Back to Journals » Medical Devices: Evidence and Research » Volume 19
A Multidimensional Index Framework for Evaluating the Regulatory Applicability of ISO 10328 Using a Prosthetic Knee Case Study
Authors Li J
Received 7 August 2025
Accepted for publication 16 January 2026
Published 27 March 2026 Volume 2026:19 558998
DOI https://doi.org/10.2147/MDER.S558998
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Scott Fraser
Jia Li
The Institute of Theory and Strategy of Standardization, China National Institute of Standardization (CNIS), Beijing, 100191, People’s Republic of China
Correspondence: Jia Li, Email [email protected]
Abstract: International biomechanical standards, such as ISO 10328 for lower-limb prosthetic testing, are widely used to guide device evaluation, yet their direct adoption into national regulatory systems often results in mismatches in safety expectations, documentation formats, and contextual use conditions. Despite extensive reliance on ISO standards, there is no structured method to assess whether these standards are appropriately aligned with regulatory requirements across different jurisdictions. This narrative review, combined with a conceptual framework and an illustrative cross-jurisdictional case study, proposes a multi-dimensional applicability index designed to evaluate the regulatory fit of international biomechanical standards before national adoption. The index comprises five dimensions clinical safety alignment, technical fit, contextual usability, documentation conformance, and regulatory interoperability, each providing a structured lens for assessing standard suitability. Using ISO 10328 and a representative prosthetic knee device as an example, the study demonstrates how the index highlights areas of strong technical alignment but also reveals gaps related to usability, documentation, and post-market expectations across the U.S. FDA, EU MDR, and China’s GB/NMPA systems. The findings underscore the need for context-aware evaluation tools to complement global standards, reducing approval delays and improving device performance in real-world environments. This work provides a foundational methodology for regulators, manufacturers, and standards bodies seeking to harmonize global testing norms while ensuring national regulatory relevance and patient safety.
Keywords: biomechanics, prosthetic knee joints, international standards, regulatory frameworks, medical device regulation
Introduction
The rapid globalization of biomedical device manufacturing and trade has intensified the need for harmonized regulatory standards that ensure safety, quality, and interoperability across jurisdictions. International bodies such as the International Organization for Standardization (ISO) and the International Electrotechnical Commission (IEC) have developed over 200 standards directly applicable to medical devices, including ISO 10328, which outlines structural testing procedures for lower limb prosthetic components.1–4 However, despite the widespread use of such standards, no structured framework currently exists for systematically evaluating whether an international biomechanical standard is suitable for adoption within a specific national regulatory context. For biomechanical medical devices, standards are critical to patient safety because they define conditions for reliable performance under repeated inserting and long-term use. In load-bearing prosthetic systems, failure to account for fatigue, real-world gait, or contextual use can lead to instability, premature failure, or secondary injury. The challenge of uniform adoption of medical device standards, despite efforts by the International Medical Device Regulators Forum (IMDRF), stems from various regulatory inconsistencies and fragmentation across nations. While the IMDRF aims to harmonize regulations, only 65% of ISO standards are integrated into national laws, leading to a lack of coherence in the global medical device market.5–7 Regulatory systems for medical devices in the U.S. and China exhibit significant differences in their frameworks, philosophies, and implementation strategies. The U.S. FDA employs a risk-based, data-intensive premarket pathway, primarily through the 510(k) and PMA routes, focusing on safety and efficacy through rigorous clinical evaluations. In contrast, China’s National Medical Products Administration (NMPA) has evolved its regulatory guidance, particularly with the 2021 CE Guidance Series, which emphasizes a lifecycle approach to clinical evaluation but still faces challenges in post-market oversight.8,9 These regulatory divergences are not merely administrative but directly shape how biomechanical standards are interpreted, supplemented, or constrained during prosthetic device testing, documentation, and conformity assessment. Although these regulatory comparisons establish the broader landscape, it is essential to explicitly connect these divergences to their practical consequences for biomechanical standards, particularly in how they shape requirements for prosthetic testing, documentation, and conformity assessment. The regulatory frameworks for medical devices in China and the European Union (EU) exhibit distinct priorities and processes. The National Medical Products Administration (NMPA) in China emphasizes domestic testing, device labeling, and post-market controls, ensuring that devices meet local safety and efficacy standards. In contrast, the EU’s Medical Device Regulation (MDR 2017/745) focuses on continuous clinical evaluation, oversight by Notified Bodies, and compliance with CE marking directives, which are essential for market access in Europe. The following sections elaborate on these differences.2,10–12 These divergences are particularly problematic for biomechanical technologies such as prosthetic limbs, where performance depends not only on material specifications, but on localized human anatomy, gait variability, rehabilitation infrastructure, and end user behavior.13–15
The prosthetic knee joint exemplifies the complex challenge of applying global standards in diverse real-world conditions. It is a high load, multi axis biomechanical interface that must accommodate residual limb geometry, dynamic torque, angular displacement, and long-term joint fatigue.16–19 During typical daily activities, a prosthetic knee may endure cyclic loads of 3–5 times body weight, with peak forces exceeding 7 times body weight during stair ascent or running. While ISO 10328 provides standardized testing protocols for structural integrity, it lacks guidance on contextual adaptation for environmental, cultural, and anatomical differences.20–22 For instance, terrain variability, barefoot gait habits, socket limb mismatch, and prosthetic access disparities all impact device function and safety in ways that a universal structural test cannot capture. Despite the regulatory importance of such factors, existing standards are often adopted without formal evaluation of their clinical or regulatory suitability in local settings.21,23–25 A 2023 comparative analysis of 36 ISO to GB standard transformations in China found that more than 60% required reinterpretation or localization due to semantic, procedural, or clinical misalignments. In the U.S., prosthetic submissions routinely pass ISO based testing yet fail FDA premarket review due to usability gaps, incomplete labeling compliance, or poorly aligned risk classification. Similar discrepancies are found in Europe, where over 40% of ISO compliant Class IIb devices are required to undergo supplementary assessments under EU MDR conformity audits.26–29 Taken together, these examples underscore the need for a clearly defined problem statement: the global regulatory ecosystem currently lacks systematic tools to evaluate the “regulatory fit” of technical standards before national adoption. Despite these challenges, few tools currently exist to systematically assess the “regulatory fit” of international standards across diverse jurisdictions. In this review, prosthetic knee devices and ISO 10328 are intentionally used as a focused illustrative case to demonstrate this broader methodological challenge, rather than as an exhaustive representation of all biomechanical standards or device categories. The literature on prosthetic knee joint evaluation is heavily skewed toward mechanical performance, computational modeling, and engineering optimization. While these domains provide essential insights into joint loading, gait symmetry, or material fatigue, they offer little guidance on regulatory adaptation, especially across countries with differing healthcare systems, reimbursement models, and clinical protocols.15,30–33 Policy literature, conversely, often focuses on broader market access, intellectual property, or trade policy without addressing device level standard applicability. Consequently, a critical gap remains between technical standard development and regulatory decision making. Stakeholders, including manufacturers, regulators, clinicians, and policymakers lack a structured, evidence-based method to evaluate whether an international standard like ISO 10328 can be seamlessly integrated into a given national framework, or whether it requires translation, localization, or reinterpretation.34–37 The key gap is not the availability of standards, but the lack of tools to assess their contextual regulatory applicability, a gap this framework addresses at the standard level, complementing system-level tools such as the WHO Global Benchmarking Tool. The central methodological gap in global regulatory science becomes evident upon recognizing that no existing tools systematically assess the contextual applicability of technical standards across national regulatory systems. Additionally, the proposed framework complements global harmonization initiatives such as the WHO Global Benchmarking Tool (GBT), which evaluates regulatory system maturity but does not examine the suitability of individual technical standards within local contexts.
To address this gap, this review proposes a multi-dimensional index framework for evaluating the regulatory applicability of international standards, using the prosthetic knee joint as a case example. The framework is built on five key dimensions: clinical safety alignment, technical fitness, contextual usability, documentation conformance, and regulatory interoperability. Each dimension incorporates both qualitative and quantitative indicators derived from global standards, national regulatory codes, biomechanical literature, and expert informed criteria. By applying this framework to compare ISO, FDA, and GB regulatory systems, the review not only highlights points of convergence and friction but also provides a practical tool for anticipatory alignment of product development with local approval pathways. Furthermore, the index system is positioned as a scalable and adaptable model that can support the development of AI assisted scoring tools, digital twins for compliance simulation, and future global applicability databases. In doing so, this work aims to contribute both theoretically and practically to the emerging domain of digital regulatory science and global health technology governance.
