Back to Journals » Journal of Asthma and Allergy » Volume 19
A Multi-Compartment Cytological Approach to Severe Asthma Phenotyping: The BRISA Study (Biomedical Research in Severe Asthma)
Authors Domínguez-Ortega J ![]() , Leon-Zambrana G
, Leon-Zambrana G ![]() , Cañas JA, García-Moguel I
, Cañas JA, García-Moguel I ![]() , Igea JM, Valverde-Monge M
, Igea JM, Valverde-Monge M ![]() , Caballero ML, Gandolfo-Cano M, De las Vecillas L
, Caballero ML, Gandolfo-Cano M, De las Vecillas L ![]() , Quirce S
, Quirce S ![]() , Del Pozo V
, Del Pozo V
Received 10 January 2026
Accepted for publication 31 March 2026
Published 25 May 2026 Volume 2026:19 591415
DOI https://doi.org/10.2147/JAA.S591415
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Luis Garcia-Marcos
Javier Domínguez-Ortega,1– 3 Gabriela Leon-Zambrana,1 José Antonio Cañas,3,4 Ismael García-Moguel,5,6 Juan Manuel Igea,7 Marcela Valverde-Monge,3,8 María Luisa Caballero,1– 3 Mar Gandolfo-Cano,1,2 Leticia De las Vecillas,1– 3 Santiago Quirce,1– 3 Victoria Del Pozo3,4,9
1Department of Allergy, Hospital Universitario La Paz, Madrid, Spain; 2Institute for Health Research (Idipaz), Hospital Universitario La Paz, Madrid, Spain; 3Biomedical Research Networking Centre in Respiratory Diseases (CIBERES), Madrid, Spain; 4Department of Immunology, Health Research Institute-Fundación Jiménez Díaz, Universidad Autónoma de Madrid (IIS-FJD, UAM), Madrid, Spain; 5Department of Allergy, Hospital Universitario 12 de Octubre, Madrid, Spain; 6Institute for Health Research, Hospital Universitario 12 de Octubre (i+12), Madrid, Spain; 7Allergy and Asthma Clinic, Salamanca, Spain; 8Allergy Department, Hospital Universitario Fundación Jiménez Díaz, Madrid, Spain; 9Medicine Department, Faculty of Medicine, Universidad Autónoma de Madrid (UAM), Madrid, 28029, Spain
Correspondence: Gabriela Leon-Zambrana, Department of Allergy, Hospital Universitario La Paz, Paseo de la Castellana 261, Madrid, 28046, Spain, Email [email protected]
Background: Accurate inflammatory phenotyping in asthma remains challenging. Nasal cytology has emerged as a potential non-invasive tool to assess airway inflammation in asthma. However, its relationship with lower airway inflammation and systemic biomarkers remains unclear, particularly in severe asthma (SA).
Objective: To evaluate whether a multi-compartment approach could improve the characterisation of type 2 inflammation and the relationship between nasal cytology, induced sputum, and systemic inflammatory biomarkers in patients with severe asthma.
Methods: In this cross-sectional exploratory BRISA study, twenty-two patients with SA underwent nasal cytology by mucosal scraping, induced sputum analysis, and serum biomarker assessment (periostin, eosinophil cationic protein, thymic stromal lymphopoietin, dipeptidyl peptidase-4, and total IgE). Patients were stratified according to blood eosinophil count (BEC < 300 vs ≥ 300 cells/μL). Correlations between compartments and associations with clinical and inflammatory variables were analysed.
Results: Higher blood eosinophil counts were associated with worse lung function, increased exacerbations, and higher serum periostin levels. Valid induced sputum samples were obtained in 16 patients: 7 eosinophilic, 3 neutrophilic, 2 mixed eosinophilic-neutrophilic and 4 paucigranulocytic. Nasal cytology predominantly showed limited agreement with induced sputum inflammatory phenotypes. Serum TSLP, DPP4, and IgE also showed an upward trend in patients with higher blood eosinophil counts, although these differences were not statistically significant. Correlation analysis demonstrated a significant positive association between sputum and blood eosinophils, as well as between blood eosinophils and serum periostin. A strong positive correlation was also observed between serum eotaxin and TSLP.
Conclusion: Nasal cytology alone cannot replace induced sputum for inflammatory phenotyping in SA, although it may provide complementary information on upper airway inflammation. Among the evaluated systemic biomarkers, periostin emerged as the most consistent marker associated with blood eosinophilia, while other biomarkers showed only non-significant trends. Further studies are needed to validate the role of combined biomarkers in predicting airway inflammation.
Keywords: asthma, nasal cytology, induced sputum, biomarkers
A Letter to the Editor has been published for this article.
