Back to Journals » Infection and Drug Resistance » Volume 11
A multicenter epidemiology study on the risk factors and clinical outcomes of nosocomial intra-abdominal infections in China: results from the Chinese antimicrobial resistance surveillance of nosocomial infections (CARES) 2007–2016
Authors Zhang J, Zhao C, Chen H ![]() , Li H
, Li H ![]() , Wang Q, Wang Z, Zhang F, Wang H
, Wang Q, Wang Z, Zhang F, Wang H
Received 1 August 2018
Accepted for publication 17 September 2018
Published 15 November 2018 Volume 2018:11 Pages 2311—2319
DOI https://doi.org/10.2147/IDR.S182180
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Suresh Antony
Jiangang Zhang, Chunjiang Zhao, Hongbin Chen, Henan Li, Qi Wang, Zhanwei Wang, Feifei Zhang, Hui Wang
On behalf of the CARES Network
Department of Clinical Laboratory, Peking University People’s Hospital, Beijing, China
Objective: This study aimed to determine the risk factors for intra-abdominal infections (IAIs), assess the clinical outcomes of IAIs, and investigate the spectrum and antimicrobial resistance of major pathogens causing IAIs.
Patients and methods: This prospective observational study enrolled patients from the Chinese Antimicrobial Resistance Surveillance of Nosocomial Infections (CARES) program between 2007 and 2016. Data on the clinicopathological factors and causative pathogens were collected. The results of antimicrobial susceptibility tests were interpreted according to the minimum inhibitory concentration (MIC) interpretive breakpoints recommended by the Clinical and Laboratory Standards Institute in 2017.
Results: A total of 2,756 patients were included. The 30-day all-cause mortality was 9.5% (262/2,756). Multivariable analysis showed that the following independent risk factors were associated with the 30-day mortality: age >60 years, pulmonary disease, tracheal cannula, infection occurring in intensive care unit (ICU), prior admission within 3 months, antibiotic use before infection, recent use of immunosuppressants, and multidrug-resistant organisms. In addition, 2,913 clinical isolates were collected. The Gram-negative and Gram-positive bacteria accounted for 70.8% and 29.2% of all isolates, respectively. The most common pathogens were Escherichia coli (33.4%), Klebsiella pneumoniae (10.8%), and Enterococcus faecium (10.7%). Pseudomonas aeruginosa and Acinetobacter baumannii were the most common non-Enterobacteriaceae Gram-negative pathogens. E. faecium, Enterococcus faecalis, and Staphylococcus aureus were the most common Gram-positive pathogens. E. coli, A. baumannii, and Enterobacter cloacae were more commonly found in ICU patients than in non-ICU patients. Overall, the antibiotics tested in the CARES exhibited diminished susceptibility to pathogens over the study period, especially extended spectrum β-lactamase producing isolates.
Conclusion: Considering the current data set and high-level resistance of intra-abdominal pathogens to various antibiotics, further monitoring of the epidemiology of IAIs and their susceptibility to antibiotics through the CARES is warranted.
Keywords: intra-abdominal infections, risk factors, clinical outcomes, antimicrobial susceptibility, epidemiology
Introduction
The Chinese Antimicrobial Resistance Surveillance of Nosocomial Infections (CARES) was launched in 2007 to investigate the antimicrobial susceptibility of causative pathogens in nosocomial infections in China. This nationwide surveillance program focuses on nosocomial infections, including bloodstream infections, hospital-acquired pneumonia, and intra-abdominal infections (IAIs), and currently includes 15 tertiary care hospitals.
IAIs are frequently encountered in clinical practice in hospital and healthcare settings. The etiology of these infections, usually polymicrobial in nature, can be diverse and often involves microorganisms derived from the intestinal microbiota.1 IAIs are the second most common cause of infectious mortality in intensive care units (ICUs) and commonly result in high mortality and morbidity rates.2,3 This study aimed to investigate the prevalence, risk factors, and outcomes of nosocomial IAIs in patients admitted to 15 Chinese teaching hospitals involved in the CARES between 2007 and 2016.
Patients and methods
Study centers and patients
A total of 15 study centers were included in the CARES, and this prospective observational study enrolled 2,756 patients with nosocomial IAIs from the CARES program between 2007 and 2016. The criteria for IAI diagnosis were as follows:
- Presence of organisms cultured from purulent material sampled from the intra-abdominal space during surgical operation or needle aspiration.
- Presence of abscess or other evidence of IAI observed during surgical operation or histopathologic examination.
- Presence of at least two of the following signs or symptoms with no other recognized cause: fever (>38°C), nausea, vomiting, abdominal pain, or jaundice. In addition, at least one of the following criteria is matched:
- Organisms cultured from drainage of a surgically placed drain (such as closed-suction drainage system, open drain, or T-tube drain).
- Organisms observed on Gram’s stain of drainage or tissue obtained during surgical operation or needle aspiration.
- Organisms cultured from blood and radiographic evidence of infection (eg, abnormal findings on ultrasound, computed tomography, magnetic resonance imaging, radiolabel scans, or abdominal X-ray radiographs).4
According to the Infectious Diseases Society of America guideline, nosocomial infection includes cases involving patients with positive culture results from a normally sterile site obtained >48 hours after hospital admission.5 This study aimed to investigate the nosocomial IAIs, so patients with positive culture results from intra-abdominal body sites obtained ≤48 hours after admission were excluded. Then all patients enrolled in this study were considered as nosocomial IAIs. Patients with incomplete data were also excluded. All data included were confirmed by chart review.