Conceptual Background: International Standard Transformation and Regulatory Divergence
The concept of international standard transformation refers to the process by which globally recognized technical norms most developed by the International Organization for Standardization (ISO) or the International Electrotechnical Commission (IEC) are adapted for use within national regulatory frameworks.35,38–40 This transformation process is neither linear nor uniform and typically occurs in three stages: translation, which involves the linguistic and semantic rendering of standards into the national language and regulatory context; localization, which adjusts the content to fit domestic healthcare infrastructure, cultural norms, and industrial capability; and reinterpretation, which aligns regulatory pathways, compliance procedures, and enforcement mechanisms with national policy objectives.41,42 The temporal evolution of these transformation processes, along with key revisions of ISO 10328 and broader contextual shifts in prosthetic regulation, is illustrated in Figure 1. In practice, these stages determine how well an international technical standard can be operationalized within a national regulatory environment, particularly for devices whose performance is highly dependent on contextual factors, such as prosthetic technologies. The complexity of post-market surveillance (PMS) in biomedical engineering arises from the interplay of human variability, clinical practice heterogeneity, and the capacity for monitoring device performance after-market release. PMS is crucial for ensuring the safety and efficacy of medical devices in real-world settings, where controlled pre-market conditions do not apply. This process involves continuous monitoring and data collection to identify adverse events and ensure compliance with regulatory standards. The following sections delve into the key aspects of PMS in biomedical engineering.43–46
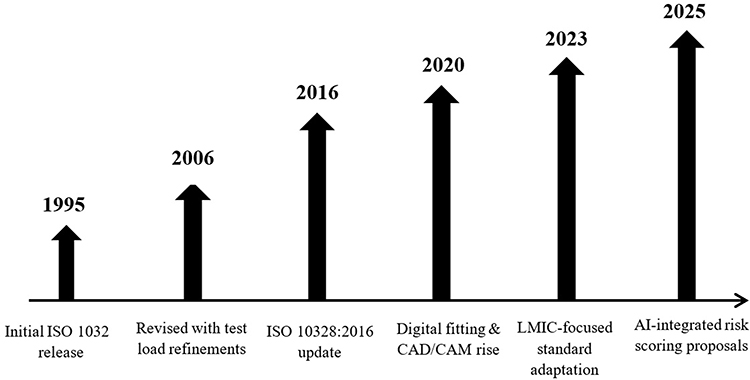 |
Figure 1 Evolution of ISO 10328 and Contextual Shifts in Prosthetic Regulation. This timeline outlines the historical development of ISO 10328, beginning with its initial release in 1995 and major revisions in 2006 and 2016. It also highlights recent global shifts, including the rise of digital fitting technologies (2020), the growing focus on accessibility in low- and middle-income countries (2023), and emerging proposals for AI-based regulatory tools and modular annexes (2025). These contextual developments justify the need for a dynamic and adaptive applicability index. |
The ISO 10328 standard is crucial for assessing the structural integrity of lower limb prostheses through static and cyclic loading tests. However, it has limitations regarding real-world variability in gait mechanics, residual limb anatomy, and environmental conditions. These limitations highlight the broader issue that biomechanical standards designed for universal application may not fully capture region-specific patterns of device use, which is a central regulatory challenge discussed in this review.47,48 In high income countries, prosthetic joints are typically fitted using gait analysis labs, pressure sensors, and dynamic alignment tools. In contrast, in many low- and middle-income countries (LMICs), fittings are often done manually, with limited post fitting follow up or patient education. A universal testing protocol may ensure mechanical safety but fall short on usability, adaptability, and clinical relevance. Consequently, regulatory agencies often impose additional requirements or reinterpret international standards to fit local conditions.49–52 Recent reviews emphasize that ISO 10328 does not simulate common prosthesis use conditions in LMICs, such as walking barefoot on uneven surfaces or limited access to follow-up rehabilitation services, reducing its contextual validity in these settings.50,53
Comparative analyses of regulatory systems reveal clear divergence in both philosophy and practice. The U.S. FDA, operating under 21 CFR Part 820 and the 510(k)/PMA pathways, requires a demonstration of substantial equivalence or clinical evidence of safety and effectiveness, even for ISO certified devices.27,54–56 Its risk-based classification system (Class I–III) governs documentation, clinical testing, and manufacturing oversight. The Chinese GB system, coordinated by the State Administration for Market Regulation (SAMR) and the National Medical Products Administration (NMPA), incorporates ISO technical content but emphasizes local conformity testing, risk specific standards (eg., YY/T 0316 2016 for risk management), and product specific technical review templates. Meanwhile, the European Union applies the MDR 2017/745 framework, which mandates CE conformity assessments, continuous clinical evaluation, and rigorous post market surveillance, often requiring additional performance data even for ISO compliant devices.57–59 Table 1 summarizes selected key differences.
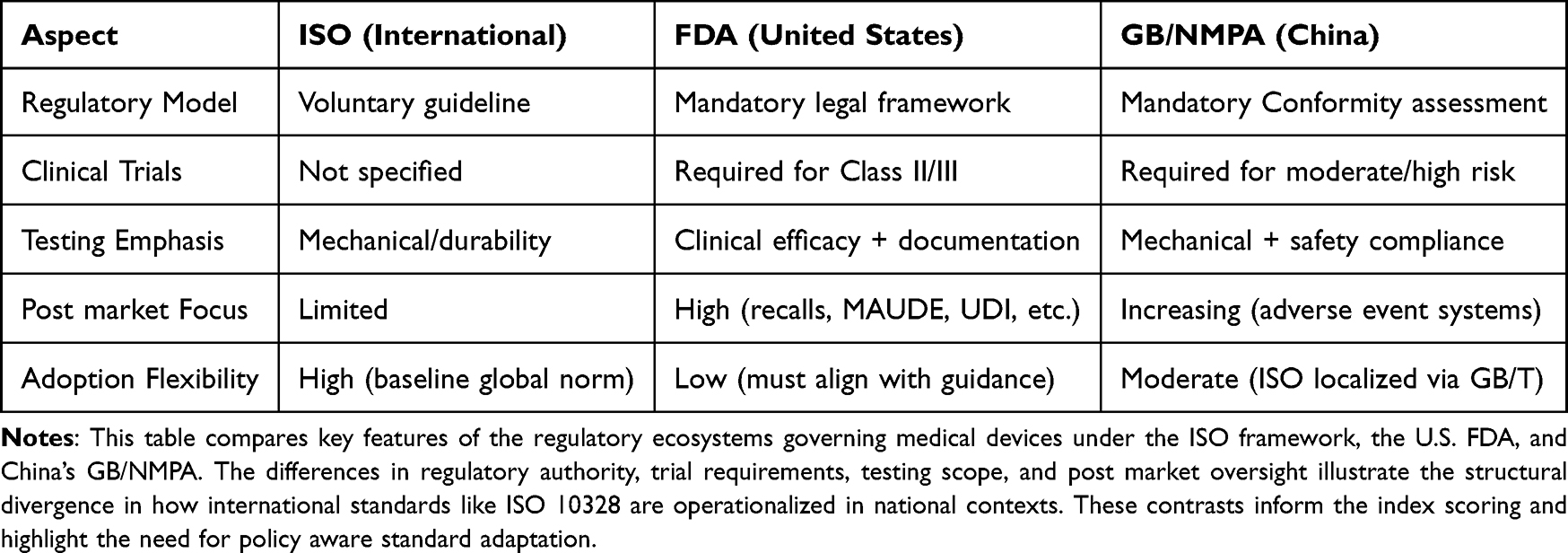 |
Table 1 Comparison of Regulatory Structures and Practices Across ISO, FDA, and GB/NMPA Systems |
While international standardization initiatives aim to streamline cross border regulatory recognition, substantial obstacles remain. According to a 2022 WHO global survey of 113 member states, fewer than 30% had a structured method to evaluate the relevance or readiness of an ISO based standard before adopting it into national regulation.2,35,60 Furthermore, case reports from the prosthetics sector illustrate that international standards, even when technically sound often fail to satisfy documentation norms, patient centric evaluation criteria, or post market reporting expectations of local regulatory authorities. These failures are typically addressed reactively, through manufacturer appeals or supplemental data submissions, rather than through a formal, preadoption evaluation mechanism.61–63 These patterns collectively demonstrate the absence of a structured method for determining whether an international biomechanical standard is suitable for direct adoption, requires modification, or should undergo full reinterpretation within a specific rregulatory setting.
This lack of structured tools for regulatory applicability assessment leads to a fragmented ecosystem in which manufacturers must individually interpret compliance risks, and regulators may inconsistently enforce or modify standards. The result is redundancy in testing, increased time to market, and a higher probability of device rejection or reclassification. In high-risk devices such as prosthetic knee joints, where technical adequacy must be balanced with anatomical and functional alignment, the absence of evaluative frameworks to guide standard transformation represents both a regulatory bottleneck and a patient safety concern.64–66 This review therefore situates prosthetic knee evaluation as a representative example of how contextual, anatomical, and regulatory differences can expose shortcomings in universally applied biomechanical standards.
