Back to Journals » OncoTargets and Therapy » Volume 9
A new prognostic score based on the systemic inflammatory response in patients with inoperable non-small-cell lung cancer
Authors Zhu L, Li X, Shen Y, Cao Y, Fang X, Chen J, Yuan Y
Received 26 February 2016
Accepted for publication 9 June 2016
Published 8 August 2016 Volume 2016:9 Pages 4879—4886
DOI https://doi.org/10.2147/OTT.S107279
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Min Li
Lizhen Zhu,1 Xiaofen Li,1 Yanwei Shen,1 Ying Cao,1 Xuefeng Fang,1 Jiaqi Chen,1 Ying Yuan1,2
1Department of Medical Oncology, The Second Affiliated Hospital of Zhejiang University School of Medicine, Hangzhou, Zhejiang Province, People’s Republic of China; 2Cancer Institute, Key Laboratory of Cancer Prevention and Intervention, Chinese National Ministry of Education, Hangzhou, Zhejiang Province, People’s Republic of China
Purpose: Pretreatment systemic inflammatory response has been confirmed to have prognostic value in patients with inoperable non-small-cell lung cancer (NSCLC). Increasing studies show that the modified Glasgow prognostic score (mGPS), a prognostic score based on C-reactive protein (CRP) and albumin, is a prognostic factor in these patients. This study was aimed at recognizing possible prognostic factors and new prognostic scores of inoperable NSCLC based on pretreatment systemic inflammatory response.
Patients and methods: We retrospectively reviewed the clinicopathological data of 105 patients with inoperable NSCLC who received first-line chemotherapy as initial treatment. Univariate and multivariate analyses of progression-free survival (PFS) and overall survival (OS) for prognostic factors and scores were performed.
Results: The serum CRP, lactate dehydrogenase (LDH), cancer antigen 125 (CA125), and pathological type were independent pretreatment prognostic factors for PFS and OS. A new score was assembled by CRP, LDH, and CA125. In multivariate analysis, when the mGPS and the new score were covariates, only the new score retained independent prognostic value for both PFS (P<0.001; hazard ratio =2.12; 95% confidence interval: 1.60–2.82) and OS (P<0.001; hazard ratio =1.82; 95% confidence interval: 1.33–2.48).
Conclusion: The new score based on pretreatment serum level of CRP, LDH, and CA125, indicates the prognosis of both PFS and OS in patients with inoperable NSCLC who were treated with first-line systemic chemotherapy, and it was found to be more effective than mGPS.
Keywords: C-reactive protein, lactate dehydrogenase, CA125 antigen, prognostic score
Introduction
The relationship between inflammation and cancer is complicated. While on the one hand, emerging inflammation-related carcinogenic agents have been detected and more are waiting to be discovered, on the other hand, a highly proliferative tumor can produce inflammation, as evidenced by increased cytokine and chemokine production, and immune cells gathering in local tumor microenvironment. Many studies have shown that cancer-related inflammation plays an important role in neoplasia, tumor growth, cancer metastases, and cancer response to therapy.1–3 It is believed that the systemic inflammatory response is a reflection of local inflammation in the circulation and works similarly to the tumor microenvironment. Moreover, it helps tumor cells survival in systemic circulation by resisting anoikis (programmed cell death induced upon cell detachment from extracellular matrix, a critical mechanism preventing adherent-independent cell growth and attachment to an inappropriate matrix, thus avoiding colonization of distant organs), thereby facilitating metastasis of tumor cells.4
An increasing number of studies have identified that systemic inflammatory response, which includes elevated level of serum cytokines, inflammatory proteins such as C-reactive protein (CRP), neutrophil to lymphocyte ratio (NLR), platelet to lymphocyte ratio (PLR), and monocyte to lymphocyte ratio (MLR), is associated with early diagnosis and poor survivals in patients with inoperable non-small-cell lung cancer (NSCLC).5,6 Many studies have suggested that a modified Glasgow prognostic score (mGPS), based on the serum CRP and albumin level, predicts worse survival in numerous cancers, such as NSCLC, colorectal cancer, breast cancer, and gastric cancer. The mGPS is calculated as follows: patients with serum CRP ≤10 mg/L with or without hypoalbuminemia are scored as 0; patients with serum CRP >10 mg/L without hypoalbuminemia are scored as 1; and patients with serum CRP >10 mg/L and serum albumin ≤35 g/L are scored as 2.7,8 Recently, the mGPS has been applied as an inclusion criterion in several clinical trials.
The present study was aimed at evaluating possible prognostic factors and new prognostic scores based on pretreatment systemic inflammatory response for progression-free survival (PFS) and overall survival (OS) in patients with inoperable NSCLC who were treated with the first-line systemic chemotherapy as initial treatment.
