Back to Journals » Patient Preference and Adherence » Volume 20
A Multidimensional Framework for Pharmaceutical Care to Enhance Medication Adherence and Patient Engagement: The CMO–MAPEX Model
Authors Morillo-Verdugo R ![]() , Ibarra-Barrueta O
, Ibarra-Barrueta O ![]() , Martin Conde MT
, Martin Conde MT ![]() , Vicente-Escrig E, Contreras Macias E
, Vicente-Escrig E, Contreras Macias E
Received 23 December 2025
Accepted for publication 25 February 2026
Published 27 February 2026 Volume 2026:20 591288
DOI https://doi.org/10.2147/PPA.S591288
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Johnny Chen
Ramón Morillo-Verdugo,1 Olatz Ibarra-Barrueta,2 Maria Teresa Martin Conde,3 Esther Vicente-Escrig,4 Enrique Contreras Macias5
1Pharmacy Department, Virgen de Valme University Hospital, South Seville Health District, Seville, Spain; 2Pharmacy Department, Galdakao-Usansolo University Hospital, Osakidetza, Biobizkaia Health Research Institute, Galdakao, Spain; 3Pharmacy Department, Hospital Clínic of Barcelona, Barcelona, Spain; 4Pharmacy Department, Castellón General University Hospital, Castellón, Spain; 5Pharmacy Department, San Juan de Dios Hospital, Seville, Spain
Correspondence: Ramón Morillo-Verdugo, Pharmacy Department, Virgen de Valme University Hospital, South Seville Health District, Seville, Spain, Tel +34 955 015 467, Email [email protected]
Purpose: This study aimed to develop Capacity–Motivation–Opportunity MAPEX (CMO–MAPEX), a multidimensional, patient-centred and operational framework to guide medication-adherence support in outpatient pharmaceutical care.
Methods: A six-stage framework-development process was undertaken. First, a narrative scoping synthesis identified behavioural, experiential and organisational determinants of medication adherence relevant to outpatient pharmaceutical care. Second, key constructs were extracted and coded into a shared analytic matrix. Third, framework analysis was applied to cluster constructs into higher-order domains. Fourth, an integrative synthesis aligned the emergent CMO structure with evidence on adherence, treatment burden, patient experience and hybrid-care models. Fifth, the conceptual architecture was translated into a structured clinical workflow incorporating CMO-based assessment, a three-level complexity stratification system, domain-specific intervention families and hybrid follow-up rules. Finally, a multidisciplinary expert panel reviewed and refined the framework to ensure ecological validity and feasibility in routine practice.
Results: The analysis yielded a stable three-domain structure—Capacity, Motivation and Opportunity—capturing patients’ ability to manage treatment, their beliefs and emotional readiness, and the contextual conditions enabling or hindering adherence. These domains were operationalised through assessment indicators, complexity-based stratification, targeted intervention mapping and longitudinal hybrid-care pathways. Patient-reported outcome and experience measures were embedded as core components to monitor treatment burden, preferences and experience, and to support dynamic re-stratification and adjustment of follow-up intensity over time.
Conclusion: CMO–MAPEX provides a pragmatic and scalable framework that translates adherence theory into patient-centred pharmaceutical care. By integrating behavioural determinants, patient experience and hybrid-care organisation within a single operational structure, it offers a reproducible approach to tailoring adherence support according to patient preferences and complexity in outpatient settings.
Keywords: medication adherence, patient preference, patient engagement, patient-reported outcome measures, telepharmacy, pharmaceutical care
Introduction
Medication adherence remains one of the most enduring and costly challenges in chronic disease management, impacting clinical outcomes, patient experience, and health-system efficiency.1,2 Despite sustained research efforts and the availability of multiple theoretical models, real-world adherence in chronic pharmacotherapy continues to be suboptimal across therapeutic areas.3 Poor adherence is associated with avoidable hospitalisations, reduced quality of life, increased therapy failure, and the unnecessary escalation of treatment.1,3 Within outpatient specialty pharmacy practice, where sustained patient support is integral to clinical practice, optimizing medication adherence and strengthening patient engagement has emerged as a critical priority, with direct implications for patient safety, continuity of care, and patient-reported outcomes.
A key difficulty in improving adherence is the inherently multidimensional nature of medication-taking behaviour.4,5 Cognitive, emotional, functional, social, logistical, and organisational factors interact to shape patients’ medication adherence behaviours.4 Traditional interventions focusing exclusively on education or reminders have shown limited effectiveness because they address only a fraction of the determinants influencing adherence.5 Consequently, recent years have seen the emergence of models emphasising behavioural and experiential dimensions—such as the Necessity–Concerns Framework,6 the ABC taxonomy,7 and treatment-burden theory.8 These frameworks have advanced conceptual understanding by highlighting that beliefs, expectations, motivation, and perceived burden are crucial in shaping adherence behaviour.
However, none of these models has been explicitly developed to address the operational realities of pharmaceutical care (PC). They offer conceptual clarity but do not explain how to translate behavioural determinants into structured workflows, how to adapt follow-up intensity to patient needs, or how to integrate in-person and remote activities in a coherent and scalable way for outpatient pharmacy team. In practice, pharmacists must balance clinical tasks, patient preferences, digital tools, resource constraints, and the increasing demand for longitudinal follow-up. Existing adherence models do not provide a practical roadmap to guide these decisions.
At the same time, health systems are undergoing rapid transformation. Hybrid models that combine face-to-face visits with telepharmacy, digital monitoring, and remote communication have become increasingly relevant, especially for chronic care.9 Patient-reported outcomes (PROMs) and experience measures (PREMs) are being incorporated into routine practice to capture patients’ perceptions of the treatment, the overall illness burden, and their interactions with the healthcare system.10 These developments require a framework capable of integrating behavioural, experiential, and organisational dimensions into a single operational structure aligned with patients’ preferences and daily lives.
In outpatient settings, clinical pharmacists are uniquely positioned to support medication adherence by providing personalised education, motivational support, care coordination, and follow-up. Yet the lack of an operational, patient-centred, and adaptable framework limits the consistency and scalability of adherence-enhancing strategies. There remains a gap between theoretical models and the practical demands of outpatient PC, particularly when addressing complex patients with fluctuating needs, multimorbidity, or barriers to accessing in-person care.11,12
The CMO–MAPEX model was developed to address this gap. Its conceptual structure is based on three domains—Capacity, Motivation, and Opportunity—but, unlike other frameworks, it is not derived from COM-B nor conceptually aligned with it, despite superficial similarity in terminology.13,14 CMO–MAPEX originates from the needs and workflow of PC, as defined in contemporary re-conceptualisations of the discipline,13 rather than from a behaviour-change theory. The model was designed independently to capture the dimensions that pharmacists routinely encounter in practice: the patient’s ability to manage treatment (Capacity), their beliefs and emotional readiness (Motivation), and the contextual conditions that facilitate or hinder adherence (Opportunity). Each of these domains is explicitly defined through assessment indicators, intervention categories, and follow-up pathways that reflect the organisation of outpatient pharmacy.15
Beyond its behavioural foundation, CMO–MAPEX incorporates two elements essential to patient-centred adherence care. First, it embeds PROMs and PREMs into the assessment and follow-up process, recognising that adherence is shaped not only by behaviour but also by the patient’s lived experience of treatment.15–18 Second, it integrates hybrid care models, digital monitoring tools, remote counselling—into a longitudinal pathway that combines accessibility with personalised support.19,20 By linking behavioural determinants, experiential measures, and operational workflows, the model aims to provide a reproducible system for tailoring interventions, stratifying patients according to their level of complexity, and adapting follow-up intensity over time.21 The framework is conceptually aligned with national quality standards for pharmaceutical care and has been progressively incorporated into Spanish hospital pharmacy practice, particularly through its compatibility with the QPEX certification framework.22
While most adherence approaches focus on identifying the factors and barriers underlying non-adherence, few provide guidance on how to systematically organise PC services to effectively address these challenges. CMO–MAPEX seeks to bridge this gap by offering a unified framework that translates theory into practice. It is designed to standardise decision-making, support consistent care delivery, incorporate patient preferences and experiences, and enhance engagement across diverse chronic conditions.23–26 Importantly, the model can be applied flexibly across therapeutic areas while maintaining a common operational structure, making it suitable for integration into routine outpatient pharmacy practice.15
This work addresses relevant gaps in the existing literature, particularly the limited availability of multidimensional adherence frameworks integrating behavioural, experiential, and pharmacotherapeutic determinants, as well as the scarcity of operational models translating these concepts into structured pharmaceutical-care workflows.