Index Framework for Evaluating Standard Applicability
To bridge the gap between international standardization and national regulatory adaptation, this review proposes a structured, multi-dimensional index system designed to evaluate the contextual applicability of biomedical standards. The goal is to provide regulators, manufacturers, and clinical stakeholders with a transparent and systematic framework that goes beyond binary compliance checks. By applying this framework, it becomes possible to assess whether an international standard, such as ISO 10328 for prosthetic limb testing, can be adopted directly, requires localization, or demands full reinterpretation. The proposed framework is grounded in principles of regulatory science, clinical biomechanics, and policy analysis, and can be adapted across device classes and regulatory systems.1–3,67 The index comprises five primary dimensions, each representing a critical facet of standard applicability in real world regulatory settings: A concise summary of these five dimensions, including their definitions and representative evaluation indicators, is presented in Table 2
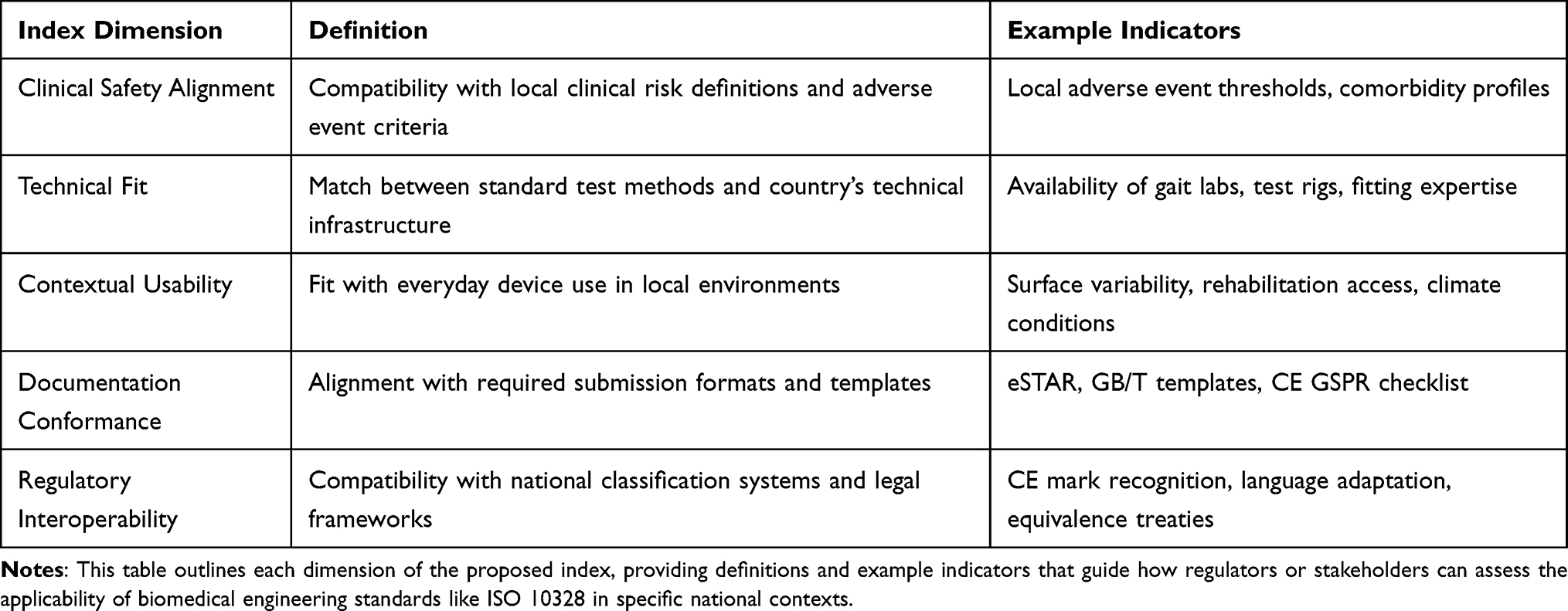 |
Table 2 Summary of the Five-Dimension Index Framework for Standard Applicability Evaluation |
Clinical Safety Alignment
Evaluates whether the standard adequately addresses patient safety concerns in the target regulatory context. This includes alignment with national definitions of clinical risk, severity classification systems, and compatibility with patient demographics, comorbidities, or local clinical practices. For example, while ISO 10328 includes fatigue and failure load testing, it may not account for adverse event thresholds or residual limb variability required by the FDA or NMPA.68,69
Technical Fit
Assesses how well the standard test methods, instrumentation, and design assumptions match the technical capabilities and constraints of the implementing country. In some regions, advanced gait simulators and 3D alignment tools are available, while in others, manual fitting and low-cost materials dominate. A standard that assumes sophisticated test setups may be technically misaligned despite being biomechanically valid.70,71
Contextual Usability
Measures the relevance of the standard to the everyday clinical, social, and environmental context in which the device is used. This includes patient use patterns, terrain, climate, cultural factors (eg., barefoot walking), and rehabilitation availability. A standard that prescribes certain thresholds for wear resistance or angular motion, for instance, may not reflect how a prosthesis is used in low income, high humidity regions.53,72
Documentation Conformance
Examine the compatibility of the standard’s required technical files (eg., labeling, IFU, clinical evidence format) with local regulatory documentation systems. This includes whether the language, structure, and content of testing records, performance claims, and labeling align with regulatory submission guidelines such as FDA’s eSTAR, China’s TCS template, or the EU’s GSPR checklist.73
Regulatory Interoperability
Captures the extent to which the standard supports integration into a local regulatory framework without creating legal, procedural, or classification conflicts. This dimension considers whether the standard can be recognized formally (eg., cited in guidance documents), whether it aligns with national legislation, and whether its adoption facilitates mutual recognition or equivalence agreements.74,75 Each dimension is scored on a normalized 5-point scale, where:
- 1 = Low applicability or high misalignment
- 5 = High applicability and full regulatory compatibility
Scores can be assigned using a combination of expert elicitation, structured literature analysis, and regulatory document review. In practice, these scores can be visualized in a radar chart, allowing direct comparison of the same standard across multiple national regulatory systems (eg., ISO vs. GB vs. FDA implementation). Figure 2 presents this multi-dimensional comparison, highlighting clear differences in regulatory interoperability, documentation conformance, and contextual usability across the FDA, GB/NMPA, and EU MDR systems.
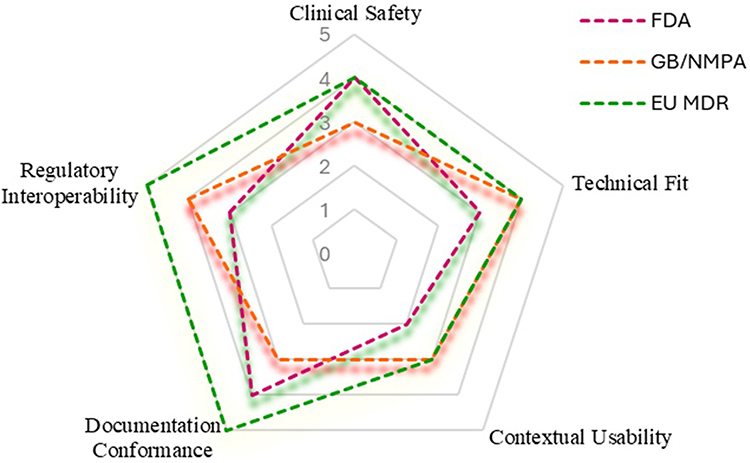 |
Figure 2 Applicability of ISO 10328 Across Major Regulatory Systems Based on a Multi-Dimensional Index Framework. This radar chart visualizes how ISO 10328 aligns with five regulatory dimensions Clinical Safety, Technical Fit, Contextual Usability, Documentation Conformance, and Regulatory Interoperability across the U.S. FDA, China’s GB/NMPA, and the EU MDR systems. Scores (1 = low, 5 = high) reflect evidence informed estimates based on national regulatory practices. The FDA recognizes ISO 10328 [FDA, 2024], but often requires additional labeling and usability data, lowering contextual usability. China’s GB/T standards are aligned with ISO but face translation and documentation adaptation issues [NMPA, 2024]. The EU MDR grants ISO harmonized status under CE marking, resulting in higher documentation and regulatory fit scores [EU MDR, 2017/745]. This figure illustrates the need for structured tools to evaluate standard applicability across diverse regulatory environments. |
This index offers several advantages over existing assessment models. First, it allows for granular analysis identifying precisely which aspects of a standard require modification or supplementation before national adoption. Second, it enables cross system comparison, helping regulators benchmark their frameworks against international peers. Third, it introduces a scalable and adaptable methodology that can evolve as new data (eg., post market surveillance, clinical outcomes, digital twin simulations) become available. Lastly, the model provides a foundation for future AI assisted regulatory tools capable of dynamic, data driven standard evaluations.76,77
Case Study Application: Evaluating ISO 10328 Using the P Knee 5000 Device
To demonstrate the utility of the proposed index system, we apply it to a hypothetical biomechanical product: the P Knee 5000, a passive hydraulic prosthetic knee joint designed for transfemoral amputees. The device incorporates an aluminum alloy frame, adjustable extension dampening, and a modular socket system, and is intended for use in urban and semi-rural environments. It is pre clinically validated using ISO 10328 fatigue, static strength, and torsional resistance protocols, with standard documentation and performance claims structured around ISO guidance.15,78 Using the five-dimension evaluation index, the performance of ISO 10328 as a regulatory support tool for the P Knee 5000 was assessed in three jurisdictions: the United States (FDA), China (GB/NMPA), and the European Union (EU MDR). Scores are derived from regulatory literature, public technical guidance, and known approval workflows, as well as device context assumptions based on product class and patient demographics.79,80 Under FDA review, ISO 10328 supports mechanical validation but fails to meet full clinical and human factors documentation standards required for 510(k) approval. For instance, usability data, patient reported outcomes, and labeling per FDA’s eSTAR submission format are not addressed in ISO testing protocols, leading to downstream documentation and usability gaps. The moderate interoperability score (3) reflects the need for additional premarket and labeling supplements.81–83
In China’s GB/NMPA system, ISO 10328 testing is accepted as a baseline, but domestic conformity testing is often still required, especially under GB/T 14710 and YY/T 0287. Documentation and clinical safety expectations diverge slightly due to unique classification codes, technical requirement forms, and post market adverse event procedures. While technical alignment is strong, documentation fit is limited by format and terminology mismatches. For instance, Mohan et al (2022) reported repeated structural failures in ISO 10328-certified knees used in rural Ghana, attributed to terrain-specific stress patterns not captured during standard testing.8 Representative examples of ISO 10328 compliant prosthetic devices that encountered region-specific performance failures or regulatory actions across different jurisdictions are summarized in Table 3 These real-world failure patterns are further contextualized in Figure 3, which summarizes the dominant causes of prosthetic knee failures in low- and middle-income countries, including terrain mismatch, poor socket fit, alignment errors, unaccounted gait variability, and material degradation.
