Back to Journals » International Journal of Women's Health » Volume 18
A Longitudinal Qualitative Study on the Perioperative Symptom-Demand Journey Map of Patients with Cervical Cancer
Authors Zhang Y, Wu Y, Yuan J, Yang J, Zhu W, Chen L, Xu C
Received 13 February 2026
Accepted for publication 11 May 2026
Published 21 May 2026 Volume 2026:18 603381
DOI https://doi.org/10.2147/IJWH.S603381
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Vinay Kumar
Yuting Zhang,1 Yaru Wu,1 Jing Yuan,1 Juan Yang,1 Wei Zhu,2,3 Ling Chen,2,3 Chunyan Xu2,3
1School of Nursing, Xinjiang Medical University, Urumqi, Xinjiang, People’s Republic of China; 2Department of Gynecological Surgery, Affiliated Tumor Hospital of Xinjiang Medical University, Urumqi, Xinjiang, People’s Republic of China; 3Health Care Research Center for Xinjiang Regional Population, Urumqi, Xinjiang, People’s Republic of China
Correspondence: Chunyan Xu, Email [email protected] Ling Chen, Email [email protected]
Background: This longitudinal qualitative study explored dynamic changes in symptoms and evolving needs among perioperative cervical cancer patients. Findings were intended to support the development of targeted perioperative nursing interventions for this population.
Methods: Using a purposive sampling approach and Maslow’s hierarchy of needs as the theoretical framework, 14 cervical cancer patients were recruited from a gynecology center at a university hospital in Northwest China. Semi-structured interviews were conducted at three stages: 1– 2 days before surgery, 1– 3 days after surgery, and before discharge, between April and June 2025. A longitudinal qualitative design was applied for data analysis, and a patient journey map was developed.
Results: (1) Six themes emerged: impacts of disease and surgery on physiological needs; worries about medical safety and prognosis; disruptions to intimate and social relationships; diminished self-worth; coexistence of information demand and overload; and redefined life meaning through illness. (2) A perioperative symptom-needs journey map was constructed, with time as the horizontal axis and five core dimensions (goals, symptoms, needs, emotions, key personnel) as the vertical axis. (3) It visualized dynamic symptoms, contributing factors and evolving needs across the three stages.
Conclusion: Perioperative symptoms in cervical cancer patients are complex and multi-factorial, with needs across physiological, safety, esteem, cognitive and self-actualization domains changing dynamically. Healthcare providers should monitor these variations, implement individualized symptom management, meet stage-specific care needs, and improve patients’ symptom experience and prognosis.
Keywords: cervical cancer, perioperative period symptoms, Maslow’s hierarchy of basic human needs, longitudinal qualitative study, patient journey mapping
A Letter to the Editor has been published for this article.
Introduction
As a prevalent malignancy, cervical cancer remains a critical threat to women’s reproductive health worldwide.1 Its substantial global burden is reflected in high incidence and mortality rates; Notably, China reported over 150, 000 new cases in 2022, the highest global incidence.2,3 Surgery, the cornerstone of treatment for early-stage cervical cancer, achieves favorable outcomes with a 5-year survival rate exceeding 90%.4 However, while surgical treatment improves prognosis, it compromises reproductive system integrity and triggers a series of perioperative symptoms, including fatigue, pain, anxiety, and gastrointestinal dysfunction, thereby exerting multifaceted impacts on postoperative rehabilitation.5,6
According to Maslow’s Hierarchy of Needs Theory,7 physical symptoms primarily impair patients’ physiological needs. When these basic needs are unmet, individuals struggle to pursue higher-level needs such as safety, love, and belonging. Persistent symptoms may further delay the fulfillment of lower-level needs, hindering the achievement of advanced needs including social interaction and self-actualization. Therefore, clinical nursing should not only perform dynamic assessment and targeted intervention for physical symptoms but also monitor the changes in patients’ hierarchical needs from physiology to self-actualization. To better track the dynamic evolution of perioperative symptoms and needs, this study employed Patient Journey Mapping (PJM). This approach visually depicts patients’ care trajectories, systematically capturing their experiences, changing needs, and emotional fluctuations throughout the care continuum,8,9 and helps identify service gaps and critical intervention time points.10 Its value has been confirmed in a qualitative study of Chinese cervical cancer patients undergoing radiotherapy.11 However, most existing studies on cervical cancer focus on patients undergoing chemo-radiotherapy or follow-up, relying predominantly on cross-sectional designs that assess complications or psychological status at a single time point. Although such studies provide preliminary evidence, they lack continuous longitudinal tracking across the preoperative, intraoperative, and postoperative phases. Compared with patients with other malignancies such as breast cancer, those with cervical cancer frequently bear unique psychosocial burdens related to femininity, fertility, and gender identity.12 These issues are especially prominent during the perioperative period yet are often neglected by healthcare providers.
Quantitative research can estimate the prevalence of symptoms and needs but fails to capture subjective experiences and individual heterogeneity. Similarly, cross-sectional designs cannot illustrate their temporal evolution. Therefore, guided by Maslow’s Hierarchy of Needs Theory,7 this longitudinal qualitative study13 aims to explore symptom experiences and dynamic changes in needs among perioperative cervical cancer patients, develop a tailored symptom management journey map, and provide evidence for optimizing perioperative nursing care.
Objects and Methods
Research Subject
This study employed a purposive sampling method, adhering to the principle of maximizing difference, “to select cervical cancer patients who underwent radical total hysterectomy at the Gynecological Center, a Grade A Tertiary Specialized Cancer Hospital in Northwest China between April 2025 and June 2025. With the patients’ voluntary and informed consent, semi-structured interviews were conducted. The sample size was determined based on the core principle of information saturation”, resulting in the selection of 14 patients.
Inclusion criteria included: ① Patients diagnosed with cervical cancer scheduled for “laparoscopic total hysterectomy+bilateral adnexectomy (and/or) pelvic lymph node dissection”, classified as clinical stage T1-T2, and without lymph node or distant metastasis; ② Individuals aged≥18 years, possessing clear consciousness and the ability to cooperate with the interview; ③ Absence of significant family events, aside from the patient’s illness, that could affect the patient’s mood; ④ Participants provided voluntary informed consent to participate in this study and to allow the publication of anonymized responses and direct quotations.
