Back to Journals » Drug, Healthcare and Patient Safety » Volume 17
A Nomogram for Predicting Survival in Patients with Respiratory Failure Following Trauma: A Retrospective Study Using the MIMIC-IV Database
Received 22 September 2024
Accepted for publication 19 February 2025
Published 5 March 2025 Volume 2025:17 Pages 63—74
DOI https://doi.org/10.2147/DHPS.S497413
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Dr Rajender Aparasu
Peihan Li, Xuejuan Wang, Li Li
Department of Anesthesiology, Beijing Friendship Hospital, Capital Medical University, Beijing, People’s Republic of China
Correspondence: Li Li, Department of anesthesiology, Beijing Friendship Hospital, Capital Medical University, Beijing, People’s Republic of China, Email [email protected]
Background: Respiratory failure (RF) after trauma is one of the major causes of patients being admitted to the ICU and leads to a high mortality rate. However, we cannot predict mortality rates based on patients’ various indicators. The aim of this study is to develop and validate a nomogram for predicting mortality in patients in the intensive care unit (ICU).
Methods: A total of 377 patients from the Medical Information Mart for Intensive Care (MIMIC)-IV database were included in the study. All participants were systematically divided into a development cohort for modelling and a validation cohort for internal validation at a ratio of 7:3. Following patient admission, a comprehensive collection of 30 clinical indicators was performed. The least absolute shrinkage and selection operator (LASSO) regression technique was employed to discern pivotal risk factors. A multivariate Cox regression model was established, and a receiver operating curve (ROC) was plotted, and the area under the curve (AUC) was calculated. Furthermore, the decision curve analysis (DCA) was performed, and the nomogram was compared with the acute physiology score III (APSIII) and Oxford acute severity of illness score (OASIS) scoring systems to assess the net clinical benefit.
Results: The indicators included in our model were age, OASIS score, SAPS III score, respiratory rate (RR), blood urea nitrogen (BUN) and hematocrit. The results demonstrated that our model yielded satisfied performance on the development cohort and on internal validation. The calibration curve underscored a robust concordance between predicted and actual outcomes. The DCA showed a superior clinical utility of our model in contrast to previously reported scoring systems.
Conclusion: In summary, we devised a nomogram for predicting mortality during the ICU stay of RF patients following trauma and established a prediction model that facilitates clinical decision making. However, external validation is needed in the future.
Keywords: a nomogram for predicting mortality, respiratory failure following trauma, MIMIC-IV database
Background
Respiratory failure (RF) is a complex condition characterized by the inability of the respiratory system to fulfil the patient’s oxygenation, ventilation, and metabolic requirements at rest and during activity. RF is also a major cause of morbidity and mortality in patients admitted to the intensive care unit (ICU). Clinically, RF is considered as a primary and prevalent cause of illness and mortality, and it is diagnosed when the PaO2 is less than 60 mmHg with or without an increase in carbon dioxide when the patient inhales room air. The causes of RF involve abnormalities in the central respiratory drive, spinal cord, motor nerves, skeletal muscle, airway and lungs. In the study of the severity of ARDS in trauma patients, it was found that the incidence of respiratory distress syndrome (ARDS) was 16%, of which 36% was severe.1 Severe trauma is frequently associated with thoracic rib fractures and abdominal organ injuries. In the diagnosis and treatment of ARDS and RF, our main goal is prevention. Because once ARDS and RF occurs, it is a late complication and an irreversible predictor of mortality.2
Estimating the incidence and prevalence of RF is challenging owing to its syndromic nature, as RF encompasses diverse pathological processes rather than a singular entity.3 Notably, one of the primary reasons for admission to the ICU among RF patients is trauma.4 Furthermore, the mortality of patients with trauma is significantly greater than that of the general population.5 Posttraumatic RF is a common complication that is particularly common in patients with diverse types of trauma and may lead to dire consequences. Therefore, exploring the living state of patients in the ICU with posttraumatic RF is highly valuable.
Recently, research has shown that models of respiratory mechanics, are required for guiding patient-specific mechanical ventilation settings in the ICU.6 RF is associated with increased morbidity and mortality in elderly patients and has a poor prognosis, especially among patients who undergo pneumonectomy.7 Mechanical ventilation is a life-saving intervention in patients with trauma-related RF, paradoxically, it has the potential for increased mortality and morbidity. Numerous studies have revealed that ultrasonography of the diaphragm improves diagnostic performance and can be used to predict extubation outcomes.8–10
In addition, other published predictive models (eg Assess Respiratory Risk in Surgical Patients in Catalonia, Prospective Evaluation of a Risk Score for Postoperative Pulmonary Complications in Europe, and Local Assessment of Ventilatory Management During General Anaesthesia for Surgery) focused on all postoperative pulmonary complications, ranging from atelectasis to respiratory failure, which occurred in 5% to 11% of patients.9 These models focus on all postoperative pulmonary complications and the inclusion of emergency surgeries makes extrapolation to elective surgery populations challenging, and external validation of the models in the patient population including the duration of anesthesia, the type of operation, and net fluid balance in the operating room is impossible.11 Few studies have investigated the long-term survival of patients with posttraumatic RF. Therefore, as RF is a complication with high mortality, it is essential to predict the rate of death of patients with RF in the ICU. However, to date, no model has been developed to predict the long-term mortality of patients with RF in the ICU. Nomograms are characterized by simplicity and visual effectiveness and have thus gained prominence as statistical tools for predicting disease occurrence, development, prognosis, and survival. Our study aimed to establish a nomogram grounded in routine clinical and laboratory parameters, thus ensuring its practical implementation in clinical settings.
Methods
Data Sources and Study Population
All the study data were obtained from the MIMIC-IV database,12 which is a publicly available database sourced from the electronic health records of the Beth Israel Deaconess Medical Center.13 The database contains comprehensive and anonymized clinical data from more than 70,000 ICU admissions between 2008 and 2019. To comply with relevant regulations, Xuejuan Wang obtained the Collaborative Institutional Training Initiative (CITI) licence and passed the CITI exam to obtain a certificate to access the database (certificate number: 60448105).
