Back to Journals » International Journal of Women's Health » Volume 17
A Multicenter Retrospective Cohort Study of Pregnancy Outcomes in Idiopathic Oligohydramnios at Term
Authors Gao H, Tao H, Zou L, Luo QQ, Zhang WY
Received 26 November 2024
Accepted for publication 17 May 2025
Published 5 June 2025 Volume 2025:17 Pages 1665—1672
DOI https://doi.org/10.2147/IJWH.S508609
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Marleen van Gelder
Hui Gao,1 Hui Tao,1 Li Zou,1 Qing-Qing Luo,1,2 Wei-Yuan Zhang3
1Department of Obstetrics and Gynecology, Union Hospital, Tongji Medical College, Huazhong University of Science and Technology, Wuhan, People’s Republic of China; 2Department of Obstetrics and Gynecology, Peking University International Hospital, Beijing, People’s Republic of China; 3Department of Obstetrics, Beijing Obstetrics and Gynecology Hospital, Capital Medical University, Beijing, People’s Republic of China
Correspondence: Hui Tao; Li Zou, Department of Obstetrics and Gynecology, Union Hospital, Tongji Medical College, Huazhong University of Science and Technology, No. 1277 Jiefang Avenue, Wuhan, 430022, People’s Republic of China, Email [email protected]; [email protected]
Objective: The effect of idiopathic oligohydramnios or isolated oligohydramnios on perinatal outcomes at term pregnancies is understudied. This study aimed to show the current epidemiological status of idiopathic oligohydramnios in mainland China, evaluate the pregnancy outcomes, and discuss the optimal delivery opportunity and mode.
Methods: We conducted a retrospective cohort study of 106,225 term pregnancies from 37 hospitals in mainland China. All cases that delivered a non-anomalous singleton fetus between 37+0 and 41+6 weeks were collected. Perinatal outcomes of different gestational weeks and different delivery modes were compared between the idiopathic oligohydramnios group and the control group.
Results: The incidence of idiopathic oligohydramnios in singleton pregnancies at term was 2.6%. Compared with control pregnancies, the idiopathic oligohydramnios group was characterized by lower birth weights and higher cesarean section rates (P < 0.01, respectively). From early-term and full-term to late-term, a pregnancy with idiopathic oligohydramnios exhibited the trend of lower risk of cesarean delivery and neonatal intensive care unit (NICU) admission but a higher risk of meconium-stained amniotic fluid, non-reassuring fetal heart rate status (NRFHRS), and emergency cesarean delivery (P < 0.01, respectively). Notably, the rate of Apgar score < 7 at 5 min and cesarean section was the lowest when delivery occurred during the 39+0 to 40+6 weeks. There was a higher incidence of NRFHRS in the idiopathic oligohydramnios vaginal delivery group when compared to the selective cesarean section group (2.6% vs 1.2%, P=0.05), but with no significant differences in postpartum hemorrhage, low Apgar score, or NICU admission.
Conclusion: The incidence of adverse pregnancy outcomes is higher in the idiopathic oligohydramnios group than in the control group. Adverse outcomes seem lowest in the group of vaginal delivery during the 39+0 to 40+6 weeks, but close intrapartum surveillance and active intervention still need to be applied.
Keywords: idiopathic oligohydramnios, term pregnancy, pregnancy outcome, delivery mode, delivery opportunity
Introduction
Oligohydramnios, recognized as a reduction of amniotic fluid volume, is one of the most common pregnancy complications occurring in the third trimester.1 Oligohydramnios can be caused by fetal abnormalities, preeclampsia, preterm rupture of membrane (PROM), or other maternal or fetal diseases.2 However, in some cases of oligohydramnios, the causes remain unknown, and therefore, are referred to as idiopathic oligohydramnios or isolated oligohydramnios (IO). The reported incidence of IO ranges from 0.5% to 5%, varying according to diagnostic criteria and study populations.3
New definitions of term pregnancy were confirmed and have been endorsed by the American College of Obstetricians and Gynecologists (ACOG) in 2013 and reaffirmed in 2017, and it categorized terms based on the gestational length:4 early term is defined as deliveries between 37 weeks and 0 days through 38 weeks and 6 days; full term is defined as deliveries between 39 weeks and 0 days through 40 weeks and 6 days; late term is defined as deliveries between 41 weeks and 0 days through 41 weeks and 6 days.
Recent studies have shown that IO does not significantly impact perinatal outcomes, although it is associated with higher obstetric intervention.5 Moreover, there is no consensus regarding the optimal management and time of delivery.6 To identify those clinical issues, studies with large sample sizes are essential. Therefore, our study aimed to evaluate the perinatal outcomes of IO during different periods of term pregnancy and determine the optimal timing and delivery mode.
Materials and Methods
Our data were extracted from a large epidemiological survey performed in mainland China. All cases of delivery between 37+0 and 41+6 weeks from January to December 2011 were collected from 37 hospitals in 14 provinces and municipalities in China. Retrospective reviews of the clinical data, including maternal medical history, pregnancy comorbidities and complications, exam results, delivery mode, and pregnancy outcomes were abstracted from the databases by two trained research assistants. To ensure data accuracy, 10% of the records were randomly re-evaluated by a senior investigator. Discrepancies were resolved through consensus discussions.
