Back to Journals » Clinical Ophthalmology » Volume 20
A Novel Conservative Approach for Managing the Phthisical Silicone Oil-Filled Eye: Conjunctival Flap Coverage and Prosthetic Fitting
Authors Yang M ![]() , Zhao T, Wang Z, Chen Y
, Zhao T, Wang Z, Chen Y
Received 24 December 2025
Accepted for publication 26 February 2026
Published 16 March 2026 Volume 2026:20 587995
DOI https://doi.org/10.2147/OPTH.S587995
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Ming Yang,1 Tong Zhao,2 Zhijun Wang,2 You Chen2
1Department of Ophthalmology, Beijing Friendship Hospital, Capital Medical University, Beijing, 100095, People’s Republic of China; 2Department of Ophthalmology, China-Japan Friendship Hospital, Beijing, 100029, People’s Republic of China
Correspondence: You Chen, Department of Ophthalmology, China-Japan Friendship Hospital, No. 2 Yinghua East Street, Chaoyang District, Beijing, 100029, People’s Republic of China, Tel +86-13810078986, Fax +86-010-84205357, Email [email protected]
Objective: To evaluate the clinical efficacy and safety of shallow lamellar keratectomy combined with total conjunctival flap coverage and subsequent customized prosthetic shell fitting for the management of atrophic, silicone oil-filled eyes following severe open globe injury.
Methods: This retrospective case series included 24 patients (24 eyes) with phthisical, silicone oil-dependent eyes after open globe injury repair between October 2010 and May 2020. All patients underwent shallow lamellar keratectomy to remove diseased corneal tissue, followed by total conjunctival flap coverage. A customized prosthetic shell was fitted approximately one month postoperatively after confirmed flap healing. Outcome measures included corneal symptom relief assessed by the Numeric Rating Scale (NRS), palpebral fissure height, exophthalmometry, cosmetic satisfaction rated on a 5-point scale, and postoperative complications.
Results: The mean postoperative follow-up duration was 4.75 ± 2.51 years. All patients achieved complete resolution of pain and foreign body sensation (postoperative NRS=0 for all; preoperative median: 2.00 [IQR: 1.75– 3.00] vs postoperative median: 0.00 [IQR: 0.00– 0.00], P=0.001). Ocular protrusion increased significantly from a preoperative median of 7.00 mm (IQR: 6.00– 8.00 mm) to 12.00 mm (IQR: 10.00– 13.00 mm) postoperatively (P=0.001). Lid height increased from a preoperative median of 3.00 mm (IQR: 2.75– 4.00 mm) to 10.00 mm (IQR: 8.00– 11.25 mm) postoperatively (P=0.001). Patient satisfaction with ocular appearance improved markedly from a preoperative median of 1.00 (IQR: 1.00– 1.25) to 5.00 (IQR: 4.75– 5.00) postoperatively (P=0.001). Two eyes developed limbal epithelial implantation cysts, which were successfully managed without recurrence. Cranial CT revealed no silicone oil migration or sympathetic ophthalmia.
Conclusion: This globe-preserving technique effectively alleviates corneal irritation and restores ocular symmetry in atrophic, silicone oil-filled eyes, offering a safe, cost-effective, and satisfactory conservative alternative to enucleation or evisceration. Further prospective studies with longer follow-up are warranted.
Keywords: open globe injuries, OGI, silicone oil tamponade, phthisis bulbi, conjunctival flap, ocular prosthesis, cosmetic rehabilitation
Introduction
Open globe injury (OGI) is a leading cause of monocular blindness worldwide, particularly in developing countries.1,2 These injuries present acutely with complex, variable manifestations and can lead to devastating complications such as traumatic cataract, retinal detachment, and infectious endophthalmitis, requiring urgent and precise intervention.3,4
Advances in vitreoretinal surgery have improved the prognosis for severe OGI, allowing for the anatomical preservation of eyes that would historically have been enucleated.5,6 The current standard of care involves primary repair followed, in cases with extensive tissue loss, by exploratory intraocular reconstruction and silicone oil (SO) tamponade to maintain volume and compartmentalize the eye.7–10 While SO aids in stabilization, long-term retention is associated with significant complications, including corneal endothelial decompensation, band keratopathy (BK), and persistent irritation.11–13 Ultimately, many of these eyes progress to phthisis bulbi, characterized by globe shrinkage, pseudoptosis, and a poor cosmetic outcome, which can impose a profound psychological burden on patients.2,14
When confronted with a blind, painful, or disfigured eye, traditional management often points toward evisceration or enucleation with orbital implantation.15,16 However, many patients are deeply reluctant to undergo eye removal due to its profound psychological impact.8 Therefore, a pressing clinical need exists for globe-preserving interventions that address both symptomatic relief and cosmetic rehabilitation.