Bacterial isolates
All isolates were collected from 15 tertiary care hospitals and cultured from specimens obtained from intra-abdominal body sites (eg, appendix, peritoneum, colon, bile, pelvis, or pancreas).6,7 Acceptable specimens included tissue, fluid, or deep wound cultures obtained intra-operatively as well as fluid from paracentesis or percutaneous aspiration of abscesses.8,9 Isolates recovered from blood, urine, and perirectal abscess sources outside the intra-abdominal body sites were excluded.3
Antimicrobial susceptibility testing
Antimicrobial susceptibility was determined by the agar dilution method and broth microdilution method (only for tigecycline), and the results were interpreted according to the minimum inhibitory concentration (MIC) interpretive breakpoints recommended by the Clinical and Laboratory Standards Institute (CLSI) in 2017.10 The tested antimicrobial agents included amikacin, ampicillin, ceftazidime, chloramphenicol, cefotaxime, erythromycin, cefepime, cefoxitin, levofloxacin, moxifloxacin, minocycline, rifampicin, sulfamethoxazole, teicoplanin, vancomycin (National Institute for Food and Drug Control of China, Beijing, China), ciprofloxacin (Bayer AG, Leverkusen, Germany), ceftriaxone (Hoffman-La Roche Ltd., Basel, Switzerland), cefoperazone/sulbactam, piperacillin/tazobactam, tigecycline (Pfizer, Inc., New York, NY, USA), imipenem (Merck & Co., Inc., Whitehouse Station, NJ, USA), and meropenem (Sumitomo Dainippon Pharma, Osaka, Japan). The tigecycline test was performed according to the Food and Drug Administration standards. The double-disk synergy test was used to determine extended spectrum β-lactamase (ESBL) production among isolates of Escherichia coli and Klebsiella pneumoniae as recommended by the CLSI.10 The reference isolates E. faecalis ATCC 29212, S. aureus ATCC29213, E. coli ATCC 25922 and P. aeruginosa ATCC 27853 were used as quality control isolates.
Statistical analyses