Exclusion criteria include the following: ① Presence of other serious diseases or malignant tumors, cognitive impairment, or mental disorders; ② Occurrence of severe complications (such as massive hemorrhage) during or after the surgery that preclude follow-up; ③ Participation in similar research studies.
Ethical Considerations
This study protocol has been meticulously reviewed and unanimously approved by the Medical Ethics Committee of the Affiliated Cancer Hospital of Xinjiang Medical University (approval number: K-2024218). The review process adhered strictly to the standards set forth in the Reporting Qualitative Research (SRQR). Prior to their participation, all study participants provided informed consent.
Qualitative Research Methods
This study was conducted with patients through semi-structured interviews. The research method integrates qualitative approaches with a longitudinal design, enabling an in-depth understanding of an individual’s experiences or behaviors over time, characterized by the concept of “time-change”.14
Based on the research objectives and the preliminary investigation on perioperative symptom changes in cervical cancer patients conducted by the research team, the average length of hospital stay for patients at this Gynecological Center was 11 days, with 75.08%of them staying for≤7 days. Therefore, interviews were carried out from the time patients confirmed their surgery to before their discharge, with the specific time points as follows: (1) 1–2 days before surgery: This period is the patients’ “preoperative preparation phase”. Having confirmed the surgery time and basic procedures but not yet experienced surgical trauma, patients can truly reflect their initial perceptions and concerns about the surgery, which provides baseline information for the journey map; (2) 1–3 days after surgery: This period is the patients’ postoperative “acute recovery phase”, during which patients experience the most prominent postoperative physical symptoms and psychological fluctuations, making it the stage where symptoms and needs are the most concentrated and urgent; (3) Before discharge: This period is the critical “transitional phase” for patients who have completed postoperative recovery treatment and are about to enter home-based rehabilitation or adjuvant therapy. Their focus shifts from “relief of acute-phase symptoms” to “post-discharge rehabilitation management”, which can reflect their concerns and needs regarding the transition from hospital to home and provide a basis for designing management measures for the “post-discharge rehabilitation phase” of the journey map.
The duration of each interview was kept within 30 minutes as much as possible. To ensure comprehensive data collection, if any aspects of the initial interview records remain ambiguous or unclear after transformation and organization, a follow-up interview must be conducted. Prior to the interview, it is essential to establish a trusting relationship with respondents, inform them of the researcher’s identity and purpose, respect the patients’ wishes, and obtain their signatures on the informed consent form.
Data Collection and Interview Outline
Following a literature review and group discussions, an interview outline was developed using Maslow’s hierarchy of basic needs as the theoretical framework. This outline encompassed three time points and six dimensions. Two patients were recruited for pilot interviews, and the interview outline was revised based on the issues identified during the interviews and finalized thereafter5,7,13 (Table 1).
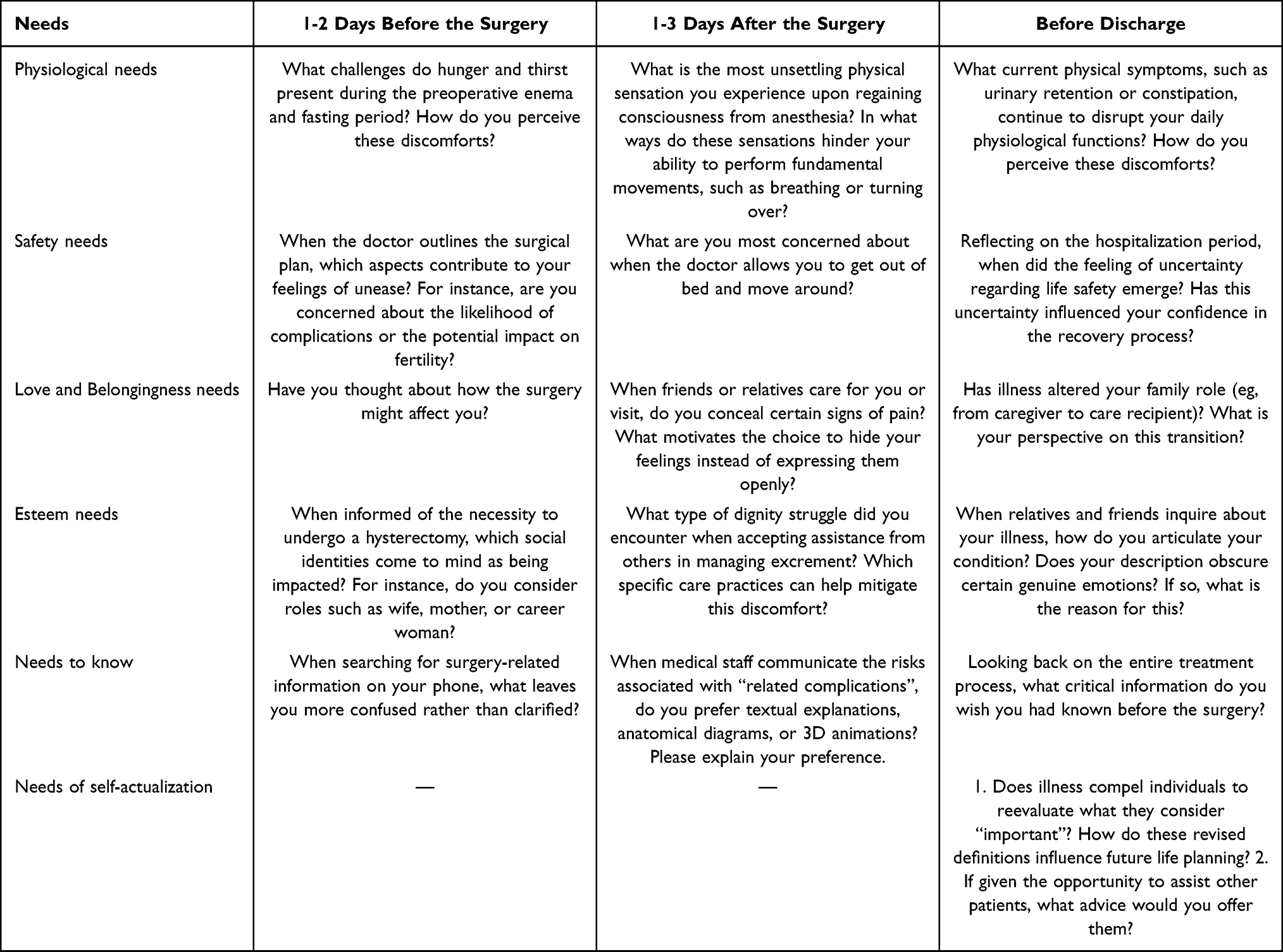 |
Table 1 Interview Outline Based on Maslow’s Hierarchy of Needs |
Although Maslow’s hierarchy of needs provides a clear framework for understanding patient needs, it has been criticized for cultural bias and its rigid linear progression. In this study, we flexibly applied the framework to guide and organize thematic content, allowing for overlapping needs while taking into account participants’ real experiences, Chinese cultural values, and the unique perioperative experiences of cervical cancer patients. For readability, results are presented in the original theoretical order. All interviews were conducted face-to-face by the same researcher. The interview location was chosen as either the gynecological examination room or an individual ward based on the patients’ preferences, with only the patient and the researcher present. Upon obtaining the patient’s consent, audio recordings were made, and non-verbal information was documented. Any uncertainties were clarified and confirmed with the patients promptly. The interviews concluded when the data reached the saturation threshold for sample size information.15
Data Organization and Analysis
With Colaizzi’s seven-step analysis method as procedural guidance, a combined approach of synchronic analysis and diachronic analysis was adopted.16 With the assistance of Nvivo 14.0 and Excel, the sorting and synchronic analysis of the research data were conducted within 24 hours after the completion of interviews at each time point. After all data were collected, we conducted a diachronic analysis across the three time points to identify evolving patterns, from which core themes were subsequently extracted.17
To ensure the clarity and completeness of our interview data, we developed three assessment criteria for identifying ambiguous or unclear responses. This included: ① Missing key information relevant to the research topic; ② Contradictory or uncertain statements; ③ Responses only loosely related to the question. If, after two or more guidance attempts, the patient did not return to the topic, a follow-up interview was scheduled.