Methods
The study was approved by the Ethics Committee of our hospital (The Second Affiliated Hospital of Zhejiang University School of Medicine), and all patients or their relatives gave their written informed consent for follow-up; patients’ identifying information has not been shown in this article.
We retrospectively reviewed the full records about clinical and pathologic information of 136 patients with histologically proven NSCLC and diagnosed as inoperable stage IIIb or IV disease, who received first-line systemic chemotherapies as initial treatment at the Department of Medical Oncology, Second Affiliated Hospital of Zhejiang University School of Medicine, from January 2011 to December 2013. Except for those patients diagnosed with cancer accompanied by obstructive pneumonia, patients who had clinical evidence of infections or other inflammatory conditions, or a second malignancy were excluded from this study. Finally, 105 patients were included in this study.
All 105 patients’ performance status (Eastern Cooperative Oncology Group score) was 0–1 before treatment. They received first-line systemic chemotherapies, most of which included cisplatin or carboplatin with other chemotherapy drugs, such as gemcitabine, pemetrexed, paclitaxel, and docetaxel, as initial treatment until disease progression or death before progression, and when the cancer progressed, the patients were started on the next-line regimen.
The following factors were reviewed in all the 105 patients: age, sex, pathological type, Eastern Cooperative Oncology Group score, weight loss within 3 months before treatment, blood parameters related to systemic inflammation, such as serum CRP concentration, white blood cell (WBC), neutrophil count, monocytes, NLR, PLR, and MLR. Besides, serum lactate dehydrogenase (LDH) level, albumin level, and tumor markers, including carcino-embryonic antigen, cancer antigen 125 (CA125), and squamous cell carcinoma, were studied as well. NLR, PLR, and MLR were calculated as neutrophil count, platelet count, and monocyte count divided by lymphocyte count, respectively. The blood parameters were all tested from day 0 to 1 week before the initial chemotherapy.
PFS was defined from the time initial chemotherapy started to the first progression (according to RECIST 1.19 guidelines) or death from any cause without progression. OS was defined from the date of initial chemotherapy to death from any cause, or the end of following-up. Continuous variables were expressed as the means ± standard deviation (SD), and univariate survival analysis was performed by the Kaplan–Meier method and compared with the log-rank test to evaluate potential prognostic factors and scores. The significant prognostic variables in univariate analysis were reassessed by multivariate survival analysis by Cox proportional hazard model and calculation of hazard ratios (HRs) and 95% confidence interval (CI). P≤0.05 was considered statistically significant in all analyses. Analyses was performed by SPSS software, version 21 (IBM Corporation, Armonk, NY, USA).
Results
All 105 patients were followed up to November 30, 2014; at the end of the follow-up period, 73 patients were dead, 24 survived, and eight were missing. The median follow-up time was 28.5 months, and varied from 11 to 47 months. Baseline characteristics are presented in Table 1. Most patients were male, had stage IV disease, PFS (median ± SD) was 5.72±4.60 months, and OS (median ± SD) was 13.14±9.67 months.
 | Table 1 Clinical characteristics and therapy responses of all 105 inoperable non-small-cell lung cancer patients |
We chose different cutoff points of CRP measurements to perform univariate analyses; the P-value was minimum at the cutoff point of 20 mg/L and therefore this cutoff point was applied in subsequent statistical analyses. The cutoff points for other continuous variables were chosen similarly. Among these, the cutoff values of LDH, CA125, and albumin were 240 U/L, 70 U/mL, and 35 g/L, respectively.
In terms of PFS, in univariate analysis, pathological type, weight loss, CRP, NLR, MLR, WBC, neutrophil, monocyte, albumin, LDH, and CA125 were all statistically related to prognosis (Table S1). In multivariate analysis by Cox proportional hazard model, only squamous and other pathological types (P<0.001; HR =1.77; 95% CI: 1.29–2.43), high CRP level (P<0.001; HR =2.95; 95% CI: 1.71–5.10), high LDH level (P=0.019; HR =1.71; 95% CI: 1.09–2.69), and high CA125 level (P<0.001; HR =3.16; 95% CI: 1.90–5.26) remained to be associated with poorer PFS (Table 2).