The chi-squared test or Fisher’s exact test was used to compare the categorical variables, and Student’s t-test was used to compare the continuous variables. To control the effects of confounding variables and identify the independent risk factors associated with death, a stepwise conditional logistic regression analysis was performed.11 All variables with a P-value <0.10 in univariate analysis were included in the multivariate logistic model.12 OR and 95% CI were calculated. P-values <0.05 were considered statistically significant, and all tests were two-tailed. The WHONET software (version 5.6, http://www.whonet.org/software.html) and SPSS (version 22.0) software program (IBM, Armonk, NY, USA) were used for data analyses.
Ethical statement
This study was approved by the research ethics board at Peking University People’s Hospital. Informed consent was not needed due to that the medical records and patient information were anonymously reviewed and collected in this observational study.
Results
Baseline data
A total of 2,756 patients were included in this study: 2,494 patients (90.5%) in the survival group and 262 patients (9.5%) in the nonsurvival group. In the survival group, the median age was 57 years (range, 1–94 years) and 1,509 (60.5%) of them were men. In the nonsurvival group, the median age was 62 years (range, 1–92 years) and 150 (57.3%) of them were men. The 30-day all-cause mortality was 9.5% (262/2756). The main demographic and clinical features of all patients are summarized in Table 1.
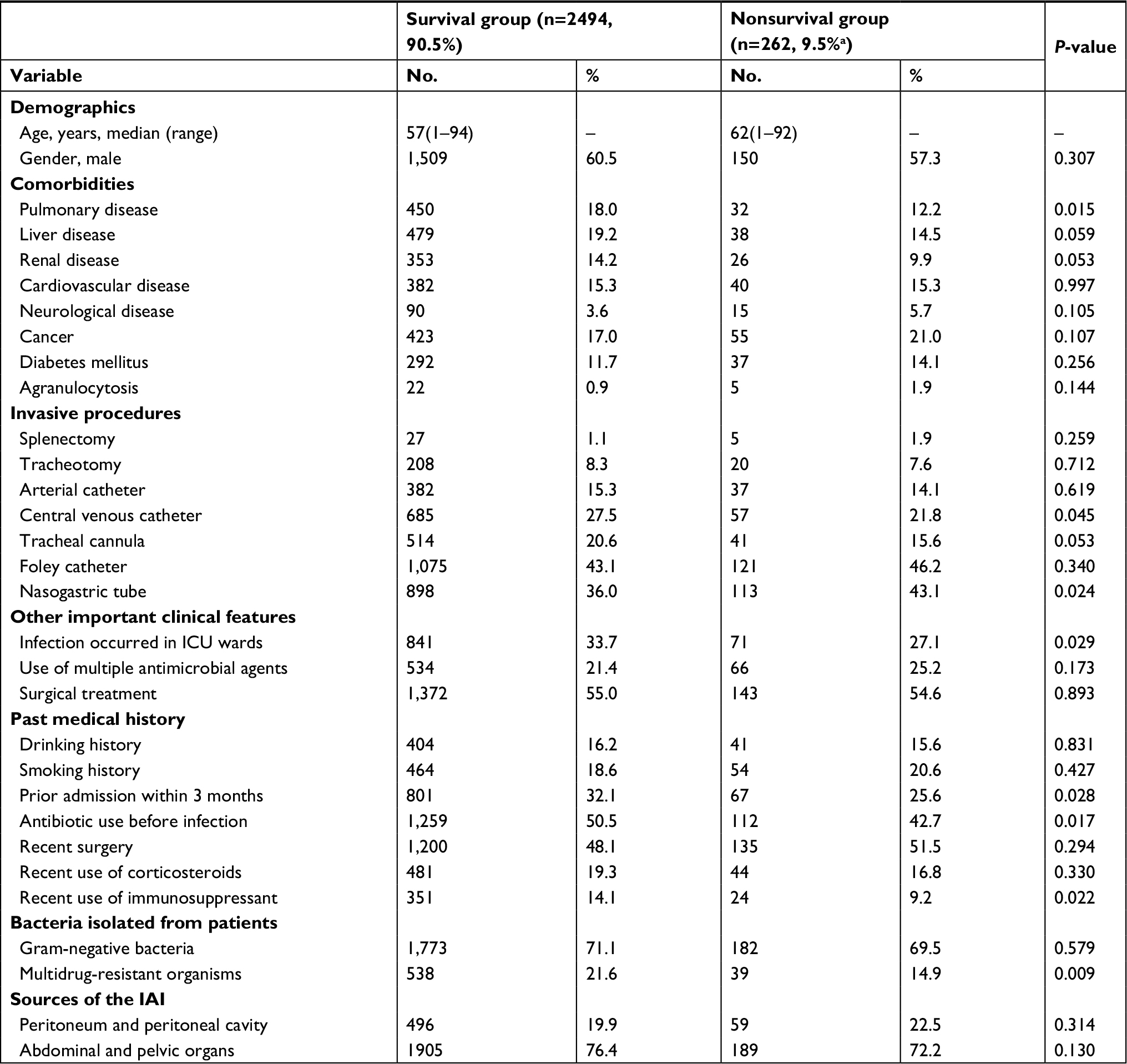 | Table 1 Demographic and clinical features of the 2,756 patients with IAIs in the study Note: a9.5% is 30-day all-cause mortality. Abbreviations: IAI, intra-abdominal infection; ICU, intensive care unit. |
Species distribution of isolates
