Back to Journals » International Medical Case Reports Journal » Volume 18
A Huge Mesenteric Chylous Cyst, Presenting as Abdominal Mass: A Rare Case Report
Authors Nazari FA, Zarif SK, Baset GY ![]() , Katawazai S
, Katawazai S
Received 9 January 2025
Accepted for publication 16 April 2025
Published 18 April 2025 Volume 2025:18 Pages 493—497
DOI https://doi.org/10.2147/IMCRJ.S513146
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Thomas E Hutson
Fareed Ahmad Nazari,1 Said Karim Zarif,1 Ghulam Yahia Baset,1 Soma Katawazai2
1Department of Emergency Surgery and Trauma, Kabul University of Medical Science, Ali Abad University Hospital, Kabul, Afghanistan; 2Gynecology and Obstetric Department, Kabul University of Medical Science, Shahr Ara University Hospital, Kabul, Afghanistan
Correspondence: Ghulam Yahia Baset, Email [email protected]
Abstract: Mesenteric cysts are rare abdominal lesions. A mesenteric chylous cyst is a very rare type of mesenteric cyst that may occur anywhere through the bowel, from the duodenum to the rectum. The etiology of mesenteric cysts is unknown and several theories have been suggested for forming these cysts. A mesenteric cyst is mostly found incidentally during investigations for another pathology. The treatment of choice for mesenteric chylous cysts in symptomatic patients is complete excision (enucleation) by either laparoscopic or open technique. The prognosis of a completely excised mesenteric cyst is generally good and its malignant transformation is reported to be around 3%. We present a case of mesenteric chylous cyst in a 60-year-old female presented with abdominal pain, constipation, nausea, and vomiting, who underwent laparotomy and complete cyst excision rate. The purpose of this case report is to consider mesenteric chylous cyst in the differential diagnosis of all abdominal masses.
Keywords: mesenteric chylous cyst, abdominal mass, enucleation
Introduction
A mesenteric chylous cyst is a rare abdominal mass that may occur anywhere through the bowel, from the duodenum to the rectum.1 It is found equally in both sexes and adults and children with an incidence of approximately 1 in every 100,000 adult admissions to the hospital.2
A mesenteric cyst is mostly found incidentally during investigations for another pathology.3 Still, patients with this cyst can sometimes present with non-specific symptoms of abdominal pain and distension, nausea, vomiting, or an abdominal mass, or may present with an acute abdomen in case of rupture, hemorrhage, or torsion.3 This lesion develops mostly from the mesentery of the small intestine from the duodenum, jejunum towards the ileum in 60% and less frequently from the mesocolon of the ascending colon in up to 24% and in the retroperitoneum in 14.5% of cases.3
Mesenteric cysts are usually unilocular and contain chylous fluid when they are located in the jejunum or serous fluid when they are located in the ilium or colon.4 Its size ranges from a few millimeters up to fill the abdominal cavity.4 Histologically, it includes a cuboid epithelium or cylindrical with microvilli, and sometimes smooth muscle component.4 Herein we present a case of mesenteric chylous cyst in a 60-year-old female presented with abdominal pain, constipation, nausea, and vomiting.
Case Presentation
A 60-year-old female presented to our hospital, with abdominal pain and distension of 4 months duration, with occasional constipation, nausea, and vomiting. The pain was located at the central areas of the abdomen most of the time, increased after meals, and was associated with nausea, vomiting, and sometimes constipation. Past medical history revealed that she had hypertension which was under control with antihypertensive medication as well as a low-salt diet.
Physical examination revealed that blood pressure was 130/80 mmHg, pulse rate 80 bpm, respiratory rate 17 cycle/minute, temperature 37°C, SpO2 95%, and she was conscious and alert. The abdomen was distended, bowel sounds were normal. There was an intra-abdominal partially mobile cystic mass in up-down direction with smooth outline and regular borders. Mild tenderness was present in the umbilical area of the abdomen, and shifting dullness was negative.