Oligohydramnios was diagnosed when the amniotic fluid index (AFI) was ≤5 cm or the largest vertical pocket measured ≤2 cm, as detected by ultrasound.7,8 All ultrasound assessments were conducted by certified sonographers. At least two scans were performed before the diagnosis was confirmed. IO referred to the presence of oligohydramnios without structural abnormalities of the fetus, without fetal growth restriction, without intrauterine infection, and in the absence of known maternal diseases. The control group consisted of singleton pregnancies without any complications. Adverse pregnancy outcomes included: low birth weight (<2500 g), macrosomia (birth weight≥4000 g), perinatal death, cesarean section delivery, emergency cesarean section delivery, postpartum hemorrhage, meconium-stained amniotic fluid, non-reassuring fetal heart rate status (NRFHRS), low Apgar score at 1 min and 5 min, and NICU admission. NRFHRS was diagnosed when one or more of the following situations (tachycardia or bradycardia for more than 10 minutes, reduced FHR variability, decelerations, and absence of accelerations) occurred in the intrapartum period.
Using the new definition of “term pregnancy”, term cases with idiopathic oligohydramnios in our study were stratified into three groups: early-term (37+0–38+6 weeks), full-term (39+0–40+6 weeks), and late-term (41+0–41+6 weeks).
Statistical analyses were conducted with SPSS 21.0 (IBM Corp., Armonk, NY, USA). Continuous variables were shown as the mean ± standard deviation, and variables were compared using Student’s t-test. The chi-square test or Fisher’s exact test was used for categorical data analysis. We defined P<0.05 as statistically significant.
Results