The interview data were independently coded by the interviewer and another postgraduate student who participated in the development of the interview outline. In case of discrepancies in coding opinions, the supervisor was involved in the adjudication to ensure the objectivity of the coding process. All interviews were audio-recorded and verbatim transcribed for documentation purposes, enabling full traceability and verification. Two graduate supervisors with experience in qualitative research (holding associate senior professional titles or above) in the research team participated in the review and analysis of the research data to mitigate the subjective bias arising from a single researcher.
Construct the Patient’s Journey Map
By synthesizing longitudinal interview data and utilizing the three designated time points from the interviews, we categorized the symptoms and needs that emerged at each stage. The interview times served as the horizontal axis, where we plotted the primary medical tasks, significant symptoms, and major challenges faced by patients at various intervals during the perioperative period. Subsequently, we aligned the reasons for changes in needs and emotions, along with the key individuals influencing these changes, with each time point. The journey map was completed using PowerPoint to visually present the findings. Researchers can review the perioperative experiences with patients during follow-up visits, engage in discussions, and refine the map content according to thematic data categories, thereby ensuring the map’s completeness and authenticity.
Results
General Patient Information
A total of 17 patients participated in the study, of which 14 were ultimately included (Table 2). A total of 14 patients completed the interviews in full and were finally included in the study, with 51 interviews conducted among these 14 patients. Among them, two patients coded as N1 and N2 were the pilot interview participants, and supplementary interviews were conducted with both of them after the revision of the interview outline. N8 rescheduled her second interview as she had to leave temporarily for routine postoperative examinations. N10 and N13 suspended their interviews at T3 due to emotional distress and completed their second interviews after regaining stability.
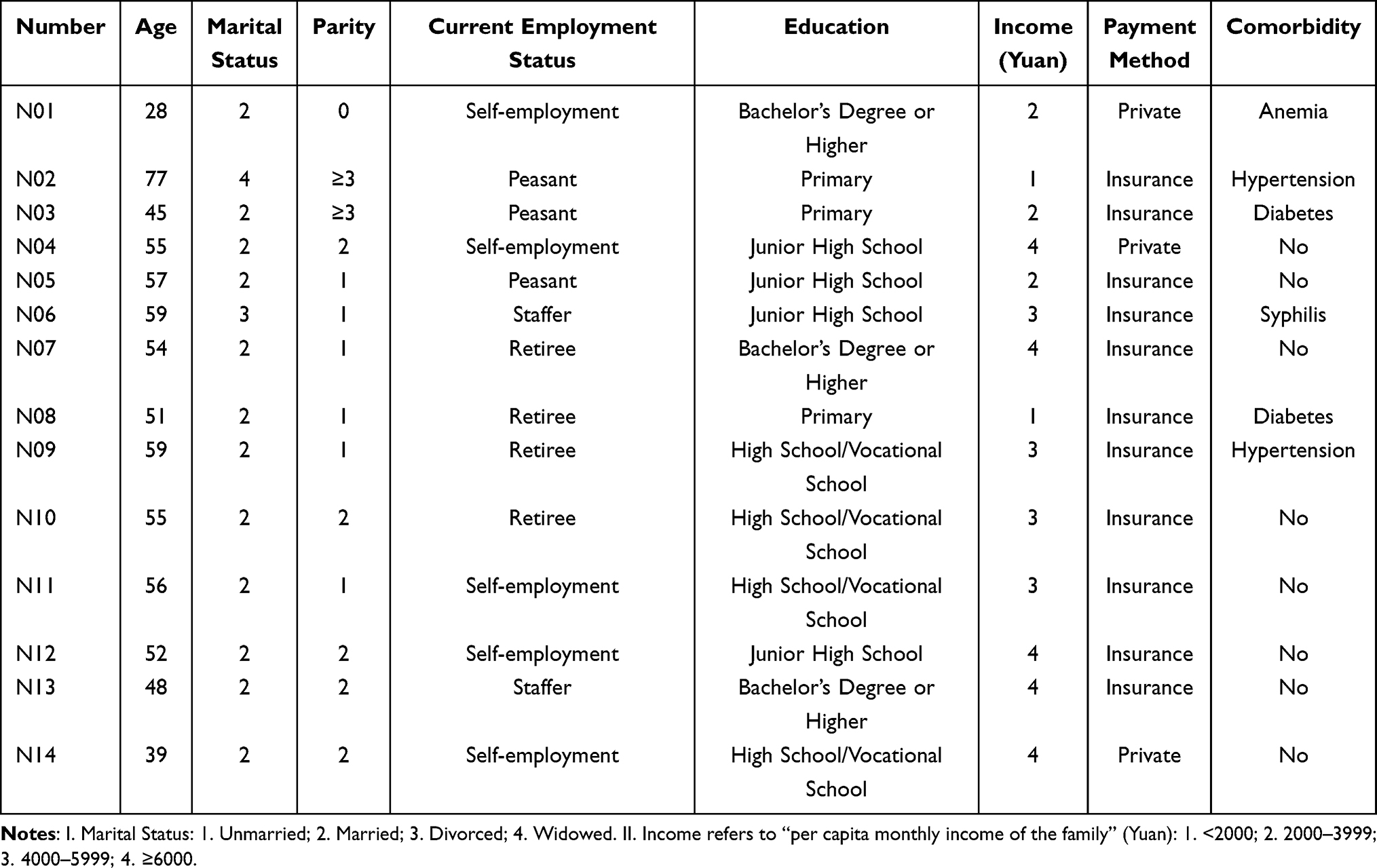 |
Table 2 Interviewee Demographics (N=14) |
Theme
(1) Physiological needs: The influence of diseases and surgical procedures on physiological needs. The patient’s most pressing need prior to surgery is to undergo the procedure to eliminate the potentially life-threatening risks associated with the disease. Once the postoperative threat is mitigated, physiological needs, including pain management and dietary considerations, become the primary focus. During the interviews, all patients stated that they could tolerate the hunger and thirst caused by preoperative enema and fasting, and accepted such physical discomfort as a necessary preparatory procedure for surgery, with no unusual distress. However, several patients expressed dissatisfaction with the preoperative preparations. N01 stated, “This is beneficial for the surgery. Not eating or drinking after 12 o’clock is actually fine. You can resume your diet once you have ventilation later”. N14 remarked, “It’s just hunger and thirst. I don’t take it seriously. If I’m really uncomfortable, there’s still a doctor who can give me an intravenous drip. It won’t lead to hypoglycemia due to hunger. These are all necessary before the surgery”. Two patients reported that the uncertainty surrounding the duration of the surgery, along with the discomfort stemming from hunger and thirst, contributed to negative experiences. N11 expressed, “Getting sick has already driven me crazy, and I still have to go hungry to prepare for the surgery”. Although these measures were intended to facilitate the smooth progress of the procedure, the patient still felt considerable self-pity. In the two interviews conducted after the surgery and prior to discharge, the patients’ symptom experiences evolved from urgent issues requiring immediate attention, such as pain, abdominal distension, and chest tightness, to more chronic concerns, including abnormal sensations in the groin area, constipation, and restricted movement due to the urinary catheter. Notably, the symptoms of insufficient sleep persisted throughout the entirety of the interviews.