A total of 2,913 clinical isolates were collected from intra-abdominal body sites. The species distribution of these isolates is listed in Table 2. Gram-negative bacteria accounted for 70.8% and Gram-positive bacteria accounted for 29.2% of the isolates. The most common species were E. coli (973, 33.4%), K. pneumoniae (314, 10.8%), and Enterococcus faecium (312, 10.7%), followed by P. aeruginosa (230, 7.9%), Acinetobacter baumannii (186, 6.4%), Enterococcus faecalis (175, 6.0%), Staphylococcus aureus (140, 4.8%), and Enterobacter cloacae (104, 3.6%).
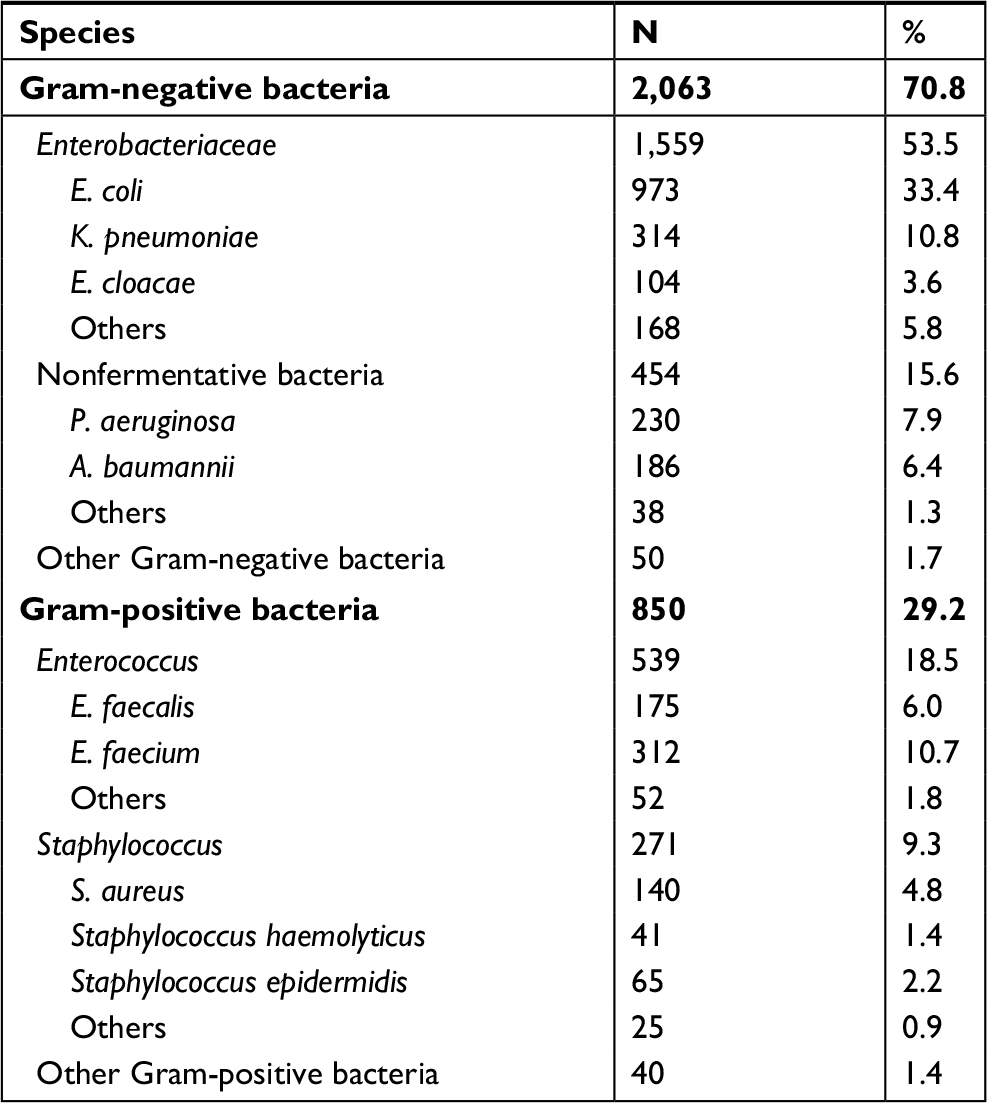 | Table 2 Species distribution of the main pathogens in all IAI cases Abbreviation: IAI, intra-abdominal infection. |
The species distribution of microorganisms collected from patients hospitalized in the ICU and non-ICU wards is presented in Table 3 (only species with ≥40 isolates are listed). E. coli, A. baumannii, and E. cloacae were more commonly found in ICU patients than in non-ICU patients (P<0.001, P<0.001, and P=0.018, respectively).
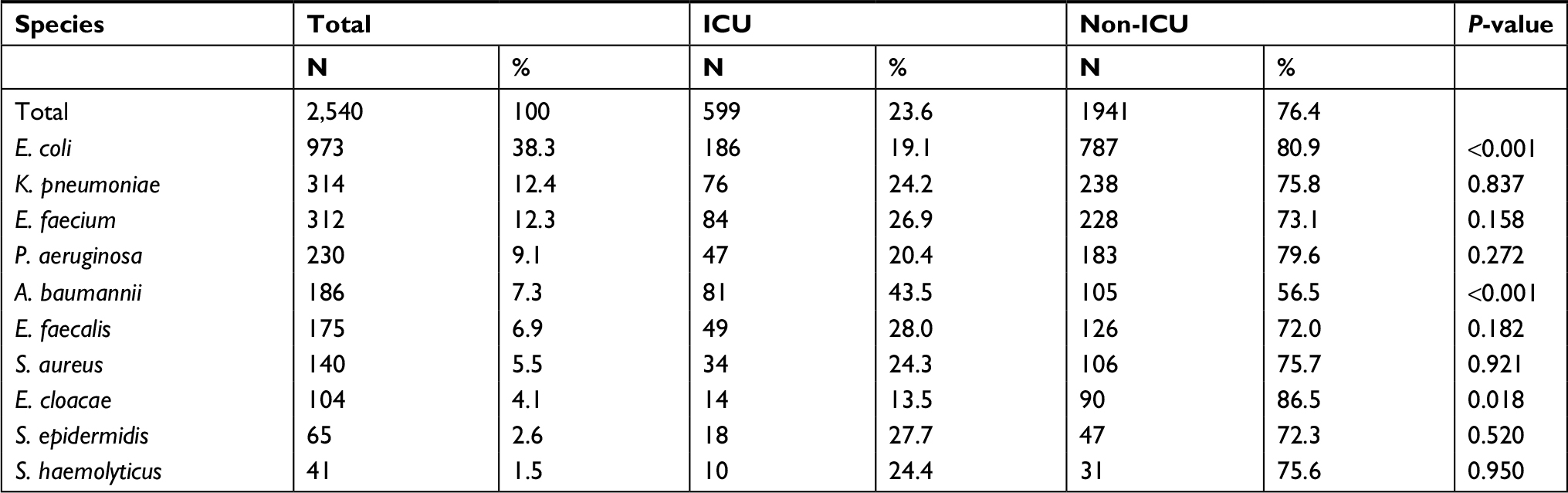 | Table 3 Species distributiona of microorganisms collected from IAI patients hospitalized in ICU and non-ICU Note: aOnly species with ≥40 isolates are listed in the table. Abbreviations: IAI, intra-abdominal infection; ICU, intensive care unit. |
Risk factors associated with the 30-day mortality
The results for the stepwise conditional logistic regression analysis of the multiple risk factors associated with death are presented in Table 4. In the univariate analysis, 30-day mortality was associated with the following 12 factors (P<0.10): age >60 years (P=0.001), pulmonary disease (18.0% vs 12.2%, P=0.015), liver disease (19.2% vs 14.5%, P=0.059), renal disease (14.2% vs 9.9%, P=0.053), central venous catheter (27.5% vs. 21.8%, P=0.045), tracheal cannula (20.6% vs 15.6%, P=0.053), nasogastric tube (36.0% vs 43.1%, P=0.024), infection occurring in ICU (33.7% vs 27.1%, P=0.029), prior admission within 3 months (32.1% vs 25.6%, P=0.028), antibiotics use before infection (50.5% vs 42.7%, P=0.017), recent use of immunosuppressants (14.1% vs 9.2%, P=0.022), and multidrug-resistant organisms (21.6% vs 14.9%, P=0.009).