There were 4097 (3.9%) pregnant women diagnosed with oligohydramnios, of which 2720 (59.1%) were diagnosed with IO. The control group consisted of 67,622 in 106,225 term deliveries, which were recognized as normal singleton pregnancies. The incidence of IO in term singleton pregnancy was 2720/106,225 (2.6%) (Figure 1). The demographic characteristics of study groups were presented in Table 1. The gestational age at delivery in the IO group and control group was both 39.3±1.1 weeks (P>0.05). The average birth weight of neonates in the IO and control groups was 3200.8 ± 448.8 g and 3352.2 ± 422.2 g, respectively (P <0.01). The average maternal age in the IO group was younger than that in the control group (27.7 ± 4.3 y vs 27.9 ± 4.6 y, P<0.01). And the portion of women with short stature, primigravidity, nulliparity, or history of adverse pregnancy in the IO group is significantly higher than that of the control group.
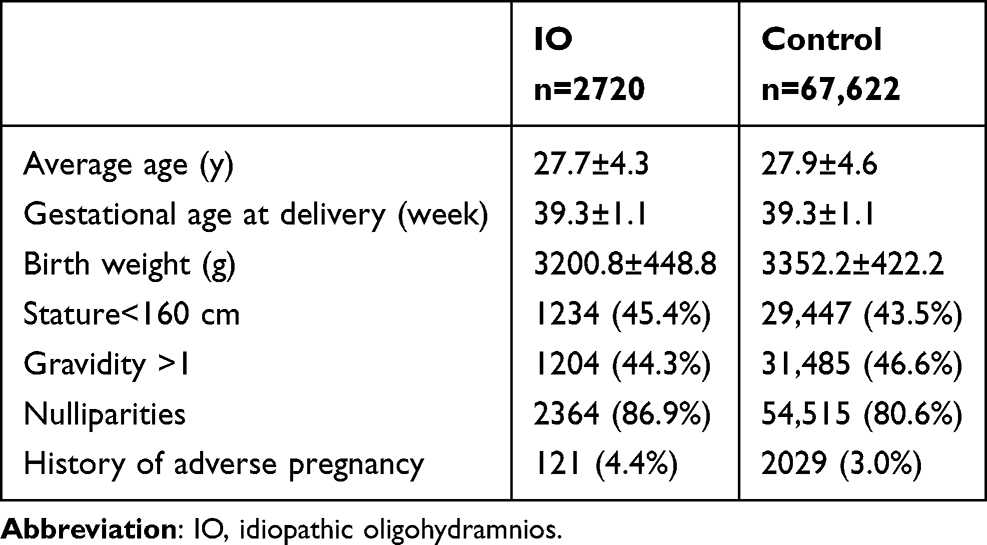 |
Table 1 Characteristics of Patients |
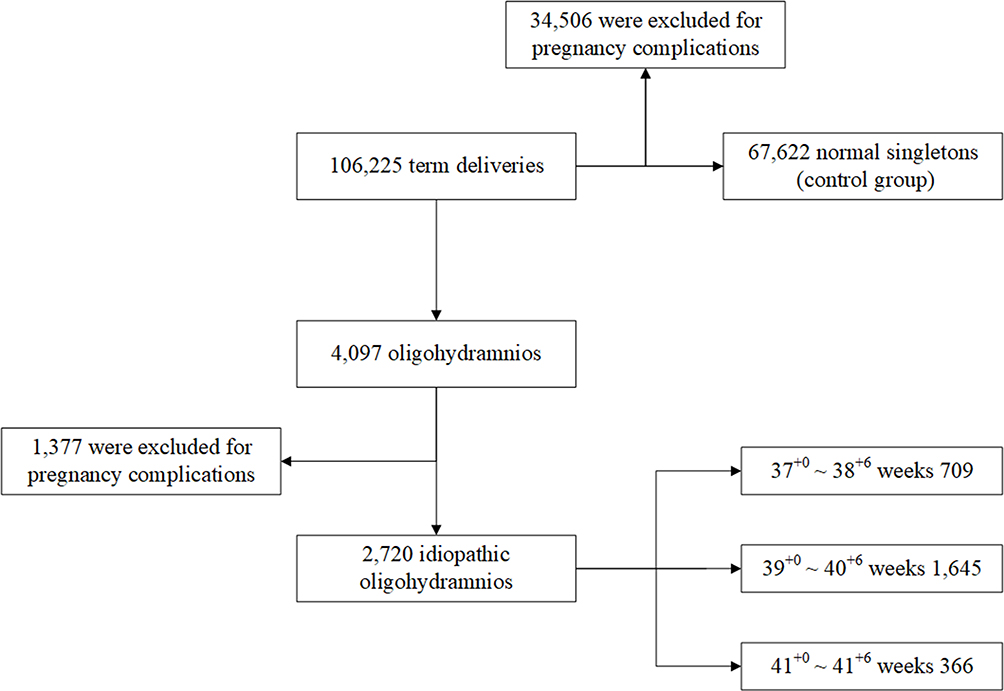 |
Figure 1 Flowchart of grouping idiopathic oligohydramnios at term. |
Pregnancy outcomes in the IO and control group were shown in Table 2. The rate of low birth weight in the IO group was significantly higher than that in the control group (5.7% vs 2.1%, P<0.01), while the rate of macrosomia in the control group was higher than that in the IO group (7.2% vs 4.7%, P <0.01). The incidence of meconium-stained amniotic fluid was higher in the IO group as compared to the control group (10.7% vs 6.4%, P<0.01). NRFHRS were more prevalent in the IO group when compared to the control group (2.3% vs 1.1%, P<0.01). Additionally, there was a higher rate of cesarean section and emergency cesarean section in the IO group than in the normal group (84.5% vs 53.9%, 33.9% vs 14.7%, P <0.01 for both), respectively. There was no statistical difference between the IO and control group regarding a low Apgar score at 1 min, but the incidence of low Apgar score at 5 min and NICU admission were significantly higher in the IO group (0.5% vs 0.3%, 0.6% vs 0.3%, P <0.05 for both), respectively. Perinatal death and postpartum hemorrhage were not statistically different between the two groups (0.1% vs 0.1%, 2.6% vs 3.1%, P >0.05 for both).