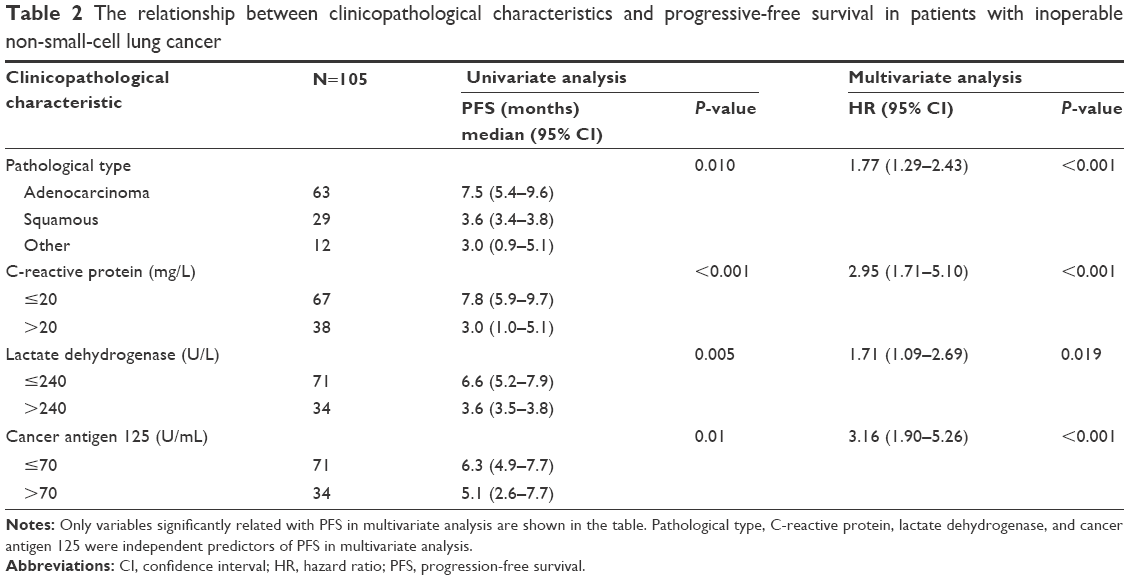 | Table 2 The relationship between clinicopathological characteristics and progressive-free survival in patients with inoperable non-small-cell lung cancer |
As for OS, pathological type, weight loss, CRP, NLR, PLR, MLR, WBC, neutrophil, monocyte, albumin, LDH, and CA125 were all statistically significant in univariate analysis (Table S2). However, in multivariate analysis, the results were similar to that of PFS; squamous and other pathological types (P<0.001; HR =2.10; 95% CI: 1.41–3.12), high CRP level (P=0.008; HR =2.46; 95% CI: 1.27–4.75), high LDH level (P=0.006; HR =2.15; 95% CI: 1.24–3.73), and high CA125 level (P=0.011; HR =2.02; 95% CI: 1.17–3.48) were still related to shorter OS (Table 3).
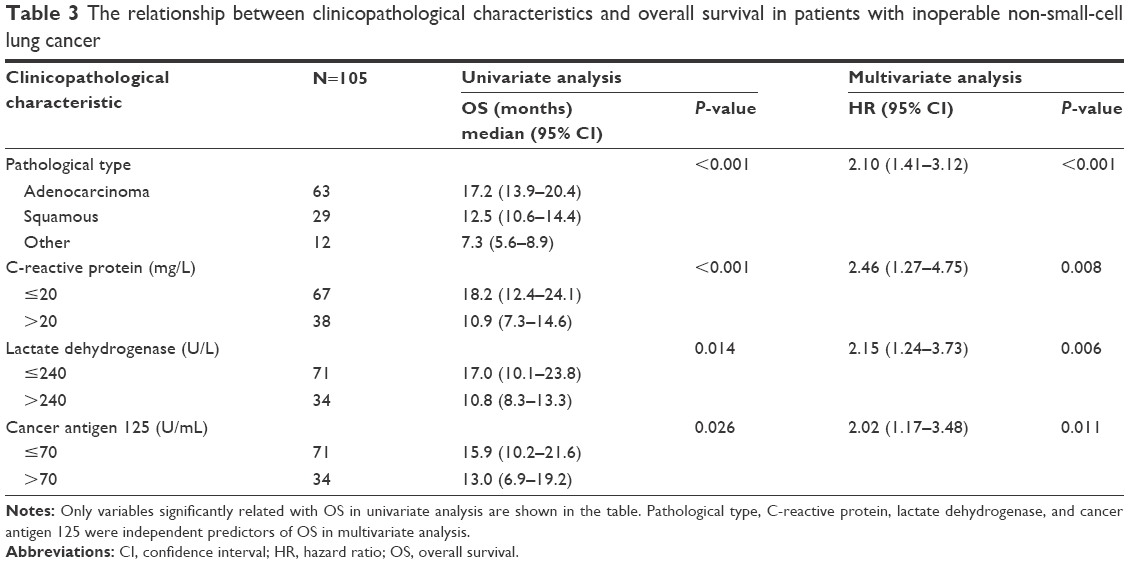 | Table 3 The relationship between clinicopathological characteristics and overall survival in patients with inoperable non-small-cell lung cancer |
Therefore, based on the multivariate survival analysis of PFS and OS, we selected CRP, LDH, and CA125 to establish a new score. Each of the following criteria was calculated as 1 point: CRP >20 mg/L, LDH >240 U/L, and CA125 >70 U/mL. The new score and mGPS are shown in Table 4. Patients who scored higher in the new score had much shorter PFS and OS than those with a lower score (Table 5). Similarly, higher scores in mGPS were associated with poorer prognosis in the univariate analysis (Table 5). But in multivariate analysis, when mGPS and the new score were covariates, only the new score retained independent prognostic value for both PFS (P<0.001; HR =2.12; 95% CI: 1.60–2.81) and OS (P<0.001; HR =1.82; 95% CI: 1.33–2.48) (Table 5).