In this context, the objective of this study is to develop a multidimensional, patient-centred, and operational framework that integrates behavioural determinants, patient-reported outcomes, and hybrid care pathways into a coherent model to guide medication-adherence support in outpatient PC.
Materials and Methods
This study followed a structured and transparent multi-stage process to develop the CMO–MAPEX framework as an operational, patient-centred model for supporting medication adherence in outpatient PC. The aim was to ensure conceptual rigour, ecological validity and traceability throughout framework development. The methodological approach was informed by recognised guidance on conceptual-framework development in health research27 and combined narrative evidence synthesis,28 framework analysis29 and expert consultation.30 The process unfolded in six iterative stages.
To ensure conceptual breadth and transparency, the first stage began with a structured narrative scoping synthesis of the behavioural, experiential and organisational determinants of medication adherence relevant to outpatient PC (Table 1). Searches were conducted in PubMed/MEDLINE, Scopus and Web of Science, using broad combinations of terms related to medication adherence, behavioural determinants, patient experience, treatment burden, PC, and hybrid or telepharmacy models. This stage followed a structured narrative scoping approach aimed at identifying conceptually relevant determinants rather than conducting a formal systematic review. Sources were selected based on conceptual relevance and contribution to framework development, applying a thematic saturation logic.
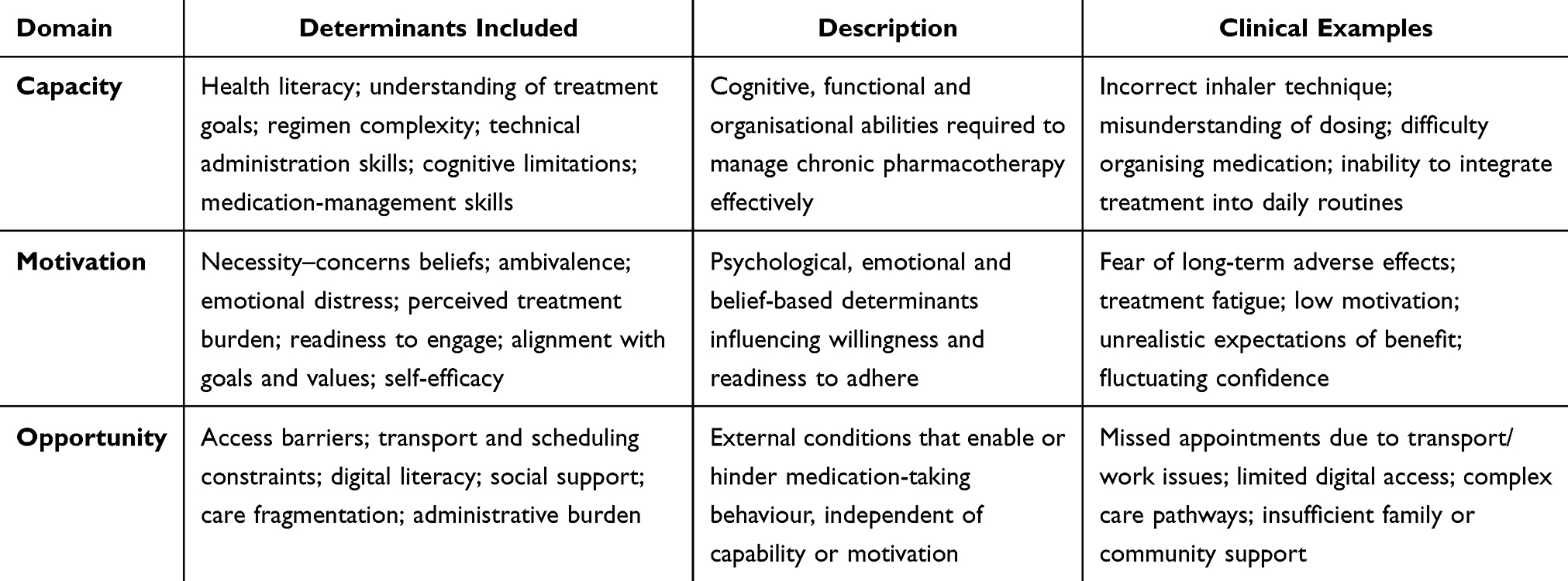 |
Table 1 Behavioural, Experiential and Contextual Determinants Mapped to the CMO–MAPEX Model |
Inclusion criteria focused on sources that: (a) examined behavioural, experiential or contextual determinants influencing adherence; (b) proposed conceptual or organisational models applicable to chronic therapy management; or(c) informed the role of outpatient pharmacist in long-term follow-up. Journal ranking was not used as an inclusion criterion, as the objective was conceptual comprehensiveness rather than hierarchical evidence selection. The literature considered spanned from database inception to December 2025. The searches yielded approximately 200–240 potentially relevant records across databases. Following screening for conceptual relevance, theoretical diversity, and thematic contribution, approximately 40–50 sources informed construct extraction and framework development. Consistent with the narrative scoping design, emphasis was placed on conceptual saturation rather than exhaustive enumeration.
Two reviewers independently screened abstracts and full texts for conceptual relevance. Extracted constructs were entered into a shared coding matrix that captured definitions, theoretical origins and illustrative content. This matrix served as the basis for subsequent framework analysis.
Data saturation was monitored continuously, and additional sources were incorporated until no new determinants, categories, or conceptual relationships emerged. The synthesis emphasised conceptual convergence rather than quantitative aggregation and provided the foundational structure upon which subsequent analytic and operational phases of the model were developed.
This narrative synthesis aimed to identify conceptually relevant determinants to inform the development of the framework rather than to provide a comprehensive evidence map.
In the second stage, key constructs were identified and coded. Two researchers independently reviewed the included bibliography and extracted adherence-relevant constructs related to: capability, literacy, and functional skills; motivational, emotional, and belief-based determinants; contextual, environmental, and organisational barriers; patient-reported outcomes, treatment burden, and experiential drivers; and operational aspects of outpatient PC.
Constructs were organised in a shared coding matrix capturing description, theoretical origin and illustrative examples. Extraction followed an iterative refinement process. Overlapping constructs were compared and merged when appropriate; disagreements were resolved through structured discussion until conceptual saturation was reached.