Introduction
Asthma is a highly prevalent chronic respiratory disease, affecting 5–10% of the general population and exhibiting marked heterogeneity in both its underlying pathophysiology and clinical manifestations. Although most patients achieve adequate control with standard therapies, approximately 5% develop severe asthma (SA), with persistent symptoms, exacerbations or airflow limitation despite optimized management with high doses of inhaled corticosteroids (ICS) and additional controller medications.1 Three broad asthma phenotypes are recognised: allergic T2 asthma, driven by IgE sensitisation and Th2 cytokines; non-allergic eosinophilic T2 asthma, mostly linked to Interleukin (IL-5) pathways; and low-T2 asthma, typically, but not only, neutrophilic, associated with Th17/IL-8 axis.2 This heterogeneity has motivated the development of targeted biologic therapies, omalizumab, anti-IL-5/IL-5R agents, dupilumab and tezepelumab, offering precision approaches to T2-driven disease.1 However, despite substantial clinical benefits, up to 60% of patients with SA fail to reach clinical remission with current available biologics.3,4
A major barrier to precision therapy is the difficulty in accurately identifying inflammatory phenotypes using accessible and reliable biomarkers. Peripheral blood eosinophil count (BEC) remains the most widely used surrogate for eosinophilic inflammation due to its ease of measurement,1 but its specificity is limited since peripheral eosinophilia can arise from multiple non-asthma conditions and can be influenced by other factors such as allergen exposure5 or the use of oral corticosteroids.6 Induced sputum, a more specific and pathophysiological relevant technique, correlates strongly with bronchial biopsy and bronchoalveolar lavage, but its clinical use is restricted by technical complexity, need for specialised personnel, biosafety limitations, and low sample validity rates outside experienced centres.7 Given these constraints, alternative, accessible tools capable of reflecting airway inflammation are needed. Nasal cytology (NC) is a simple, inexpensive, and reproducible diagnostic test widely used in the study of allergic rhinitis (AR) and chronic rhinosinusitis with nasal polyps (CRSwNP).8 NC may have important value in subtyping AR and optimizing AR treatment.9 Through mucosal scraping or brushing followed by May-Grünwald–Giemsa staining, it allows direct assessment of epithelial morphology and inflammatory cell composition, evaluating the number, type and morphological characteristics of the cells present in the mucosa or of the nasal secretion.10 This procedure allows to identify bacteria, fungal hyphae and spores.8 NC correlates well with nasal biopsy, is minimally invasive, and is feasible even in resource-limited settings. Because asthma, AR, and CRS frequently coexist and are considered manifestations of a unified airway inflammatory process,11 NC might have the potential to provide insights into lower airway inflammation. However, the utility of NC for asthma phenotyping remains poorly defined. De Farias et al showed that nasal lavage could identify eosinophilic asthma with high specificity (94%),12 but those results need further validation in other populations or with direct cytology scraping. Recently, De Corso et al observed a significant association between higher blood eosinophil counts and increased eosinophilic inflammation on NC in a cohort of 425 subjects with CRSwNP and comorbidities (such as asthma, allergy and non-steroidal anti-inflammatory drug-exacerbated respiratory disease) when compared to subjects with CRSwNP alone.13 Moreover, the relationship between epithelial remodelling, local mucus characteristics, and systemic inflammation remains underexplored.
In addition to cellular assessment across airway compartments, circulating biomarkers have emerged as accessible indicators of T2 inflammation. Molecules such as periostin and Dipeptidyl Peptidase-4 (DPP4), (markers of IL-13 activity/IL-13 driven inflammation), total IgE, thymic stromal lymphopoietin (TSLP) as a key epithelial alarmin, and eotaxin-3 and eosinophil cationic protein (ECP) involved in eosinophil recruitment, have been associated with T2 inflammation and asthma severity.2 However, their relationship with airway-specific inflammatory patterns remains incompletely understood.
The aim of the BRISA study was to explore whether a multi-compartment approach, integrating nasal mucosa, induced sputum (IS), peripheral blood, and circulating inflammatory mediators, may provide a more accurate representation of T2 inflammation than single biomarkers alone to enhance phenotyping in adults with SA. Additionally, we sought to determine the relationship between cytological findings and systemic biomarkers of T2 inflammation. By exploring inter-compartment correlations, we aimed to determine the feasibility, complementariness, and potential clinical value of NC in routine severe asthma evaluation.
Materials and Methods
BRISA (Biomedical Research in Severe Asthma; ESR-17-13154) was an exploratory multicentre cross-sectional study conducted in three tertiary hospitals in Madrid, Spain (Hospital Universitario La Paz, Hospital Universitario 12 de Octubre and Hospital Universitario Fundación Jiménez Díaz) between January 2020 to December 2023. Given the exploratory nature of the study, no formal sample size calculation was performed. All consecutive patients meeting inclusion criteria during the study period were included. Eligible patients were adults aged 18–80 years with confirmed SA according to GINA criteria and whose lung function allowed safe sputum induction, according to usual clinical practice in those three Severe Asthma Units. Exclusion criteria included nasal pathology preventing mucosal sampling, active smoking >10 pack-years, and treatment with monoclonal antibodies during the previous 6 months. All participants provided informed consent in compliance with the Declaration of Helsinki. The study was approved by the three local Ethics Committees of the participating centers.