 | Table 4 Assessment of the new score and modified Glasgow prognostic score |
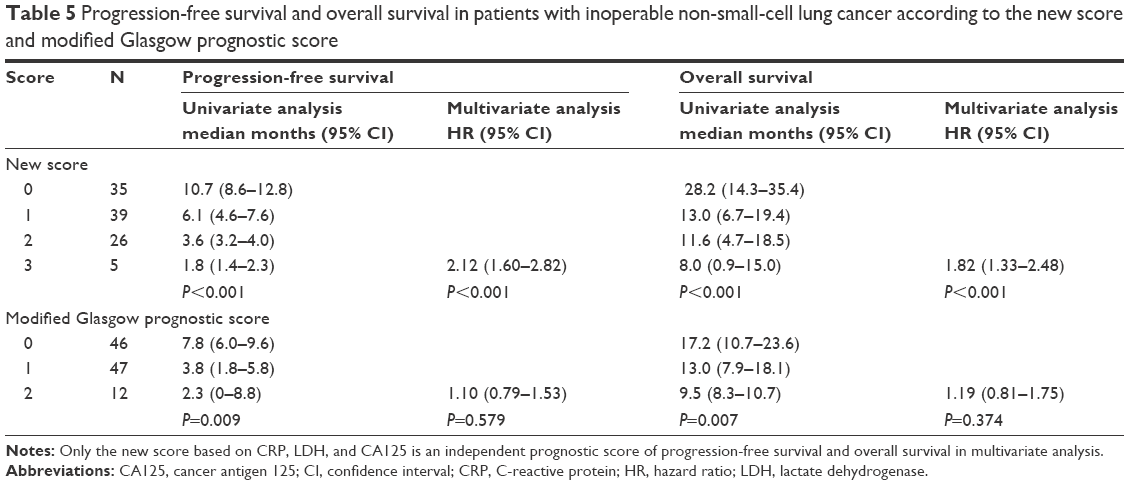 | Table 5 Progression-free survival and overall survival in patients with inoperable non-small-cell lung cancer according to the new score and modified Glasgow prognostic score |
Discussion
Many studies, including the present work, have demonstrated that elevated levels of CRP are associated with both increased risk and poor prognosis of cancers. Interestingly, in this study, among the blood parameters indicating systemic inflammation, only CRP, rather than other factors such as WBC, neutrophil count, monocyte count, or NLR, has retained a significantly independent prognostic role for both PFS and OS in multivariate analysis. This may suggest that CRP is the main prognostic factor of inoperable NSCLC in the systemic inflammatory response. However, reasons for CRP elevation in cancer patients are not clearly understood and several hypotheses have been proposed about the relationship between CRP and cancer.
One possible mechanism might be that tumor growth could cause inflammation around the tumor, thereby increasing the serum CRP level. Since CRP is synthesized in the response to cytokines such as interleukin-6, interleukin-1β, or tumor necrosis factor-α, and these cytokines activate the transcription factors in signal-transducer and activator of transcription 3 and nuclear factor kappa light chain enhancer of activated B cells pathways, inactivating mutation of tumor-suppressor genes or triggering posttranslational modifications in DNA repair- or apoptosis control-related proteins eventually upregulates anti-apoptotic or pro-proliferative factors to prevent apoptosis.10 In addition, CRP and inflammatory response can promote each other. CRP is composed of five identical subunits arranged in a pentameric structure (pCRP); when pCRP is attached to damaged cells with Ca-mediated, it forms monomeric subunits of CRP. Delayed apoptosis of neutrophils is reported to be caused by a decrease in pCRP concentration, whereas monomeric subunits of CRP promotes neutrophil survival, therefore, amplifying the inflammatory response. Studies have suggested that lymphocytes and monocytes are able to synthesize CRP as well.11,12
Another possible source of CRP is pulmonary disorders, such as pulmonary infection, bronchitis, chronic obstructive pulmonary disease, asthma, and other lung diseases, as the pulmonary diseases can stimulate respiratory tract epithelium to produce local CRP in lung tissues;13 these pulmonary diseases are reported to be presumable carcinogens. Therefore, CRP may reflect the connection between pulmonary inflammation and lung cancer, but its specific role in the development of lung malignancies remains unknown. Patients with obstructive pneumonia caused by NSCLC were not excluded in this study, so the high level of serum CRP may be caused by both obstructive pneumonia and cancer itself. Besides, although the details of how CRP interacts with chemotherapy remain obscure, the inflammatory response can compromise pharmacodynamics of anticancer drugs.14
Besides its prognostic value, the level of serum CRP also plays a predictive role in cancer. In a Phase II study of ruxolitinib or placebo with capecitabine as second-line therapy in patients with metastatic pancreatic cancer, the OS significantly favored ruxolitinib over placebo in patients with CRP >13 mg/L, although the relationship between ruxolitinib and CRP was uncertain, while in patients with CRP ≤13 mg/L, no such benefit was observed.15 In metastatic renal cell carcinoma, the serum CRP level predicts the effect of targeted molecular therapy as well.16 In addition, a CRP inhibitor has been demonstrated to abrogate the increase in infarct size and cardiac dysfunction caused by CRP injections.17 Although the use of CRP targeting drugs in cancers has not yet been reported, targeting CRP may offer a therapeutic opportunity since it plays a key role in tumor cell proliferation.