We extracted patient information from the MIMIC-IV database and analysed posttraumatic RF patients who were admitted to the ICU. Through the International Classification of Diseases 9th Edition (ICD-9) code=5185%, we obtained 1282 patients. The inclusion criteria were as follows: (1) patients were diagnosed with acute, chronic or unclassified respiratory insufficiency following trauma; (2) patients had relatively complete data on potential predictors. The exclusion criteria were as follows: (1) diagnostic sequence >5 in the MIMIC-IV database; (2) missing data >20% for vital signs or laboratory tests; (3) considering the possibility of major diseases prior to trauma, which may affect the final outcome, we also excluded patients who were repeatedly admitted to the ICU. Ultimately, 377 patients were included in the study (Figure 1). The primary endpoint of this study was the mortality rate of RF patients following trauma at one month, six months and one year. This study was exempt from ethics investigations from the Beijing Friendship Hospital affiliated with the Capital Medical University ethics committee (ID:2024-P2-242). The data for the included patients were derived from publicly available databases.
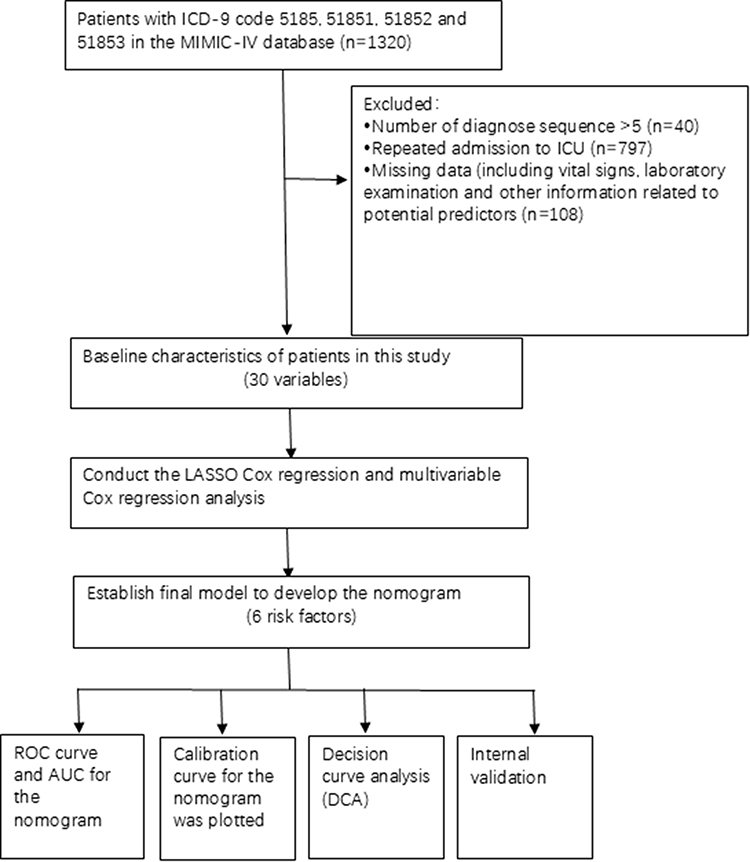 |
Figure 1 Workflow of the study. Abbreviations: MIMIC-IV, Medical Information Mart for Intensive Care IV; LASSO, least absolute shrinkage and selection operator; ROC, receiver operating characteristic; AUC, area under the curve. |
Missing Data
The missing data of variables in this study had missing values of <5% and were all quantitative data. We imputed the missing values via the missForest method in the mice R package and incorporated all of the data for modelling.14
Statistical Analysis
Normally distributed continuous data are presented as the mean ± SD and were analyzed via unpaired, 2-tailed t-tests; nonnormally distributed continuous data are presented as the medians and interquartile ranges (IQRs) and were analysed via the Mann–Whitney U-test. Categorical data are presented as numbers (%) and were analysed via the chi-squared test. When the counts of the categorical variables were <5, Fisher’s exact test was used.
First, the total participants were randomly split into a development cohort and a validation cohort at a ratio of 7:3 to perform internal validation of the model. We conducted a balance test between the two datasets. The patients in the development cohort were subsequently categorized into two groups, namely, the death group and the survival group, based on their survival status. A comparison of variables was subsequently conducted between these two groups.
In the development cohort, LASSO Cox regression was used to analyse the potential risk factors, which is a shrinkage and variable selection method for a linear regression model. LASSO regression minimizes the risk of prediction error for a quantitative response variable by imposing a constraint on the model parameters that cause the regression coefficients for some variables to shrink towards zero. We also use k-fold (tenfold in this case) cross-validation for centralization and normalization of the included variables and then pick the optimal lambda value with good performance. Therefore, the LASSO method was used to analyse the data in the development cohort to select the optimal predictors of the present risk factors, including age, the APSIII score, OASIS,15 RR, BUN and Hematocrit. The risk factors were initially screened using these abovementioned inclusion variables.
We then conducted a multivariable Cox regression analysis using a backwards stepdown selection process with the Akaike information criterion by introducing the features selected in the LASSO regression model. The features were considered hazard ratios and a P value with a 95% confidence interval. The statistical significance levels were all two-sided.
A nomogram was subsequently formulated as the prediction model on the basis of the selected variables. To assess the reproducibility and robustness of the model, internal validation was subsequently used in the validation cohort. The C-index, displayed as the area under the receiver operating characteristic (ROC) curve, was used to assess the discriminative performance of this prediction model. The calibration plots were used to assess the accuracy of the prediction model. In addition, decision curve analysis (DCA) was implemented to estimate the clinical availability and benefits of the nomogram. In brief, our study used ROC curves, calibration plots, and DCA to evaluate the performance of the nomogram. The performance of the developed model was compared with that of the SOFA score and the APS III score via decision curve analysis.