Clinical Evaluation
Patients underwent a structured clinical assessment including asthma duration, current asthma medication, severe exacerbations in the last year, comorbidities, family history of allergy, pulmonary function testing by spirometry, fractional exhaled nitric oxide (FeNO), skin prick testing, Asthma Control Test (ACT) and Mini Asthma Quality of Life Questionnaire (miniAQLQ) score.
Induced Sputum
Sputum was induced by inhalation of hypertonic saline following Hargreaves’ method,14 and cytological analysis was subsequently performed on the collected sample. Sputum samples were classified as eosinophilic or neutrophilic when cell counts showed ≥3% eosinophils or ≥ 61% neutrophils, respectively. When both thresholds were met, the sample was considered to have a mixed inflammatory pattern.
Nasal Cytology
Mucosal specimens were obtained from the middle third of the inferior turbinates using the Rhino-probe small scraper (Arlington Scientific, Springville, UT, USA) under anterior rhinoscopy. Samples were transferred onto glass slides, air-dried for fixation, and stained using the May–Grünwald–Giemsa method. Eosinophils and neutrophils were counted at 400× magnification under a light microscope by the same observer. Nasal cytology inflammatory patterns were classified descriptively according to the predominant cell type (eosinophilic, neutrophilic, mixed, or paucigranulocytic). Given the absence of universally accepted cutoffs for nasal cytology,15,16 no predefined quantitative thresholds were applied, and classification was based on relative cellular predominance. Alterations in the respiratory epithelium, including epithelial islets, goblet cell hyperplasia, squamous metaplasia, and excessive mucus production, were documented. The presence of bacteria and biofilm was also assessed. At least 10 well-spread high-power fields were examined, and all evaluations were performed blinded to the patients’ clinical status. Results are presented as the percentage of each cell group. A semiquantitative evaluation of the slides was also performed, grading inflammatory cells as: none, occasional, few, moderate number, large clumps, and clumps covering the field.17
Determination of Cytokines and Proinflammatory Mediators in Serum by ELISA
Three millilitres (mL) of peripheral blood were collected from the patients included in the study. Patients were categorized according to peripheral BEC (<300 and ≥300 cells/μL). TSLP, and periostin levels in serum were determined using human TSLP and Periostin/OSF-2 DuoSet ELISA kits (R&D Systems, Bio-Techne, Minneapolis, MN, USA), following the manufacturer’s protocol. For the TSLP ELISA, serum was diluted 1:10, while for the periostin ELISA, serum samples were used undiluted. Additionally, Eosinophil Cationic Protein (ECP), Dipeptidyl Peptidase-4 (DPP4) and eotaxin-3 (CCL26) were quantified using human-ECP, human-DPP4, and human-CCL26 ELISA kits (Cusabio technology LLC, Houston, TX, USA), according to the manufacturer’s instructions. For CCL26 determination, undiluted serum was used; for ECP, serum was diluted 1:2; and for DPP4 analysis, serum was diluted 1:20. The lower limits of detection (LLD) for the ELISA assays were as follows: periostin 62.5 pg/mL (R&D Systems, Minneapolis, MN, USA), TSLP 31.2 pg/mL (R&D Systems), CCL26 9.75 pg/mL (Cusabio), DPP4 0.39 ng/mL (Cusabio) and ECP 0.39 ng/mL (Cusabio).
Statistical Methods
This was an exploratory cross-sectional study. A formal a priori sample size calculation was not performed. All consecutive patients meeting inclusion criteria during the study period were included. Given the limited number of patients with complete paired data across compartments, the study was not powered for formal correlation or predictive analyses. Qualitative data were described using absolute frequencies and percentages, whereas quantitative data were summarised using the mean and standard deviation or the median and interquartile range, depending on their distribution. The normality of continuous variables was assessed using the Shapiro–Wilk test. Comparisons between qualitative variables were performed using Fisher’s exact test. Associations between qualitative and quantitative variables were analysed using the Student’s t-test or, when assumptions were not met, the non-parametric Mann–Whitney U-test. For comparisons involving more than two groups, the non-parametric Kruskal–Wallis test was applied followed by Dunn’s multiple comparisons post hoc test. Relationships between quantitative variables were examined using Pearson’s correlation coefficient or its non-parametric counterpart, Spearman correlation. All statistical tests were two-tailed, with significance set at p-values < 0.05. Data analysis was conducted using the R statistical software, version 4.3.3 (R Core Team, 2024).
Results
Clinical and Demographic Characteristics
Twenty-two patients were finally included, of whom 16 (73%) were women. Most participants (73%) were non-smokers, 18% former-smokers and only 4% active-smokers. Table 1 summarizes their main demographic and clinical characteristics. Notably, 72% of the subjects presented concomitant AR, 45.5% of them moderate to severe persistent AR, and 50% had CRSwNP. BEC were a key differentiator: 81.8% of patients had BEC≥150 cells/µL and 59.1% had BEC≥300 cells/µL. Higher BEC was associated with more exacerbations in the previous year and poorer lung function, as reflected by lower FEV1/FVC ratios and significantly increased FeNO levels (Table 1).