Studies have demonstrated that high serum LDH level predicts poor prognosis in inoperable NSCLC patients.18,19 Moreover, high LDH-5 expression (both nuclear and cytoplasmic) is linked to poor prognosis in patients with operable NSCLC, although it is not related to elevated serum LDH.20
The reasons that LDH indicates poor survival may be as follows: 1) according to the Warburg effect, tumor cells rely on anaerobic respiration even under oxygen-sufficient condition.21 The tetrameric enzyme LDH contains two major subunits H and/or M, thus resulting in five isozymes (4H, 3H1M, 2H2M, 1H3M, and 4M) that can catalyze the interconversion of pyruvate and lactate. The H-subunit weakens the enzyme’s ability to catalyze the reaction. LDH-5 is composed of four M-subunits and without H-subunit, therefore it has the highest efficiency among all other isozymes to convert pyruvate to lactate, providing the substrate for anaerobic respiration.22 2) Hypoxia-inducible factor binds to the promoter regions of several hypoxia-response genes, including LDH-5, under hypoxic conditions, stimulating the expression of vascular endothelial growth factor, therefore promoting tumor angiogenesis. In addition, it provides a potential cancer therapy targeting LDH.23
CA125, also known as MUC16 and encoded by MUC16 gene, is a member of glycoproteins of the mucin family.24 CA125 is a biomarker that may be elevated in cancers, such as endometrial cancer, fallopian tube cancer, lung cancer, and especially in ovarian cancer. Other diseases or conditions can lead to an elevation in CA125 as well, such as pregnancy. Studies show that in patients with cancers, including advanced NSCLC, high serum CA125 level is related to shorter survival, which is also evidenced by our study.25,26
CA125, overexpressed in tumor cells, binds to mesothelin, a glycoprotein expressed by tumor cells and mesothelial cells of the peritoneum, and the combination of CA125 and mesothelin promotes tumor cell metastasis to peritoneum and metastatic sites.27 On the other hand, natural killer cells cannot recognize ovarian cancer cells expressing CA125, leading to selective survival of ovarian cancer cells,28 and these phenomena may also occur in NSCLC cells. Furthermore, CA125 is a counter receptor for galectin-1,29 a member of β-galactoside-binding proteins associated with immunosuppression and other biological activities that can promote tumor cell proliferation.30
The results of clinical trials testing oregovomab and abagovomab, two antibodies developed for ovarian cancer immunotherapy, were disappointing, as no benefit was observed in ovarian cancer patients. Other anti-CA125 antibody – 3A5 and 11D10 – were developed and conjugated to the cytotoxic drug monomethyl auristatin E and are being tested clinically; so far, the results from a Phase I clinical trial have been encouraging.27
Albumin plays an important role in transporting compounds, maintaining osmotic pressure and other functions. Low albumin level is associated with malnutrition and systemic inflammation,31 and can increase chemotherapy toxicity, including anemia, fatigue, and appetite loss as well.32 Due to these, hypoalbuminemia is demonstrated to have negative prognostic value in different types of cancer, including NSCLC.7 However, this is not evident in the multivariate analysis of this study.