The Gundersen conjunctival flap, a well-established procedure for managing painful bullous keratopathy and refractory ocular surface diseases,17–20 provides a potential solution. By covering the diseased cornea with a vascularized conjunctival flap, it effectively eliminates surface irritation and pain.
In this study, we propose and evaluate a novel application of this technique. We hypothesize that shallow lamellar keratectomy combined with total conjunctival flap coverage, followed by fitting of a prosthetic cosmetic shell, can effectively alleviate symptoms and improve cosmesis in patients with atrophic, SO-filled eyes, thereby offering a conservative yet effective alternative to radical surgery.
Methods
General Information
This retrospective study was approved by the Institutional Review Board of China-Japan Friendship Hospital, China, and adhered to the tenets of the Declaration of Helsinki. Data were collected from patients who had sustained OGI with loss of ocular contents and subsequently underwent SO tamponade for eyeball preservation between October 2010 and May 2020. This study was reviewed and approved by the Ethics Committee of China-Japan Friendship Hospital, Beijing, China. The approval number is 2020–12-K09. The study was conducted in accordance with the Declaration of Helsinki. Written informed consent was obtained from all participants. A total of 24 patients (24 eyes) were included. All patients underwent comprehensive preoperative and postoperative examinations, including visual acuity (VA) testing, slit-lamp biomicroscopy, gonioscopy, and intraocular pressure (IOP) measurement.
Inclusion criteria were: (1) small eyeball size and pseudoptosis, accompanied by corneal irritation symptoms; (2) no light perception (NLP) or inaccurate light projection in the affected eye; (3) the eyeball retained some tension or exhibited cicatricial induration; (4) absence of uveitis signs and no systemic or local surgical contraindications in the contralateral healthy eye; (5) strong patient desire to improve ocular appearance, agreement to undergo surgery and facial photography, and provision of signed informed consent. The exclusion criterion was the presence of contraindications to local or systemic surgery.
For the 15 eyes with SO filling duration exceeding 5 years, cranial and orbital computed tomography (CT) was performed preoperatively to assess potential migration of SO into the ventricles or orbit. Corneal pain was evaluated using a Numeric Rating Scale (NRS), ranging from 0 (no pain) to 10 (worst imaginable pain).21
Surgical Methods
Under retrobulbar anesthesia (4 mL of a 1:1 mixture of 0.1% ropivacaine and 2% lidocaine), a 360° conjunctival peritomy was performed at the limbus. The bulbar conjunctiva was completely dissected to the equator, with radial incisions of 2–3 mm made at the 3 and 9 o’clock positions. A shallow lamellar keratectomy was performed to remove all superficial corneal tissue, including the limbus, reaching the stromal layer (beneath Bowman’s membrane) (Figure 1B). The bulbar conjunctiva was then advanced to cover the entire remaining corneal surface and sutured continuously using 6–0 absorbable sutures. To relieve tension, the conjunctiva was also sutured to the superficial sclera near the limbus at the 3 and 9 o’clock positions (Figure 1C). Postoperatively, tobramycin-dexamethasone eye ointment was applied to the conjunctival sac, followed by a pressure bandage. The bandage was removed after 48 hours, and antibiotic eye drops were administered four times daily for two weeks (Figure 1). A customized prosthetic shell was fitted approximately one month after surgery, once the conjunctival flap was confirmed to be healed firmly to the corneal stromal bed with no signs of inflammation or edema on slit-lamp examination. In our cohort, no patient experienced wound dehiscence, infection, or other complications attributable to the timing of prosthetic fitting.