In Stage 3, constructs were categorised into higher-order domains. Using a framework-analysis approach, the extracted constructs were clustered into conceptually coherent higher-order domains. Through constant comparison, three overarching and mutually exclusive categories emerged:
Capacity – patient knowledge, skills, functional ability, literacy and treatment-management capability.
Motivation – beliefs, expectations, emotional state, ambivalence, readiness and perceived burden.
Opportunity – logistical, organisational, social, contextual and system-level determinants that enable or hinder adherence.
These domains demonstrated internal coherence and external distinction and accommodated all extracted determinants.
In Stage 4, an integrative synthesis was undertaken to build the conceptual model. The emergent Capacity–Motivation–Opportunity structure was aligned with evidence-based determinants of adherence, theories of treatment burden, and patient-experience outcome (PROMs and PREMs). In addition, preference-sensitive care frameworks, hybrid care and telepharmacy models, and organisational workflows in outpatient pharmacy services were incorporated. Constructs were mapped to each domain and cross-referenced with theoretical frameworks using analytic matrices. We refined the boundaries of each domain and identified the core behavioural and experiential mechanisms influencing adherence. The synthesis produced a multidimensional conceptual architecture linking C–M–O determinants with operational needs of outpatient PC.
In Stage 5, the conceptual architecture was operationally translated into PC workflows to ensure ecological validity. This process was informed by task analysis of routine outpatient pharmacy practices and focused on mapping Capacity–Motivation–Opportunity determinants to key clinical and organisational components. These included: (i) assessment indicators and structured interview elements; (ii) triage criteria and decision nodes; (iii) a three-level complexity-based stratification system (Level 1 = higher complexity; Level 3 = lower complexity); (iv) domain-specific intervention families; (v) follow-up intensity rules and integration of telepharmacy modalities; and (vi) PROM/PREM-guided monitoring and criteria for dynamic re-stratification.
This step produced the operational backbone of CMO–MAPEX, allowing pharmacists to identify dominant limiting factors, personalise interventions and organise longitudinal hybrid follow-up (Table 2).
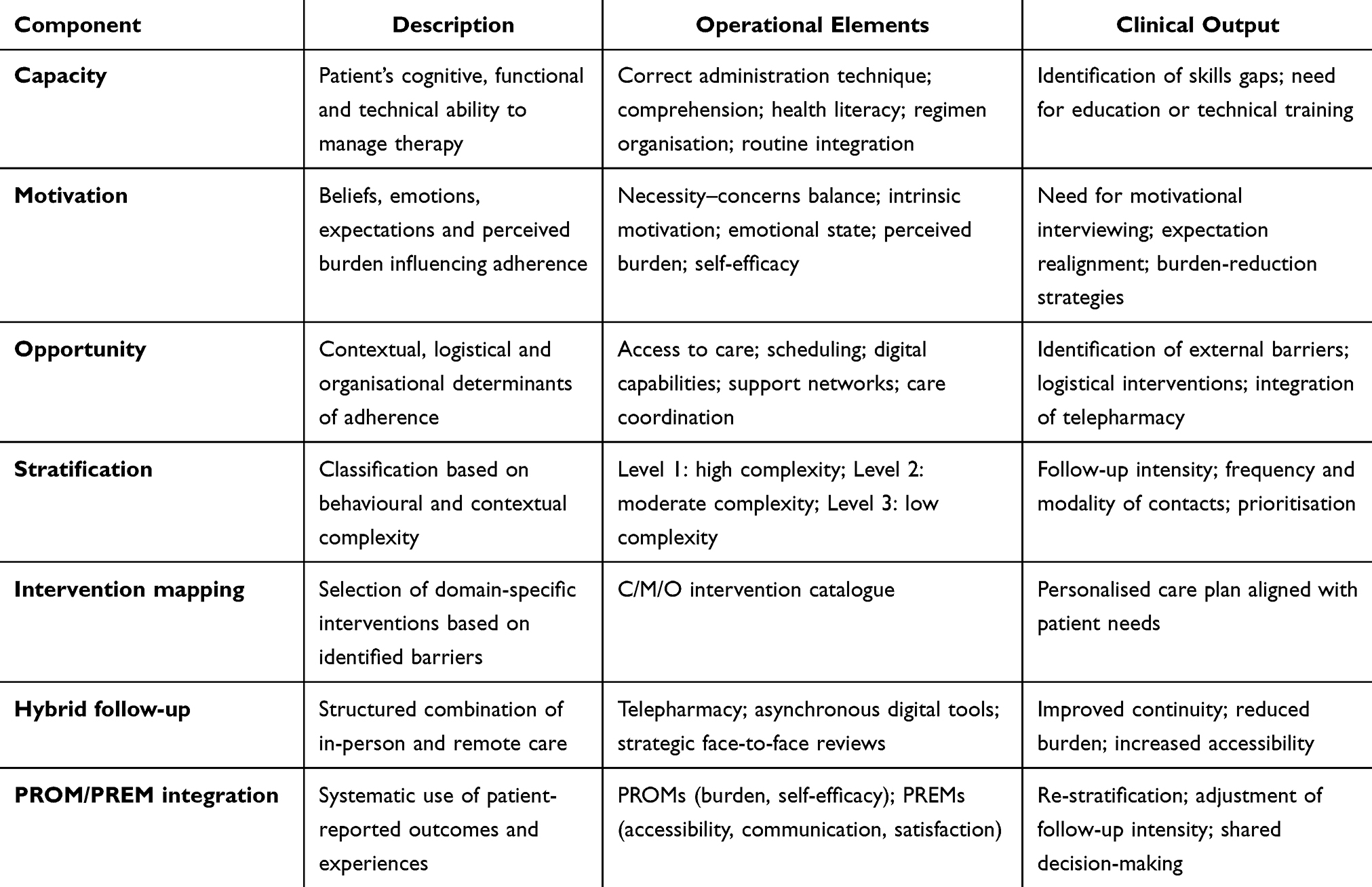 |
Table 2 CMO–MAPEX Model Architecture: Domains, Subdomains and Operational Components |
Finally, in Stage 6, expert review, refinement, and ecological validation were conducted. This stage consisted of an ecological validation process (refers to a structured expert-based appraisal process designed to evaluate conceptual clarity, coherence, feasibility, usability, and alignment with real-world outpatient pharmaceutical-care workflows) involving a multidisciplinary panel of experts. The panel included hospital pharmacists specialised in outpatient care, clinicians from chronic-care specialties, behavioural science researchers, and professionals experienced in PROM/PREM development.
Experts received a structured dossier summarising the emerging framework, including domain definitions, stratification logic, intervention mapping and workflow diagrams.
Feedback was collected through iterative rounds combining synchronous meetings and written annotations. Experts were asked to evaluate conceptual clarity, internal coherence, clinical feasibility, and alignment with patient-centred and hybrid care principles.
Comments were thematically analysed and used to refine definitions, streamline subdomains, adjust the stratification criteria and improve operational pathways.
Although not designed as a formal Delphi or RAND/UCLA process, this structured expert review provided ecological validity and ensured the model was usable and acceptable in routine outpatient PC.
Methodological rigour was addressed through triangulation of behavioural, experiential and organisational sources; independent data extraction followed by consensus procedures; explicit documentation of analytic decisions; and external expert review. The analytic process was further informed by alignment with routine outpatient pharmaceutical care workflows. All coding matrices, analytical steps and decision logs were maintained as part of an internal audit trail to support transparency and reproducibility. As no human participants, identifiable data or clinical interventions were involved, ethics approval was not required in accordance with international research guidelines.