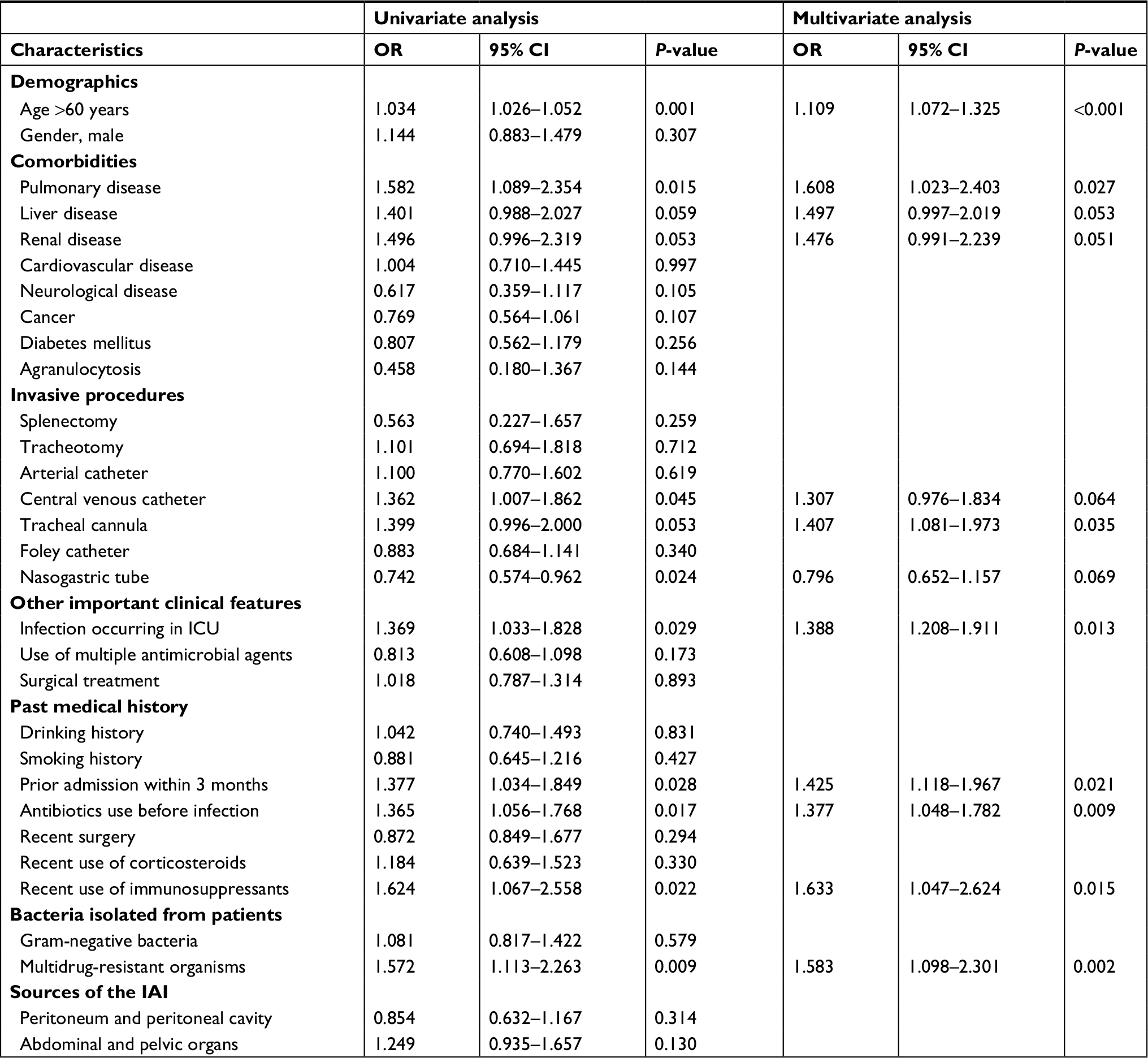 | Table 4 Univariate and multivariate analyses of the risk factors associated with 30-day all-cause mortality Abbreviations: IAI, intra-abdominal infection; ICU, intensive care unit. |
Multivariate analysis demonstrated the following independent predictors of death: age >60 years (OR, 1.109; 95% CI, 1.072–1.325; P<0.001), pulmonary disease (OR, 1.608; 95% CI, 1.023–2.403; P=0.027), tracheal cannula (OR, 1.407; 95% CI, 1.081–1.973; P=0.035), infection occurring in ICU (OR, 1.338; 95% CI, 1.208–1.911; P=0.013), prior admission within 3 months (OR, 1.425; 95% CI, 1.118–1.967; P=0.021), antibiotics use before infection (OR, 1.377; 95% CI, 1.048–1.782; P=0.009), recent use of immunosuppressants (OR, 1.633; 95% CI, 1.047–2.624; P=0.015), and multidrug-resistant organisms (OR, 1.583; 95% CI, 1.098–2.301; P=0.002).
Antimicrobial susceptibility of isolates and antimicrobial resistance trends
Susceptibility rates, MIC50, MIC90, and MIC ranges of all isolates causing IAIs between 2007 and 2016 are shown in Tables S1–S6. The antimicrobial resistance trends of the main pathogens causing IAIs between 2007 and 2016 are also presented in Figures S1–S4.