All the statistical analyses were performed via R software version 4.3.1 (R Foundation for Statistical Computing). For all analyses, two-sided p values <0.05 were considered statistically significant.
Results
Patients Characteristics
A total of 377 eligible patients were ultimately included in this study; these patients were randomly divided into a development cohort (n=263) and a validation cohort (n=114). The baseline characteristics of all the enrolled patients are listed in Table 1, which indicates that there was no difference between the development cohort and the validation cohort. In our study, the median age (IQR) of the patients was 70.0 [52.0;80.0]. A total of 57.6% (n=217) of the patients were female, and the mortality rate was 24.0%; 42.4% (n=160) of the patients were male, and their mortality rate was 34.4%. We also compared the differences in patient characteristics between the survival group and death group. Compared with those in the survival group, patients in the death group were older (64.0 [46.0;75.0] vs 80.0 [71.0;87.0]), had faster respiratory rates(19.0 [17.0;21.0] vs 21.0 [18.0;24.0]), and had higher PT14.4 ([12.8;16.4] vs 15.6 [13.3;19.8]), PTT (31.6 [28.1;40.1] vs 38.3 [29.4;64.4]) and INR (1.30 [1.10;1.50] vs 1.40 [1.20;1.80]) values, thus indicating poor coagulation function. Moreover, there was a significant difference between the survival and death groups in terms of DBP, MBP, SpO2, blood glucose, BUN, bicarbonate, and creatinine levels and treatment with vasoactive agents. In addition, the APSIII, OASIS and SOFA scores were significantly higher.
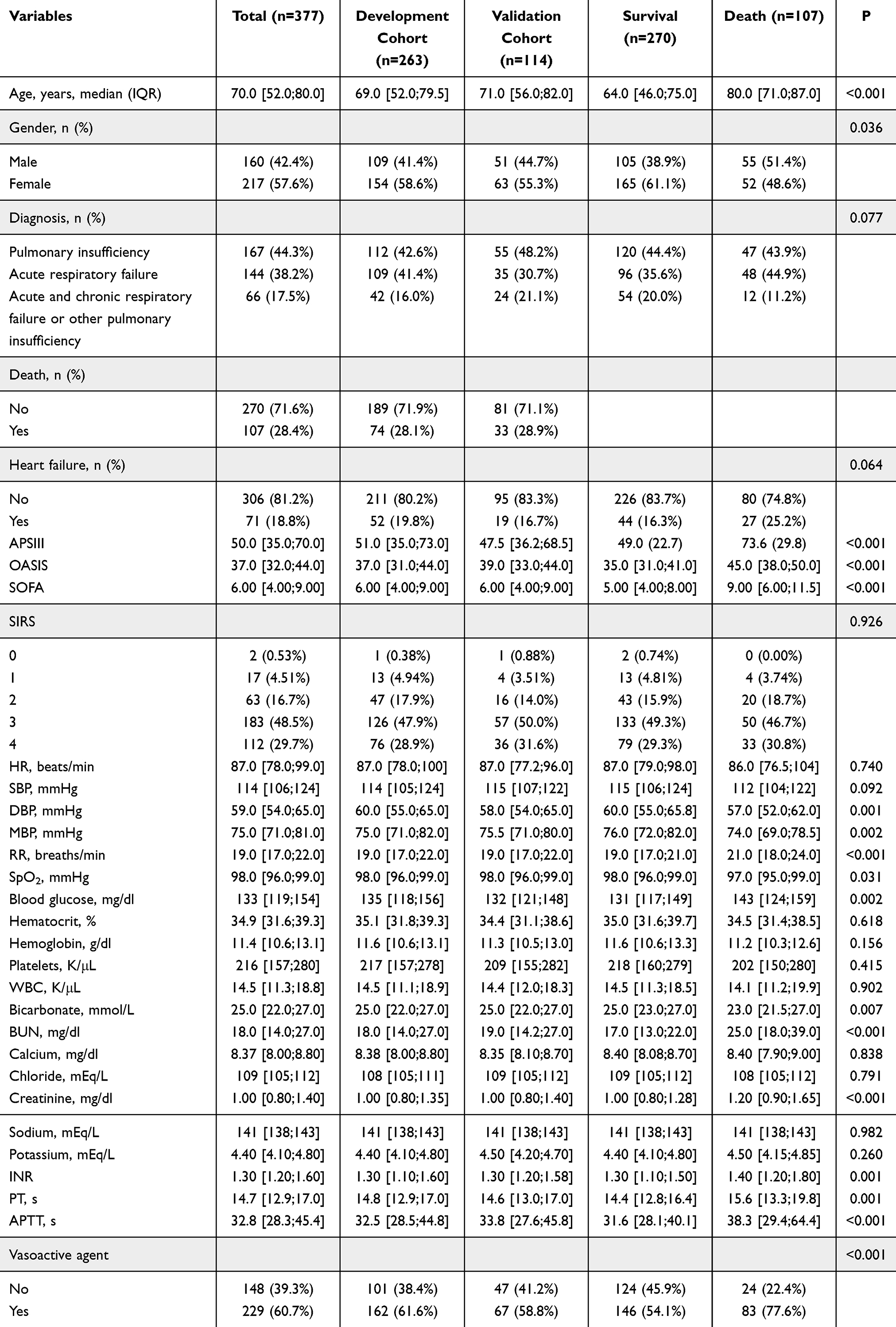 |
Table 1 Characteristics of the Patients With Pulmonary Insufficiency Following Trauma Enrolled in the Study According to Live or Dead and Randomization to Development and Validation Cohorts |
Selection of Patient Characteristics and Risk Prediction Nomogram Development
The following six variables remained in the LASSO Cox regression model after applying the binomial deviance minimum criteria (Figure 2A and B): age (HR: 1.067; 95% CI 1.043–1.090), the APSIII score (HR: 1.013; 95% CI 1.000–1.027), OASIS (HR: 1.037; 95% CI 0.999–1.075), RR (HR: 1.041; 95% CI 0.979–1.107), BUN (HR: 1.018; 95% CI 1.007–1.030), and hematocrit (HR: 1.045; 95% CI 1.000–1.092) (Table 2). Multivariate Cox regression analysis revealed that age, the APSIII score, BUN levels and hematocrit levels were independent prognostic factors for mortality in patients with respiratory failure following trauma.