Results
The multi-stage development process led to the formulation of CMO–MAPEX, a multidimensional and operational framework designed to structure medication-adherence support in outpatient PC. Rather than emerging from a single theoretical lineage, the model took shape through the gradual integration of behavioural evidence, experiential insights, and the practical realities of contemporary pharmacy services. The results of this process reflect both the conceptual refinement of the framework and its translation into an operational system designed for use in routine clinical practice.
The initial scoping phase produced a broad and heterogeneous set of determinants of adherence, illustrating the complexity of the behaviour it sought to capture. Constructs ranged from literacy, skills and cognitive abilities to emotional readiness, decisional conflict, logistical constraints, digital limitations and experiences of treatment burden. During iterative analysis, these determinants consistently gravitated toward three coherent clusters corresponding to Capacity, Motivation and Opportunity. The three domains demonstrated internal cohesion and external distinctiveness, with no relevant constructs remaining outside the triad. This provided a stable conceptual foundation on which to build (Table 1).
As refinement progressed, the relationship between these domains became more clearly defined. Capacity captured the cognitive, functional and organisational prerequisites for managing long-term therapy: understanding treatment goals, mastering administration techniques, integrating medication into daily routines, and navigating complex regimens. Motivation encompassed the psychological and emotional landscape that underpins adherence—beliefs about necessity and harm, ambivalence, confidence, readiness to change, and the broader experiential processes that shape how patients perceive their treatment. Opportunity consolidated the environmental and organisational conditions that can either enable or obstruct adherence, including access barriers, fragmentation of care, digital and logistical limitations, support networks and appointment burden.
Through successive rounds of synthesis, these domains were progressively linked to each other in ways that reflected real-world patterns of behaviour. For example, low literacy (Capacity) often magnified perceived burden (Motivation) and made patients more dependent on system-level facilitators (Opportunity). Conversely, strong motivation was frequently insufficient when access or logistical barriers remained unresolved. These interactions reinforced the need for a unified framework in which behavioural, experiential and contextual dimensions could be assessed together and addressed in an integrated manner. The key domains, constructs, and operational components of the framework are summarised in Table 2.
With this conceptual architecture established, attention turned to translating it into a practical system that pharmacists could apply consistently. This required moving from what shapes adherence to how these determinants should guide decisions in everyday practice. The three-level stratification system emerged naturally from this process (Table 3). Rather than classifying patients solely by diagnosis or clinical severity, it organises them according to the nature and intensity of their behavioural and contextual barriers. Patients with multiple