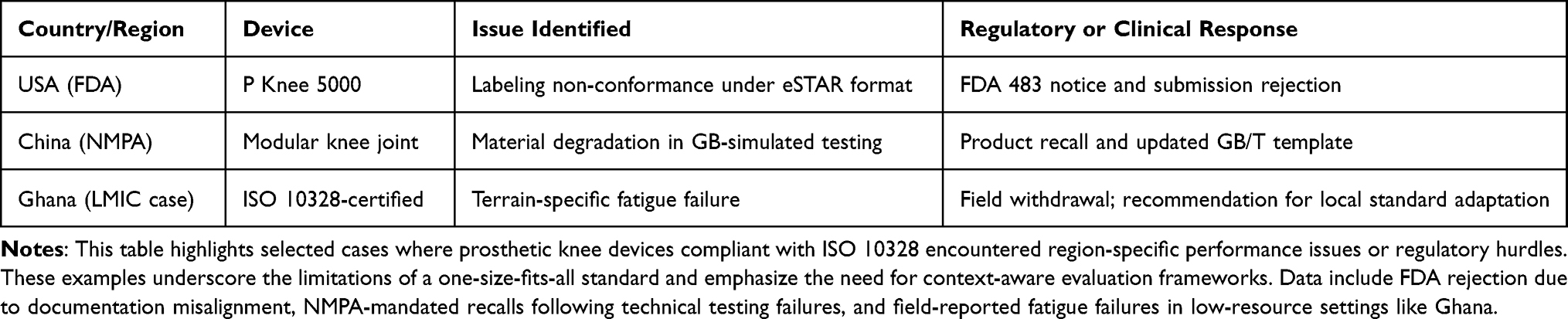 |
Table 3 Real-World Failures and Regulatory Actions Involving ISO-Compliant Prosthetic Devices |
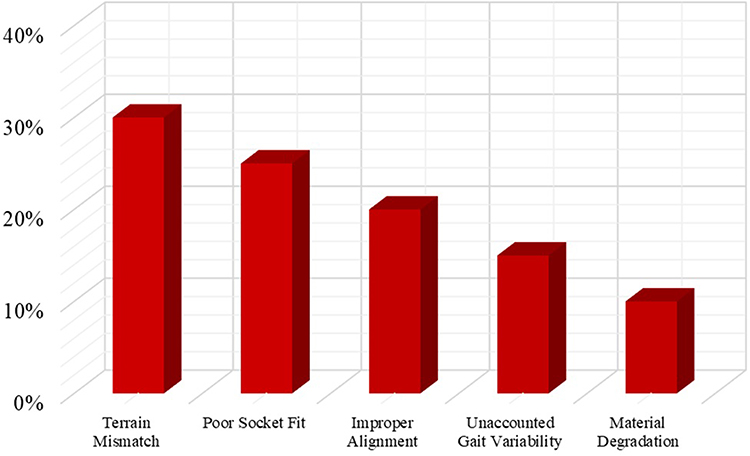 |
Figure 3 Common Failure Causes in LMICs for Prosthetic Knee Devices. This bar chart illustrates the primary causes of prosthetic knee failures reported in low- and middle-income countries (LMICs), based on terrain mismatch, socket misfit, alignment errors, unmodeled gait variability, and material degradation. These real-world challenges highlight gaps in the applicability of ISO 10328, which does not account for contextual use patterns or environmental conditions prevalent in LMICs. |
The EU MDR provides the most consistent alignment. ISO 10328 is listed as a harmonized standard for CE conformity under MDR 2017/745, and performance claims based on ISO data are accepted with limited supplementation. The high documentation and interoperability scores reflect this harmonized status and stronger recognition of biomechanical performance indicators.84 These cross-jurisdictional differences in regulatory alignment for the P Knee 5000 are synthesized in Figure 4, which applies the proposed index framework to visualize how ISO 10328 performs across clinical safety, technical fit, contextual usability, documentation conformance, and regulatory interoperability in the FDA, GB/NMPA, and EU MDR systems. The corresponding numerical index scores underlying this visualization are summarized in Table 4, which presents a comparative applicability matrix of ISO 10328 across regulatory dimensions and jurisdictions. This visualization highlights the uneven regulatory applicability of ISO 10328 across jurisdictions, demonstrating that while technical fit remains relatively consistent, substantial divergence persists in contextual usability, documentation conformance, and regulatory interoperability.
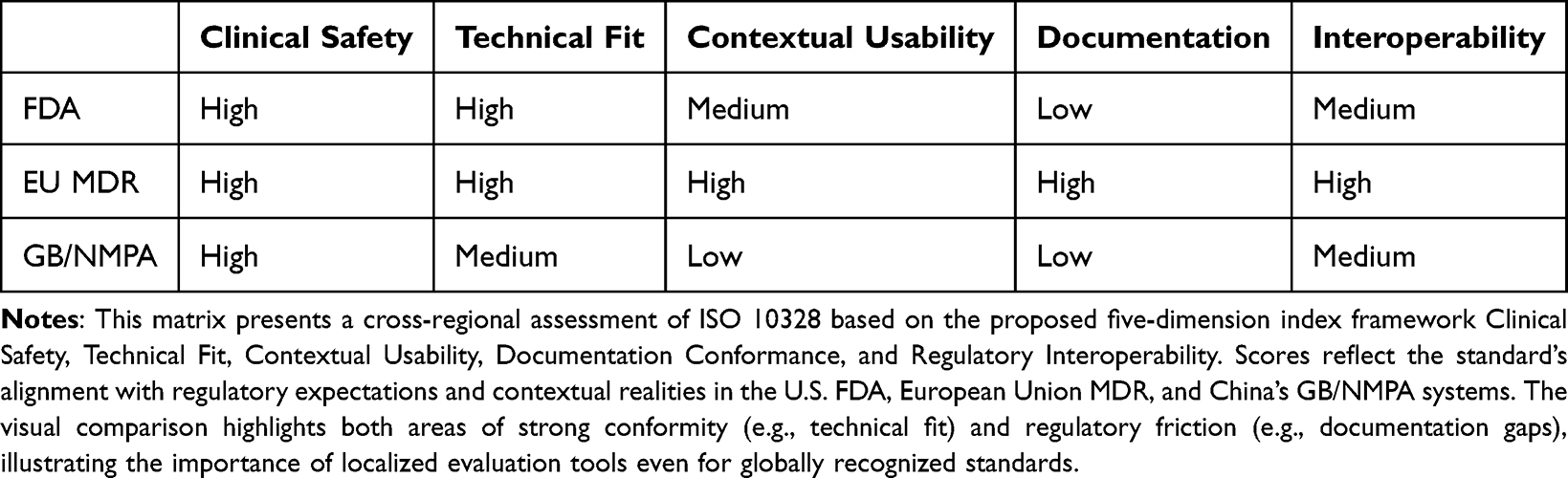 |
Table 4 Comparative Applicability Matrix of ISO 10328 Across Regulatory Dimensions and Jurisdictions |
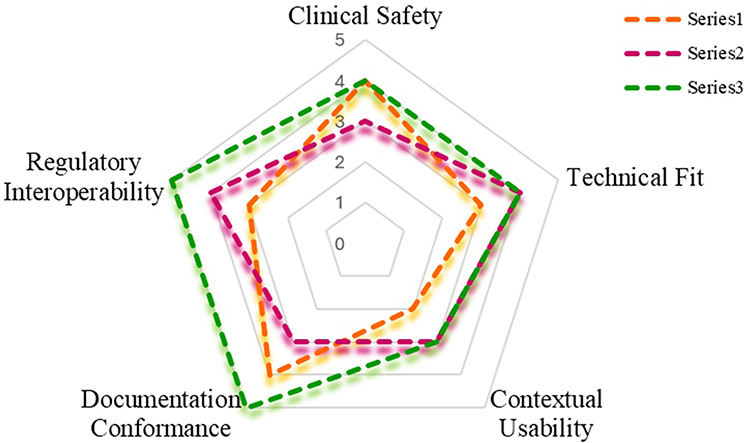 |
Figure 4 Regulatory Applicability of ISO 10328 for the P Knee 5000 Prosthetic Knee Across FDA, GB/NMPA, and EU MDR. This radar chart applies the proposed multi-dimensional index framework covering Clinical Safety, Technical Fit, Contextual Usability, Documentation Conformance, and Regulatory Interoperability to evaluate how ISO 10328 aligns with the regulatory requirements of the FDA (USA), GB/NMPA (China), and EU MDR. The scores (1 = low alignment, 5 = high alignment) are evidence-informed estimates based on known practices, submission formats, and policy documents in each jurisdiction. While the EU MDR exhibits the highest overall alignment due to harmonized standard recognition, both the FDA and GB/NMPA require supplemental testing or documentation, particularly in areas such as contextual usability and post-market integration. This application illustrates how the index can identify policy-relevant gaps even in technically certified devices. |
Policy and Practice Implications
The application of the index framework to ISO 10328 and the hypothetical P Knee 5000 device reveals systemic inconsistencies in how international standards are adopted and enforced across regulatory jurisdictions. While ISO based testing offers a strong biomechanical foundation, it often fails to meet the nuanced documentation, contextual, and legal requirements of national systems. These observations carry important implications for regulatory science, device development, and global standardization policy.2,85,86 By making these inconsistencies visible, the index provides a structured way to distinguish between deficiencies inherent to the standard and those arising from jurisdiction-specific regulatory expectations, which is critical for informed policymaking. Regulatory agencies should move toward institutionalizing structured, preadoption assessments of international standards using tools like the proposed index. Rather than defaulting to full harmonization or rejecting international norms outright, regulators can use such frameworks to assess gaps early in the review process. This enables clearer identification of whether a standard requires direct adoption, targeted modification, or full reinterpretation, thereby reducing downstream review delays and inconsistent enforcement. This would help identify potential friction in areas such as contextual usability or documentation alignment and allow regulatory bodies to issue clearer, targeted guidance to manufacturers. Additionally, embedding such evaluative tools within routine regulatory workflows can help ensure that standards remain responsive to evolving clinical practices and emerging real-world evidence. Integrating the index into digital submission platforms, such as FDA’s eSTAR or China’s TCS system, could enhance transparency and reduce regulatory uncertainty by flagging incompatibilities before formal submission.35,87 The complementary roles of regulators, manufacturers, standards bodies, and researchers in applying and refining the index are summarized in Figure 5, which illustrates how stakeholder-specific interactions support coordinated, context-aware adaptation of international standards. The specific responsibilities and benefits for each stakeholder group when applying the index framework across the device lifecycle are further detailed in Table 5. Figure 6 further demonstrates how these stakeholder inputs are operationalized across the regulatory lifecycle, showing the integration of index-based assessment from standard development and national guidance adaptation through manufacturer planning, regulatory review, and post-market feedback, thereby enabling continuous regulatory learning and refinement.