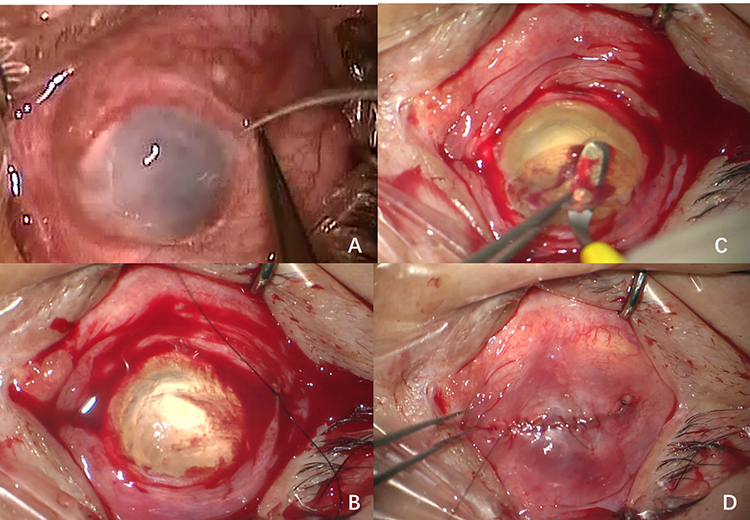 |
Figure 1 Surgical procedures. (A) Peritomy of the bulbar conjunctiva and dissection of Tenon’s capsule. (B) Removal of the superficial lamellar tissue beneath Bowman’s membrane using a tunnel knife, with scraping of limbal stem cells. (C) Suturing of the contralateral bulbar conjunctiva with 6–0 suture. (D) Completion of the surgery. |
Observations
Assessment parameters included patient comfort, wound healing status, stability of the prosthetic shell, improvement in palpebral fissure height and degree of eyeball protrusion after shell fitting. All cosmetic measurements, including palpebral fissure height (measured with a millimeter ruler at the central pupillary line) and exophthalmometry (measured using a Hertel exophthalmometer), were performed by the same experienced clinician under standardized lighting conditions to ensure consistency and reproducibility. Corneal irritation and pain were assessed using the standard, full-range Numeric Rating Scale (NRS). Corneal irritation and pain were assessed using the patient-reported Numeric Rating Scale (NRS, range 0–10) during each follow-up visit. The primary outcome for pain relief was based on the NRS score recorded at the three-month postoperative follow-up, ensuring that the assessment was conducted in a stable and healed state. Satisfaction was rated on a 5-point scale (1 = very dissatisfied, 2 = dissatisfied, 3 = neutral, 4 = satisfied, 5 = very satisfied). Photographs of the ocular appearance were taken preoperatively, postoperatively, and after prosthetic shell fitting. Examinations also included VA assessment and evaluation of the anterior segment and fundus of the contralateral eye. Cranial and orbital CT scans were performed to check for silicone oil droplets in the ventricles or orbit.
Statistical Analysis
Data were analyzed using SPSS version 19.0 (SPSS Inc., Chicago, IL, USA). Continuous data were tested for normality using the Shapiro–Wilk test. Normally distributed data were expressed as mean ± SD and compared using the Student’s t-test (for unpaired comparisons) or paired t-test (for paired comparisons). Non-normally distributed data were expressed as median with interquartile range (IQR) and analyzed using the Mann–Whitney U-test (unpaired) or Wilcoxon signed-rank test (paired). A p-value < 0.05 was considered statistically significant.
Results