(2) Safety needs: Concerns regarding medical safety and uncertainty about prognosis. During the perioperative period, the patient experienced a fluctuation and overlap between physical and psychological safety. Analysis suggests that negative emotions, including anxiety and fear stemming from surgical risks or potential postoperative complications, heighten patients’ urgent need for psychological safety prior to surgery. Once postoperative patients are able to get out of bed and ambulate, they typically perceive that they have navigated the critical period. At this stage, their focus shifts to the risk of accidental injuries, such as falls and incision pain, that may occur upon mobilization. Prior to discharge, reflecting on the entire hospitalization period, if a patient’s needs regarding symptom management or care activities are not addressed promptly, they may perceive a threat to their safety, which can undermine their confidence in recovery. For instance, N04 expressed discomfort, stating, “This drainage tube is uncomfortable. It hurts as soon as I move it. No one told me how to manage it either. Wouldn’t it be even more troublesome if it became inflamed? I believe this has affected my confidence in recovery. I’m afraid I won’t recover well and will have to endure more complications”. Conversely, another patient N11 reported, “As soon as I can’t see the doctor in the ward, I feel anxious. Whenever I feel unwell, I’m afraid I won’t recover properly”. Only N05 explicitly stated that her smooth recovery had greatly relieved the financial burden on her family. This perspective suggests that patients’ safety needs extend beyond medical concerns. A favorable postoperative prognosis can reduce family financial worries and strengthen their overall sense of security. Unlike most participants focused on surgical risks, a few patients like N05 emphasized financial security, reflecting individual differences in perioperative safety needs.
(3) Love and belongingness needs: The impact of illness on intimate relationships and social interactions. Throughout the preoperative period and up to discharge, patients have engaged in varying degrees of reflection regarding the unknown consequences of their illness. More than half of the patients primarily consider their family roles and express a desire to maintain their original positions within the family structure. Five patients acknowledged that surgical treatment might lead to changes prior to the surgery, yet they did not explore these implications in depth. The remaining patients, viewing their situations through the lenses of their grandmothers, mothers, wives, and daughters, express concern that changes in their roles may impose burdens on their families. N05: “My husband is not in good health. I used to care for him constantly, but now he comes to the hospital to be with me every day. I simply wish to recover soon and return to normal life. This situation also impacts my son’s ability to find a partner”. N06: “If I die, the girl will have no mother. I cannot allow that to happen”. N07: “Recently, my husband and son have been diligently caring for me, which has delayed their recent exams. I feel a profound sense of guilt”. N01: “I do not want my parents to worry. As soon as I returned from surgery, I quickly moved my hands and feet, battling against the illness and my own limitations. I refuse to feel useless”. After the surgery, when confronted with care or visits from relatives and friends, many patients choose to conceal certain painful manifestations to protect their families and maintain existing social relationships. N06: “To be honest, I no longer want to be looked down upon. I can live well independently”. N13: “I still do not want everyone to worry”. N14: “I dare not think about it. I feel that as a woman, I am incomplete”. Prior to discharge, the patient’s temporary alteration of family role due to illness resulted in varying degrees of psychological conflict, imposing economic, social, and psychological burdens on the family. N03: “I feel like I am causing trouble for my child and adding to the family’s financial burden, yet I am powerless to change the situation”.