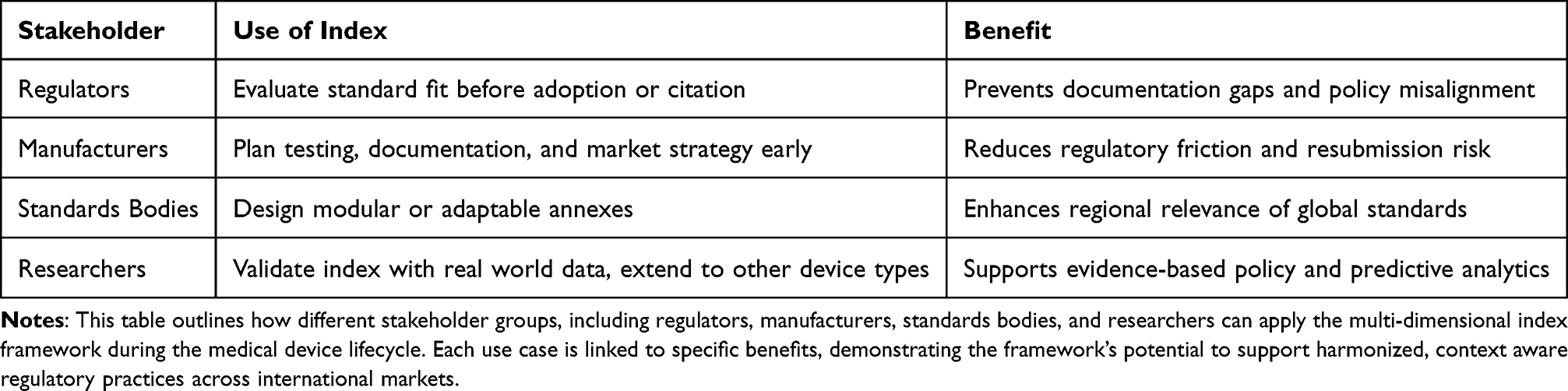 |
Table 5 Stakeholder Specific Roles and Benefits of the Proposed Applicability Index Framework |
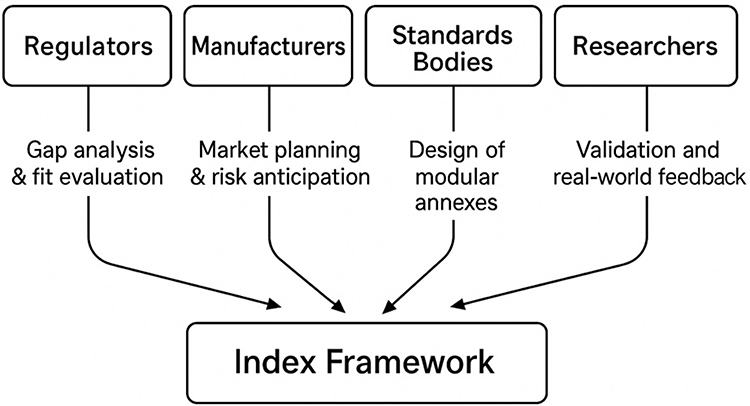 |
Figure 5 Stakeholder-Specific Applications of the Index Framework. This diagram visualizes the interaction of key stakeholders’ regulators, manufacturers, standards bodies, and researchers with the proposed regulatory index. Each entity contributes uniquely to the refinement and application of biomedical standards: regulators apply it to assess pre-adoption fit, manufacturers use it for early compliance planning, standards bodies to develop regional annexes, and researchers for validation and expansion. The framework thus facilitates coordinated adaptation of global standards across diverse policy environments. |
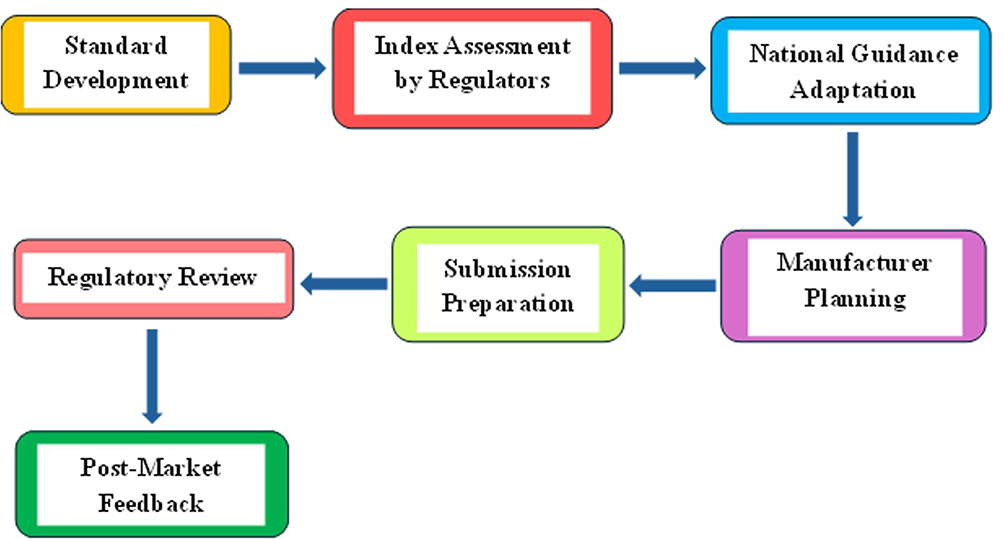 |
Figure 6 Integration of the Applicability Index into the Regulatory Lifecycle. This flowchart illustrates how the proposed multi-dimensional index can be embedded into the regulatory process for medical devices. The process begins with international standard development and proceeds through regulatory evaluation, national adaptation, manufacturer planning, submission, and review. Post market feedback informs future refinements of both national guidance and the index itself, creating a continuous improvement loop. The diagram emphasizes how structured index assessment can enhance both premarket alignment and long-term regulatory learning. |
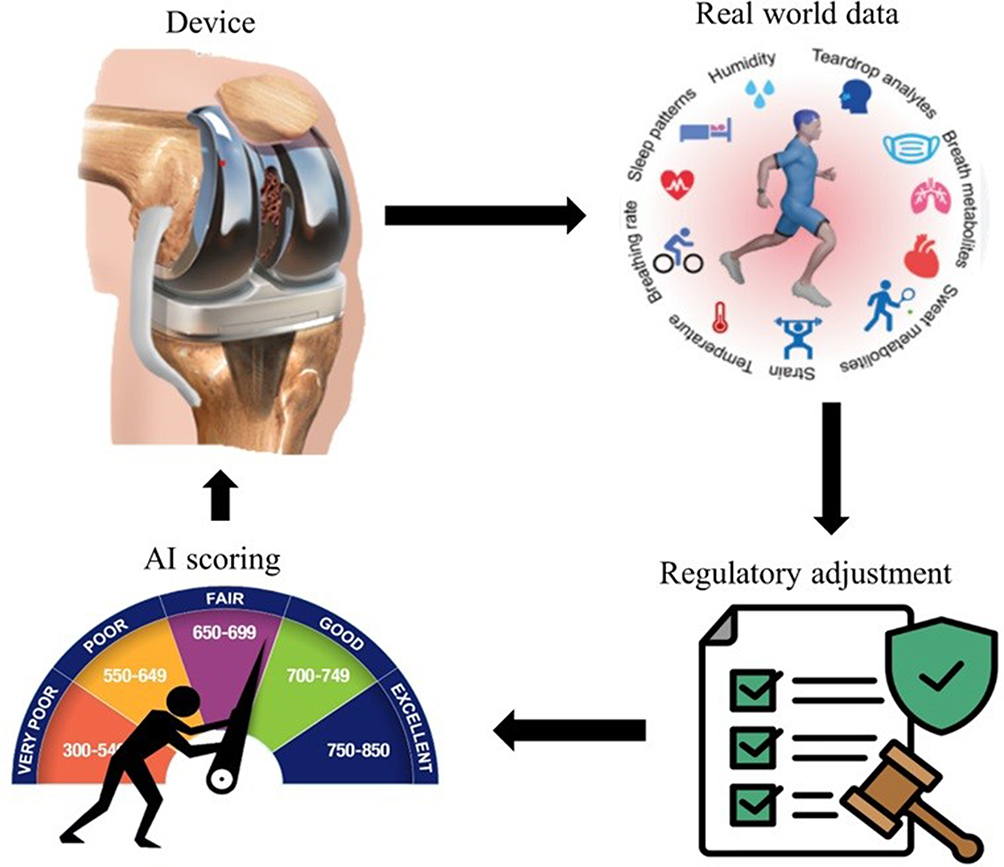 |
Figure 7 Digital Twin + AI Feedback Loop in Standard Scoring. This schematic illustrates a closed-loop model where regulatory standard scoring is dynamically improved using real-world data and AI. It starts with the physical medical device, mirrored by a digital twin model that simulates usage in specific environments. Real-world performance data such as from IMUs or mobile monitoring apps feed into the twin model and are analyzed by an AI engine. The AI evaluates risk patterns, documentation alignment, and post-market outcomes. This analysis updates index scores in real time, which feeds back into both regulatory systems and product design, enabling smarter and more responsive compliance across jurisdictions. |
For manufacturers, especially small and medium sized enterprises, the index provides a practical tool for regulatory readiness planning. By applying the index early during product development, developers can select appropriate standards for targeted markets and adapt their testing or documentation strategies accordingly. A manufacturer aiming for both CE marking and NMPA registration, for example, could use ISO 10328 for baseline mechanical validation while supplementing it with localized documentation formats and additional usability testing. This anticipatory approach would reduce the need for post hoc corrections and redundant submissions.88 International standard setting bodies, including ISO Technical Committees, should consider restructuring standards like ISO 10328 to adopt modular architecture. A core testing methodology could be preserved globally, while context specific annexes could be developed to address regional conditions such as clinical infrastructure, gait pattern variability, and material availability. This model would preserve standard comparability while enabling national flexibility, thereby avoiding one size fits all applications that often undermine practical utility.89,90 The index presented here is conceptual, but it offers a foundation for future policy research and AI driven regulatory analytics. Subsequent studies should apply it to a broader range of devices, from cardiovascular implants to diagnostic imaging tools, and link scoring to real world performance data such as rejection rates and adverse event reports. This would allow the development of dynamic, data driven tools that can automate and personalize standard evaluation processes. In the long term, such tools could be embedded into national regulatory infrastructures or harmonization programs such as the WHO Global Benchmarking Tool.91,92
Ultimately, this framework addresses not only safety and compliance, but also equity. By explicitly evaluating contextual usability and regulatory interoperability, it ensures that international standards are not just technically robust, but also accessible, adaptable, and ethically aligned with diverse clinical environments particularly in low resource or rapidly developing settings. This shift from binary compliance toward adaptive regulatory fit is essential to making global health technologies, such as prosthetics, more inclusive and effective.67,93,94