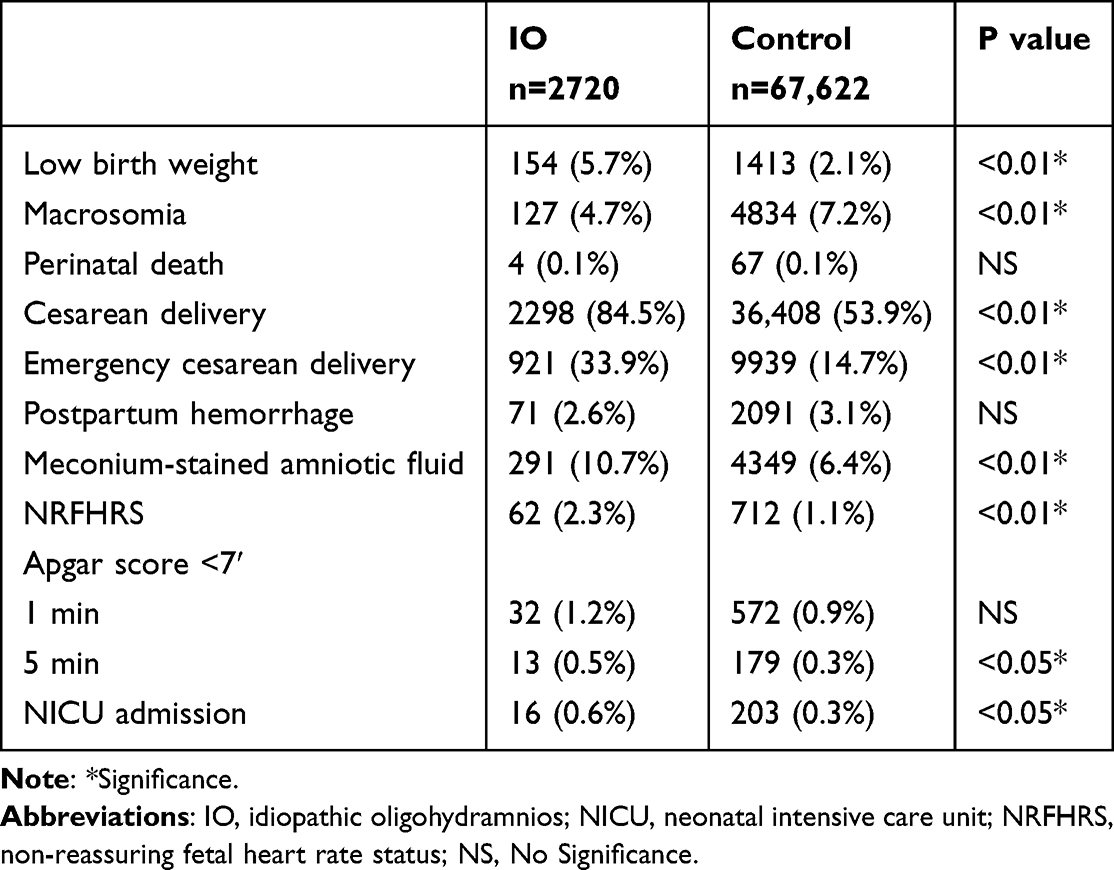 |
Table 2 Pregnancy Outcomes in Idiopathic Oligohydramnios and Normal Pregnancy Group |
Furthermore, given that multiple confounding factors may influence pregnancy outcomes, such as maternal age, gravidity, parity, history of adverse pregnancy, maternal stature, and gestational age at delivery, we performed multiple regression analysis. The result was presented in Table 3, which confirmed that IO is an independent risk factor for adverse pregnancy outcomes with the largest regression coefficient. Here, we defined adverse pregnancy outcomes as the occurrence of one or more of the aforementioned outcome measures (excluding cesarean section).
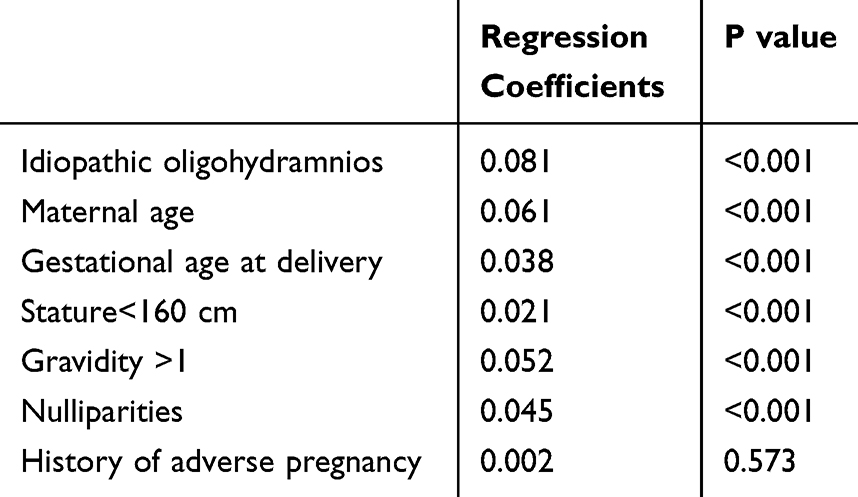 |
Table 3 Multiple Regression Analysis of Factors Influencing Pregnancy Outcomes |
Applying the new definitions of “term pregnancy”, pregnancy outcomes at different gestational ages in IO were illustrated in Table 4. The incidence of low-birth-weight neonates decreased but macrosomia increased with increasing gestational age (12.0% vs 3.7% vs 2.8%, P<0.01; 1.6% vs 5.0% vs 9.4%, P <0.01), respectively. There was a decreasing trend in cesarean section rate with increasing gestational age (88.9% vs 82.9% vs 82.3%, P<0.01), while the emergency cesarean section rate increased (30.9% vs 33.9% vs 39.6%, P<0.01). Also, the risk of meconium-stained amniotic fluid and NRFHRS gradually increased with increasing gestational age in IO patients (3.9% vs 11.8% vs 18.9%, P<0.01; 1.3% vs 2.5% vs 3.3%, P<0.01 for all). There were no statistical differences in postpartum hemorrhage, low Apgar score, or NICU admission with increasing gestational age.