concurrent limitations across Capacity, Motivation and Opportunity were assigned to Level 1, requiring close, often hybrid follow-up and targeted interventions. Those with a single predominant barrier were categorised as Level 2, while stable patients with limited complexity were placed in Level 3, with minimal follow-up needs. The system was designed to be dynamic: changes in PROM/PREM patterns, worsening of contextual challenges or signs of behavioural drift trigger reassessment and re-stratification. Through task analysis of outpatient workflows, the framework evolved into a structured pathway that links assessment, patient stratification, intervention planning (Table 4) and longitudinal monitoring.
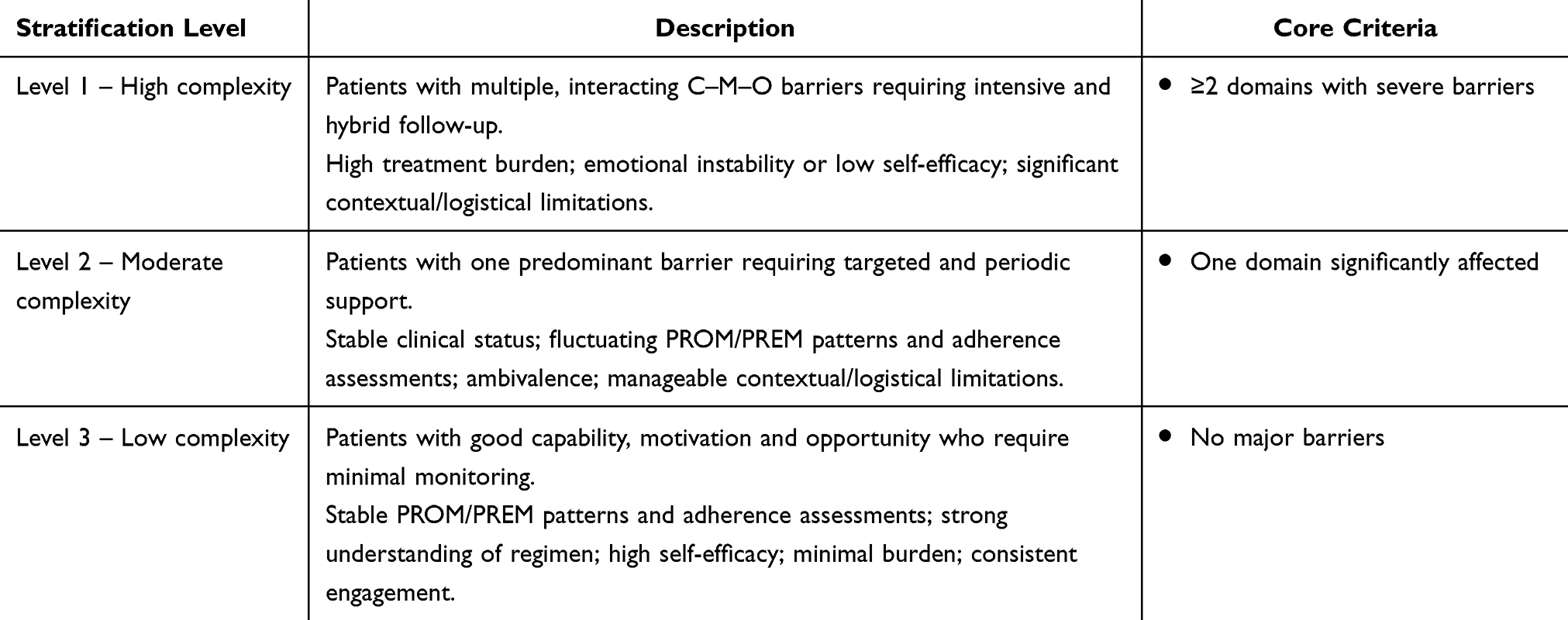 |
Table 3 CMO-Based Stratification System: Levels, Criteria and Clinical Indicators |
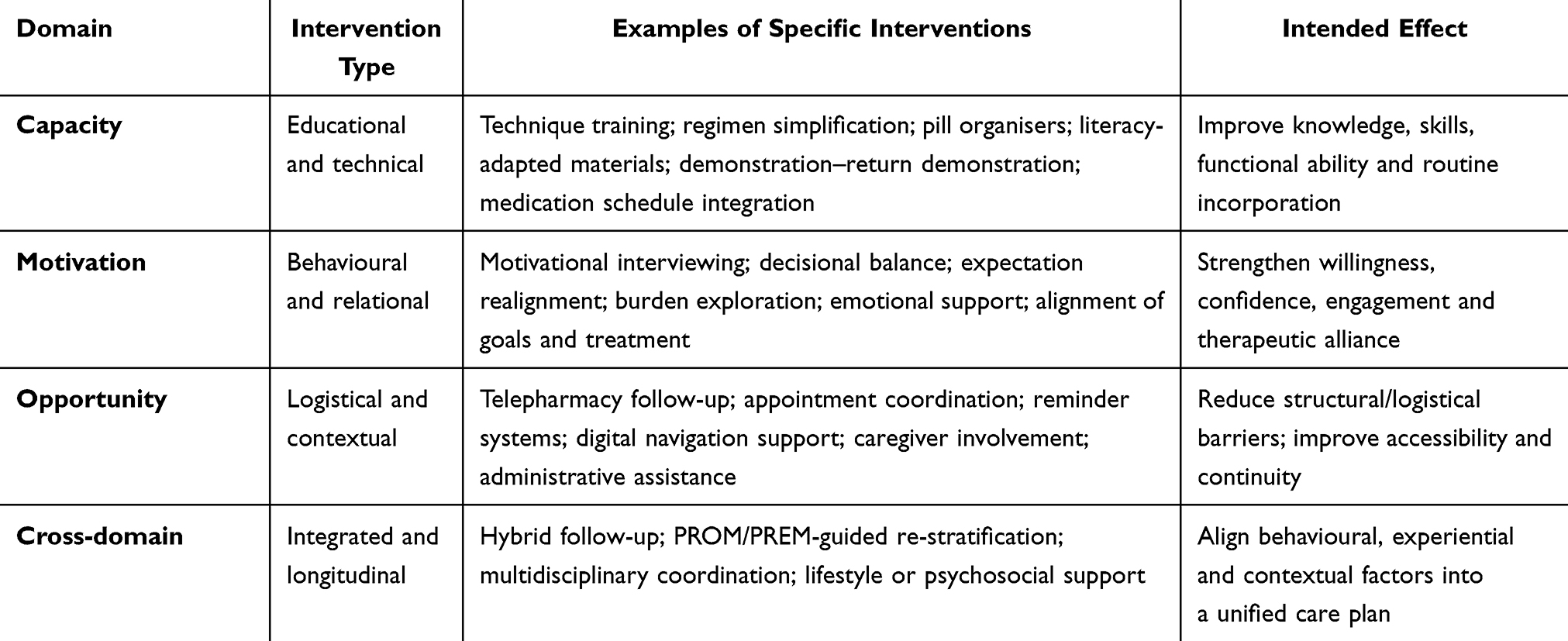 |
Table 4 CMO–MAPEX Intervention Catalogue: Targeted Actions by Domain |
A key outcome of the framework-development process was the integration of PROMs and PREMs as structural components of the model rather than as supplementary tools. Patient-reported outcomes and experiences were formally incorporated into assessment, monitoring and decision-making, recognizing that adherence is not only a behavioural act but also an experiential process. PROM/PREM data provided a way to capture burden, emotional impact, perceived difficulty and communication quality, enabling pharmacists to detect early deviations in adherence behavior and adjust follow-up accordingly. This element proved essential for ensuring alignment between the framework and preference-sensitive care (Table 5).
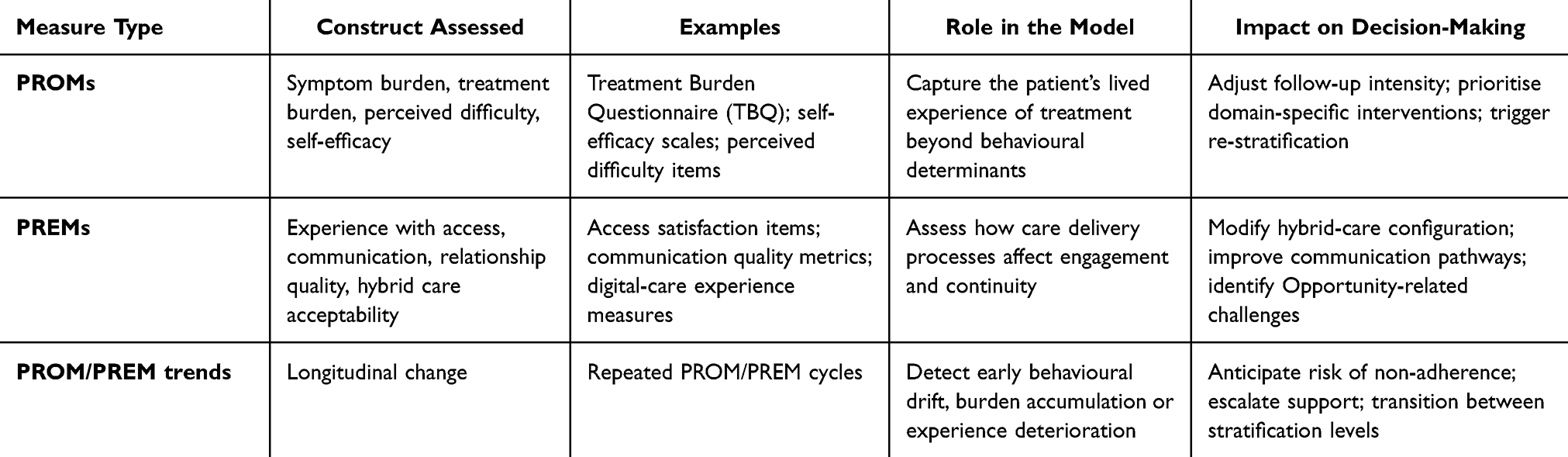 |
Table 5 Integration of PROMs and PREMs in the CMO–MAPEX Framework |
Finally, the operational model incorporated the realities of modern care delivery by embedding hybrid pathways. Telepharmacy, asynchronous communication tools, and remote monitoring were positioned alongside face-to-face contacts as routine components of longitudinal care. This allowed the framework to address logistical challenges within the Opportunity domain, accommodate patient preferences, and ensure continuity for those with mobility, work-related or access barriers.
Taken together, these results describe a framework with a coherent conceptual structure and clearly defined operational pathways for outpatient PC. CMO–MAPEX does not replicate existing models; rather, it offers a new, operationally grounded approach that integrates behavioural determinants, patient experience and modern hybrid care structures into a unified system for adherence support.
The final CMO–MAPEX framework comprises: (1) a three-domain architecture capturing Capacity, Motivation and Opportunity determinants; (2) a set of assessment indicators aligned with each domain; (3) a three-level complexity-based stratification system; (4) domain-specific intervention families; (5) a hybrid care pathway integrating in-person and remote follow-up; and (6) a PROM/PREM-guided monitoring cycle that supports continuous re-stratification. Together, these components form a reproducible and patient-centred structure designed to guide adherence support in real-world pharmacy practice (Tables 4 and 5). Figure 1 provides a visual overview of the integrated CMO–MAPEX workflow, whereas Table 6 details the sequential operational steps required for implementation in routine outpatient PC.