Conclusion and Future Directions
This review introduces and applies a multi-dimensional, conceptual index framework for evaluating the regulatory applicability of international biomechanical standards, using ISO 10328 and a hypothetical prosthetic knee device as an illustrative case across the FDA, GB/NMPA, and EU MDR systems. By examining not only technical conformity but also contextual usability, documentation conformance, and regulatory interoperability, the framework reveals systematic misalignments between globally harmonized standards and national regulatory expectations. These findings demonstrate that while ISO standards provide a robust technical baseline, their regulatory effectiveness depends on structured, jurisdiction-specific evaluation mechanisms rather than binary compliance alone. The proposed index offers a practical, standard-level evaluation tool that can support regulators in pre-adoption assessment, manufacturers in regulatory readiness planning, and researchers in comparative regulatory analysis. Application to the P Knee 5000 case illustrates that even widely accepted standards may perform unevenly across regulatory systems, reinforcing the need for transparent methods to identify where direct adoption is appropriate and where targeted adaptation is required. In this sense, the primary contribution of this work lies in bridging technical standard development and regulatory decision-making through a systematic, context-aware assessment approach. Future work may extend this framework by linking index dimensions to real-world evidence, such as approval outcomes and post-market surveillance data, enabling more dynamic evaluation of standard applicability over time. Emerging tools, including digital twins, AI-assisted conformity analysis, and structured data infrastructures, may further enhance this approach by supporting adaptive and data-informed regulatory decision-making. Such developments could complement existing system-level initiatives, including the WHO Global Benchmarking Tool, by strengthening standard-level evaluation without duplicating broader regulatory maturity assessments. Overall, this study supports a shift from one-size-fits-all standardization toward adaptive regulatory fit, ensuring that international biomechanical standards remain technically sound, contextually appropriate, and aligned with patient safety and equity across diverse healthcare settings.
Future Integration with Digital Twins and AI
Emerging tools such as digital twins, AI-driven conformity analysis, and real-time data feedback systems offer opportunities to further enhance the proposed applicability index. Digital twin simulations could be used to test ISO standards under context-specific conditions, revealing stress patterns and failure scenarios not captured by conventional laboratory protocols. AI-based scoring engines informed by regulatory decisions, post-market surveillance data, and wearable sensor outputs may enable dynamic updating of risk classifications and identification of documentation gaps. As wearable IMUs and mobile applications increasingly support continuous gait monitoring, performance assumptions embedded in ISO 10328 could be recalibrated using real-world data. Such integration would shift standard evaluation from a static checklist toward a learning system capable of adapting to evolving clinical and regulatory environments. FThis closed-loop interaction between physical devices, digital twin simulations, AI-based scoring, and regulatory adjustment is illustrated in Figure 7, which depicts how real-world evidence can continuously inform and refine standard applicability scores across jurisdictions. Linking the index with Unique Device Identification systems and adverse event databases (e.g., MAUDE, NMPA alerts, EUDAMED) may further support automated, responsive, and equitable device oversight.95
Funding
Research on the transformation evaluation method and application of international standards based on applicability (State Administration for Market Regulation Science and Technology Program, No. 2023MK190; Dean Fund project, No. 572023Y-10377).
Disclosure
The author reports no conflicts of interest in this work.
References
1. Mattei E, Censi F, Calcagnini G. Definition and International Regulations for Medical Devices. In: Medical Devices: Improving Health Care Through a Multidisciplinary Approach. Springer; 2022:55–16.
2. Lamph S. Regulation of medical devices outside the European Union. J Royal Soc Med. 2012;105(1_suppl):12–21. doi:10.1258/jrsm.2012.120037
3. Ehrlich G. Medical Devices IEC International Standards and Conformity Assessment Services in Support of Medical Regulation and Governance. In: Medical Regulatory Affairs. Jenny Stanford Publishing; 2022:209–216.
4. Bonython WE, Arnold BB. Transitioning Up to Best Practice, or Down to the Bare Minimum? Global Harmonisation of Regulation of Therapeutic Goods. In: Globalisation in Transition: Human and Economic Perspectives. Springer; 2023:45–65.