Enterobacteriaceae species
In general, tigecycline showed the highest activity (99.8% susceptible) against Enterobacteriaceae, followed by imipenem (98.3%), meropenem (97.9%), and amikacin (93.4%). Antimicrobial agents with susceptibility <50% included cefepime (47.9%), ceftriaxone (33.9%), cefotaxime (32.9%), levofloxacin (30.5%), and ciprofloxacin (29.7%). In addition, there was an increasing trend of carbapenem-resistant Enterobacteriaceae species (mainly carbapenem-resistant E. coli and carbapenem-resistant K. pneumoniae) between 2007 and 2016. The increasing trend of carbapenem-resistant K. pneumoniae was more rapid than that of carbapenem-resistant E. coli.
E. coli
A total of 973 isolates were collected, including 491 ESBL-positive isolates and 482 ESBL-negative isolates. For these isolates, meropenem, imipenem, and tigecycline showed the highest activity (all ≥97.8% susceptible) against E. coli. However, some antibiotics exhibited very poor potency. Notably, ceftriaxone and cefotaxime were the least active agents, only displaying 0.8% susceptibility against ESBL-positive isolates. In addition, there was a relatively smooth uptrend of ESBL-producing E. coli isolates from 47.4% in 2007 to 52.7% in 2016.
K. pneumoniae
A total of 314 isolates were collected, including 77 ESBL-positive isolates and 237 ESBL-negative isolates. Meropenem, imipenem, and tigecycline showed highest activity (all ≥92.0% susceptible) against K. pneumoniae. In addition, there was a relatively smooth uptrend of ESBL-producing K. pneumoniae isolates between 2007 and 2016 (except in 2011).
P. aeruginosa and A. baumannii
A total of 230 P. aeruginosa isolates and 186 A. baumannii isolates were tested. Almost all the isolates showed high-level resistance to diverse antimicrobial agents. However, only amikacin exhibited good activity (83.4% susceptible) against P. aeruginosa.
With regard to A. baumannii isolates, tigecycline exhibited the highest activity (84.4% susceptible) among the tested antimicrobial agents. A. baumannii was alarmingly resistant to diverse classes of antibiotics including third-generation cephalosporins, fluoroquinolones, aminoglycosides, and carbapenems.
Both P. aeruginosa and A. baumannii showed the same trend of an initial increase followed by a decrease in resistance to carbapenems. Nonetheless, a high resistance to carbapenems was a big threat with both the organisms.
S. aureus
A total of 140 S. aureus isolates were collected, including 89 methicillin-susceptible S. aureus (MSSA) isolates (63.6%) and 51 methicillin-resistant S. aureus (MRSA) isolates (36.4%). All these isolates were susceptible to teicoplanin and vancomycin. In addition, all MSSA isolates were susceptible to minocycline. In contrast, fluoroquinolones (ciprofloxacin, levofloxacin, and moxifloxacin) exhibited very poor activity against MRSA isolates. Erythromycin exhibited poor activity against both MRSA (13.8% susceptible) and MSSA (37.2% susceptible) isolates. The MRSA isolates showed an increasing trend from 2011 to 2016.
E. faecalis and E. faecium
A total of 175 E. faecalis and 312 E. faecium isolates were collected. All the isolates were susceptible to teicoplanin and vancomycin (≥97.4% susceptible). Overall, E. faecium isolates had a high resistance (84.0% resistant) to ampicillin, whereas E. faecalis isolates were much more susceptible to ampicillin (93.5% susceptible). Only 1.9% of E. faecium isolates showed resistance to vancomycin with a decreasing trend in resistance between 2007 and 2016.
Discussion
In this study, we investigated the risk factors for nosocomial IAIs and the outcomes of these infections. We found that age >60 years, pulmonary disease, tracheal cannula, infection occurring in ICU, prior admission within 3 months, antibiotics use before infection, recent use of immunosuppressants, and multidrug-resistant organisms were independent predictors of patient survival. Compared to other representative surveillance programs which monitor the epidemiology and trends in antibiotic resistance of intra-abdominal pathogens to currently used therapies, such as the Study for Monitoring Antimicrobial Resistance Trends (SMART) program, this study collected the demographic and clinical data of the patients in detail and analyzed the risk factors and clinical outcomes of nosocomial IAIs in China. The data and results of this study may be helpful to the IAI treatment in clinic.
A total of 2,913 isolates were collected from 15 tertiary care teaching hospitals involved in the CARES between 2007 and 2016. We analyzed the updated epidemiology and antimicrobial susceptibility of the causative pathogens. The epidemiological data from our study highlights the diversity of intra-abdominal pathogens, as many different species causing IAIs were isolated. Of these, the most common species were E. coli (33.4%), K. pneumoniae (10.8%), and E. faecium (10.7%). Not surprisingly, Enterobacteriaceae isolates were the predominant species causing IAIs, accounting for at least 50% of all isolated pathogens.