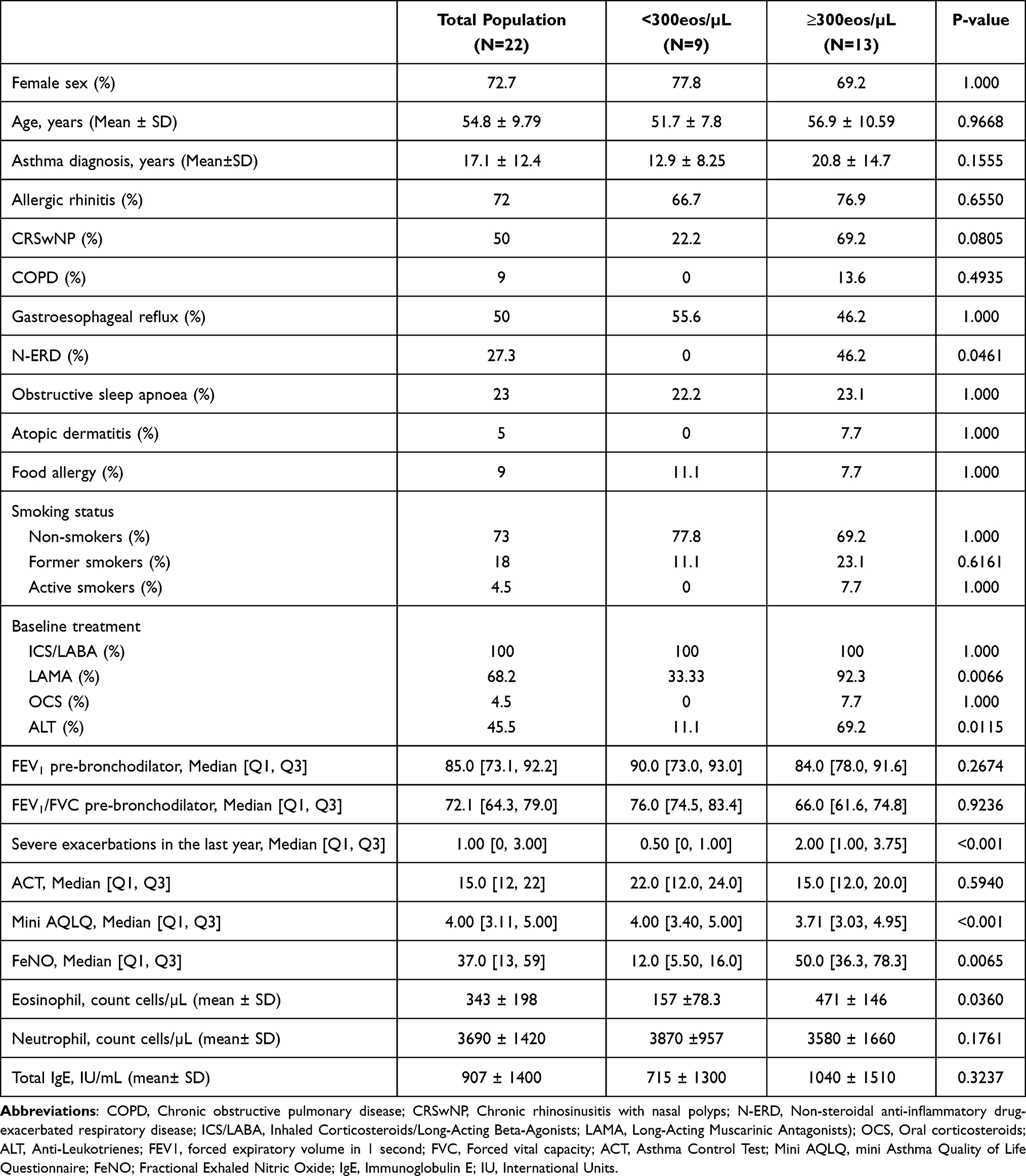 |
Table 1 Clinical and Demographic Characteristics |
Evaluation of Immune and Clinical Profile in NC and Sputum Samples
A valid induced sputum sample was obtained from 16 of the 22 patients: 7 showed an eosinophilic pattern, 3 a neutrophilic pattern, 2 a mixed eosinophilic–neutrophilic pattern, and 4 were paucigranulocytic. Regarding NC, most samples displayed a neutrophilic inflammatory pattern (58.82%), while 29.41% showed a mixed eosinophilic–neutrophilic pattern, and only 11.76% showed a purely eosinophilic pattern.
With regard to the NCs, it should be noted that only 22.7% of patients presented a normal nasal epithelium; 50% exhibited epithelial islets, 13.6% goblet cell hyperplasia, and 36.4% squamous metaplasia. The presence of epithelial islets was significantly associated with BEC≥300 cells/µL (p < 0.05), whereas goblet cell hyperplasia was more frequent in individuals with high FeNO levels (p = 0.0360). Concordance between induced sputum and nasal cytology inflammatory patterns was poor (p = 0.615).