There is another factor that needs to be considered. All the 105 patients included in this study received first-line systemic chemotherapies as initial treatment. Many of them refused to test for epidermal growth factor receptor mutation and use tyrosine kinase inhibitor even if they were epidermal growth factor receptor-mutation positive owing to, financial reasons, because during that time, first-line tyrosine kinase inhibitor were not covered by the Chinese medical insurance. By the last follow-up date, November 30, 2014, of this study, only 12 patients had used tyrosine kinase inhibitor after being tested as EFGR mutation positive in the subsequent treatment after the cancer progressed. This group of patients did not have improved OS than other patients in the univariate analysis (P=0.16), which might be because of the limited number of patients. Besides, among the 105 patients, 60 patients had one organ with metastasis, 15 patients had two organs with metastases, seven patients had three organs with metastases, two patients had four organs with metastases, and one patient had five organs with metastases. There were 31 patients who had only one organ metastasis with only one single metastatic lesion. In the univariate analysis, the number of organs with metastases had no prognostic value for PFS (P=0.10) and OS (P=0.08), neither did only one organ metastasis with only one single metastatic lesion (P=0.13) and OS (P=0.12); this may be due to the limited patient data in the study.
Several scoring systems based on CRP are being proposed to play the role of prognostic markers of cancers. Among these, mGPS, which is calculated from the serum CRP and albumin level, is a well-received independent prognostic system and has been applied to clinical trials.15 However, the new score calculated based on CRP, LDH, and CA125 levels, as described in the present study, appears to be superior to mGPS in predicting the survival of inoperable NSCLC patients (Table 5). This result may be explained as follows: while mGPS only focuses on system inflammation and hypoalbuminemia in patients, the new score not only suggests system inflammation of the patients but can also indicate anaerobic respiration based on LDH level, and proliferation and metastatic ability of tumor cell based on CA125 level.
Conclusion
In conclusion, CRP, LDH, and CA125 aggravate tumor cell proliferation and metastasis through different mechanisms. As supported by our study, the score calculated based on CRP, LDH, and CA125 levels proved to be a better prognostic indicator for both PFS and OS in patients with inoperable NSCLC. However, our study is a retrospective analysis with limited patient data. Even though this study suggests that the new prognostic system described here is better for prognosis, a definite conclusion requires further studies.
Disclosure
Authors received no specific funding for this work and have no conflicts of interest in this work.
References
Diakos CI, Charles KA, McMillan DC, Clarke SJ. Cancer-related inflammation and treatment effectiveness. Lancet Oncol. 2014;15(11):e493–e503. | ||
Tauchi Y, Tanaka H, Kumamoto K, et al. Tumor-associated macrophages induce capillary morphogenesis of lymphatic endothelial cells derived from human gastric cancer. Cancer Sci. Epub 2016 May 26. | ||