Our study using data from the CARES program revealed several important findings. First, the combinations of cephalosporins, fluoroquinolones, and β-lactam/β-lactamase inhibitors tested in the CARES exhibited diminished susceptibility against the collected isolates over the study period. Second, the nonfermentative Gram-negative bacilli were alarmingly resistant to diverse classes of antimicrobial agents. The susceptibilities of A. baumannii isolates to carbapenems, third- or fourth-generation cephalosporins, fluoroquinolones, and aminoglycosides were less than ~30%, which presents a key problem for empirical therapeutic choice. Although A. baumannii was not a major pathogen for IAIs, the trends of its resistance, especially, to carbapenems should be monitored.13 Third, amikacin, tigecycline, and carbapenems including imipenem and meropenem were consistently potent against Enterobacteriaceae isolates throughout the study period. Thus, tigecycline monotherapy, carbapenem monotherapy, or amikacin-based combination therapy could provide the strongest activity against Enterobacteriaceae causing IAIs.8 Fourth, the overall increase in the isolation of Gram-positive pathogens was accompanied by an increase in the multidrug-resistant phenotypes, making it difficult to choose the appropriate therapy for IAIs.
In our study, ESBL-producing isolates showed high-level resistance to diverse antimicrobial agents. A high prevalence of ESBL-producing isolates in China has been reported in several studies, and the continually diminishing susceptibility to many antimicrobial agents is alarming.6,14 The SMART study, which monitored the resistance of Gram-negative pathogens causing IAIs, showed that 43.9% of E. coli and 30.4% of K. pneumoniae isolates were ESBL producers.3 These ESBL-producing strains exhibited resistance to more antibiotics than non-ESBL-producing strains. Our current study showed that carbapenems and amikacin are the most active antibiotics, which was consistent with our antimicrobial susceptibility results. So far, the recommended antibiotics for the treatment of serious infections caused by ESBL-producing bacteria are carbapenems, particularly for patients with severe sepsis.15 A previous study showed that the adequacy of initial antibiotic therapy for serious ESBL-infection was associated with mortality.16
A steady decrease in the susceptibility to most non-carbapenem antimicrobial agents has been observed over time; however, the carbapenem consumption has increased and maybe the reason for the increasing carbapenem resistance reported among Enterobacteriaceae species.17 Despite increased consumption of carbapenems and the emergence of varieties of carbapenem resistant mechanisms, susceptibility of Enterobacteriaceae species to carbapenems was consistently high in our study.
Infections caused by resistant microorganisms increase the risk of mortality, especially because the initial empiric therapy may be inadequate.1 Due to the dissimilarity in the nature of the IAI pathogens, appropriate antibiotics for IAIs were studied, leading to differences in antibiotic treatment. Two publications were recommended as guidelines for empirical antibiotic treatment for IAIs.18,19 To select adequate therapy for IAIs in clinical practice, updated data on the local resistance epidemiology of these pathogens should be available;1 therefore, surveillance studies are necessary. Many epidemiological surveillance programs and studies worldwide, such as the SMART, China antimicrobial Surveillance Network (http://www.chinets.com), and CARES, have provided important information on the pathogens involved in many infections and ongoing resistance to the main classes of antibiotics used in clinical practice. Surveillance studies are key in not only identifying specific pathogens associated with IAIs but also assessing resistance rates and trends in resistance for antimicrobials commonly used to treat IAIs. The combination of resistance rates, trends in resistance over time, and trends in mechanisms of resistance will help physicians, pharmacists, and clinical microbiologists understand the evolution and spread of pathogens.20
Despite our important findings, the main problem of the present study is that it is observational in nature, which might result in limitations that preclude accurate comparisons, and thus unknown risk factors might have been unequally distributed between groups.
Conclusion
Antibiotic resistance among IAI-causing species is a serious threat in China, and close monitoring of antibiotic resistance among pathogens associated with IAIs is crucial for guiding measures to prevent further emergence of resistance and to provide clinicians with the necessary information to appropriately select empirical therapy. Up-to-date national, regional, and global microbial surveillance is needed to provide updated information for the optimal therapy of IAIs.
Data availability
The data sets supporting the conclusion of this article are included within the article and its Supplementary materials.
Acknowledgments
The authors thank all the investigators for their participation in the CARES program. The CARES team included Peking University People’s Hospital, Peking University Third Hospital, Zhongshan Hospital Affiliated to Fudan University, The First Affiliated Hospital of Sun Yat-sen University, Guangzhou Institute of Respiratory Disease, The First Hospital of China Medical University, Tianjin Medical University General Hospital, Xijing Hospital Affiliated to the Fourth Military Medical University, The Second Affiliated Hospital of Zhejiang University School of Medicine, Xiangya Hospital Affiliated to Central South University, Chinese PLA General Hospital, Beijing Chaoyang Hospital Affiliated to Capital Medical University, Shandong Provincial Hospital Affiliated to Shandong University, Peking Union Medical College Hospital, and Wuhan Union Hospital Affiliated with Tongji Medical College, and Huazhong University of Science and Technology. This study (CARES program) was supported by a research grant from Pfizer Inc. The funder had no role in the study design, data collection, and interpretation or the decision to submit this work for publication.
Author contributions
On behalf of the CARES group, Hui Wang conceived and designed the study. She also checked the data and revised the article. Jiangang Zhang analyzed the data and wrote the paper. All authors contributed to data analysis, drafting and revising the article, gave final approval of the version to be published, and agree to be accountable for all aspects of the work.
Disclosure
The authors report no conflicts of interest in this work.