(4) Esteem needs: The deprivation of self-worth due to illness. The dual impact of a cervical cancer diagnosis and its surgical treatment often force patients to confront a profound loss of self-worth. Patients’ views were mainly reflected in three aspects: fertility, caring for the next generation, and sharing the family financial burden. These perspectives are highly consistent with those in Erikson’s Theory of Psychosocial Development,7,18 this life stage is typically centered on nurturing the next generation and achieving personal accomplishments. The illness and consequent hysterectomy can severely disrupt these core tasks, damaging the patient’s self-identity. Representative views are as follows: N01: “For me and my newly formed family, the surgery deprived me of the opportunity to become a mother”. N03: “The cancer delays my farm work, and I also need my school-aged children to care for me”. N04: “my daughter-in-law has just had a baby and needs care. And here I am, as the mother-in-law, feeling like a burden more than anything”. N06: “I love my job and maintain a good relationship with my colleagues. When my boss learned of my illness, he promptly granted me leave to seek proper medical attention and assured me that my position would be held”. Only one patient believed that the removal of the uterus did not affect her social status. N02: “At my age, I already have great-grandchildren. There is no impact at all”. Furthermore, some patients expressed a deep sense of “shame” about their condition, often refusing visits from concerned relatives and friends to avoid difficult questions, indicating how the disease itself can be internally stigmatizing.
(5) Needs to know: The dual phenomena of information hunger and information overload. Patients’ needs for knowledge varied, with not all experiencing intense information thirst or overload. During the perioperative period, the strongest drive for information was closely tied to “safety-related information”. When patients lacked essential knowledge about the surgery, what to expect afterward, or how to manage recovery, they actively sought information-a behavior that can be understood as a compensatory response to unmet safety or physiological needs. By gathering relevant details from medical staff, they aimed to reduce uncertainty and regain a sense of control. N02: “I have a heart condition. Among the risks associated with anesthesia are respiratory and cardiac arrest. Am I at an increased risk for these complications?” N11: “It is stated that lymph node dissection will be performed during the surgery. How will this procedure effectively clear and rapidly remove cancer cells? Is there a possibility of recurrence?” Patients were also particularly eager for explanations about new postoperative symptoms. When experiencing issues like abdominal distension or constipation, they often turn to clinicians for clarity. N03: “Whenever I lift my leg or walk, I experience numbness in my thigh. I am so afraid of falling that I hesitate to walk. What could be causing this? How long will it take to improve?” N06: “My abdomen is so bloated that it causes more pain than my surgical wound. I feel compelled to eat. What foods can I consume to alleviate this discomfort?” Notably, six patients described feeling information hunger before surgery. Some of them actively looked up information but had difficulty filtering what was useful, which led to a sense of overload-a finding consistent with the work of Zhang Zuxue et al.19
The interviews also revealed that over half of the patients felt overwhelmed by the amount of information they received after their cancer diagnosis-often more than they could meaningfully process. For instance, being confronted with numerous technical terms at once made it difficult for them to translate this information into practical knowledge, ultimately leading to a sense of information overload. We suggest that this reflects a form of overload driven by what might be called “compulsive information assimilation”-where patients feel pressured to absorb information despite feeling unable to manage it. As several participants expressed: “I’m scared. The more I search, the more scared I become”, and “I don’t really understand it either. I’ll just leave it to fate and follow whatever the doctors say”. When patients did seek out information on their own, their inquiries generally fell into four main categories: hormonal and bodily changes, postoperative pathology, effects on marital life, and postoperative complications and causes of recurrence.
In the later stages of the interview, it became evident that patients preferred an educational approach that combined textual explanations with animations; However, insufficient time was allocated for them to fully absorb the information. As a result, patients were susceptible to information overload. For instance, one patient (N09) remarked, “Animations are more intuitive, and text is convenient to read at any time. However, if you talk too much and can’t digest it, it will make you feel dizzy”. Prior to discharge, an interview was conducted to review the entire treatment process. Patients who initially exhibited no clear need for information unexpectedly developed a desire for knowledge as symptoms emerged. At this stage, their inquiries predominantly centered on postoperative complications, daily living, dietary considerations, exercise guidance, and care precautions for concurrent chronic conditions. This represents a significant shift from the preoperative mindset of most patients, who “did not search and just accepted it as it was”.
(6) Needs of self-actualization: The reshaping of the meaning of life through disease experiences. Most interviewees assume the roles of “mother-in-law, mother, wife, and daughter” simultaneously, with their value priorities predominantly centered on family members. Only three patients explicitly emphasized the necessity of attending to their own needs. For instance, N04 stated, “It is most important for oneself to be well. If I can take the doll, I will; if not, they will manage on their own. The most important thing is that I feel comfortable myself”. N08: “I consider myself to be of greater importance”. It is essential to adhere to the doctor’s recommendations, prioritize recovery, and allow for adequate rest. This illness did not manifest overnight; it requires gradual changes over time. In fact, I postponed addressing it until it progressed to cancer”. N14: “I believe I should focus more on myself”. While I do not have specific plans, I recognize the importance of being kind to myself, prioritizing my own needs, and living for my own sake. During the Q&A session on “offering advice or words to fellow patients”, participants expressed not only recurring sentiments of shared experience and helplessness, such as “we share the same illness” and “individual joys and sorrows differ”, but also frequent positive suggestions, including “There is always a solution to every problem; do not give up, maintain a positive attitude”, and “Schedule regular check-ups, take care of your health, and collaborate with medical professionals”. Simultaneously, three patients, including N12, expressed, “There’s nothing I can offer. I’ll treat it as I please”, indicating their current inability to continue assisting others. These patients remain in a state of anxiety regarding their illness and experience significant exhaustion.
Journey Process Drawing
This section delves into the intrinsic connections within the interview content to construct a map of the symptom management journey for perioperative patients. The three time points of the perioperative interview serve as the horizontal axis, while the patient journey map is organized along the vertical axis according to five dimensions: key objective, predominant symptom and greatest concern, needs, emotions, and key personnel.20 By integrating Maslow’s hierarchy of needs with the characteristics of symptom changes, we visually represent the perioperative symptom management of cervical cancer patients. The perioperative symptom management journey map for patients with cervical cancer is illustrated in Figure 1.