Erez N, Glanz S, Raz Y, Avivi C, Barshack I. Cancer associated fibroblasts express pro-inflammatory factors in human breast and ovarian tumors. Biochem Biophys Res Commun. 2013;437(3):397–402. | ||
Kim YN, Koo KH, Sung JY, Yun UJ, Kim H. Anoikis resistance: an essential prerequisite for tumor metastasis. Int J Cell Biol. 2012;2012:306879. | ||
Teramukai S1, Kitano T, Kishida Y, et al. Pretreatment neutrophil count as an independent prognostic factor in advanced non-small-cell lung cancer: an analysis of Japan Multinational Trial Organisation LC00-03. Eur J Cancer. 2009;45(11):1950–1958. | ||
Liu H, Wu Y, Wang Z, et al. Pretreatment platelet-to-lymphocyte ratio (PLR) as a predictor of response to first-line platinum-based chemotherapy and prognosis for patients with non-small cell lung cancer. J Thorac Dis. 2013;5(6):783–789. | ||
McMillan DC. The systemic inflammation-based Glasgow Prognostic Score: a decade of experience in patients with cancer. Cancer Treat Rev. 2013;39(5):534–540. | ||
Fan H, Shao ZY, Xiao YY, et al. Comparison of the Glasgow Prognostic Score (GPS) and the modified Glasgow Prognostic Score (mGPS) in evaluating the prognosis of patients with operable and inoperable non-small cell lung cancer. J Cancer Res Clin Oncol. 2016;142(6):1285–1297. | ||
Eisenhauer EA, Therasse P, Bogaerts J, et al. New response evaluation criteria in solid tumours: revised RECIST guideline (version 1.1). Eur J Cancer. 2009;45(2):228–247. | ||
Agrawal A, Cha-Molstad H, Samols D, Kushner I. Overexpressed nuclear factor-κB can participate in endogenous C-reactive protein induction, and enhances the effects of C/EBPβ and signal transducer and activator of transcription-3. Immunology. 2003;108(4):539–547. | ||
Khreiss T, József L, Hossain S, Chan JS, Potempa LA, Filep JG. Loss of pentameric symmetry of C-reactive protein is associated with delayed apoptosis of human neutrophils. J Biol Chem. 2002;277(43):40775–40781. | ||
Murphy TM, Baum LL, Beaman KD. Extrahepatic transcription of human C-reactive protein. J Exp Med. 1991;173(2):495–498. | ||
Agassandian M, Shurin GV, Ma Y, Shurin MR. C-reactive protein and lung diseases. Int J Biochem Cell Biol. 2014;53:77–88. | ||
Slaviero KA, Clarke SJ, Rivory LP. Inflammatory response: an unrecognised source of variability in the pharmacokinetics and pharmacodynamics of cancer chemotherapy. Lancet Oncol. 2003;4(4):224–232. | ||
Hurwitz HI, Uppal N, Wagner SA, et al. Randomized, double-blind, phase II study of ruxolitinib or placebo in combination with capecitabine in patients with metastatic pancreatic cancer for whom therapy with gemcitabine has failed. J Clin Oncol. 2015;33(34):4039–4047. | ||
Teishima J, Kobatake K, Kitano H, et al. The impact of change in serum C-reactive protein level on the prediction of effects of molecular targeted therapy in patients with metastatic renal cell carcinoma. BJU Int. 2015;117(6B):E67–E74. | ||
Pepys MB, Hirschfield GM, Tennent GA, et al. Targeting C-reactive protein for the treatment of cardiovascular disease. Nature. 2006;440(7088):1217–1221. | ||
Ulas A, Turkoz FP, Silay K, et al. A laboratory prognostic index model for patients with advanced non-small cell lung cancer. PLoS One. 2014;9(12):e114471. | ||