Blood Inflammatory Profile
Patients with BEC≥300 cells/µL showed significantly higher serum periostin levels (p = 0.0034, Figure 1). Serum TSLP, DPP4, and total IgE showed a tendency toward higher values in this group, although these differences did not reach statistical significance (Figure 1 and Table 1). No significant differences were observed for the remaining biomarkers (Figure 1). Eosinophilic sputum was significantly associated with BEC≥300 cells/µL (p = 0.0462). By contrast, although eosinophilic NC tended to be more frequent in patients with BEC≥300 cells/µL, this association did not reach statistical significance (p = 0.08). Concordance between induced sputum and nasal cytology inflammatory patterns was poor, the kappa index was –0.0862 (95% CI –0.4225 to 0.2501), with a p-value of 0.6154. Interestingly, nasal samples with abundant mucus were associated with higher DPP4 values [2040 ± 550 ng/mL in low-mucus samples vs. 3020 ± 756 ng/mL in high-mucus samples (p = 0.0045)].
 |
Figure 1 Biomarkers in serum. Mediators’ concentration of ECP, eotaxin, DPP4, periostin and TSLP was evaluated by conventional ELISA in serum. Data represented mean ± standard deviation. **p < 0.01. |
Figure 2 shows a correlation matrix between cellular parameters (sputum, nasal and blood eosinophils and neutrophils percentages) and serum biomarker levels. Analysis revealed both a moderate positive correlation between blood and sputum eosinophil percentage (ρ = 0.58, p = 0.012), as well as between serum periostin and eosinophil percentage (ρ = 0.61, p = 0.006). Additionally, serum biomarkers such as periostin and TSLP show a strong positive correlation between them (ρ = 0.79, p = 0.048).
 |
Figure 2 Correlation matrix of blood, sputum and nasal cellular parameters and serum biomarkers. The heatmap illustrates Spearman correlation coefficients (ρ) between blood, sputum and nasal immune cell populations (eosinophils and neutrophils) and selected soluble mediators. Positive correlations are shown in green and negative correlations in red, with colour intensity proportional to the strength of the association. *p < 0.05, **p < 0.01. Abbreviations: IS, induced sputum; NS, nasal smear/nasal cytology; Eos, eosinophils; Neu; neutrophils; tIgE, total immunoglobulin E; DPP4, dipeptidyl peptidase-4; TSLP, thymic stromal lymphopoietin; ECP, eosinophil cationic protein. |
Discussion
This study evaluated whether NC obtained by mucosal scraping could serve as a reliable surrogate or complementary tool to induced sputum for the inflammatory phenotyping of SA. Serum biomarkers were selected because blood sampling is minimally invasive, reproducible, and widely available in routine clinical practice. In contrast, induced sputum requires specialized processing and is not always feasible in patients with severe asthma. By integrating nasal, bronchial (sputum), blood, and serum biomarkers, we aimed to explore a multi-compartment model of T2 inflammation and assess its potential clinical utility. Several important observations emerged.
First, we found that NC and induced sputum frequently revealed discordant inflammatory patterns. While eosinophilic inflammation predominated in sputum samples, the nasal mucosa more often exhibited mixed or neutrophilic profiles. Concordance between compartments was poor, and nasal eosinophilia did not reliably predict sputum eosinophilia. These findings indicate that, despite the well-established concept of “united airways”, the inflammatory environment of the upper and lower airways may diverge substantially in SA. Elucidating the mechanisms that govern the interplay between the upper and lower airways is essential for understanding, for instance, the heterogeneous therapeutic responses observed in patients with concomitant asthma and CRSwNP.18 Differences in epithelial exposure to environmental stimuli, microbial burden,19 corticosteroid deposition,20 and tissue remodelling likely to contribute to this compartmental heterogeneity. Our findings reinforce that the presence of eosinophilia/neutrophilia in the nasal mucosa cannot be assumed to reflect the inflammation pattern of the lower airway. However, our results may have been influenced by the high prevalence of nasal polyposis in our cohort which may have influenced nasal cytology findings. CRSwNP is associated with a distinct inflammatory profile, often characterized by T2 inflammation and epithelial alterations, which may not parallel lower airway inflammation. Moreover, the interpretation of epithelial alterations observed in nasal cytology is limited by the lack of detailed upper airway phenotyping, including CRS classification, N-ERD status, and standardized symptom, use of intranasal and inhaled steroids or radiological scores. Therefore, these findings should be interpreted as descriptive rather than indicative of disease severity or structural remodelling. Finally, to date, no standardized cut-off values have been established for the evaluation of nasal cytology to differentiate between cellular patterns, this is largely due to the use of different sampling techniques (nasal lavage, scraping or brushing), which complicates the comparison of cellular findings and prevents the definition of consistent numerical thresholds across collection methods.15,16 This represents an important limitation that could also influence our findings.
