3389/fcimb.2019.00102
14. Niu L, Zhao F, Chen J, et al. Isothermal amplification and rapid detection of Klebsiella pneumoniae based on the multiple cross displacement amplification (MCDA) and gold nanoparticle lateral flow biosensor (LFB). PLoS One. 2018;13(10):e204332. doi:10.1371/journal.pone.0204332
15. Wang Y, Li H, Li D, et al. Multiple cross displacement amplification combined with gold nanoparticle-based lateral flow biosensor for detection of Vibrio parahaemolyticus. Front Microbiol. 2016;7:2047.
16. Gong L, Liu E, Che J, et al. Multiple cross displacement amplification coupled with gold nanoparticles-based lateral flow biosensor for detection of the mobilized colistin resistance gene mcr-1. Front Cell Infect Microbiol. 2019;9:226. doi:10.3389/fcimb.2019.00226
17. Wang Y, Yan W, Fu S, et al. Multiple cross displacement amplification coupled with nanoparticles-based lateral flow biosensor for detection of Staphylococcus aureus and identification of methicillin-resistant S. aureus. Front Microbiol. 2018;9:907. doi:10.3389/fmicb.2018.00907
18. Wang Y, Wang Y, Zhang L, et al. Multiplex, rapid, and sensitive isothermal detection of nucleic-acid sequence by endonuclease restriction-mediated real-time multiple cross displacement amplification. Front Microbiol. 2016;7:753.
19. Wang Y, Li H, Wang Y, et al. Nanoparticle-based lateral flow biosensor combined with multiple cross displacement amplification for rapid, visual and sensitive detection of Vibrio cholerae. Fems Microbiol Lett. 2017;364(23):1–11. doi:10.1093/femsle/fnx234
20. Wang Y, Wang Y, Ma A, et al. Rapid and sensitive isothermal detection of nucleic-acid sequence by multiple cross displacement amplification. Sci Rep. 2015;5:11902. doi:10.1038/srep11902
21. Weaver KE. The type I toxin–antitoxin par locus from Enterococcus faecalis plasmid pAD1: RNA regulation by both cis-and trans-acting elements. Plasmid. 2015;78:65–70. doi:10.1016/j.plasmid.2014.10.001
22. Madsen KT, Skov MN, Gill S, et al. Virulence factors associated with Enterococcus faecalis infective endocarditis: a mini review. Open Microbiol J. 2017;11:1–11. doi:10.2174/1874285801711010001
23. Bolocan AS, Upadrasta A, Bettio P, et al. Evaluation of phage therapy in the context of Enterococcus faecalis and its associated diseases. Viruses. 2019;11(4):1–18. doi:10.3390/v11040366
24. Heidari H, Hasanpour S, Ebrahim-Saraie HS, et al. High incidence of virulence factors among clinical Enterococcus faecalis isolates in Southwestern Iran. Infect Chemother. 2017;49(1):51–56. doi:10.3947/ic.2017.49.1.51
25. Wang Y, Li H, Wang Y, et al. Loop-mediated isothermal amplification label-based gold nanoparticles lateral flow biosensor for detection of Enterococcus faecalis and Staphylococcus aureus. Front Microbiol. 2017;8:192. doi:10.3389/fcimb.2018.00192
26. Cheng X, Yang J, Wang M, et al. Visual and rapid detection of Acinetobacter baumannii by a multiple cross displacement amplification combined with nanoparticles-based biosensor assay. AMB Expr. 2019;9(1):30. doi:10.1186/s13568-019-0754-0
27. Li S, Liu Y, Wang Y, et al. Rapid detection of Brucella spp. and elimination of carryover using multiple cross displacement amplification coupled with nanoparticles-based lateral flow biosensor. Front Cell Infect Microbiol. 2019;9:78. doi:10.3389/fcimb.2019.00078
 © 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.