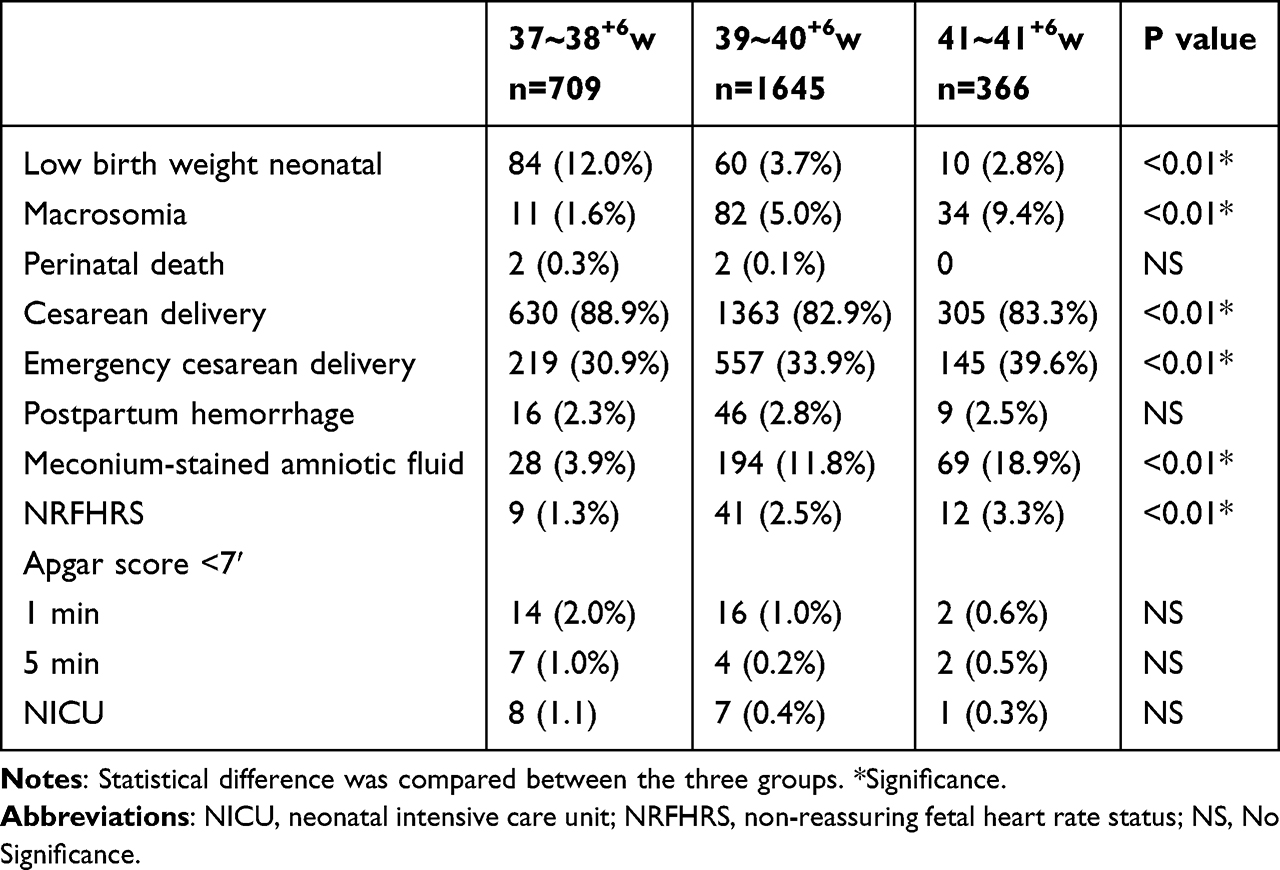 |
Table 4 Maternal and Perinatal Outcomes at Different Gestational weeks in Idiopathic Oligohydramnios at Term |
Pregnancy outcomes of IO patients according to delivery mode were compared in Table 5. There were 1378 elective cesarean deliveries and 422 vaginal deliveries among all term pregnancies with IO. Here, elective cesarean deliveries mean cesarean sections performed prior to the onset of labor, solely at the mother’s request, without any medical indication. This is considered a separate category of indication.9 Considering that abnormal birth weight is a conflicting factor of pregnancy outcomes, macrosomia and low birth weight cases were excluded in this analysis. Finally, perinatal outcomes of 1221 elective cesarean section deliveries and 378 vaginal deliveries with normal birth weight were assessed. There was no perinatal death case. The incidence of NRFHRS in the vaginal delivery group was higher than that in the cesarean section group (2.6% vs 1.2%, P=0.05). There were no significant differences in postpartum hemorrhage, low Apgar score, or NICU admission when the two groups were compared.