A total of 24 patients (24 eyes) were enrolled in this study. The demographic and clinical characteristics are summarized in Table 1. The mean age of the patients was 31.38 ± 14.72 years. There were 16 males (66.7%) and 8 females (33.3%). The median intraocular pressure (IOP) was 5.6 mmHg (range, 4.2–9.1 mmHg). The mean silicone oil retention time (SORT) was 6.06 ± 3.22 years, with 16 eyes (66.67%) having SORT exceeding 5 years. Preoperatively, the median NRS pain score was 2 (IQR: 1.75–3.00), with 5 eyes (21.83%) presenting NRS scores greater than 3. Corneal decompensation was observed in 20 eyes (83.33%). One eye (4.27%) had a scar in the inner canthus. All 24 eyes (100%) exhibited eyeball atrophy. Four eyes (16.67%) required a second SO tamponade procedure. The mean postoperative follow-up duration was 4.75 ± 2.51years. During follow-up, all patients reported complete absence of pain and foreign body sensation or experienced immediate relief postoperatively. Conjunctival flaps healed firmly, with no congestion or discharge observed from the underlying corneal stroma.
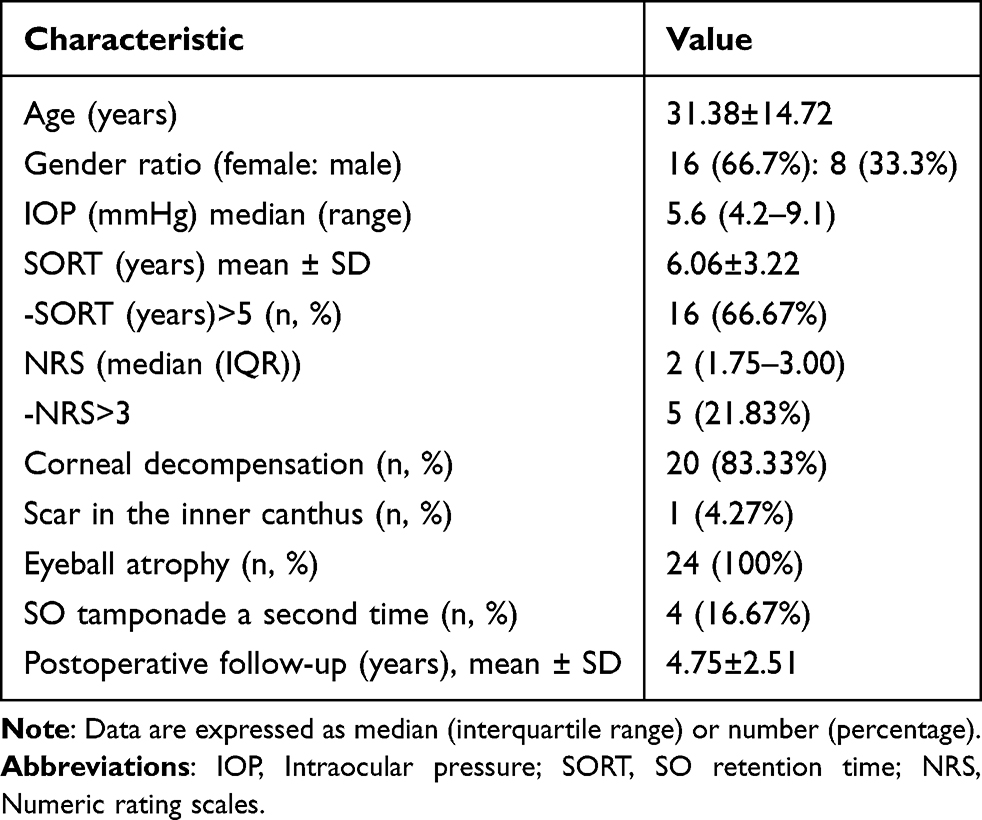 |
Table 1 Patient Characteristics |
A comparison of preoperative and postoperative characteristics is presented in Table 2. Significant improvements were observed in eyeball protrusion and palpebral fissure height after prosthetic shell fitting, resulting in improved bilateral symmetry. The globe and the previously smaller palpebral fissure showed no retraction during follow-up.
 |
Table 2 Comparison of Preoperative and Postoperative Characteristics |
Preoperatively, 18 eyes exhibited corneal decompensation, presenting with corneal edema and symptoms of foreign body irritation (Figure 1A). The silicone oil-filled eyes exhibited mild atrophy, accompanied by pseudoptosis and corneal irritation symptoms (Figure 2A and B). Additionally, band keratopathy was evident, accompanied by corneal irritation symptoms and ptosis (Figure 3A and B). Similarly, another patient exhibited ocular atrophy along with band keratopathy, pseudoptosis, and corneal irritation symptoms (Figure 4A and B). At 48 hours after shallow lamellar keratectomy combined with total conjunctival flap coverage, the conjunctiva had completely covered the corneal surface, with the underlying corneal tissue faintly visible (Figure 3C and C). At the one-month postoperative follow-up examination, the conjunctiva was observed to cover the corneal surface with reduced congestion, and the foreign body sensation had resolved (Figure 2C and D). At 1 to 3 months postoperatively, the appearance after prosthetic shell fitting is shown in Figures 2D and E, and D, demonstrating significant cosmetic improvement and restoration of normal palpebral fissure height.
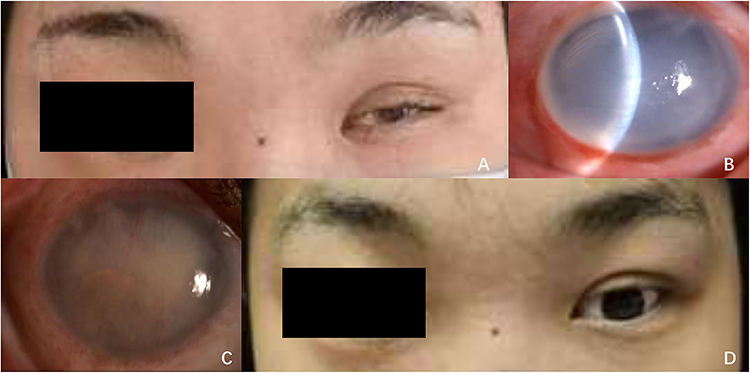 |
Figure 2 Silicone oil tamponade following left ocular trauma surgery in March 2008. (A) Follow-up examination in May 2013 revealed left eye phthisis bulbi, corneal irritation symptoms, and pseudoptosis. (B) Preoperative anterior segment photograph of the left eye. (C) Anterior segment photograph at 1 months postoperatively. (D) Appearance with prosthetic shell fitting at 1 year postoperatively. |