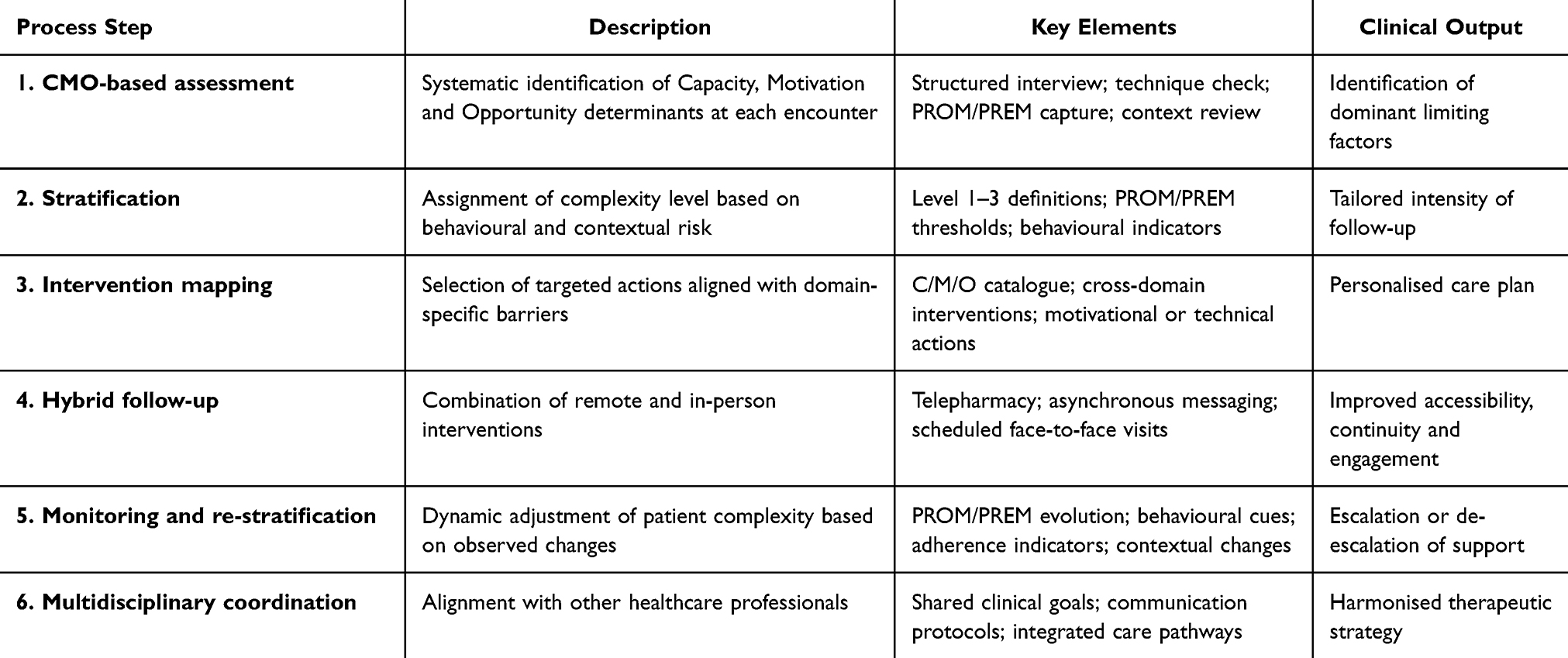 |
Table 6 Operational Workflow of the CMO–MAPEX Model |
 |
Figure 1 International Clinical Implementation Workflow of the CMO–MAPEX Model. The figure depicts the operational workflow of the CMO–MAPEX framework across five interconnected phases: (1) initial Capacity–Motivation–Opportunity assessment incorporating baseline PROM/PREM measures; (2) three-level complexity stratification; (3) domain-specific tailored intervention planning; (4) hybrid longitudinal follow-up combining in-person and remote care; and (5) dynamic re-stratification guided by changes in adherence, PROM/PREM trends, and clinical or contextual factors. |
Discussion
Addressing the persistent gap between behavioural theories of medication adherence and their translation into routine clinical practice, this study introduces the CMO–MAPEX framework, a multidimensional and operational model designed to support patient-centred, preference-sensitive adherence care in outpatient PC settings.
The primary value of this work lies in its ability to bridge a long-standing gap between behavioural theory and clinical implementation by offering a model that is not only conceptually sound but fully operational and aligned with the realities of contemporary pharmacy practice. Unlike most adherence frameworks—which describe determinants but leave unanswered the question of how healthcare professionals should act on them—CMO–MAPEX provides a structured, reproducible and scalable pathway for assessment, stratification, intervention planning and hybrid longitudinal follow-up. Recent qualitative evidence from outpatient pharmacy consultations in Spain confirms that CMO-based approaches are perceived as feasible, clinically meaningful and aligned with real-world workflow and patient priorities.31 Potential barriers to implementation should be acknowledged, including variability in organisational structures, workflow integration challenges, and differences in professional readiness across centres.
Time constraints and workload pressures represent additional real-world challenges. The CMO–MAPEX framework was designed to mitigate this limitation by supporting patient stratification, prioritisation of care, and alignment of intervention intensity with individual complexity. In addition, CMO–MAPEX explicitly incorporates patient preference as a core determinant of treatment engagement. By embedding PROMs and PREMs into the assessment and follow-up cycle, the framework captures how patients value different aspects of their therapy, the burden they perceive, and the level of support they prefer to receive. This preference-sensitive approach allows pharmacists to tailor interventions beyond clinical indicators alone, ensuring that follow-up intensity, mode of care and communication are aligned with what matters most to each patient. Because patient preference strongly predicts adherence behaviour, integrating it into routine decision-making reinforces the model’s capacity to promote sustained engagement and person-centred outcomes.
Emerging evidence from previous applications of CMO-based approaches in outpatient PC provides additional support for the conceptual logic of the model. Studies conducted in chronic heart failure demonstrate that structured pharmacist-led interventions significantly improve medication adherence and clinical engagement.32 Similar benefits have been reported in populations with multimorbidity, where pharmacist-led adherence interventions tailored to behavioural and contextual barriers show consistent improvements in treatment engagement.33 In older people living with HIV, the application of the CMO methodology has been associated with improvements in pharmacotherapy optimisation and patient support needs.34 Moreover, real-time, pharmacist-integrated alert systems have been shown to improve antiretroviral therapy optimisation and adherence in routine care, further reinforcing the relevance of structured, operational models for adherence management.35 Such consistency across diverse clinical contexts suggests that operationalising adherence determinants through structured workflows can yield meaningful benefits for patients managed in real-world outpatient settings.
Beyond its operational contribution, the framework also advances conceptual integration within adherence research.
A central achievement of this study is the articulation of a multidimensional architecture that integrates behavioural, experiential and contextual determinants without forcing artificial symmetry or borrowing incomplete elements from existing models. The inductive origin of the CMO structure—emerging from the intersection of behavioural evidence, experience-based literature and outpatient-pharmacy workflow analysis—confers a degree of ecological validity that existing frameworks often lack.
This grounding in clinical reality allows the model to directly address a limitation repeatedly noted in the adherence literature: the difficulty of translating theoretical constructs into actionable processes that improve patient engagement and continuity of care.
The ABC taxonomy provides definitional clarity but does not guide intervention planning. PROM/PREM-based initiatives emphasise the importance of experience, burden and satisfaction, but do not articulate how such data should influence decision-making. Telepharmacy and Hybrid care models—while increasingly studied and implemented—also require integration into behavioural and experiential frameworks to reach their full potential.36,37 Recent evidence confirms that digital tools and hybrid models are being incorporated into chronic disease management, offering opportunities to enhance accessibility, reduce logistical burden and support longitudinal engagement.38
CMO–MAPEX extends this literature by offering a unified model that traverses these boundaries. It captures the behavioural logic, the subjective experience and the organisational structure required to operationalise adherence support. In doing so, it aligns closely with international calls for patient-centred, preference-sensitive models of care, particularly within chronic therapies where medication-taking behaviour is deeply intertwined with daily life, identity, emotional state and the capacity to navigate the healthcare system.
This coherence between theory, experience and practice constitutes a central feature of the framework.