Second, although NC did not correlate with sputum inflammation, it provided important complementary information suggesting epithelial involvement. The frequent presence of epithelial islets, squamous metaplasia, goblet cell hyperplasia, and excess mucus suggests active structural changes in the nasal mucosa of patients with SA. These features may be associated with worse outcomes and poorer therapeutic response. Lee et al evaluated the histopathology of sinus mucosa by evaluating the inflammatory cell count and tissue remodelling markers (squamous metaplasia, subepithelial gland proliferation, basement membrane [BM] thickening, stromal edema, and fibrosis).21 They demonstrated that tissue eosinophilia was commonly associated with BM thickening and stromal edema, while subepithelial gland proliferation predicted a poor surgical prognosis in CRS. These features also align with chronic T2 inflammation and impaired epithelial barrier function, both of which are key drivers of airway remodelling and disease severity.22 The association between epithelial islets and elevated blood eosinophils supports the link between systemic eosinophilic inflammation and upper airway remodelling. Similarly, the higher prevalence of goblet hyperplasia among patients with elevated FeNO points to a shared epithelial-cytokine axis across respiratory compartments. These epithelial changes, readily detectable under light microscopy, may reflect the ongoing epithelial–mesenchymal transition processes that sustain inflammation and mucus hypersecretion. In addition, the relatively higher frequency of mixed inflammatory patterns in nasal samples may point to more complex local interactions between T2 and non-T2 pathways at the nasal level. Although, we have not explored local TSLP in nasal or bronchial mucosa, the higher levels of TSLP in blood among patients with higher counts of eosinophils, could contribute to reinforce the importance of epithelial dysfunction in upper and lower airways.
Third, serum biomarker analysis suggested a systemic T2-inflammatory profile in patients with higher blood eosinophil counts, only periostin showed a statistically significant association. The rest of inflammatory markers evaluated, TSLP, DPP4, and total IgE showed upward trends, which should be interpreted cautiously given the limited sample size. The positive correlation between blood eosinophils and serum periostin further supports periostin as the most robust systemic biomarker identified in this cohort. Periostin, a matrix-protein secreted by epithelial and stromal cells, showed the strongest correlation with blood eosinophils, consistent with its role as a downstream product of IL-13-mediated epithelial activation reflecting a high T2 inflammation pathway. Periostin, has been linked to remodelling23 and associated with the T2-high endotype and persistent airflow obstruction in patients with severe asthma.24 More recently, it has been described that periostin expression is upregulated in nasal polyps and might determine a crucial role in the occurrence and evolution of the disease.25 Interestingly, serum DPP4 levels did not differ according to eosinophil status but were significantly higher in nasal samples with abundant mucus. DPP4 has been implicated as a regulator of airway epithelial function.26 Given that DPP4 is upregulated by IL-13 and associated with mucus production and epithelial responses,27 this finding suggests a mucus-dominant phenotype with epithelial activation that is not necessarily eosinophil-driven. This novel association warrants further investigation as a potential non-eosinophilic T2 pathway. However, although serum biomarkers are attractive due to their accessibility, their ability to accurately predict airway eosinophilia remains to be fully established and future studies with larger cohorts should evaluate the predictive performance of individual and combined biomarkers.
Taken together, these results support a model in which the nose and bronchi share common immunological pathways but may express them differently depending on local microenvironmental pressures. Nasal cytology therefore offers a window into epithelial dynamics and upper airway inflammation, but not a direct substitute for induced sputum in identifying eosinophilic asthma. Instead, it should be viewed as an additional, accessible tool that complements systemic biomarkers and sputum analysis, particularly in centres where sputum induction is unavailable.
Several factors may have influenced the lack of concordance between nasal and sputum inflammation. Because BRISA was an exploratory study, the number of included patients is small, and our findings require further validation in larger populations. Moreover, many patients had been receiving high-dose ICS for a prolonged period, which may reduce lower airway eosinophilia28 more effectively than upper airway inflammation due to differences in deposition and tissue penetration. Moreover, the adherence to intranasal corticosteroids is at least, in many cases, suboptimal.29 A subset of patients also had chronic rhinosinusitis or nasal polyp disease, conditions that alter epithelial architecture and may introduce neutrophilic or mixed inflammatory patterns independent of asthma phenotype. An additional limitation is the incompleteness of some paired compartment data, particularly for analyses involving sputum and nasal variables, which restricted the scope of correlation analyses and prevented a more detailed evaluation. Of the initially recruited patients, only those with available paired data (nasal cytology, induced sputum, and/or serum biomarkers) were included in the corresponding analyses. Missing data were mainly due to technical limitations, insufficient sample quality, or inability to obtain induced sputum. Recruitment was severely affected by the COVID-19 pandemic, which hindered sputum induction due to biosafety restrictions. Moreover, consistent with other recent studies, with a success rate for the induced sputum in asthma close to 80%,30 the difficulty in obtaining valid induced sputum samples (22.7% invalid in our cohort) may have affected subgroup analyses and requires a former validation of our results in larger populations. Despite these constraints, the consistency of trends observed across different biomarkers (FeNO, IgE, periostin, and blood eosinophils) strengthens the internal validity of our findings. We should also acknowledge that the lack of additional non–T2 biomarkers, such as CRP or IL-6, limited the characterization of non-eosinophilic endotypes. We neither perform diagnostic performance analyses (eg, ROC curves or predictive modelling) due to the limited sample size and the presence of missing paired data across compartments, which could result in unstable estimates. Therefore, our findings should be considered exploratory and hypothesis-generating.