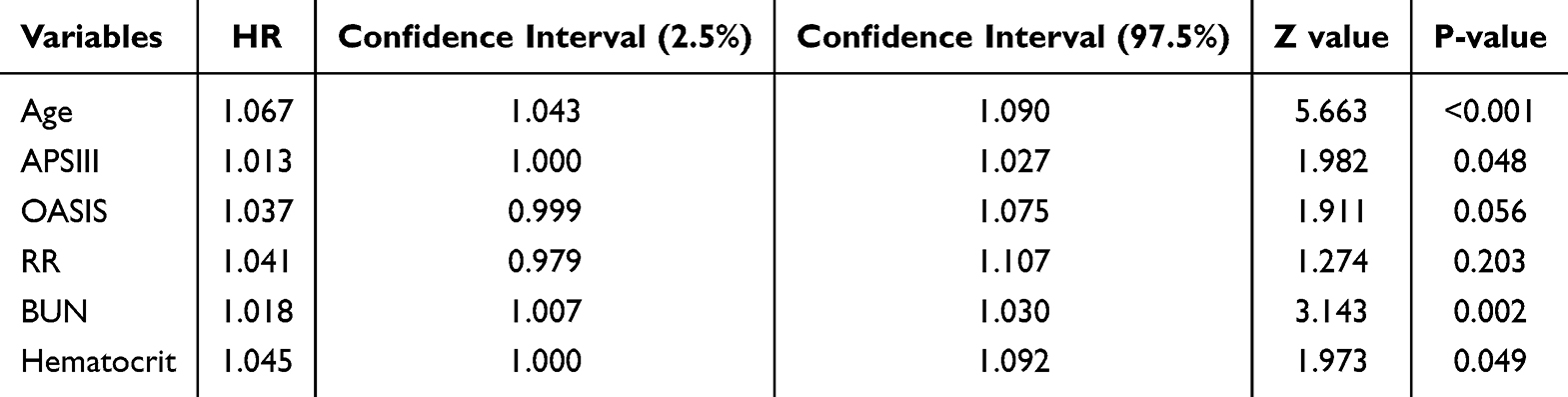 |
Table 2 Multivariate Regression Model Based on LASSO Regression Results |
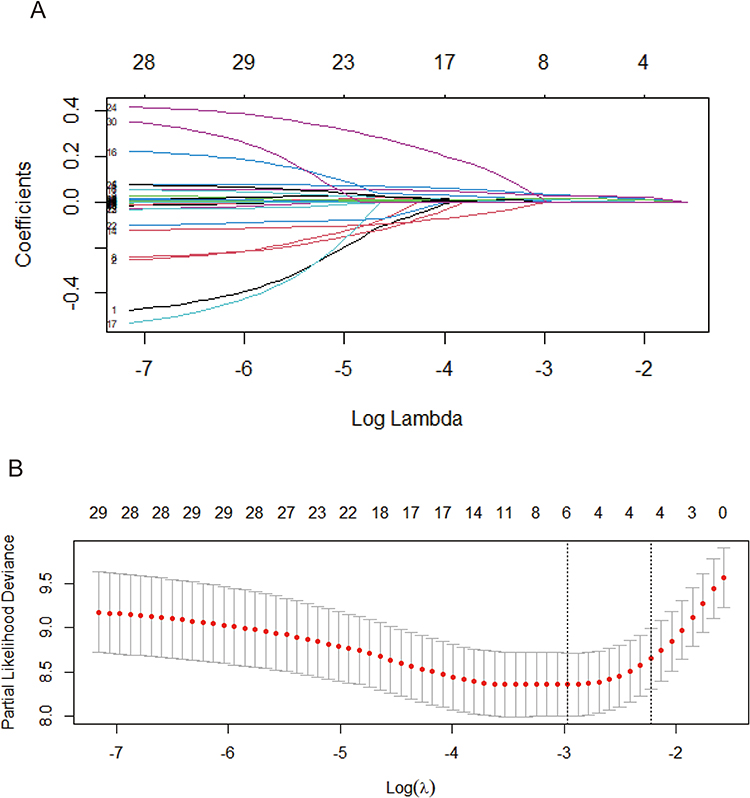 |
Figure 2 Clinical variables were selected via the LASSO Cox regression model. A coefficient profile plot was constructed against the log(lambda) sequence. (A) Tuning parameter (λ) selection via LASSO penalized logistic regression with 10-fold cross-validation. (B) Following verification of the optimal parameter (lambda) in the LASSO model, we plotted the partial likelihood deviance (binomial deviance) curve versus log(lambda) and drew dotted vertical lines based on 1 standard error criterion. Abbreviation: LASSO, least absolute shrinkage and selection operator. |
Based on the LASSO results, we constructed a nomogram to predict the probability of death in ICU patients with pulmonary insufficiency following trauma (Figure 3A). For example, according to the nomogram model, for a patient with posttraumatic RF at 39 years of age, and an RR of 16 breaths/min, a hematocrit level of 25.5%, a BUN of 12 mg/dl, an APSIII score of 91 and an OASIS score of 43, the estimated risk of death at one month, six months and one year was 1.84%, 2.47% and 2.66%, respectively (Figure 3B). Furthermore, to facilitate clinical use, we constructed a web calculator (https://tudoutudouni.shinyapps.io/DynNomapp/). We used the DynNom and the resconnect R package with the associated R shiny web app to implement this function.