5. Tamura A, Kutsumi H. Multiregional medical device development: regulatory perspective. Clin J Gastroenterol. 2014;7(2):108–116. doi:10.1007/s12328-014-0478-2
6. Tranquillo J, Goldberg J, Allen R. Biomed Engineer Design. Academic Press; 2022.
7. Elahi B. Safety Risk Management for Medical Devices. Academic Press; 2021.
8. Su G, Deng D. Evolution of China regulatory guidance on the clinical evaluation of medical devices and its implication on pre-market and post-approval clinical evaluation strategies. Exp Rev Med Devices. 2023;20(3):167–178. doi:10.1080/17434440.2023.2184258
9. Sun Q, Yan L. Better medical devices regulations for better health care: enlightenment for medical devices regulatory reform in China, from experiences of the EU and the USA. Chin J Med Instrument. 2006;30(1):43–52.
10. Fink M, Akra B. Comparison of the international regulations for medical devices–USA versus Europe. Injury. 2023;54:110908. doi:10.1016/j.injury.2023.110908
11. Martelli N, Eskenazy D, Déan C, et al. New European regulation for medical devices: what is changing? Cardiovasc Intervent Radiol. 2019;42(9):1272–1278. doi:10.1007/s00270-019-02247-0
12. Melvin T. The European medical device regulation–what biomedical engineers need to know. IEEE J Translat Engineer Health Med. 2022;10:1–5. doi:10.1109/JTEHM.2022.3194415
13. Kumar A, Vinita. Prosthetic socket designs in rehabilitation and improving healthcare to the transtibial amputee: challenges and opportunities. Revolut Product Design Healthc. 2022;143–161.
14. Hansen AH. A biomechanist’s perspective on partial foot prostheses. JPO. 2007;19(8):P80–P84.
15. Liang W, Qian Z, Chen W, et al. Mechanisms and component design of prosthetic knees: a review from a biomechanical function perspective. Front Bioengineer Biotechnol. 2022;10:950110. doi:10.3389/fbioe.2022.950110
16. Affatato S, Valigi MC, Logozzo S, et al. Wear distribution detection of knee joint prostheses by means of 3D optical scanners. Materials. 2017;10(4):364.
17. Sophie H, Silvia T, Renaud R. Online learning of the dynamical internal model of transfemoral prosthesis for enhancing compliance. IEEE Robotic Automat Lett. 2021;6(4):6156–6163.
18. Mallon CM, Hill RG, Moore AJ. Infection after knee replacement: a qualitative study of impact of periprosthetic knee infection. BMC Musculoskeletal Disord. 2018;19(1):1–10.
19. Villa T, Migliavacca F, Gastaldi D, et al. Contact stresses and fatigue life in a knee prosthesis: comparison between in vitro measurements and computational simulations. J Biomechanics. 2004;37(1):45–53.
20. Mohanty RK, Mohanty R, Sabut S, Pandey M. Conformity assessment with structural strength requirements of mechanical polycentric prosthetic knee used for amputee rehabilitation. Comput Method Biomechan Biomed Engineer. 2023;26(7):764–776. doi:10.1080/10255842.2022.2088233
21. Bergmann G, Kutzner I. Wear of knee implants: are the ISO test loads realistic? Bone Joint. 2013:15.
22. Paul J. Mechanics of the knee joint and certain joint replacements. In: Total Knee Replacement: Proceeding of the International Symposium on Total Knee Replacement, May 19–20, 1987, Nagoya, Japan 1988. Tokyo: Springer; 1988:25–37.
23. Kent JA, Takahashi KZ, Stergiou N. Uneven terrain exacerbates the deficits of a passive prosthesis in the regulation of whole body angular momentum in individuals with a unilateral transtibial amputation. J Neuroengineer Rehabilitat. 2019;16(1):25. doi:10.1186/s12984-019-0497-9
24. Olsen J, Turner S, Chadwell A, et al. The impact of limited prosthetic socket documentation: a researcher perspective. Front Rehabilitat Sci. 2022;3:853414. doi:10.3389/fresc.2022.853414
25. Sullivan LM, Creveling S, Cowan M, Gabert L, Lenzi T. Powered knee and ankle prosthesis control for adaptive ambulation at variable speeds, inclines, and uneven terrains.
26. Xiaofang Y, Chunren W, Deyu L. Reviews on Medical Devices Standardization System in China. Springer; 2013:1529–1532.
27. Levin M. More than standards and regulations are needed to provide safe and effective devices. Biomed Instrumentat Technol. 2001;35(5):331–337.
28. Cho IY, Choi KH, Sheen YY. How does “Regulatory practice” create discrepancies in drug label information between Asian and Western countries? Different label information for direct oral anticoagulants approved in the United States, Europe, Korea, and Japan. Therap Innovat Regulat Sci. 2019;53(2):233–242. doi:10.1177/2168479018769301
29. Panteghini M. Implementation of standardization in clinical practice: not always an easy task. Clin Chem Laborat Med. 2012;50(7):1237–1241. doi:10.1515/cclm.2011.791
30. Henshaw F, Karasouli E, King R, et al. Engineering standards for trauma and orthopaedic implants worldwide: a systematic review protocol. BMJ Open. 2018;8(10):e021650. doi:10.1136/bmjopen-2018-021650
31. Mell S, Fullam S, Wimmer M, Lundberg H. Are there differences between the old and new international standards for TKR pre-clinical wear testing? An FEA analysis using adaptive remeshing. Bone Joint. 2017:6.
32. Consortium METR. Development of a prosthetic fit and alignment assessment (ProFit) in persons with post-traumatic transtibial amputation. Prosthetics Orthotics Int. 2023;47(6):599–606.
33. Clarke L, Ridgewell E, Dillon MP. Identifying and linking prosthetic outcomes to the ICF framework: a step to inform the benefits measured in prosthetic health economic evaluations. Disab Rehabilitat. 2023;45(6):1103–1113. doi:10.1080/09638288.2022.2049902
34. De Carvalho NP. Technical standards, intellectual property, and competition-a holistic view. Wash UJL Pol’y. 2015;47:61.
35. Schonfeld R, Dobinson J. Using international standards: a wake-up call to regulators? ASTM Standardizat News. 2004;32(1).
36. Zhong D, Kirwan MJ, Duan X. Regulatory barriers blocking standardization of interoperability. JMIR mHealth uHealth. 2013;1(2):e2654. doi:10.2196/mhealth.2654
37. Baron J, Contreras JL, Husovec M, Larouche P, Thumm N. The technical standardization ecosystem and institutional decision making: the case of intellectual property rights policies. TIlburg Univer TILEC Discus. 2020;2020:1–46.
38. Clougherty JA, Grajek M. International standards and international trade: empirical evidence from ISO 9000 diffusion. Int J Indust Organizat. 2014;36:70–82. doi:10.1016/j.ijindorg.2013.07.005
39. Spickernell DG. The role of international standards in removing barriers to trade and assisting developing countries. Int J Technol Manage. 1986;1(1–2):197–208.
40. Delimatsis P. Continuity and change in international standardization. Contin Change Int Standard. 2015.
41. Tkaczyk KM. Translating medical devices: a rule-driven game. Medical Writing. 2024;33(1):54–56. doi:10.56012/kiyl5926
42. Al-Tarawneh A, Al-Badawi M, Hatab WA. Translating governance and legal compliance: exploring the role of translation in facilitating corporate reporting and policy implementation. Corporate Law Governance Rev. 2024;6(3):27–36. doi:10.22495/clgrv6i3p3
43. Judd T. Post-market Surveillance (PMS) of Medical Devices: from a Clinical Engineering Perspective. In: Inspection of Medical Devices: For Regulatory Purposes. Springer; 2023:93–114.
44. Feigal DW. Postmarket Considerations in Biomaterials and Medical Devices. In: Biomaterials Science. Elsevier; 2013: 1472–1476.
45. Mattox E. Medical devices and patient safety. Critical Care Nurse. 2012;32(4):60. doi:10.4037/ccn2012925
46. Harer J. Post-market surveillance and vigilance on the European market. In: Medical Devices and in Vitro Diagnostics: Requirements in Europe. Springer; 2023:585–623.
47. Fiedler G, Johnson MS. Correlation of transtibial prosthetic alignment quality and step-by-step variance of gait. JPO. 2017;29(1):19–25.
48. Owen MK, DesJardins JD. Transtibial prosthetic socket strength: the use of ISO 10328 in the comparison of standard and 3D-printed sockets. JPO. 2020;32(2):93–100.
49. Hamner S, Narayan V, Rappin N, Donaldson K. ReMotion Knee: scaling of an Affordable Prosthetic Knee for Developing Countries. In: Technologies for Development: What Is Essential? Springer; 2015:137–151.
50. Jensen JS, Treichl HB. Mechanical testing of prosthetic feet utilized in low-income countries according to ISO-10328 standard. Prosthetics Orthotics Int. 2007;31(2):177–206. doi:10.1080/03093640701210986
51. Hamner SR, Narayan VG, Donaldson KM. Designing for scale: development of the remotion knee for global emerging markets. Ann Biomed Engineer. 2013;41(9):1851–1859. doi:10.1007/s10439-013-0792-8
52. Reddie M, Bedi S, Vaidya M, Griffin A, Petelina NT, Winter AG. Achieving High Performance and Low Cost: Development of a High-Performing Passive Prosthetic Knee for Emerging Markets. American Society of Mechanical Engineers; 2023:V03BT03A021.