Another key contribution of this work is the development of a stratification system grounded not in diagnosis or clinical severity, but in the interplay of behavioural and contextual determinants. Classifying patients by the complexity and nature of their barriers—rather than by disease label—enables a more rational allocation of clinical effort and resources. This is consistent with emerging value-based healthcare models and resonates with implementation-science literature emphasising the need for differentiated care pathways that adapt to patient complexity, preferences and evolving circumstances. The integration of PROMs and PREMs into this structure further supports preference-sensitive decision-making, ensuring that the patient’s experience, goals and burden are not peripheral considerations but central drivers of care. Evidence from coordinated telematic PC models demonstrates that hybrid structures can meaningfully improve patient experience, accessibility and continuity.39
Despite these strengths, several limitations merit attention. First, CMO–MAPEX remains a conceptual model whose components require empirical validation. Its stratification system has not yet been formally evaluated for predictive validity, reliability or sensitivity to change. Although expert consultation enriched the model, the process did not follow a formal Delphi or RAND/UCLA methodology, and future refinements will benefit from structured consensus procedures and the inclusion of patients and caregivers. The digital aspects of the model may also face implementation barriers in settings with limited technological infrastructure or reduced digital literacy, which could constrain Opportunity-focused interventions. Finally, while the model is theoretically adaptable across therapeutic areas, empirical validation is required to determine how condition-specific nuances should be incorporated. Preliminary evidence suggests that structured CMO-based approaches can enhance primary adherence to concomitant medication in people living with HIV.40 However, further studies are needed to confirm these findings across diverse patient populations.
The framework has relevant implications for clinical practice, particularly in supporting structured, preference-sensitive medication-adherence care in outpatient pharmacy settings. This supports more consistent, equitable and efficient use of resources, reducing unwarranted variability in care delivery. Incorporating PROM/PREM data enhances shared decision-making and strengthens the therapeutic alliance, which has been shown to be a determinant of long-term engagement. For health systems, the model offers a coherent structure for designing scalable, high-quality adherence programmes and aligns with policy directions focused on digital transformation, integrated care and patient experience.
Future research should focus on validating the operational components of the framework through prospective studies, including evaluation of stratification performance, assessment of intervention fidelity and examination of clinical and experiential outcomes. Comparative-effectiveness trials could quantify the added value of CMO-guided care relative to traditional approaches. Implementation-science frameworks will be essential for assessing feasibility, acceptability, sustainability and contextual determinants of adoption. Further work should explore how PROM/PREM-driven decision-making modifies adherence trajectories and how emerging digital tools, AI-supported classification systems and remote-monitoring strategies can strengthen the Opportunity domain.
The CMO–MAPEX framework provides a practical structure for supporting medication adherence in outpatient PC by aligning interventions with patient preferences, lived experience and behavioural needs. By systematically identifying Capacity, Motivation and Opportunity barriers, the model enables pharmacists to target the drivers of non-adherence rather than relying on generic education or reminder strategies. The integration of PROMs and PREMs allows clinicians to monitor treatment burden, emotional readiness and patient experience over time, making follow-up more personalised and responsive. The inclusion of hybrid care pathways improves accessibility, reduces treatment-related workload and supports continuity for patients with chronic conditions. Overall, CMO–MAPEX offers a reproducible and scalable approach that strengthens patient engagement, supports shared decision-making and facilitates consistent, preference-sensitive PC across diverse therapeutic areas.
Conclusion
In conclusion, CMO–MAPEX offers a rigorous, multidimensional and operational model that advances the field of medication adherence by integrating behavioural theory, patient experience and hybrid care innovation within the real constraints and possibilities of outpatient PC. By providing a structured pathway for personalised and preference-sensitive intervention, the framework lays the foundation for a new generation of adherence programmes capable of improving outcomes, enhancing patient experience and supporting the evolving role of pharmacists in modern health systems. Future dissemination strategies include integration into outpatient pharmaceutical-care programmes, incorporation into digital clinical tools, and alignment with professional training and quality frameworks.
Acknowledgments
The authors would like to thank all professionals participating in the MAPEX–SEFH initiative, including pharmacists and multidisciplinary collaborators, for their active involvement and sustained contribution to the development, refinement and dissemination of the CMO-MAPEX model.
Author Contributions
RMV was responsible for drafting the original manuscript. The remaining authors reviewed and contributed to the text. All authors made a significant contribution to the work reported, whether in the conception, study design, execution, data acquisition, analysis and interpretation, or all these areas. They all participated in drafting, revising, or critically reviewing the article, approved the final version to be published, have agreed on the journal to which the article has been submitted, and agree to be accountable for all aspects of the work.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Kengne AP, Brière JB, Zhu L, et al. Impact of poor medication adherence on clinical outcomes and health resource utilization in patients with hypertension and/or dyslipidemia: systematic review. Expert Rev Pharmacoecon Outcomes Res. 2024;24(1):143–13. doi:10.1080/14737167.2023.2266135
2. Iuga AO, McGuire MJ. Adherence and health care costs. Risk Manag Healthc Policy. 2014;7:35–44. doi:10.2147/RMHP.S19801
3. Bosworth HB, Granger BB, Mendys P, et al. Medication adherence: a call for action. Am Heart J. 2011;162(3):412–424. doi:10.1016/j.ahj.2011.06.007
4. Chauke GD, Nakwafila O, Chibi B, Sartorius B, Mashamba-Thompson T. Factors influencing poor medication adherence amongst patients with chronic disease in low-and-middle-income countries: a systematic scoping review. Heliyon. 2022;8(6):e09716. doi:10.1016/j.heliyon.2022.e09716
5. Nieuwlaat R, Wilczynski N, Navarro T, et al. Interventions for enhancing medication adherence. Cochrane Database Syst Rev. 2014;2014(11):CD000011. doi:10.1002/14651858.CD000011.pub4
6. Horne R, Chapman SC, Parham R, Freemantle N, Forbes A, Cooper V. Understanding patients’ adherence-related beliefs about medicines prescribed for long-term conditions: a meta-analytic review of the Necessity-Concerns Framework. PLoS One. 2013;8(12):e80633. doi:10.1371/journal.pone.0080633
7. Vrijens B, De Geest S, Hughes DA, et al; ABC Project Team. A new taxonomy for describing and defining adherence to medications. Br J Clin Pharmacol. 2012;73(5):691–705. doi:10.1111/j.1365-2125.2012.04167.x