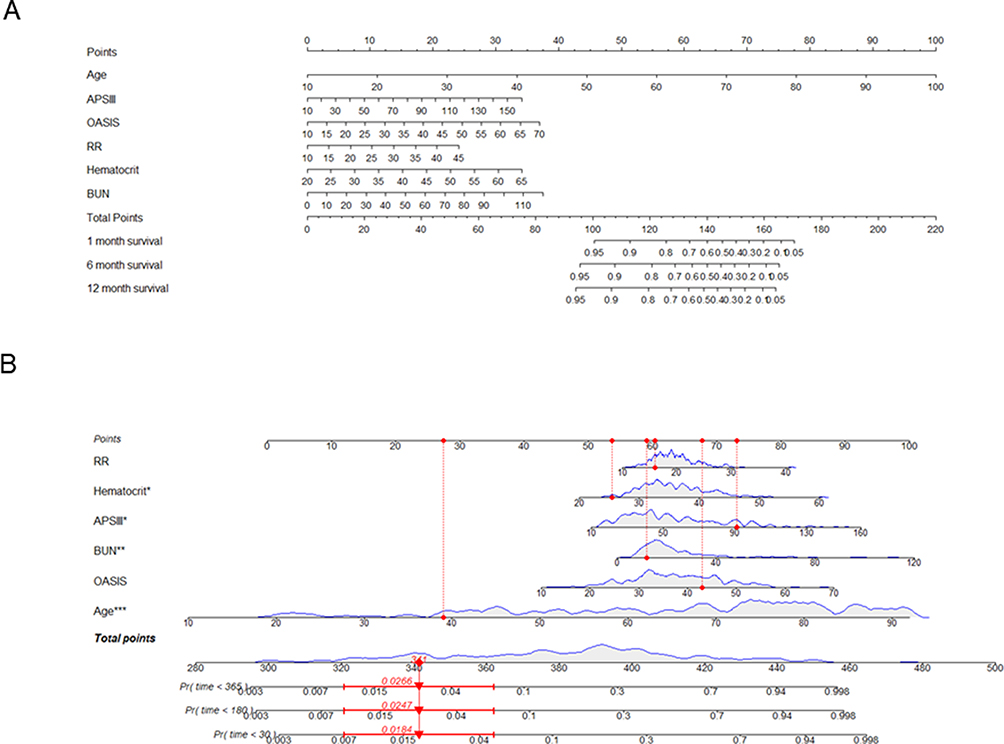 |
Figure 3 (A) Risk factors for hematocrit, APSIII, BUN, OASIS, RR and age according to the nomogram prediction model. (B) Dynamic nomogram used as an example. |
Predictive Model Validation
To verify the performance of the established nomogram, an ROC curve was used to evaluate the discriminatory capacity of the predictive model. For the predictive model, we calculated the pooled area under the ROC curve (AUC) values for the nomogram in the development cohort and validation cohort (Figure 4A and B). In the development cohort, the AUC values at 1 month, six months and 1 year were 0.864, 0.881 and 0.890, respectively, and in the validation cohort, the AUC values at 1 month, 6 months and 1 year were 0.822, 0.827 and 0.834, respectively. These values indicate moderately good performance. Moreover, a calibration curve was used to describe the fitting ability of the model in the development and validation cohorts. Figure 5 shows that the established model exhibited good agreement between the predictive and actual survival statuses at 1 month, 6 months and 1 year in the development and validation cohorts.
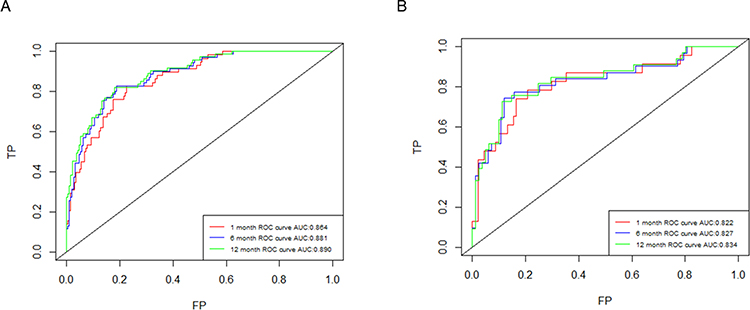 |
Figure 4 Receiver operating characteristic curve (ROC) validation of the nomogram prediction. The y-axis represents the true positive rate of the risk prediction, and the x-axis represents the false positive rate of the risk prediction. The red line represents the performance of the nomogram in the development cohort (A) and validation cohort (B) at 1 month, the blue line represents 6 months and the green line represents 1 year. |
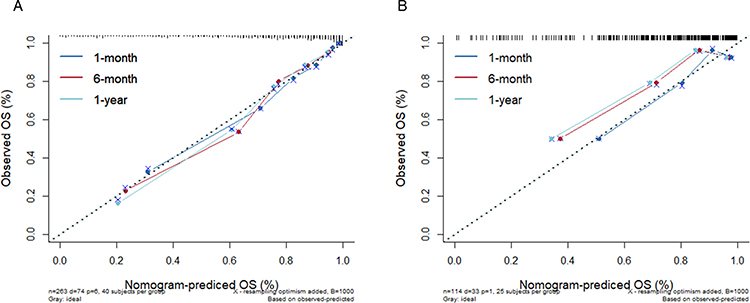 |
Figure 5 Calibration curves of the predictive RF death risk nomogram. The y-axis represents the actual death risk of the RF following trauma, and the x-axis represents the predicted death risk of the RF following trauma. The diagonal dotted line represents a perfect prediction by an ideal model, and the solid line represents the performance of the development (A) and validation cohorts (B), with the results indicating that a closer fit to the diagonal dotted line represents a better prediction. |
Clinical Practice
Finally, we plotted the DCA curves to compare the clinical application of the developed model, the APS III score and the OASIS score (Figure 6). The straight green-yellow curve in the figure represents the assumption that no patients exhibited long-term overall survival (OS), the orange line represents the assumption that all patients exhibited long-term OS, and the green curve represents the clinical benefit of our model. The DCA curves indicated that our model had a greater net clinical benefit than the OASIS and APS III scoring systems did, which means that the established model has greater clinical value than the OASIS and APS III scoring systems do.