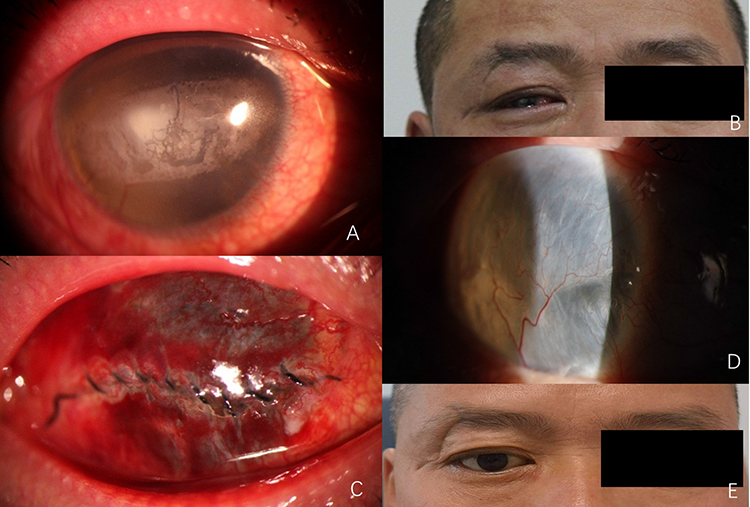 |
Figure 3 Retained silicone oil tamponade following left ocular trauma surgery in 2001. (A) Follow-up examination in July 2013 revealed band keratopathy with irritation symptoms in the right eye. (B) External appearance of the right eye before conjunctival flap coverage surgery. (C) Anterior segment photograph 48 hours after conjunctival flap coverage surgery. (D) Anterior segment photograph 1 months after conjunctival flap coverage surgery. (E) External appearance of the right eye after prosthetic shell fitting. |
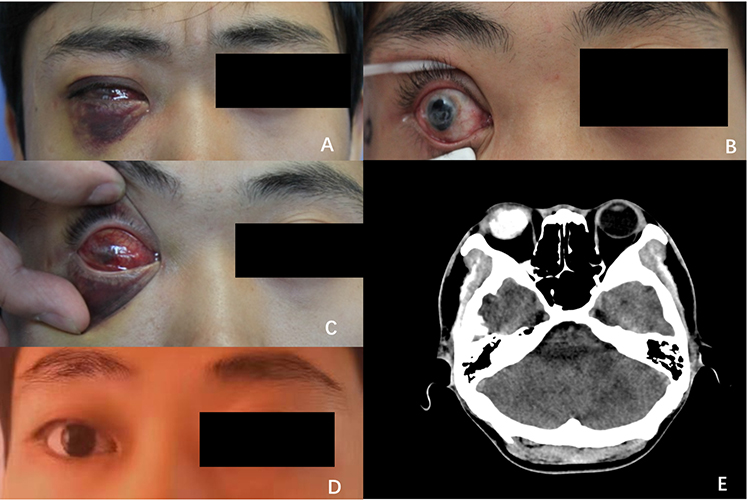 |
Figure 4 Retained silicone oil following right ocular trauma surgery in August 2010. (A) External appearance of the right eye after trauma. (B) Follow-up examination revealed corneal irritation symptoms and corneal edema. (C) External appearance 48 hours after conjunctival flap coverage surgery of the right eye. (D) Appearance 10 years after prosthetic shell fitting in the right eye. (E) CT scan at 3 years postoperatively showed the prosthetic shell positioned on the ocular surface, silicone oil filling in the right eye, and no silicone oil migration into the cerebral ventricles or orbit. |
Two eyes developed limbal epithelial implantation cysts (Figure 5A). Cyst incision was performed at 2 and 4 months postoperatively, respectively, with the surgical procedure illustrated in Figure 5. After injection of trypan blue into the cyst lumen, incision was made, and the inner and outer epithelial margins of the cyst incision were sutured with 10–0 nylon sutures. The cysts subsequently resolved without recurrence (Figure 5B–D). Following the reparative surgery, the conjunctival flaps healed firmly to the corneal stroma, achieving complete corneal coverage.
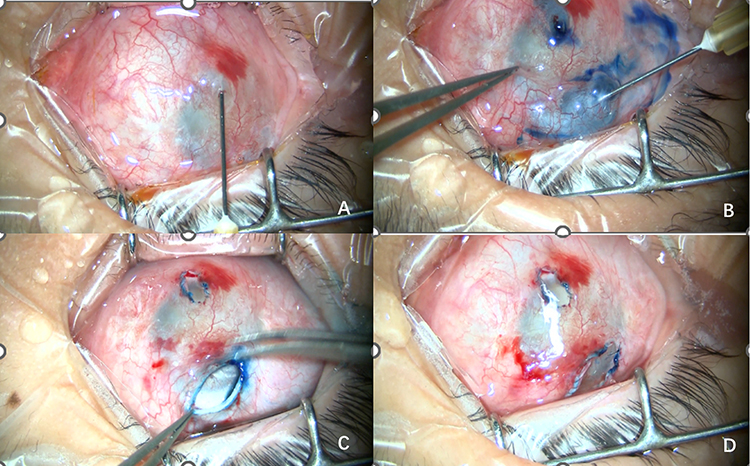 |
Figure 5 A case of conjunctival epithelial implantation cyst occurring 3 months after conjunctival flap coverage surgery and its surgical management. (A) Two epithelial implantation cysts located superior and inferior to the limbus at 3 months postoperatively. (B) The cysts were stained with methylene blue. (C) Incision of the cysts. (D) The inner and outer epithelial margins of the incision were apposed and sutured with 6–0 sutures. |
For the four eyes with smaller globes that required supplemental silicone oil (SO) filling to maintain intraocular pressure (IOP), computed tomography (CT) imaging confirmed the stable position of the SO-filled eyes and the prosthetic shells. Although a gap was present due to ocular deformation and shrinkage, the thickened prosthetic shells remained stable within the orbits and fitted well with the retained eyeballs (Figure 4E).