8. Tran VT, Barnes C, Montori VM, Falissard B, Ravaud P. Taxonomy of the burden of treatment: a multi-country web-based qualitative study of patients with chronic conditions. BMC Med. 2015;13(1):115. doi:10.1186/s12916-015-0356-x
9. Baldoni S, Amenta F, Ricci G. Telepharmacy services: present status and future perspectives: a review. Medicina. 2019;55(7):327. doi:10.3390/medicina55070327
10. Mercadal-Orfila G, Herrera-Pérez S, Piqué N, et al. Implementing systematic patient-reported measures for chronic conditions through the Naveta value-based telemedicine initiative: observational retrospective multicenter study. JMIR mHealth uHealth. 2024;12:e56196. doi:10.2196/56196
11. Zolnierek KB, Dimatteo MR. Physician communication and patient adherence to treatment: a meta-analysis. Med Care. 2009;47(8):826–834. doi:10.1097/MLR.0b013e31819a5acc
12. Ho PM, Bryson CL, Rumsfeld JS. Medication adherence: its importance in cardiovascular outcomes. Circulation. 2009;119(23):3028–3035. doi:10.1161/CIRCULATIONAHA.108.768986
13. Morillo-Verdugo R, Calleja-Hernández MÁ, Robustillo-Cortés MLA, Poveda-Andrés JL. A new definition and refocus of pharmaceutical care: the Barbate Document. Farm Hosp. 2020;44(4):158–162. English. doi:10.7399/fh.11389
14. Michie S, van Stralen MM, West R. The behaviour change wheel: a new method for characterising and designing behaviour change interventions. Implement Sci. 2011;6(1):42. doi:10.1186/1748-5908-6-42
15. Greenhalgh J, Gooding K, Gibbons E, et al. How do patient reported outcome measures (PROMs) support clinician-patient communication and patient care? A realist synthesis. J Patient Rep Outcomes. 2018;2(1):42. doi:10.1186/s41687-018-0061-6
16. Black N. Patient reported outcome measures could help transform healthcare. BMJ. 2013;346(1):f167. doi:10.1136/bmj.f167
17. Weldring T, Smith SM. Patient-Reported Outcomes (PROs) and Patient-Reported Outcome Measures (PROMs). Health Serv Insights. 2013;6:61–68. doi:10.4137/HSI.S11093
18. Beattie M, Murphy DJ, Atherton I, Lauder W. Instruments to measure patient experience of healthcare quality in hospitals: a systematic review. Syst Rev. 2015;4(1):97. doi:10.1186/s13643-015-0089-0
19. Rutledge CM, Kott K, Schweickert PA, Poston R, Fowler C, Haney TS. Telehealth and eHealth in nurse practitioner training: current perspectives. Adv Med Educ Pract. 2017;8:399–409. doi:10.2147/AMEP.S116071
20. Alexander E, Butler CD, Darr A, et al. ASHP statement on telepharmacy. Am J Health Syst Pharm. 2017;74(9):e236–e241. doi:10.2146/ajhp170039
21. Morillo-Verdugo R, Romero-Murillo M, Solis-Martin C, Robustillo-Cortes MLA, Contreras-Macias E. Stratification tools in pharmaceutical care using the capacity-motivation-opportunity framework: a scoping review. Res Social Adm Pharm. 2025;21(10):743–752. doi:10.1016/j.sapharm.2025.05.009
22. Morillo Verdugo R, Calvin Lamas M, Delgado Latorre ATJ, et al. Development of the Q-PEX standard for quality certification of pharmaceutical care for outpatients of Pharmacy services. J Healthc Qual Res. 2021;36(6):324–332. Spanish. doi:10.1016/j.jhqr.2021.03.010
23. Nkansah N, Mostovetsky O, Yu C, et al. Effect of outpatient pharmacists’ non-dispensing roles on patient outcomes and prescribing patterns. Cochrane Database Syst Rev. 2010;2010(7):CD000336. doi:10.1002/14651858.CD000336.pub2
24. Hatah E, Braund R, Duffull SB, Tordoff J. General practitioners’ views of pharmacists’ current and potential contributions to medication review and prescribing in New Zealand. J Prim Health Care. 2013;5(3):223–233. doi:10.1071/HC13223
25. Nilsen P. Making sense of implementation theories, models and frameworks. Implement Sci. 2015;10(1):53. PMID: 25895742. doi:10.1186/s13012-015-0242-0
26. Damschroder LJ, Aron DC, Keith RE, Kirsh SR, Alexander JA, Lowery JC. Fostering implementation of health services research findings into practice: a consolidated framework for advancing implementation science. Implement Sci. 2009;4(1):50. doi:10.1186/1748-5908-4-50
27. Jabareen Y. Building a conceptual framework: philosophy, definitions, and procedure. Int J Qual Methods. 2009;8(4):49–62. doi:10.1177/160940690900800406
28. Mays N, Pope C, Popay J. Systematically reviewing qualitative and quantitative evidence to inform management and policy-making in the health field. J Health Serv Res Policy. 2005;10(Suppl 1):6–20. doi:10.1258/1355819054308576
29. Gale NK, Heath G, Cameron E, Rashid S, Redwood S. Using the framework method for the analysis of qualitative data in multi-disciplinary health research. BMC Med Res Methodol. 2013;13(1):117. doi:10.1186/1471-2288-13-117
30. Tong A, Sainsbury P, Craig J. Consolidated criteria for reporting qualitative research (COREQ): a 32-item checklist for interviews and focus groups. Int J Qual Health Care. 2007;19(6):349–357. doi:10.1093/intqhc/mzm042
31. Álvarez-Díaz AM, Crespo Diz C, Monte Boquet E, et al. Qualitative study on the adoption and enhancement of the capacity-motivation-opportunity model for pharmaceutical care in outpatient pharmacy consultations in Spain. Farm Hosp. 2025;49(6):T384–T391. English, Spanish. doi:10.1016/j.farma.2025.05.002
32. Wang L, Zhao Y, Han L, et al. Pharmacist-led management model and medication adherence among patients with chronic heart failure: a randomized clinical trial. JAMA Network Open. 2024;7(12):e2453976. Erratum in: JAMA Netw Open. 2025;8(4):e2511780. doi:10.1001/jamanetworkopen.2024.53976
33. Sholihah S, Rahayu FP, Farhana L, Alshehri S, Alfian SD, Abdulah R. Pharmacist-led interventions to improve medication adherence among patients with multimorbidity: a scoping review. Patient Prefer Adherence. 2025;19:3589–3602. doi:10.2147/PPA.S542881
34. Sánchez-Yáñez E, Huertas-Fernández MJ, Robustillo-Cortes MA, et al. Application of CMO (capacity, motivation, and opportunity) methodology in pharmaceutical care to optimize the pharmacotherapy in older people living with HIV. DISPIMDINAC project. Rev Esp Quimioter. 2023;36(6):584–591. doi:10.37201/req/021.2023
35. Morillo-Verdugo R, Solis-Martin C, Marquez-Saavedra E, Robustillo-Cortes MLA, Romero Gil E, Contreras-Macias E. Implementation and evaluation of a real-time prescription alert system to optimize antiretroviral therapy and medication adherence in people living with HIV. SANPAT PROJECT. Patient Prefer Adherence. 2025;19:3493–3508. doi:10.2147/PPA.S549933
36. Peyroteo M, Ferreira IA, Elvas LB, Ferreira JC, Lapão LV. Remote monitoring systems for patients with chronic diseases in primary health care: systematic review. JMIR mHealth uHealth. 2021;9(12):e28285. doi:10.2196/28285
37. Lewinski AA, Walsh C, Rushton S, et al. Telehealth for the longitudinal management of chronic conditions: systematic review. J Med Internet Res. 2022;24(8):e37100. doi:10.2196/37100
38. Pong C, Tseng RMWW, Tham YC, Lum E. Current implementation of digital health in chronic disease management: scoping review. J Med Internet Res. 2024;26:e53576. doi:10.2196/53576
39. Morillo-Verdugo R, Morillo-Lisa R, Espolita-Suarez J, Delgado-Sanchez O. Evaluation of patient experience with a model of coordinated telematic pharmaceutical care between hospital and rural pharmacies in Spain: a proof of concept. J Multidiscip Healthc. 2023;16:1037–1046. doi:10.2147/JMDH.S406636
40. Morillo-Verdugo R, Vélez-Díaz-Pallarés M, Fernández-Pacheco García-Valdecasas M, Fernández-Espínola S, Sánchez-Rubio Ferrández J, Navarro-Ruiz A. Application of the CMO methodology to the improvement of primary adherence to concomitant medication in people living with-HIV. The PRICMO Project. Farm Hosp. 2021;45(5):247–252. English.
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.