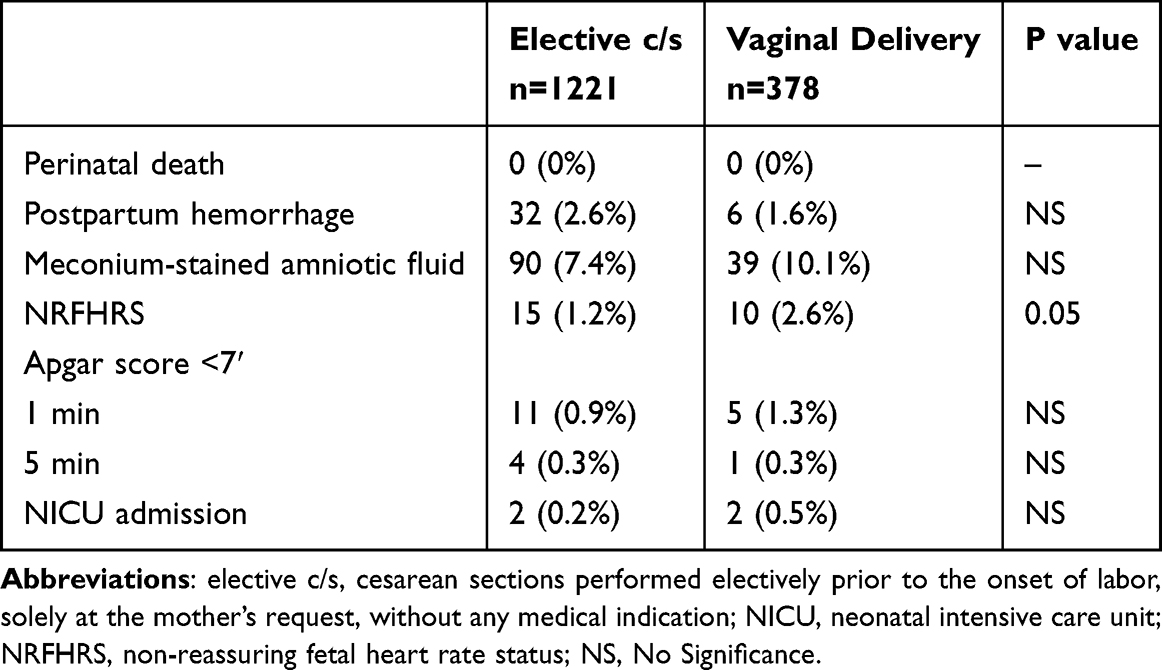 |
Table 5 Maternal and Perinatal Outcomes of Different Delivery Modes in Idiopathic Oligohydramnios at Term |
Discussion
Our multicenter study evaluated the association between IO and term pregnancy outcomes. The average maternal age in the IO group was younger than the normal group. We speculate that most of the older cases in the IO group were excluded since they are associated with a greater likelihood of pre-existing medical conditions or a higher risk of obstetric complications. Our study revealed that there was a higher cesarean section rate for term pregnancies with IO when compared with normal singleton pregnancies. Additionally, in the IO group, we found a significantly increased risk of adverse perinatal outcomes, such as meconium-stained amniotic fluid, NRFHRS, low Apgar score at 5 min, and NICU admission. There was no statistical difference between the two groups in terms of postpartum hemorrhage, perinatal death, and low Apgar scores at 1 min.
Tweed et al10 discovered a dose-response relationship between the Apgar score and overall additional support needs (ASN) status, therefore, concluded that Apgar scores are associated with both long-term and short-term prognoses, as well as with educational and clinical outcomes at the population level. Population-based cohort studies also showed that risks of cerebral palsy and epilepsy increased in children with low Apgar scores and a low Apgar score at 5 minutes conferred a higher risk when compared to a low Apgar score at 1 minute.11 Therefore, the increasing rate of the low Apgar score at 5 min in the IO group in our research may indicate more serious adverse effects on neonatal well-being of this group. One research team seems to have verified our study, which found a significant association between pregnancies complicated by IO and long-term neurological morbidity of the offspring;12 while controlling for confounders, IO was found to be independently associated with long-term cardiovascular morbidity of the offspring as well.13
IO is strongly associated with lower birth weight. Previous studies concluded that the low birth weight in pregnancies with IO might be attributed to iatrogenic preterm deliveries.14,15 However, the clear correlation still existed despite that all deliveries were term pregnancies in our study. This result is consistent with studies by Naveiro-Fuentes et al.15 In our study, a higher incidence of meconium-stained amniotic fluid and NRFHRS was found in the IO group, which may be due to placental perfusion insufficiency. This coincides with Hadas’s research, which demonstrated higher rates of placental maternal vascular malperfusion (MVM) lesions and worse neonatal outcomes in pregnancies complicated by IO, and suggested that IO should be seen as part of the “placental insufficiency” spectrum. Subsequently, these adverse neonatal manifestations may lead to a higher rate of emergency cesarean sections (or cesarean sections).16 Coincidentally, a meta-analysis by Chauhan et al17 also showed that patients with antepartum AFI≤5 cm were associated with an increased risk of cesarean delivery in response to NRFHRS.
Even though there is a reasonable deduction for the higher rate of cesarean sections in IO patients, conflicting conclusions remain. Ahmad et al studied 421 cases in Pakistan, and concluded that the increase in cesarean section rates in the IO group was secondary to a higher rate of labor induction rather than the increased risk of NRFHRS.18 Conway et al studied 183 labor induction cases complicated with IO at term, and found that in the IO group, there was a higher failure rate for labor induction compared with controls, which led to an increase in the cesarean section rate.19 Kansu-Celik also found that labor induction with dinoprostone in term pregnancies of IO was associated with an increased rate of cesarean sections, but there was no higher risk of perinatal complications.20 Nevertheless, according to systematic reviews and Meta-analyses, Shrem et al concluded that IO at term was associated with significantly higher rates of labor induction and cesarean sections, and higher short-term neonatal morbidity.21 These findings are consistent with our results. We also found a gradually increasing rate of meconium-stained amniotic fluid and NRFHRS with increasing gestational age, which indicates that timely obstetric intervention in IO patients at term is especially important.