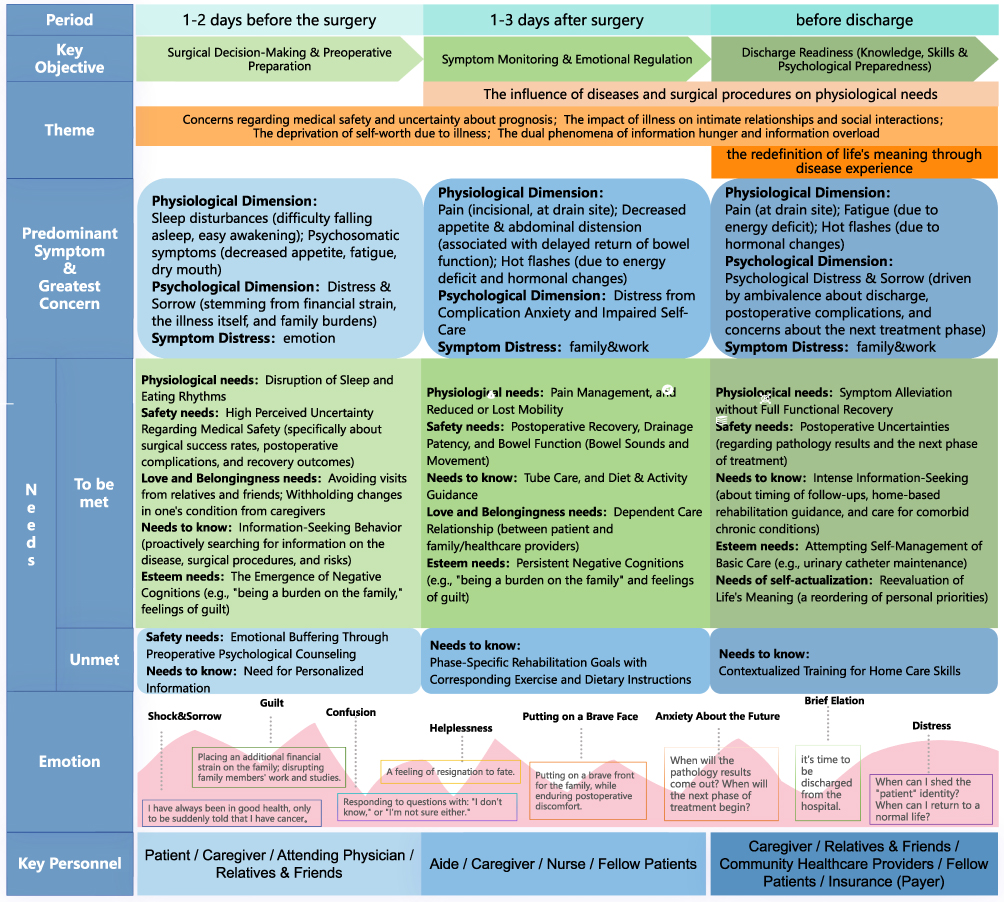 |
Figure 1 Symptom and Need Journey Map of Cervical Cancer Patients During the Perioperative Period. Note: Bold text is used only to distinguish headings from main content. |
Discussion
Core Findings and Innovations Regarding Perioperative Symptoms and Needs of Cervical Cancer Patients
By developing the perioperative symptom-need journey map for cervical cancer patients, this study confirms that similar perioperative symptoms exist across different cancer types and also identified the unique demand patterns of cervical cancer patients arising from the anatomical location of the disease and their sociocultural attributes. The specific findings are as follows:
First, certain similarities exist in how symptoms shape patients’ needs across different disease groups. Similar to patients undergoing breast cancer surgery and spinal surgery,21,22 cervical cancer patients are also dominated by physical symptoms such as pain and sleep disorders during the acute postoperative phase (1–3 days), with their core needs focusing on the physiological level (eg, pain management, activity guidance). Meanwhile, the prevalent anxiety and fear regarding surgical safety and prognosis during the perioperative period constitute a common manifestation of unmet safety needs.23 Furthermore, patients generally experience a contradiction of “the coexistence of information hunger and overload”: they crave comprehensive information before surgery yet develop avoidance behavior after surgery due to the overwhelm caused by the complexity and overload of information. Such ambivalence is directly influenced by the dual impact of their physical discomfort and safety anxiety.24,25 Notably, while patients’ information-seeking needs change dynamically with the perioperative phases, their demand for core information such as key points and precautions for rehabilitation care remains consistently high, and the need for pre-discharge home care guidance is particularly prominent.26
Secondly, the distinctive symptoms and needs of cervical cancer patients are as follows: ① At the physiological level, besides the common symptoms, patients explicitly express concerns about the “physical sensations arising from reproductive function loss”, and this need is significantly different from that of patients with non-reproductive system cancers; ② At the level of belonging and love, the “sense of shame” caused by the disease is particularly prominent, and specifically impairs their intimate relationships and social interactions. Unlike the social distress experienced by breast cancer patients due to body image changes,27 the social avoidance of cervical cancer patients stems more from anxieties about disease stigmatization and postoperative sexual life, a concern rarely observed in patients with lung cancer, gastric cancer and other such malignancies;28,29 ③ At the level of self-actualization, the “reconstruction of life meaning” among cervical cancer patients is distinctive. Benefiting from the generally favorable prognosis of cervical cancer, their focus of reflection shifts from the “fear of cancer” before surgery to “rehabilitation and improvement of quality of life” before discharge, which stands in contrast to the earlier and more profound exploration of life meaning in patients with advanced cancers such as lung cancer.30
It was also observed in the study that some patients, due to insufficient knowledge reserve, not only easily experience emotional symptoms such as distress and sorrow, but are even more likely to make adverse decisions including refusing surgery and abandoning standardized treatment because of cognitive biases, which directly impairs their diagnosis and treatment outcomes and prognosis. Therefore, stepped health education should be implemented for different perioperative phases. In particular, a separate education model for patients and their caregivers can be adopted in the early postoperative phase, and knowledge delivery optimized on a needs-based basis, which is of great help in alleviating patients’ emotional somatization symptoms and improving the quality of perioperative nursing care.