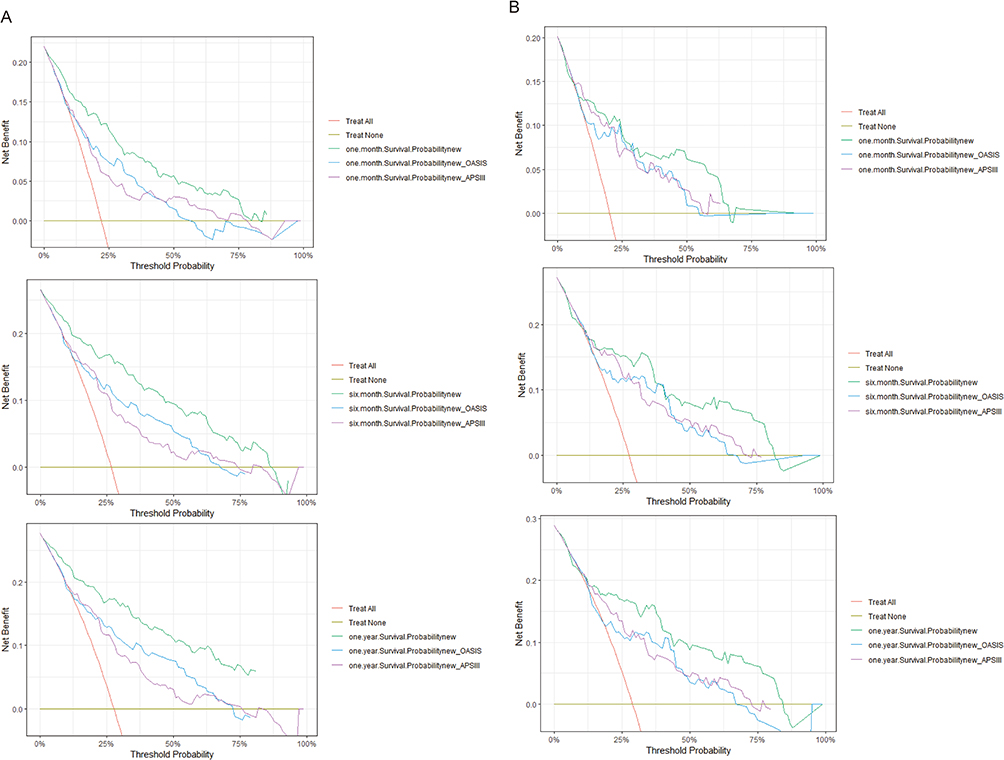 |
Figure 6 DCA of the nomogram for OS in both the development (A) and validation (B) cohorts. |
Discussion
RF is one of the most common reasons for hospitalization and ICU admissions and is associated with increases in health care expenses, mortality rates and lengths of hospital stay.16,17 Predicting mortality in ICU patients with posttraumatic RF could improve the management and prognosis of RF-related complications. Because trauma often causes significant damage to various organs of patients, the fundamental purpose of all our medical treatments is to save their lives. While existing treatments for RF demonstrate notable symptom relief, the absence of an effective and pragmatic scoring system for mortality prediction remains a noteworthy gap. Our comprehensive study included 30 variables and identified 6 key factors, including age, the APSIII score, the OASIS score, RR, BUN and hematocrit. These variables were seamlessly integrated into the nomogram for predicting the mortality outcomes of patients with posttraumatic RF and succeeded in constructing a model to predict and validate the mortality outcomes for these patients at three time points. This approach contributes to the understanding and management of RF-related challenges and provides guidelines for critical care research.
These changes, in turn, may result in increased morbidity.18–20 Our study also confirmed that age was an independent risk factor, and we succeeded in constructing a model to predict and validate the mortality outcomes for these patients at three time points. This approach contributes to the understanding and management of RF-related challenges and provides guidelines for critical care post-RF. Ageing increases the risk of postoperative complications because of the decrease in physiologic reserve and airway defence; these limitations are more likely to become apparent after the stressors of trauma, surgery and anaesthesia.21 The APS II (Acute Physiology Score II) and APS III are international multidimensional instruments designed for the comprehensive assessment of ICU admission mortality estimates.22,23 Emerging evidence suggests that the APSIII is a valuable tool for predicting mortality and may surpass the performance of the APSII and APCHEII (Acute Physiology and Chronic Health Evaluation II).24–26 APSIII was also an independent risk factor in our study. The SIRS, APSIII, OASIS and SOFA scores have been widely used to assess disease severity and predict in-hospital mortality in the ICU; however, a single scoring system cannot accurately indicate the magnitude of the mortality rate. In the model we established, we found that modelling with the APSIII and OASIS scoring systems rather than the SOFA and SIRS scoring systems was more effective in predicting patient mortality. In addition, our model can provide greater net clinical benefits to patients than a single APSIII or OASIS scoring system. Notably, both the APSIII and OASIS scores encompass respiratory status, which underscores the importance of not only factors such as age, BUN, and haematocrit levels but also mechanical ventilation and RR. However, certain variables within the APSIII and OASIS scores, such as HR, T, and WBC, were excluded from the final model construction following separate extraction for statistical analysis. The associations of BUN and hematocrit levels with pulmonary disease have been well documented in prior studies;27–29 interestingly, BUN is one of the risk factors for mortality in elderly patients with acute kidney injury or heart failure.30,31 Moreover, our findings suggest that BUN is also associated with disease and related surgeries.32,33 We also examined whether patients had heart failure; however, in our study, we did not find a significant difference between the survival and death groups (226 (83.7%) vs 80 (74.8%)), which may be related to our insufficient sample size or the type of population included in the study.