Discussion and Conclusion
This study is the first to systematically report the use of a modified Gundersen total conjunctival flap coverage combined with postoperative customized prosthetic shell fitting for managing atrophic, non-functional eyes resulting from long-term silicone oil (SO) tamponade following severe ocular trauma, aimed at improving appearance and alleviating symptoms. The results indicate that this combined approach can significantly enhance patient satisfaction and represents a safe, effective, and promotable conservative cosmetic rehabilitation strategy for the eyeball.
Severe ocular trauma often leads to extensive retinal and choroidal detachment, which in turn causes persistent hypotony. Currently, there is a lack of radical treatment in clinical practice for this condition, and the affected eye often progresses to phthisis bulbi and irreversible visual loss.1 With advancements in vitreoretinal surgical techniques, many severely injured eyes previously deemed unsalvageable, including those with no light perception (NLP), can now be spared from enucleation, with some even having the potential to recover light perception or limited visual function.5 However, when these aggressively repaired eyes remain in an NLP state and develop irritating symptoms due to corneal issues, there is a lack of effective intervention beyond enucleation/evisceration. Such surgeries are inherently traumatic, and the incidence of sympathetic ophthalmia has been proven to be low.4 Moreover, due to profound psychological fear and aversion to losing an eye, the vast majority of patients have a strong desire to retain the non-functional eye.16 Therefore, how to effectively address the cosmetic defects and discomfort caused by corneal opacity, edema, etc., in such atrophic eyes without resorting to enucleation has become a subject of significant clinical importance and humanistic concern. This study aims to investigate the safety and efficacy of a conservative combined surgical approach—superficial lamellar keratectomy combined with total conjunctival flap coverage, followed by customized prosthetic shell fitting—for improving ocular appearance and symptoms in these patients.
The modified Gundersen procedure (lamellar keratectomy combined with total conjunctival flap coverage) has been proven safe and effective for treating bullous keratopathy, advanced Acanthamoeba keratitis, and other ocular surface diseases.17–19 Building on this foundation, we applied this technique to SO-filled, preserved eyeballs, followed by prosthetic shell fitting, achieving satisfactory results in improving ocular appearance and eliminating corneal irritation secondary to edema. Compared to the traditional evisceration/enucleation combined with hydroxyapatite orbital implantation, this method simplifies the procedure by omitting the orbital implant and associated steps, thereby reducing surgical complexity and cost. It offers comparable efficacy in preserving extraocular muscles and maintaining a certain degree of ocular motility. Our clinical practice confirms that performing superficial lamellar keratectomy to eliminate the source of opacity or edema, followed by permanent ocular surface coverage with a well-vascularized total conjunctival flap, can create a stable and healthy foundation for subsequent prosthetic shell wear. The degree of atrophy in silicone oil-filled eyes varies; through customized prosthetic shells of different thicknesses, we can precisely compensate for the volume loss caused by atrophy, achieving a high degree of symmetry between the affected side and the healthy contralateral eye (as shown in Figures 2A and C and 3D and E)—an outcome difficult to achieve with fixed-size orbital implants.
Notably, the safety of performing such surgery on eyes with long-term silicone oil retention is a primary concern, and our study provides important evidence for the safety of this technique. Silicone oil tamponade is commonly used for retinal detachment, and although rare, migration into the cerebral ventricles has been reported.20,22 Tatewaki et al detected silicone oil in the lateral ventricle, demonstrating characteristic densities on CT and MRI.21 Cao et al utilized CT to track silicone oil and proposed that migration between the eye and brain may not be unidirectional.23 Sympathetic ophthalmia was a major concern. In this study, cranial CT revealed no ventricular abnormalities, suggesting no silicone oil migration and indicating stable retention of silicone oil within the vitreous cavity. Preoperatively and postoperatively, no signs of uveitis were observed in the contralateral healthy eyes. Therefore, this surgical approach achieved satisfactory clinical outcomes in improving appearance and alleviating corneal irritative symptoms, with no related complications observed in the operated eyes and no sympathetic ophthalmia induced in the fellow eyes.