Despite these limitations, this study provides relevant insights. It confirms the feasibility and potential clinical value of nasal cytology as an inexpensive, minimally invasive method to assess epithelial changes and local inflammation in severe asthma. It highlights the incomplete overlap between upper and lower airway inflammation, supporting the need for multi-compartment assessment rather than reliance on a single biomarker. Finally, it identifies mechanistic signals, such as the association between nasal mucus-rich samples and DPP4 elevation, that may refine future biomarkers. Further research could explore the correlation of this finding with bronchial mucus production.
Conclusions
Induced sputum represents a useful tool for inflammatory phenotyping in patients with severe asthma. Nasal Cytology can serve as a useful complementary method informing about epithelial remodelling and upper-airway inflammatory patterns, although it does not replace induced sputum. In this exploratory cohort, serum periostin emerged as the most consistent systemic biomarker associated with blood eosinophilia, while other biomarkers showed only non-significant trends. Larger studies are warranted to validate these findings and clarify the potential role of multi-compartment assessment in severe asthma phenotyping.
Abbreviations
BEC, Peripheral Blood eosinophils count; IgE, Total Immunoglobulin E; IU, International Units; µg, micrograms; mL, millilitre; µL, microlitre; ng, nanograms; ECP, Eosinophilic Cationic Protein; DPP4, Dipeptidyl Peptidase-4; TSLP, Thymic Stromal Lymphopoietin.
Acknowledgments
The authors acknowledge Itsaso Losantos and the biostatisticians team for their contribution to the statistical analysis and AstraZeneca Spain for funding the project without any influence on the results.
Disclosure
SQ has been on advisory boards for and has received speaker’s honoraria from Allergy Therapeutics, AstraZeneca, Chiesi, GlaxoSmithKline, Gebro, Sanofi and Stallergenes. JAC reports receiving payments for lectures and/or educational events from AstraZeneca and GSK. JAC reports receiving research grant support from AstraZeneca. JD-O reports personal fees from AstraZeneca, personal fees from GSK, personal fees from Sanofi-Regeneron, personal fees from Celtrion, personal fees from Chiesi, personal fees from LETI-Pharma, personal fees from Menarini, outside the submitted work. GL-Z has nothing to disclose. IG-M reports grants, personal fees from GSK, grants, personal fees from AstraZeneca, grants, personal fees from Sanofi-Genzyme, outside the submitted work. MV-M reports personal fees from GSK, personal fees from Roxall, outside the submitted work. LDlV reports personal fees from GSK, Astra Zeneca, Sanofi, outside the submitted work. The authors report no other conflicts of interest in this work.
References
1. 2025 GINA severe asthma guide. Global Initiative for Asthma - GINA. Available from: https://ginasthma.org/2025-gina-severe-asthma-guide/.
2. D’Amato M, Pastore D, Lupia C, et al. Biologic therapy in severe asthma: a phenotype-Driven and Targeted Approach. J Clin Med. 2025;14(13):4749. doi:10.3390/jcm14134749
3. Perez-de-Llano L, Scelo G, Tran TN, et al. Exploring definitions and predictors of severe asthma clinical remission after biologic treatment in adults. Am J Respir Crit Care Med. 2024;210(7):869–11. doi:10.1164/rccm.202311-2192OC
4. Shackleford A, Heaney LG, Redmond C, McDowell PJ, Busby J. Clinical remission attainment, definitions, and correlates among patients with severe asthma treated with biologics: a systematic review and meta-analysis. Lancet Respir Med. 2025;13(1):23–34. doi:10.1016/S2213-2600(24)00293-5
5. Guida G, Bagnasco D, Carriero V, et al. Critical evaluation of asthma biomarkers in clinical practice. Front Med. 2022;9:969243. doi:10.3389/fmed.2022.969243
6. Caballero M, Dominguez-Ortega J, Nin-Valencia A, Sánchez-Ocando H, Barranco P. Eosinophil count could be more sensitive in induced sputum than in peripheral blood for phenotyping of patients with severe eosinophilic asthma. J Investig Allergol Clin Immunol. 2021;31(4):360–361. doi:10.18176/jiaci.0647
7. Zhang F, Wang H, Wang W, et al. Induced sputum: current progress and prospect. Eur J Med Res. 2025;30(1):795. doi:10.1186/s40001-025-02974-w
8. Marcuccio G, Raffio G, Ambrosino P, et al. The potential role of nasal cytology in respiratory diseases: clinical research and future perspectives. J Clin Med. 2025;14(3):884. doi:10.3390/jcm14030884
9. Gelardi M, Iannuzzi L, Quaranta N, Landi M, Passalacqua G. NASAL cytology: practical aspects and clinical relevance. Clin Exp Allergy. 2016;46(6):785–792. doi:10.1111/cea.12730
10. Scadding GK, Durham SR, Mirakian R, et al. BSACI guidelines for the management of allergic and non-allergic rhinitis. Clin Exp Allergy. 2008;38(1):19–42. doi:10.1111/j.1365-2222.2007.02888.x
11. Blanco-Aparicio M, Domínguez-Ortega J, Cisneros C, et al. Consensus on the management of united airways disease with type 2 inflammation: a multidisciplinary Delphi study. Allergy Asthma Clin Immunol. 2023;19(1):34. doi:10.1186/s13223-023-00780-9
12. De Farias CF, Amorim MMF, Dracoulakis M, Caetano LB, Santoro IL, Fernandes ALG. Nasal lavage, blood or sputum: which is best for phenotyping asthma? Respirology. 2017;22(4):671–677. doi:10.1111/resp.12958
13. De Corso E, Corbò M, Montuori C, et al. Blood and local nasal eosinophilia in chronic rhinosinusitis with nasal polyps: prevalence and correlation with severity of disease. Acta Otorhinolaryngol Ital. 2025;45(1):39–46. doi:10.14639/0392-100X-N2877
14. Hargreave FE, Pizzichini E, Pizzichini M. Induced sputum examination. J Allergy Clin Immunol. 1998;101(4 Pt 1):569–570. doi:10.1016/s0091-6749(98)70370-7
15. Deutschle T, Friemel E, Starnecker K, Riechelmann H. Nasal cytologies--impact of sampling method, repeated sampling and interobserver variability. Rhinology. 2005;43(3):215–220.