In this study, we found considerable differences in age, the APSIII score, the OASIS score, the SOFA score, DBP, MBP, RR, bicarbonate, blood glucose, creatinine, PT, APTT, the INR and the use of vasoactive agents between the survival and death groups. The ROC curves of our model in the development and validation cohorts were 0.864 and 0.822 at 1 month, 0.881 and 0.827 at 6 months, and 0.890 and 0.834 at 1 year, respectively, which indicated that the nomogram had good discrimination ability in predicting mortality for patients with traumatic respiratory insufficiency. Moreover, the calibration curves also revealed that the nomogram had good accuracy for predicting mortality. Finally, the DCA curves in our study indicated that the model has greater net benefit than the APSIII and OASIS scoring systems of clinical value. With the nomogram, an individual predictive score of mortality can be measured for any individual. The critical care physicians can use the nomogram in multidisciplinary team meetings to make real-time decisions, accurately assess the severity of disease and predict the prognosis of critically ill patients.34 However, the intensive care doctors should not rely solely on predictive scores, and should take into account the actual clinical situation of each patient to achieve individualized treatment.
Our study has several limitations. First, it was a retrospective study, and inherent bias was challenging to avoid. Second, although the database has relatively complete data, the sample size that met the inclusion criteria was still relatively small. Previous studies have shown that the risk factors for postoperative pulmonary complications are age, surgery type, smoking, preoperative anaemia, general anaesthesia, and intraoperative ventilation strategies,17 and the incidence of posttrauma pulmonary complications is also associated with surgical intervention and the number of surgeries.35 However, our study did not include surgery- or anesthesia-related variables, and it is necessary to conduct larger-scale multicentre studies to validate the applicability of this model in the future.
Conclusions
This research established a nomogram that includes the variables of age, APSIII, OASIS, respiratory rate, hematocrit levels and BUN, which can be applied to accurately predict the ICU mortality of ICU patients with post traumatic RF. Treatment strategies should consider the relevant factors in the model, which may improve in-hospital survival rates for these ICU patients.
Abbreviations
RF, Respiratory failure; ICU, intensive care unit; MIMIC-IV database, Medical Information Mart for Intensive Care; LASSO, least absolute shrinkage and selection operator; ROC, receiver operating curve; AUC, area under the curve; DCA, decision curve analysis; APSIII, acute physiology score III; OASIS, Oxford acute severity of illness score; RR, respiratory rate; BUN, blood urea nitrogen; ICD-9, International Classification of Diseases 9th Edition.
Data Sharing Statement
We obtained both a Collaborative Institutional Training Initiative (CITI) licence and the necessary permissions to utilize the MIMIC-IV database.
Acknowledgments
The authors are grateful for the cooperation and participation of the anesthesiologists in the department of anesthesiology and the instructions from the corresponding author.
Author Contributions
Peihan Li and Xuejuan Wang contributed equally and shared first authorship with the manuscript. All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
There is no funding to report.
Disclosure
The authors declare that they have no competing interests in this work.
References
1. Daher P, Teixeira PG, Coopwood TB, et al. Mild to moderate to severe: what drives the severity of ARDS in trauma patients? Am Surg. 2018;84(6):808–812. doi:10.1177/000313481808400623
2. Birkner DR, Halvachizadeh S, Pape HC, Pfeifer R. Mortality of adult respiratory distress syndrome in trauma patients: a systematic review over a period of four decades. World J Surg. 2020;44(7):2243–2254. doi:10.1007/s00268-020-05483-5
3. Lamba TS, Sharara RS, Singh AC, Balaan M. Pathophysiology and classification of respiratory failure. Crit Care Nurs Q. 2016;39(2):85–93. doi:10.1097/CNQ.0000000000000102
4. Karamchandani K, Khorsand S, Ebeling C, Yan L, Nakonezny PA, Carr ZJ. Predictors of failure to rescue after postoperative respiratory failure: a retrospective cohort analysis of 13,047 patients using the ACS-NSQIP dataset. J Surg Res. 2024;293:482–489. doi:10.1016/j.jss.2023.09.030
5. Frydrych LM, Keeney-Bonthrone TP, Gwinn E, Wakam GK, Anderson MS, Delano MJ. Short-term versus long-term trauma mortality: a systematic review. J Trauma Acute Care Surg. 2019;87(4):990–997. doi:10.1097/TA.0000000000002430
6. Redmond DP, Chiew YS, Major V, Chase JG. Evaluation of model-based methods in estimating respiratory mechanics in the presence of variable patient effort. Comput Methods Programs Biomed. 2019;171:67–79. doi:10.1016/j.cmpb.2016.09.011
7. Wang G, Wu X, Sun X, et al. Value of N1 lymph node examination in the prognosis of patients with pT1-3N0M0 non-small cell lung cancer. Front Oncol. 2020;10:603378. doi:10.3389/fonc.2020.603378
8. De Carvalho H, Javaudin F, Le Bastard Q, Boureau AS, Montassier E, Le Conte P. Effect of chest ultrasound on diagnostic workup in elderly patients with acute respiratory failure in the emergency department: a prospective study. Eur J Emerg Med. 2021;28(1):29–33. doi:10.1097/MEJ.0000000000000732
9. Palkar A, Narasimhan M, Greenberg H, et al. Diaphragm excursion-time index: a new parameter using ultrasonography to predict extubation outcome. Chest. 2018;153(5):1213–1220. doi:10.1016/j.chest.2018.01.007