For corneal irritation caused by conditions such as corneal dystrophy, conjunctival flap coverage surgery combined with postoperative prosthetic shell wear can effectively alleviate the irritation. In this study, the median preoperative pain score was a median score of 2, and the postoperative scores were all 0. All patients reported a reduction in pain. This consistent and marked relief can be attributed to the elimination of the primary pain source. The superficial lamellar keratectomy removes the diseased, edematous corneal epithelium and subepithelial nerve plexus, which are directly responsible for the nociceptive stimuli. Subsequently, the avascular, healed conjunctival flap provides a permanent, insensate barrier over the corneal surface, preventing recurrent irritation. Compared to the preoperative period, both ocular prominence and palpebral fissure height increased significantly after prosthetic shell fitting. Similar to the findings of Wu et al,24 who discovered that for eyeball atrophy occurring in patients with severe ocular trauma treated with foldable capsular vitreous body (FCVB) as a vitreous substitute, conjunctival flap coverage and prosthetic shell fitting could significantly improve patient appearance while preserving the eyeball, this suggests that such surgery not only alleviates ocular surface discomfort but also meets the patient’s psychological need to retain the eye, provides better cosmetic outcomes, and better preserves extraocular muscles and partial ocular motility. Furthermore, the lower surgical cost reduces the economic burden on patients. Patient postoperative satisfaction improved significantly.
Postoperatively, gradually enlarging conjunctival cysts at the limbus occurred in two eyes, likely due to residual limbal epithelial cells. Incising the cysts and suturing the epithelial margins effectively prevented recurrence, avoiding the need for conjunctival resection.
The present study has several limitations. First, as a retrospective case series with a relatively small sample size (n=24), the statistical power is limited, and we did not perform a priori power calculation. Second, the lack of a control group (eg, patients undergoing enucleation/evisceration or no intervention) precludes direct comparative effectiveness inferences. Third, our inclusion criteria required a “strong patient desire to improve ocular appearance.” This criterion, while ethically necessary and reflective of real-world clinical decision-making, inherently selects for a population with high motivation and potentially greater baseline willingness to be satisfied with surgical outcomes. Consequently, the exceptionally high postoperative satisfaction scores reported here may not be fully generalizable to all patients with similar anatomical conditions but differing psychological expectations. Despite these limitations, it demonstrates the efficacy of total conjunctival flap coverage combined with prosthetic shell fitting for SO-filled eyes.
In conclusion, for retained, atrophic, non-inflamed eyeballs following exploratory/reparative surgery and long-term SO retention due to OGI with ocular content loss, shallow lamellar keratectomy combined with total conjunctival flap coverage and subsequent prosthetic shell fitting can significantly improve ocular appearance and relieve corneal irritation symptoms. This study provides a novel therapeutic concept for managing ocular trauma sequelae. Further prospective studies with larger, controlled cohorts and extended long-term follow-up are warranted to confirm the durability of cosmetic outcomes, validate broader applicability, and directly compare this approach with conventional enucleation or evisceration procedures.
Abbreviations
SO, silicone oil; OGI, open globe injures; NRS, numeric rating scales; BK, band keratopathy; SORT, silicone oil retention time; VA, visual acuity; IOP, intraocular pressure; NLP, no light perception; CT, computerized tomography.
Ethics Approval and Consent to Participate
The Medical Ethics Committee of China-Japan Friendship Hospital approved the study protocol according to the declaration of Helsinki and all study participants gave their written informed consent. Informed consent was obtained from all participants or, if participants are under 16, from a parent and/or legal guardian.
Consent for Publication
All subjects and/or their legal guardian(s) publication gave their written statements attesting to informed consent of identifying information/images in an online open-access publication.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
The authors have no relevant affiliations or financial involvement with any organization or entity with a financial interest in or financial conflict with the subject matter or materials discussed in the manuscript. This includes employment, consultancies, honoraria, stock ownership or options, expert testimony, grants or patents received or pending, or royalties.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Gervasio Kalla A, Weinstock Brett M, Wu, et al. Prognostic value of ocular trauma scores in patients with combined open globe injuries and facial fractures. Am J Ophthalmol. 2015;160:882–888.e2. doi:10.1016/j.ajo.2015.08.007
2. Ing S, Tan AK, Hoskin A, et al. Prognostic factors of open-globe injuries: a review. Indian J Ophthalmol. 2023;71:3587–9. doi:10.4103/IJO.IJO_1496_23
3. Fujikawa A, Mohamed YH, Kinoshita H, et al. Visual outcomes and prognostic factors in open⁃globe injuries. BMC Ophthalmol. 2018;18(1):138. doi:10.1186/s12886-018-0804-4
4. Ying Z, Jialu Z, Caixia W, et al. Perioperative nursing of vitrectomy for ocular trauma under the guidance of ophthalmoscope. Contrast Media Mol Imaging. 2022;2022:8906306. doi:10.1155/2022/8906306
5. Deniz G, Mirza M, Okka E, et al. The causes and frequency of monocular and binocular blindness in adults applying to the health committee of a university hospital in central anatolia. Turk J Ophthalmol. 2021;51:282–287.x. doi:10.4274/tjo.galenos.2020.88120
6. Yang SS, Jiang T. Vitrectomy combined with silicone oil tamponade in the treatment of severely traumatized eyes with the visual acuity of no light perception. Int J Opthalmol. 2013;6(2):198–203.