In our study, there was no significant difference in low Apgar score at 1 and 5 min among the three term groups, but the rate of Apgar score <7 at 5 min was the lowest when delivery occurred during the 39+0 to 40+6 weeks. The lowest cesarean section rate of 39+0 to 40+6 weeks indicates a higher success rate in vaginal delivery or labor induction. These findings imply that induction of labor at 39+0 to 40+6 weeks is feasible, in both IO and non-IO cases, but still requires close intrapartum surveillance.
It is worth noting that, in 2010, the Chinese cesarean delivery rate was one of the highest in the world. Between 2007 and 2016, the rate was dramatically reduced at county-level and provincial-level hospitals (from 46% to 32% and 68% to 44%, respectively).22 The high rate of cesarean delivery in the IO and normal group when our study was conducted included a significant proportion of elective cesarean deliveries on maternal request (CDMR). The large sample size of CDMR enabled us to evaluate the delivery modes in the IO group. In our study, the incidence of NRFHRS in the vaginal delivery group was higher than that in the cesarean section group, which is attributed to the increased stress on the fetus during vaginal birth, especially with reduced amniotic fluid. However, there were no significant differences in low Apgar score or NICU admission between the two groups, implying that vaginal delivery did not cause adverse perinatal outcomes. Nevertheless, for the safety of the fetus, close intrapartum surveillance and rapid response for emergency cesarean section are essential.
Strengths and Limitations
The research data used for this study came from multiple levels of medical institutions. The multicenter design made our findings generalizable with minor selection bias. Furthermore, we evaluated the optimal delivery time and mode in IO cases, which provides the potential valuable advice for clinical management. However, there are several limitations. First, we did not assess whether the onset of labor was artificial or spontaneous. Second, further studies are needed to determine whether pregnancy outcomes of IO at term differ between an immediate delivery group once IO is diagnosed and a group that delays delivery until a specific gestational age. Finally, given that the severity of oligohydramnios can be classified as mild (AFI = 41–50 mm), moderate (AFI = 21–40 mm), or severe (AFI = 0–20 mm),5 it would be valuable for future research to present outcomes stratified by the degree of oligohydramnios.
Conclusion
This multicenter study demonstrates that IO is associated with increased perinatal risks, particularly fetal/neonatal complications including meconium-stained amniotic fluid, NRFHRS, and low birth weight. These complications contribute to elevated cesarean delivery rates, particularly emergency procedures. Optimal management requires comprehensive maternal-fetal assessment to determine delivery timing and mode. Vaginal delivery during 39+0 to 40+6 weeks appears optimal, with IO cases requiring enhanced intrapartum monitoring. Liberalized cesarean indications may be warranted in selected IO pregnancies to improve neonatal outcomes.
Data Sharing Statement
The data that support the findings of this study are available on request from the corresponding author.
Ethics Approval and Consent to Participate
All procedures performed in the study involving human participants conform to the 1964 helsinki Declaration and its later amendments or comparable ethical standards. This study received ethics approval from the Human Ethics Committee of Union Hospital, Tongji Medical College, Huazhong University of Science and Technology (Approval No. 2025LSZ0145). Additionally, this is a retrospective study; no interventions were applied to the subjects, so written informed consent from participants is not required.
Acknowledgments
We thank the subjects for their participation and also thank the medical staff involved in this survey at the following hospitals: Capital Medical University Beijing Obstetrics and Gynecology Hospital, Capital Medical University Friendship Hospital, Obstetrics and Gynecology Hospital of Fudan University, First Affiliated Hospital of Medical College of Xi’an Jiaotong University, Nanjing Drum Tower Hospital, Shandong Provincial Hospital, the Second Affiliated Hospital of West China Hospital, Shengjing Hospital of China Medical University, Nanfang Hospital of Nanfang Medical University, the Second Hospital of Jilin University, the First Affiliated Hospital of Xinjiang Medical University, Hebei Changzhou Central Hospital, the First Affiliated Hospital of Inner Shandong Provincial Hospital.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
The research performed herein was part of the project supported by “Health Industry Special Funds for Public Benefit Research Foundation” from the Ministry of Health, People’s Republic of China (Grant number 201002013). The research was supported by Nature Science Foundation of Hubei Province (grant No. 2016CFB656, to Hui Gao).
Disclosure
The authors declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this paper.