10. Raj I, Kumar Nagaiah S. Ultrasonography of diaphragm to predict extubation outcome. Cureus. 2023;15(3):e36514. doi:10.7759/cureus.36514
11. Stocking JC, Taylor SL, Fan S, et al. A least absolute shrinkage and selection operator-derived predictive model for postoperative respiratory failure in a heterogeneous adult elective surgery patient population. CHEST Crit Care. 2023;1(3):100025. doi:10.1016/j.chstcc.2023.100025
12. Johnson A, Bulgarelli L, Pollard T, Horng S, Celi LA, Mark R. MIMIC-IV (version 2.0). 2022. doi:10.13026/7vcr-e114
13. Johnson AEW, Bulgarelli L, Shen L, et al. MIMIC-IV, a freely accessible electronic health record dataset. Sci Data. 2023;10(1):1. doi:10.1038/s41597-022-01899-x
14. Stekhoven DJ, Buhlmann P. MissForest--non-parametric missing value imputation for mixed-type data. Bioinformatics. 2012;28(1):112–118. doi:10.1093/bioinformatics/btr597
15. Johnson AE, Kramer AA, Clifford GD. A new severity of illness scale using a subset of acute physiology and chronic health evaluation data elements shows comparable predictive accuracy. Crit Care Med. 2013;41(7):1711–1718. doi:10.1097/CCM.0b013e31828a24fe
16. Nicolini A, Stieglitz S, Bou-Khalil P, Esquinas A. Cost-utility of non-invasive mechanical ventilation: analysis and implications in acute respiratory failure. A brief narrative review. Respir Investig. 2018;56(3):207–213. doi:10.1016/j.resinv.2017.12.011
17. Miskovic A, Lumb AB. Postoperative pulmonary complications. Br J Anaesth. 2017;118(3):317–334. doi:10.1093/bja/aex002
18. Frederick DE. Pulmonary issues in the older adult. Crit Care Nurs Clin North Am. 2014;26(1):91–97. doi:10.1016/j.ccell.2013.09.008
19. Skloot GS. The Effects of Aging on Lung Structure and Function. Clin Geriatr Med. 2017;33(4):447–457. doi:10.1016/j.cger.2017.06.001
20. Schneider JL, Rowe JH, Garcia-de-Alba C, Kim CF, Sharpe AH, Haigis MC. The aging lung: physiology, disease, and immunity. Cell. 2021;184(8):1990–2019. doi:10.1016/j.cell.2021.03.005
21. Tran D, Rajwani K, Berlin DA. Pulmonary effects of aging. Curr Opin Anaesthesiol. 2018;31(1):19–23. doi:10.1097/ACO.0000000000000546
22. Vazquez G, Benito S, Rivera R; Spanish Project for the Epidemiological Analysis of Critical Care P. Simplified Acute Physiology Score III: a project for a new multidimensional tool for evaluating intensive care unit performance. Crit Care. 2003;7(5):345–346. doi:10.1186/cc2163
23. Le Gall JR, Lemeshow S, Saulnier F. A new Simplified Acute Physiology Score (SAPS II) based on a European/North American multicenter study. JAMA. 1993;270(24):2957–2963. doi:10.1001/jama.1993.03510240069035
24. Zheng X, Hu T, Liu T, Wang W. Simplified acute physiology score III is excellent for predicting in-hospital mortality in coronary care unit patients with acute myocardial infarction: a retrospective study. Front Cardiovasc Med. 2022;9:989561. doi:10.3389/fcvm.2022.989561
25. Sakr Y, Krauss C, Amaral AC, et al. Comparison of the performance of SAPS II, SAPS 3, APACHE II, and their customized prognostic models in a surgical intensive care unit. Br J Anaesth. 2008;101(6):798–803. doi:10.1093/bja/aen291
26. Haq A, Patil S, Parcells AL, Chamberlain RS. The simplified acute physiology score III is superior to the simplified acute physiology score II and acute physiology and chronic health evaluation II in predicting surgical and ICU mortality in the “Oldest Old”. Curr Gerontol Geriatr Res. 2014;2014:934852. doi:10.1155/2014/934852
27. Gao H, Wang J, Zou X, Zhang K, Zhou J, Chen M. High blood urea nitrogen to creatinine ratio is associated with increased risk of sarcopenia in patients with chronic obstructive pulmonary disease. Exp Gerontol. 2022;169:111960. doi:10.1016/j.exger.2022.111960
28. Goto N, Wada Y, Ikuyama Y, et al. The usefulness of a combination of age, body mass index, and blood urea nitrogen as prognostic factors in predicting oxygen requirements in patients with coronavirus disease 2019. J Infect Chemother. 2021;27(12):1706–1712. doi:10.1016/j.jiac.2021.08.009
29. Marini CP, Russo GC, Nathan IM, Jurkiewicz A, McNelis J. Effect of hematocrit on regional oxygen delivery and extraction in an adult respiratory distress syndrome animal model. Am J Surg. 2000;180(2):108–114. doi:10.1016/S0002-9610(00)00424-4
30. Li Q, Mao Z, Hu P, Kang H, Zhou F. Analysis of the short-term prognosis and risk factors of elderly acute kidney injury patients in different KDIGO diagnostic windows. Aging Clin Exp Res. 2020;32(5):851–860. doi:10.1007/s40520-019-01261-z
31. Massari F, Scicchitano P, Iacoviello M, et al. Multiparametric approach to congestion for predicting long-term survival in heart failure. J Cardiol. 2020;75(1):47–52. doi:10.1016/j.jjcc.2019.05.017
32. Marchioli R, Finazzi G, Specchia G, et al. Cardiovascular events and intensity of treatment in polycythemia vera. N Engl J Med. 2013;368(1):22–33. doi:10.1056/NEJMoa1208500
33. Inzucchi SE, Zinman B, Fitchett D, et al. How does empagliflozin reduce cardiovascular mortality? Insights from a mediation analysis of the EMPA-REG OUTCOME trial. Diabetes Care. 2018;41(2):356–363. doi:10.2337/dc17-1096
34. Wang Y, Sun X, Lu J, Zhong L, Yang Z. Construction and evaluation of a mortality prediction model for patients with acute kidney injury undergoing continuous renal replacement therapy based on machine learning algorithms. Ann Med. 2024;56(1):2388709. doi:10.1080/07853890.2024.2388709
35. Goode V, Punjabi V, Niewiara J, et al. Using a retrospective secondary data analysis to identify risk factors for pulmonary complications in trauma patients in Pietermaritzburg, South Africa. J Surg Res. 2021;262:47–56. doi:10.1016/j.jss.2020.12.034
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.