16. Lin RY, Nahal A, Lee M, Menikoff H. Cytologic distinctions between clinical groups using curette-probe compared to cytology brush. Ann Allergy Asthma Immunol. 2001;86(2):226–231. doi:10.1016/S1081-1206(10)62696-8
17. Bartoli ML, Cristofani-Mencacci L, Scarano M, et al. Nasal cytology: a comparative study of two different techniques of processing—smeared versus cytocentrifuged slides. Mediators Inflamm. 2018;2018:1640180. doi:10.1155/2018/1640180
18. Gilani S, Bhattacharyya N. Rethinking the relationships between chronic rhinosinusitis and asthma severity. Am J Otolaryngol. 2023;44(3):103814. doi:10.1016/j.amjoto.2023.103814
19. van BGJ, Said H, van HMA, Bogaert D. The respiratory microbiome in childhood asthma. J Allergy Clin Immunol. 2023;152(6):1352–1367. doi:10.1016/j.jaci.2023.10.001
20. Tan LH, Lin C, Ungerer H, et al. Steroid affected cytokines in aspirin-exacerbated respiratory disease. Int Forum Allergy Rhinol. 2022;12(10):1232–1241. doi:10.1002/alr.22977
21. Lee HY, Pyo JS, Kim SJ. Distinct Patterns of tissue remodeling and their prognostic role in chronic rhinosinusitis. ORL. 2021;83(6):457–463. doi:10.1159/000515005
22. Petalas K, Goudakos J, Konstantinou GN. Targeting epithelium dysfunction and impaired nasal biofilms to treat immunological, functional, and structural abnormalities of chronic rhinosinusitis. Int J Mol Sci. 2023;24(15):12379. doi:10.3390/ijms241512379
23. Hoshino M, Ohtawa J, Akitsu K. Association of airway wall thickness with serum periostin in steroid-naive asthma. Allergy Asthma Proc. 2016;37(3):225–230. doi:10.2500/aap.2016.37.3945
24. Bobolea I, Barranco P, Del Pozo V, et al. Sputum periostin in patients with different severe asthma phenotypes. Allergy. 2015;70(5):540–546. doi:10.1111/all.12580
25. Danielides G, Lygeros S, Kyriakopoulos G, et al. Serum and tissue periostin expression in rhinosinusitis with nasal polyps. Am J Rhinol Allergy. 2025;39(4):259–265. doi:10.1177/19458924251332546
26. Zhang T, Tong X, Zhang S, et al. The roles of dipeptidyl peptidase 4 (DPP4) and DPP4 inhibitors in different lung diseases: new evidence. Front Pharmacol. 2021;12:731453. doi:10.3389/fphar.2021.731453
27. Emson C, Pham TH, Manetz S, Newbold P. Periostin and dipeptidyl peptidase-4: potential biomarkers of interleukin 13 pathway activation in asthma and allergy. Immunol Allergy Clin North Am. 2018;38(4):611–628. doi:10.1016/j.iac.2018.06.004
28. Rial M, Betancor D, Cañas J, et al. Stability of asthma phenotypes in the Spanish cohort of the MEGA project. J Investig Allergy Clin Immunol. 2025;35(1):53–55. doi:10.18176/jiaci.1026
29. Villamañán E, Laorden D, Ibáñez ME, et al. Adherence to intranasal corticosteroids in patients with severe asthma and nasal polyposis: pharmacological and clinical factors Involved. J Clin Med. 2025;14(14):5070. doi:10.3390/jcm14145070
30. Moermans C, Schleich F, Gerday S, et al. The success rate and safety of induced sputum is better than you think: give it a try! ERJ Open Res. 2025;11(3):00871–02024. doi:10.1183/23120541.00871-2024
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.