7. Heidari E, Taheri N. Surgical treatment of severely traumatized eyes with no light perception. Retina. 2010;30(2):294–299. doi:10.1097/IAE.0b013e3181babd75
8. Salehi-Had H, Andreoli CM, Andreoli MT, et al. Visual outcomes of vitreoretinal surgery in eyes with severe open-globe injury presenting with no-light-perception vision. Graefes Arch Clin Exp Opthalmol. 2009;247(4):477–483. doi:10.1007/s00417-009-1035-4
9. Savar A, Andreoli MT, Kloek CE, et al. Enucleation for open globe injury. Am J Ophthalmol. 2009;147(4):595–600. doi:10.1016/j.ajo.2008.10.017
10. Feng K, Hu YT, Ma ZZ. Prognostic indicators for no light perception after open-globe injury: eye injury vitrectomy study. Am J Ophthalmol. 2011;152:654–662. doi:10.1016/j.ajo.2011.04.004
11. Ambar N, Merly L, Lorena A, et al. Risk factors leading to enucleation or evisceration in infectious endophthalmitis. J Clin Med. 2022;11.
12. Parikh Hardik A, Kalbag Neil S, Zarbin Marco A, et al. Characteristics, demographics, outcomes, and complications of diabetic traction retinal detachments treated with silicone oil tamponade. Eur J Ophthalmol. 2016;26:497–502. doi:10.5301/ejo.5000760
13. Shimmura-Tomita M, Takano, Takano H, et al. Status of corneal endothelial cells in the presence of silicone oil in the anterior chamber. Sci Rep. 2021;11:14055. doi:10.1038/s41598-021-93338-x
14. Kai H, Mengyu L, Yun Z, et al. Risk factors for band keratopathy in aphakic eyes with silicone oil tamponade for open-globe injuries: a multicenter case-control study. Front Med. 2021;8:713599. doi:10.3389/fmed.2021.713599
15. du Toit N, Motala MI, Richards J, Murray ADN, Maitra S. The risk of sympathetic ophthalmia following evisceration for penetrating eye injuries at Groote Schuur Hospital. Br J Ophthalmol. 2008;92:61–63. doi:10.1136/bjo.2007.120600
16. Rupesh A, Sue H, Wei S. Teoh,Predictive factors for final outcome of severely traumatized eyes with no light perception. BMC Ophthalmol. 2012;12:16. doi:10.1186/1471-2415-12-16
17. Gustavo C, María A, Carrasco A, et al. Treatment of advanced acanthamoeba keratitis with deep lamellar keratectomy and conjunctival flap. Cornea. 2002;21:705–708. doi:10.1097/00003226-200210000-00014
18. Mihail Z, Alina-Cristina S, Petru C, et al. Conjunctival flap surgery in the management of ocular surface disease (Review). Exp Ther Med. 2020;20:3412–3416. doi:10.3892/etm.2020.8964
19. Milena K, Szymon M, Nowak M, et al. The association between diabetes mellitus and keratoplasty in Poland in the years 2013-2017. Int J Environ Res Public Health. 2021;18. doi:10.3390/ijerph18189767
20. Yukako I, Sosuke I, Ideta, Ryuichi R. Ideta,Subretinal air migration after pars plana vitrectomy and air tamponade for rhegmatogenous retinal detachment. Am J Ophthalmol Case Rep. 2022;25:101279. doi:10.1016/j.ajoc.2022.101279
21. Tatewaki Y, Kurihara N, Sato A, et al. Silicone oil migrating from intraocular tamponade into the ventricles. J Computer Assisted Tomograp. 2011;35(1):43–45. doi:10.1097/RCT.0b013e3181fc938d
22. Matthew B, Potts A, Wu C, et al. Seeing floaters: a case report and literature review of intraventricular migration of silicone oil tamponade material for retinal detachment. World Neurosurg. 2018;115:201–205. doi:10.1016/j.wneu.2018.04.049
23. Cao J, Bian L, Zhou P, et al. Watch out for the special location of intraventricular silicone oil following an intraocular tamponade - a 10-year follow-up case report based on CT/MRI. BMC Ophthalmol. 2019;19(1). doi:10.1186/s12886-019-1286-8.
24. Ling-Dan W, Pei-Jie H, Zhou P, et al. Combined anterior corneal elastic sublaminectomy, conjunctival flap, and prosthetic eyepiece for ocular atrophy following foldable capsular vitreous body implantation in severe trauma. Int J Ophthalmol. 2025;18:2149–2154. doi:10.18240/ijo.2025.11.18
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.