References
1. McCurdy CM, Seeds JW. Oligohydramnios: problems and treatment. Semin Perinatol. 1993;17(3):183–196.
2. Munn MB. Management of oligohydramnios in pregnancy. Obstet Gynecol Clin North Am. 2011;38(2):387–395, xii. doi:10.1016/j.ogc.2011.02.021
3. Leytes S, Kovo M, Weiner E, Ganer Herman H. Isolated oligohydramnios in previous pregnancy is a risk factor for a placental related disorder in subsequent delivery. BMC Pregnancy Childbirth. 2022;22(1):912. doi:10.1186/s12884-022-05230-9
4. Spong CY. Defining “term” pregnancy: recommendations from the defining “term” pregnancy workgroup. JAMA. 2013;309(23):2445–2446. doi:10.1001/jama.2013.6235
5. Zilberman Sharon N, Pekar-Zlotin M, Kugler N, et al. Oligohydramnios: how severe is severe? J Matern Fetal Neonatal Med. 2022;35(25):5754–5760. doi:10.1080/14767058.2021.1892068
6. Marks Kazatsker M, Sammour R, Sagi S. [Isolated oligohydramnios - the dilemma of proper management]. Harefuah. 2019;158(11):728–731.
7. Wax JR, Pinette MG. The amniotic fluid index and oligohydramnios: a deeper dive into the shallow end. Am J Clin Exp Obstet Gynecol. 2022;227(3):462–470. doi:10.1016/j.ajog.2022.04.016
8. Nishi K, Ozawa K, Kamei K, et al. Long-term outcomes, including fetal and neonatal prognosis, of renal oligohydramnios: a retrospective study over 22 years. J Pediatr. 2024;273:114151. doi:10.1016/j.jpeds.2024.114151
9. Mylonas I, Friese K. Indications for and risks of elective cesarean section. Dtsch Arztebl Int. 2015;112(29–30):489–495. doi:10.3238/arztebl.2015.0489
10. Tweed EJ, Mackay DF, Nelson SM, Cooper SA, Pell JP. Five-minute Apgar score and educational outcomes: retrospective cohort study of 751,369 children. Arch Dis Child Fetal Neonatal Ed. 2016;101(2):F121–126. doi:10.1136/archdischild-2015-308483
11. Persson M, Razaz N, Tedroff K, Joseph KS, Cnattingius S. Five and 10 minute Apgar scores and risks of cerebral palsy and epilepsy: population based cohort study in Sweden. BMJ. 2018;360:k207. doi:10.1136/bmj.k207
12. Dorot A, Wainstock T, Sheiner E, Walfisch A, Landau D, Harlev A. Isolated oligohydramnios and long-term neurological morbidity of the offspring. J Dev Orig Health Dis. 2020;11(6):648–652. doi:10.1017/S2040174419000795
13. Hadar O, Wainstock T, Sheiner E, Pariente G. Prenatal exposure to isolated amniotic fluid disorders and the risk for long-term cardiovascular morbidity in the offspring. Gynecol Endocrinol. 2020;36(10):873–878. doi:10.1080/09513590.2019.1706082
14. Ashwal E, Hiersch L, Melamed N, Aviram A, Wiznitzer A, Yogev Y. The association between isolated oligohydramnios at term and pregnancy outcome. Arch Gynecol Obstet. 2014;290(5):875–881. doi:10.1007/s00404-014-3292-7
15. Naveiro-Fuentes M, Puertas Prieto A, Ruíz RS, Carrillo Badillo MP, Ventoso FM, Gallo Vallejo JL. Perinatal outcomes with isolated oligohydramnios at term pregnancy. J Perinat Med. 2016;44(7):793–798. doi:10.1515/jpm-2015-0198
16. Miremberg H, Grinstein E, Herman HG, et al. The association between isolated oligohydramnios at term and placental pathology in correlation with pregnancy outcomes. Placenta. 2020;90:37–41. doi:10.1016/j.placenta.2019.12.004
17. Chauhan SP, Sanderson M, Hendrix NW, Magann EF, Devoe LD. Perinatal outcome and amniotic fluid index in the antepartum and intrapartum periods: a meta-analysis. Am J Obstet Gynecol. 1999;181(6):1473–1478. doi:10.1016/S0002-9378(99)70393-5
18. Ahmad H, Munim S. Isolated oligohydramnios is not an indicator for adverse perinatal outcome. J Pak Med Assoc. 2009;59(10):691–694.
19. Conway DL, Adkins WB, Schroeder B, Langer O. Isolated oligohydramnios in the term pregnancy: is it a clinical entity? J Matern Fetal Med. 1998;7(4):197–200. doi:10.1002/(SICI)1520-6661(199807/08)7:4<197::AID-MFM7>3.0.CO;2-D
20. Kansu-Celik H, Gun-Eryılmaz O, Dogan NU, et al. Prostaglandin E2 induction of labor and cervical ripening for term isolated oligohydramnios in pregnant women with Bishop score ≤ 5. J Chin Med Assoc. 2017;80(3):169–172. doi:10.1016/j.jcma.2016.07.004
21. Shrem G, Nagawkar SS, Hallak M, Walfisch A. Isolated oligohydramnios at term as an indication for labor induction: a systematic review and meta-analysis. Fetal Diagn Ther. 2016;40(3):161–173. doi:10.1159/000445948
22. Wang E, Hesketh T. Large reductions in cesarean delivery rates in China: a qualitative study on delivery decision-making in the era of the two-child policy. BMC Pregnancy Childbirth. 2017;17(1):405. doi:10.1186/s12884-017-1597-9
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.