Ramalingam S, Goss G, Rosell R, et al. A randomized phase II study of ganetespib, a heat shock protein 90 inhibitor, in combination with docetaxel in second-line therapy of advanced non-small cell lung cancer (GALAXY-1). Ann Oncol. 2015;26(8):1741–1748. | ||
Koukourakis M, Giatromanolaki A, Sivridis E, et al. Lactate dehydrogenase-5 (LDH-5) overexpression in non-small-cell lung cancer tissues is linked to tumour hypoxia, angiogenic factor production and poor prognosis. Br J Cancer. 2003;89(5):877–885. | ||
Vander Heiden MG, Cantley LC, Thompson CB. Understanding the Warburg effect: the metabolic requirements of cell proliferation. Science. 2009;324(5930):1029–1033. | ||
Gallo M, Sapio L, Spina A, Naviglio D, Calogero A, Naviglio S. Lactic dehydrogenase and cancer: an overview. Front Biosci. 2015;20:1234–1249. | ||
Signoretti S, Billiard J, Duffy KJ, et al. Targeting lactate dehydrogenase-a inhibits tumorigenesis and tumor progression in mouse models of lung cancer and impacts tumor-initiating cells. Cell Metab. 2014;19(5):795–809. | ||
Yin BW, Dnistrian A, Lloyd KO. Ovarian cancer antigen CA125 is encoded by the MUC16 mucin gene. Int J Cancer. 2002;98(5):737–740. | ||
Cedres S, Nunez I, Longo M, et al. Serum tumor markers CEA, CYFRA21-1, and CA-125 are associated with worse prognosis in advanced non-small-cell lung cancer (NSCLC). Clin Lung Cancer. 2011;12(3):172–179. | ||
Kim HS, Choi HY, Lee M, et al. Systemic inflammatory response markers and CA-125 levels in ovarian clear cell carcinoma: A Two Center Cohort Study. Cancer Res Treat. 2015;48(1):250–258. | ||
Felder M, Kapur A, Gonzalez-Bosquet J, et al. MUC16 (CA125): tumor biomarker to cancer therapy, a work in progress. Mol Cancer. 2014;13:129. | ||
Gubbels J, Felder M, Horibata S, et al. MUC16 provides immune protection by inhibiting synapse formation between NK and ovarian tumor cells. Mol Cancer. 2010;9:1476–4598. | ||
Seelenmeyer C, Wegehingel S, Lechner J, Nickel W. The cancer antigen CA125 represents a novel counter receptor for galectin-1. J Cell Sci. 2003;116(Pt 7):1305–1318. | ||
Camby I, Le Mercier M, Lefranc F, Kiss R. Galectin-1: a small protein with major functions. Glycobiology. 2006;16(11):137R–157R. | ||
McMillan DC. An inflammation-based prognostic score and its role in the nutrition-based management of patients with cancer. Proc Nutr Soc. 2008;67(3):257–262. | ||
Arrieta O, Michel Ortega RM, Villanueva-Rodríguez G, et al. Association of nutritional status and serum albumin levels with development of toxicity in patients with advanced nonsmall cell lung cancer treated with paclitaxel–cisplatin chemotherapy: a prospective study. BMC Cancer. 2010;10:50. |
Supplementary materials
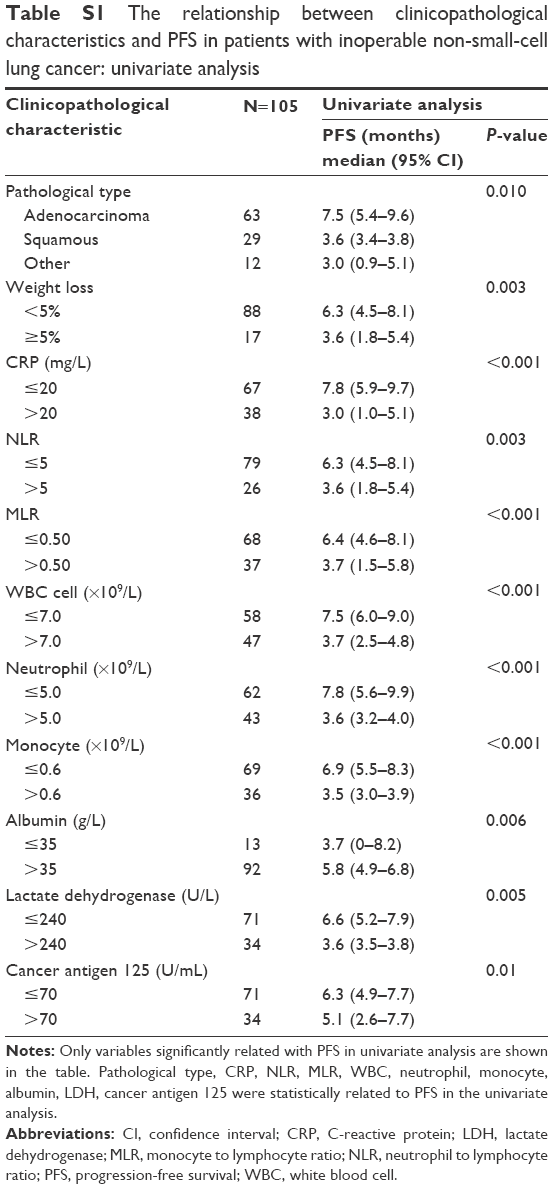 | Table S1 The relationship between clinicopathological characteristics and PFS in patients with inoperable non-small-cell lung cancer: univariate analysis |
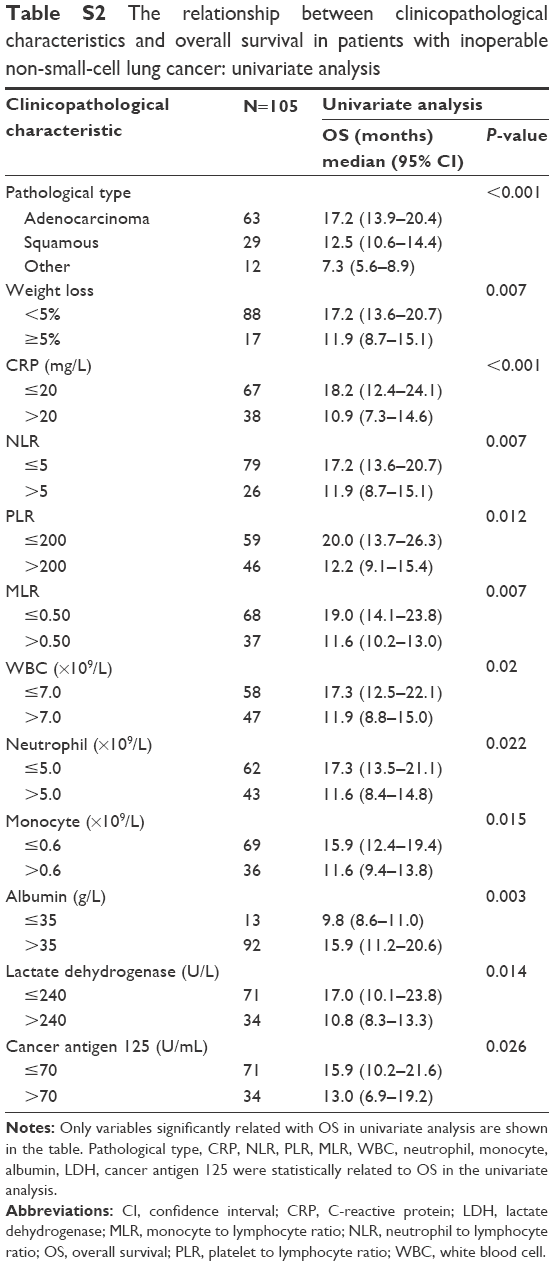 | Table S2 The relationship between clinicopathological characteristics and overall survival in patients with inoperable non-small-cell lung cancer: univariate analysis |
 © 2016 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2016 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.