53. Chen C, Chen X, Yin S, et al. Enhancing prosthetic safety and environmental adaptability: a visual-inertial prosthesis motion estimation approach on uneven terrains.
54. Darrow JJ, Avorn J, Kesselheim AS. FDA regulation and approval of medical devices: 1976-2020. JAMA. 2021;326(5):420–432. doi:10.1001/jama.2021.11171
55. Kramer DB, Tan YT, Sato C, Kesselheim AS. Ensuring medical device effectiveness and safety: a cross-national comparison of approaches to regulation. Food Drug Law J. 2014;69(1):1.
56. Sorenson C, Drummond M. Improving medical device regulation: the United States and Europe in perspective. Milbank Quarterly. 2014;92(1):114–150. doi:10.1111/1468-0009.12043
57. Sharma A, Luthra G. Implementing a risk-based approach to quality management system ISO-13485 processes in compliance with EUMDR 2017/745 for medical device industry. J Pharmaceut Res Int. 2023;35(13):8–19. doi:10.9734/jpri/2023/v35i137365
58. Smogavc Cestar A, Harer J. Mastering Quality System Audits and Inspections for Medical Devices. In: Medical Devices and in Vitro Diagnostics: Requirements in Europe. Springer; 2023:543–584.
59. Harer J. Manufacturing and Quality Assurance in Compliance with the MDR and IVDR. In: Medical Devices and in Vitro Diagnostics: Requirements in Europe. Springer; 2023:1–38.
60. Nah E-H, Cho S, Kim S, et al. International organization for standardization (ISO) 15189. Ann Laborat Med. 2017;37(5):365–370. doi:10.3343/alm.2017.37.5.365
61. Heneghan C, Thompson M. Rethinking Medical Device Regulation. London, England: SAGE Publications Sage UK; 2012:186–188.
62. Egbosimba D. Medical devices industry: the problem of clinical evaluation reports. 2019:514–516.
63. Resnic FS, Majithia A. Postmarket Medical Device Safety: Moving Beyond Voluntary Reporting. BMJ Publishing Group Ltd; 2018:174–175.
64. Venkatesh M, Bandla D. Regulatory assessment of premarket approval of medical devices in US and EU. Int J Pharm Clin Res. 2017;9(4):281–285. doi:10.25258/ijpcr.v9i04.8534
65. Kearney B, McDermott O. The challenges for manufacturers of the increased clinical evaluation in the European medical device regulations: a quantitative study. Therapeut Innovat Regulat Sci. 2023;57(4):783–796. doi:10.1007/s43441-023-00527-z
66. Han Y, Bergmann J. Transforming medical regulations into numbers: vectorizing a decade of medical device regulatory shifts in the usa, eu, and China. arXiv preprint arXiv:241100567. 2024.
67. Teli MS, Jhawat V, Sharma AK. Development of a comprehensive regulatory model for medical devices. BIO Integration. 2024;5(1):972. doi:10.15212/bioi-2024-0030
68. Valli C. Transforming perioperative patient safety clinical guidelines recommendations into measurable standards: insights from the SAFEST project. Eur J Public Health. 2023;33(Supplement_2):
69. Oikonomou E, Carthey J, Macrae C, Vincent C. Patient safety regulation in the NHS: mapping the regulatory landscape of healthcare. BMJ Open. 2019;9(7):e028663. doi:10.1136/bmjopen-2018-028663
70. Armand S, Sawacha Z, Goudriaan M, et al. Current practices in clinical gait analysis in Europe: a comprehensive survey-based study from the European society for movement analysis in adults and children (ESMAC) standard initiative. Gait Posture. 2024;111:65–74. doi:10.1016/j.gaitpost.2024.04.014
71. You R, Tang W, Duffield CF, Zhang L, Hui F, Kang Y. Analytical framework for understanding the differences between technical standards originating from various regions to improve international hydropower project delivery. Water. 2022;14(4):662. doi:10.3390/w14040662
72. Bosman CE, van der Sluis CK, Geertzen JH, Kerver N, Vrieling AH. User-relevant factors influencing the prosthesis use of persons with a transfemoral amputation or knee-disarticulation: a meta-synthesis of qualitative literature and focus group results. PLoS One. 2023;18(1):e0276874. doi:10.1371/journal.pone.0276874
73. Jordan D. An overview of the Common Technical Document (CTD) regulatory dossier. Medical Writing. 2014;23(2):101–105. doi:10.1179/2047480614Z.000000000207
74. Christl LA, Woodcock J, Kozlowski S. Biosimilars: the US regulatory framework. Ann Rev Med. 2017;68(1):243–254. doi:10.1146/annurev-med-051215-031022
75. Schroder HZ. Harmonization, Equivalence and Mutual Recognition of Standards in WTO Law. Kluwer Law International BV; 2011.
76. Shi J, Chen X, Hu H, Ung COL. Benchmarking drug regulatory systems for capacity building: an integrative review of tools, practice, and recommendations. Int J Health Polic Manage. 2023;12:8100. doi:10.34172/ijhpm.2023.8100
77. Pantanowitz L, Hanna M, Pantanowitz J, et al. Regulatory aspects of artificial intelligence and machine learning. Modern Pathol. 2024;37(12):100609. doi:10.1016/j.modpat.2024.100609
78. Fu H, Zhang X, Wang X, et al. A novel prosthetic knee joint with a parallel spring and damping mechanism. Int J Advanc Robotic Syst. 2016;13(4):1729881416658174. doi:10.1177/1729881416658174
79. Sun S, Heske S, Mercadel M, Wimmer J. Predicting regulatory product approvals using a proposed quantitative version of FDA’s benefit–risk framework to calculate net-benefit score and benefit–risk ratio. Therap Innovat Regulat Sci. 2021;55(1):129–137. doi:10.1007/s43441-020-00197-1
80. Su G. Could one strategy fit all? A comparison of regulatory guidance from China, Europe, and the USA on medical device clinical evaluation throughout the total product lifecycle. Exp Rev Med Dev. 2025;22(1):5–13. doi:10.1080/17434440.2024.2448848
81. Rojas KM, Sharareh N, Cosier L, Santos DL. Considering the Dynamics of FDA Human Factors ValidationRequirement: Implications of Failure and Need to Ensure Projectsuccess-A Conceptual Framework. Los Angeles, CA: SAGE Publications Sage CA; 2019:234–247.
82. Sawyer D. Medical Device Requirements, Human Factors, and the Food and Drug Administration (FDA). Los Angeles, CA: SAGE Publications Sage CA; 2000:526–527.
83. US Food and Drug Administration. Clinical performance assessment: considerations for computer-assisted detection devices applied to radiology images and radiology device data in premarket notification (510 (k)) submissions. Guid Indust Food Drug Administ Staff. 2020.
84. Soundarya Reddy K, Sahitya Reddy K, Haripriya. Regulatory skeleton of medical devices in the European Union. Int J Drug Regulat Affairs. 2023;11(4). doi:10.22270/ijdra.v11i4.630
85. Bartolini C, Giurgiu A, Lenzini G, Robaldo L. Towards Legal Compliance by Correlating Standards and Laws with a Semi-Automated Methodology. Springer; 2016:47–62.
86. Casati S, Aschberger K, Barroso J, et al. Standardisation of defined approaches for skin sensitisation testing to support regulatory use and international adoption: position of the International Cooperation on Alternative Test Methods. Archiv Toxicol. 2018;92(2):611–617. doi:10.1007/s00204-017-2097-4
87. Wijkström EN, McDaniels D. Improving regulatory governance: international standards and the WTO TBT agreement. J World Trade. 2013;47(5).
88. Basu AK, Basu A, Ghosh S, Bhattacharya S. MEMS Applications in Electronics and Engineering. AIP Publishing LLC; 2022.
89. by SME A. The emerging ISO10303 modular architecture. 2005.
90. Feeney AB, Price DM. A modular architecture for STEP. 2000.
91. Khinvasara T, Tzenios N, Shanker A. Post-market surveillance of medical devices using AI. J Complement Alternat Med Res. 2024;25(7):108–122. doi:10.9734/jocamr/2024/v25i7552
92. Wellnhofer E. Real-world and regulatory perspectives of artificial intelligence in cardiovascular imaging. Front Cardiovascul Med. 2022;9:890809. doi:10.3389/fcvm.2022.890809
93. Iserson KV. Providing Ethical Healthcare in Resource-Poor Environments. Springer; 2020:293–312.
94. Jain A, Singh RK, Bhushan P. Policy and regulatory frameworks for financing smart healthcare. In: Driving Global Health and Sustainable Development Goals with Smart Technology. IGI Global Scientific Publishing; 2025:367–388.
95. Valdes T, Robinson D, Fellhauer D, Waheed S, Konduri I. Utilizing unique device identifiers to enhance adverse event analysis. J Clin Engineer. 2025;50(1):39–43. doi:10.1097/JCE.0000000000000682
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Wear of Femoral Head Taper Connections of Contemporary Total Hip Prostheses: An Experimental Study
Ribeiro de Sousa M, Neuvonen PS, Saikko V
Medical Devices: Evidence and Research 2025, 18:595-613
Published Date: 29 November 2025