References
Nicoletti G, Nicolosi D, Rossolini GM, Stefani S. Intra-abdominal infections: etiology, epidemiology, microbiological diagnosis and antibiotic resistance. J Chemother. 2009;21(Suppl 1):5–11. | ||
Armstrong C. Updated guideline on diagnosis and treatment of intra-abdominal infections. Am Fam Physician. 2010;82(6):694–709. | ||
Chang YT, Coombs G, Ling T, et al. Epidemiology and trends in the antibiotic susceptibilities of Gram-negative bacilli isolated from patients with intra-abdominal infections in the Asia-Pacific region, 2010–2013. Int J Antimicrob Agents. 2017;49(6):734–739. | ||
Horan TC, Andrus M, Dudeck MA. CDC/NHSN surveillance definition of health care-associated infection and criteria for specific types of infections in the acute care setting. Am J Infect Control. 2008;36(5):309–332. | ||
Solomkin JS, Mazuski JE, Bradley JS, et al. Diagnosis and management of complicated intra-abdominal infection in adults and children: guidelines by the Surgical Infection Society and the Infectious Diseases Society of America. Clin Infect Dis. 2010;50(2):133–164. | ||
Hawser SP, Bouchillon SK, Hoban DJ, Badal RE, Hsueh PR, Paterson DL. Emergence of high levels of extended-spectrum-beta-lactamase-producing gram-negative bacilli in the Asia-Pacific region: data from the Study for Monitoring Antimicrobial Resistance Trends (SMART) program, 2007. Antimicrob Agents Chemother. 2009;53(8):3280–3284. | ||
Hawser S, Hoban DJ, Badal RE, et al. Epidemiology and antimicrobial susceptibility of Gram-negative aerobic bacteria causing intra-abdominal infections during 2010-2011. J Chemother. 2015;27(2):67–73. | ||
Ko WC, Hsueh PR. Increasing extended-spectrum beta-lactamase production and quinolone resistance among Gram-negative bacilli causing intra-abdominal infections in the Asia/Pacific region: data from the Smart Study 2002-2006. J Infect. 2009;59(2):95–103. | ||
Chen YH, Hsueh PR, Badal RE, et al. Antimicrobial susceptibility profiles of aerobic and facultative Gram-negative bacilli isolated from patients with intra-abdominal infections in the Asia-Pacific region according to currently established susceptibility interpretive criteria. J Infect. 2011;62(4):280–291. | ||
Clinical and Laboratory Standards Institute. Performance standards for antimicrobial susceptibility testing; twenty-seventh informational supplement. Document M100-S27. Wayne, PA: CLSI; 2017. | ||
Boontham P, Soontomrak R. Intra-Abdominal Infections: Prevalence and Risk Factors of ESBLs Infections. J Med Assoc Thai. 2015;98(11):1097–1103. | ||
Wang Q, Zhang Y, Yao X, et al. Risk factors and clinical outcomes for carbapenem-resistant Enterobacteriaceae nosocomial infections. Eur J Clin Microbiol Infect Dis. 2016;35(10):1679–1689. | ||
Lautenbach E, Weiner MG, Nachamkin I, Bilker WB, Sheridan A, Fishman NO. Imipenem resistance among pseudomonas aeruginosa isolates: risk factors for infection and impact of resistance on clinical and economic outcomes. Infect Control Hosp Epidemiol. 2006;27(9):893–900. | ||
Morrissey I, Hackel M, Badal R, Bouchillon S, Hawser S, Biedenbach D. A Review of Ten Years of the Study for Monitoring Antimicrobial Resistance Trends (SMART) from 2002 to 2011. Pharmaceuticals. 2013;6(11):1335–1346. | ||
Tumbarello M, Sanguinetti M, Montuori E, et al. Predictors of mortality in patients with bloodstream infections caused by extended-spectrum-beta-lactamase-producing Enterobacteriaceae: importance of inadequate initial antimicrobial treatment. Antimicrob Agents Chemother. 2007;51(6):1987–1994. | ||
Peralta G, Lamelo M, Alvarez-García P, et al. Impact of empirical treatment in extended-spectrum beta-lactamase-producing Escherichia coli and Klebsiella spp. bacteremia. A multicentric cohort study. BMC Infect Dis. 2012;12:245. | ||
Hsueh PR, Badal RE, Hawser SP, et al. Epidemiology and antimicrobial susceptibility profiles of aerobic and facultative Gram-negative bacilli isolated from patients with intra-abdominal infections in the Asia-Pacific region: 2008 results from SMART (Study for Monitoring Antimicrobial Resistance Trends. Int J Antimicrob Agents. 2010;36(5):408–414. | ||
Hsueh PR, Hawkey PM. Consensus statement on antimicrobial therapy of intra-abdominal infections in Asia. Int J Antimicrob Agents. 2007;30(2):129–133. | ||
Solomkin JS, Mazuski JE, Bradley JS, et al. Diagnosis and management of complicated intra-abdominal infection in adults and children: guidelines by the Surgical Infection Society and the Infectious Diseases Society of America. Clin Infect Dis. 2010;50(2):133–164. | ||
Kazmierczak KM, Lob SH, Hoban DJ, Hackel MA, Badal RE, Bouchillon SK. Characterization of extended-spectrum beta-lactamases and antimicrobial resistance of Klebsiella pneumoniae in intra-abdominal infection isolates in Latin America, 2008-2012. Results of the Study for Monitoring Antimicrobial Resistance Trends. Diagn Microbiol Infect Dis. 2015;82(3):209–214. |
 © 2018 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2018 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.