Application and Barriers of the Perioperative Symptom and Need Journey Map for Cervical Cancer Patients
By means of the Patient Journey Mapping tool, the core application value of this study lies in integrating the dispersed data on patients’ symptoms and needs according to different perioperative phases and rendering them in a visual form. This not only enhances patients’ understanding of their own disease course and treatment compliance, but also integrates symptoms with needs, clarifies the specific causes of patients’ symptom experiences and changes in needs, and thus provides better guidance for clinical practice. On the one hand, the map fully integrates the symptom characteristics at the three key perioperative time points 1–2 days before surgery, 1–3 days after surgery and before discharge (such as preoperative anxiety, postoperative pain, and pre-discharge nursing-related confusion) with Maslow’s Hierarchy of Basic Needs, presenting the impact of symptoms on needs in a visual manner. This not only helps patients understand the changes in their own symptoms and needs and improve their treatment compliance, but also assists healthcare providers in predicting and quickly identifying key nursing time points, thereby optimizing nursing plans, implementing personalized interventions, and improving patient satisfaction.20
On the other hand, the development of the map has also identified potential optimization directions for perioperative nursing care: firstly, by sorting out the consistency between symptoms and needs, we can accurately locate intervention time points, thus providing a reference for precision nursing; secondly, communicate with patients and their family members in a timely and effective manner-while understanding the dynamic changes of patients’ needs and symptoms, guide family members and their caregivers to participate in the care process, which helps with the real-time adjustment of individual nursing plans and alleviates patients’ negative emotions. Therefore, the patient journey map not only provides a basis for clinical practice to develop phased nursing pathways, but also inspires ideas for subsequent nursing plans, such as implementing timely and phased health education, and developing family care participation plans and knowledge education programs. In this way, it offers theoretical and practical support for improving the quality of perioperative nursing care. However, there may be barriers to its clinical popularization: first, the development and dynamic update of the map require additional investment in time and training, which poses a challenge to clinical human resources; second, individual differences may result in the personalized journey maps not being fully consistent with the standard template, which demands nursing staff to have the judgment to apply the map flexibly.
Implications for Clinical Practice
First, stepped and needs-tailored health education may be considered to address patients’ core and urgent needs: ① Upon admission and 1–2 days preoperatively: Clear information regarding surgical procedures and safety could be provided to patients and their families to help alleviate anxiety related to medical safety. ② At 1–2 days postoperatively: Separate guidance may be delivered to patients and caregivers. For patients, emphasis could be placed on key physical symptoms such as pain management and early mobilization; for primary caregivers, basic care skills and important monitoring indicators may be introduced. ③ Before discharge: Written or digital home care checklists might be provided, focusing on recognition of abnormal symptoms, follow-up arrangements, and rehabilitation behaviors.
In addition, routine brief screening using scales for anxiety, pain, and related indicators may be implemented during the preoperative and early postoperative periods. Timely psychological support or referral to specialists could be considered for patients with moderate to severe symptoms.
Second, reproductive and sexual health care may be integrated into routine clinical communication to address the specific needs of patients with cervical cancer: ① Peer support groups could be organized preoperatively or postoperatively to facilitate experience sharing, normalize patients’ emotional experiences, assist them in developing more positive cognitive appraisals, encourage mutual support, and help preserve their sense of self-worth. ② Guidance on family communication may be offered to help families better understand patients’ psychological status and provide appropriate emotional support rather than unintentional pressure. ③ Before discharge, trained nurses or clinicians may proactively and sensitively initiate discussions about postoperative physical changes and resumption of intimate relationships, providing professional support to reduce the “silence” surrounding these topics.
Third, sustained care and consultation pathways following discharge may be established to support long-term rehabilitation and ongoing treatment: ① Before discharge or at the first follow-up visit, patients may be encouraged to participate in activities such as developing a “rehabilitation wish list” to help redirect their focus toward life reconstruction in the future. ② Ongoing monitoring of patients’ psycho-social adaptation and rehabilitation progress could be provided through regular telephone follow-ups or online support groups.
Limitations of the Study
Although this study tracked the changes in symptoms and needs of cervical cancer patients during the perioperative period and fully developed the patient journey map, it still has several limitations. First, the study was conducted in a single hospital, which only reflects the symptom and need trajectories of patients at this institution, thus limiting the generalizability of the findings; Next, the construction of the patient journey map was mainly based on patients’ subjective narratives. While this method allows for in-depth capture of experiences and meanings, it may also be influenced by individual recall bias and expressive differences. Especially for highly subjective topics such as “life meaning”, relying only on self-reports at a single time point may fail to fully reflect the full picture of symptom management and dynamic need changes. Future research may adopt a multicenter, prospective design and use mixed methods. While collecting patients’ subjective experiences, objective physiological indicators and multi-dimensional assessments from healthcare providers and caregivers can be included. Through triangulation, a more robust and generalizable symptom-need management model can be established.
Conclusion
Guided by Maslow’s Hierarchy of Needs Theory, this longitudinal qualitative study explored dynamic changes in symptom experiences and supportive care needs among patients with cervical cancer during the perioperative period. Six core themes were identified from interview data: physical impact, safety anxiety, social impact, changes in self-worth, information inconsistency, and reconstruction of life meaning. Based on these findings, a perioperative symptom and needs journey map was constructed with three key time points (preoperative, early postoperative, and pre-discharge phases) as the horizontal axis, combined with five dimensions: core tasks, symptom distress, needs, emotions, and key individuals. Using patient journey mapping, this study clarified the common patterns and unique characteristics of perioperative experiences among cervical cancer patients. The findings provide hypothesis-generating, stratified implications for nursing practice covering urgent to long-term and general to personalized care. Future studies are warranted to verify the effectiveness of such nursing strategies and explore digital applications of the journey map to better support clinical decision-making.
Ethical Approval
This study protocol has been meticulously reviewed and unanimously approved by the Medical Ethics Committee of the Affiliated Cancer Hospital of Xinjiang Medical University (approval number: K-2024218). The review process adhered strictly to the standards set forth in the Helsinki Declaration. Prior to their participation, all study participants provided informed consent.
Funding
This work was supported by “Tian shan Ying cai” high-level talent training program for medicine and health [Grant No. TSYC202301B161].
Disclosure
The authors report no conflicts of interest in this work.
References
1. Wang PY, Huang Q, Wang SD. Interpretation of key points of “global cancer statistics 2022”. Chin Clin J Thoracic Cardiovasc Surg. 2024;31(07):933–12. doi:10.7507/1007-4848.202405013
2. Bray F, Lavers Anne M, Sung H, et al. Global cancer statistics 202: GLOBOCANN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin. 2024;74(3):229–263. PMID: 38572751. doi:10.3322/caac.21834
3. Han B, Zheng R, Zeng H, et al. Cancer incidence and mortality in China 2022. J Natl Cancer Cent. 2024;4(1):47–53. doi:10.1016/j.jncc.2024.01.006
4. Ramirez PT, Robledo KP, Frumovitz M, et al. LACC trial: final analysis on overall survival comparing open versus minimally invasive radical hysterectomy for early-stage cervical cancer. J Clin Oncol. 2024;42(23):2741–2746. PMID: 38810208. doi:10.1200/JCO.23.02335
5. Zheng YY. Sinicization and clinical application of the perioperative module of gynecological malignant tumors of the Anderson symptom series scale. Chengdu University of Traditional Chinese Medicine; 2020.
6. Cui XY, Su J, Zhang J, et al. Study of perioperative symptom clusters and core symptoms in pati-ents with gynecological malignancies. J Nurs. 2024;39(08):33–38. doi:10.3870/j.issn.1001-4152.2024.08.033
7. Li XM. Fundamentals of Nursing: An Introduction.
8. Bulto LN, Davies E, Kelly J, Hendriks JM. Patient journey mapping: emerging methods for understanding and improving patient experiences of health systems and services. Eur J Cardiovasc Nurs. 2024;23(4):429–433. PMID: 38306596. doi:10.1093/eurjcn/zvae012
9. Wu H, Ren H, Chu S. Applications, challenges and strategies of patient journey maps in care transitions: a scoping review. J Adv Nurs. 2025;1–13. doi:10.1111/jan.70213
10. Yang YX, Wang JN, Tian L, et al. Application of patient journey map in health management of cancer patients: a scoping review. Chin Nurs Manag. 2020;25(8):1205–1210. doi:10.3969/j.issn.1672-1756.2025.08.016
11. Wang H, Zhang Y, Li X, et al. Understanding experiences and improvement needs of Chinese cervical cancer patients with external beam radiotherapy and 3D brachytherapy: a qualitative study using persona-driven journey maps. Eur J Oncol Nurs. 2025;78:102943. PMID: 40849975. doi:10.1016/j.ejon.2025.102943
12. Du YM, Liu L, Wang BH, et al. Meta-integration of disease experience in cervical cancer patients. General Nurs. 2024;22(6):1150–1155. doi:10.12104/j.iSSN.1674-4748.2024.06.038
13. Yang XX, Lv LM, Ren YY, et al. Research progress of health-related information self-report tool for patients with cervical Cancer. Chin J Pract Nurs. 2022;38(33):2631–2636. doi:10.3760/cma.J.c.n211501-20211116-03155
14. Smith Battle L, Lorenz R, Reangsing C, et al. A methodological review of qualitative longitudinal research in nursing. Nurs Q. 2018;25(4):e12248. PMID: 29926526. doi:10.1111/nin.12248
15. Li Z, Liu Y. Nursing Research Methods.
16. Nevedal AL, Ayalon L, Briller SH. A qualitative evidence synthesis review of longitudinal qualitative research in gerontology. Gerontologist. 2019;59(6):e791–e801. PMID: 30395232. doi:10.1093/geront/gny134
17. Chen LX, Zhou YX. Analysis of status of longitudinal qualitative research in nursing in China. China Nurs Educ. 2022;19(02):113–118. doi:10.3761/j.issn.1672-9234.2022.02.003
18. Knight ZG. A proposed model of psychodynamic psychotherapy linked to Erik Erikson’s eight stages of psychosocial development. Clin Psychol Psychother. 2017;24(5):1047–1058. PMID: 28124459. doi:10.1002/cpp.2066
19. Zhang ZX, Wang Y, Jian R, et al. Latent profiles and influencing factors of perioperative information overload in cervical cancer patients. Military Nursing. 2025;42(04):83–86+90. doi:10.3969/j.issn.2097-1826.2025.04.020
20. Shi JF, Li ZY. Cui QF Research progress on the application of patient journey mapping to improve patient medical experience. China Nurs Manag. 2024;24(11):1749–1754. doi:10.3969/j.issn.1672-1756.2024.11.029
21. Wu FQ. Observation on the effect of rapid rehabilitation surgery on perioperative care of modified radical resection of breast cancer. Chin J Rehabil Med. 2019;34(03):342–345. doi:10.3969/j.iSSN.1001-1242.2019.03.020
22. Accardi-Ravid M, Eaton L, Meins A, et al. A qualitative descriptive study of patient experiences of pain before and after spine surgery. Pain Med. 2020;21(3):604–612. PMID: 31081884; PMCID: PMC7060399. doi:10.1093/pm/pnz090
23. Zhang L, Lingxia Z, Lin N, et al. A qualitative study on perioperative disease perception and experience in patients with thyroid cancer. General Pract Nurs. 2022;20(28):4023–4026. doi:10.12104/j.issn.1674-4748.2022.28.037
24. Ju XX, Feng J, Yang J, et al. The impact of illness perception on pre-operative anxiety in lung cancer patients multiple mediating effects of information needs and patient trust. Military Nursing. 2024;41(11):74–78. doi:10.3969/j.iSSN.2097-1826.2024.11.018
25. Wan SW, Chong CS, Jee XP, Pikkarainen M, He HG. Perioperative experiences and needs of patients who undergo colorectal cancer surgery and their family Youdaoplaceholder0: a qualitative study. Support Care Cancer. 2022;30(6):5401–5410. PMID: 35298716; PMCID: PMC8929239. doi:10.1007/s00520-022-06963-1
26. Yuan J, Zhang J, Cui XY, et al. Current status of discharge readiness of patients undergoing cervical cancer surgery and its influencing factors analysis. Chin Med Herald. 2024;21(34):88–93. doi:10.20047/j.issn.sn1673-7210.2024.34.17
27. Xu M, Mei RR, Luo YH, et al. Qualitative study on the stigma of upper extremity lymphedema patients after breast cancer surgery. Contemporary Nurses. 2024;31(06):115–119. doi:10.19791/j.cnki.1006-6411.2024.16.028
28. Zheng YY, Lu HY, Chen ZF, et al. Symptoms and psychological experience of cervical cancer patients after radical hysterectomy: qualitative research. Chin J Nurs. 2020;55(04):569–573. doi:10.3761/j.issn.0254-1769.2020.04.017
29. Shrestha G, Mulmi R, Phuyal P, et al. Experiences of cervical cancer survivors in Chitwan Nepal: a qualitative study. PLoS One. 2020;15(11):e0234834. PMID: 33151965; PMCID: PMC7644025. doi:10.1371/journalpone.0234834
30. Kang MX, Li XY, Li HS. Correlation analysis between the sense of meaning of life and the fear of recurrence and social support in patients with advanced lung cancer. Oncol Basic Clin. 2024;37(05):607–609. doi:10.3969/j.iSSN.1673-5412.2024.05.031
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.