On investigations, Complete Blood Count, urea and creatinine, Liver Function Test, serum amylase, serum electrolytes, ECG, Chest x-ray, and urinalysis were normal. Ultrasonography of the abdomen revealed a 15 x 14cm cystic mass. Contrast-enhanced CT scan of the abdomen revealed a cystic mass measuring 16 x 14cm arising from mesentery of the jejunum and suggested the probability of a mesenteric cyst (Figure 1).
 |
Figure 1 A cystic mass in the CT scan of the abdomen. |
A laparotomy was performed with a midline incision. There was a huge, mobile, pedunculated, cystic mass arising from the mesentery of jejunum with some adhesions to adjacent structures (Figure 2). The adhesions were carefully released without any damage to surrounding structures. The mass was completely excised from its pedicle and the adjacent small bowel and its mesenteric vessels were preserved (Figure 3). The mass was opened outside of the abdomen and it was realized that it was full of chylous liquid material with no septations (Figure 4). As it was arising from the jejunum and containing chylous liquid material, intraoperative diagnosis of mesenteric chylous cyst was certain grossly. The specimen was also sent for pathologic study, the result was chylous cyst. The abdomen was closed layer by layer.
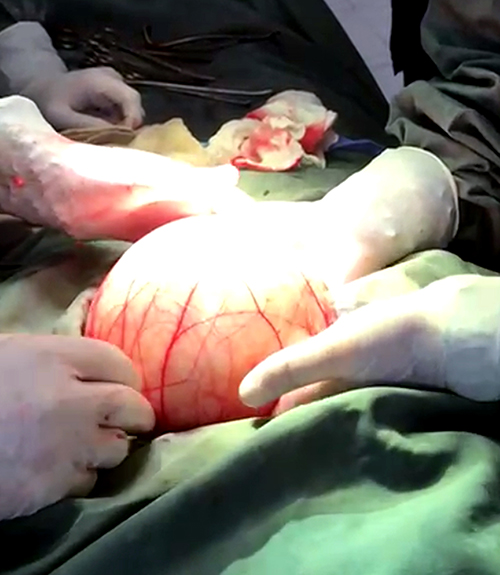 |
Figure 2 Cystic mass (chylous cyst) of the abdomen. |
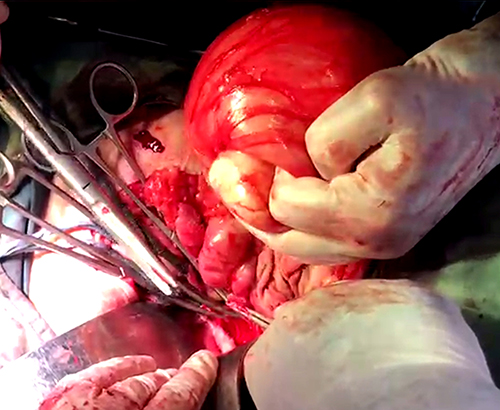 |
Figure 3 Excised cystic mass (chylous cyst). |
 |
Figure 4 Drained chylous liquid of the cyst. |
The post-operative course was uneventful and the patient was discharged home on the third postoperative day with full recovery. The patient was followed up for one year with abdominal ultrasonography, and fortunately, there was not any complication or recurrence of the disease.
Discussion
Mesenteric chylous cysts are rare benign abdominal pathologic entities that possess the risk of malignant transformation in 3% of cases as reported.5 A mesenteric chylous cyst is defined as a cyst in the mesentery of the gastrointestinal tract anywhere from the duodenum to the rectum, and which may extend from the base of the mesentery into the retroperitoneum.6
Mesenteric cysts are classified into four types according to their characteristics. Type 1 or pedunculated mesenteric cyst has extensive mobility and growth with a risk of complications. Type 2 or sessile mesenteric cyst has less mobility and implies probable intestinal resection. Type 3 mesenteric cyst involves retroperitoneal structures and surgery may be difficult in this case, because of the proximity of great vessels. Type 4 mesenteric cyst involves intra and extraperitoneal structures.3
The etiology of mesenteric cysts is unknown.7 The pathogenesis of chylous mesenteric cysts is not well understood and several theories have been suggested for the formation of these cysts.6 One of the theories proposed that the cyst represents a benign proliferation of ectopic lymphatics, which lack communication with the main lymphatic system.6 Another theory proposed that embryonic lymphatic channels gradually enlarges in size, due to the failure of joining the venous system.6 It may also result from lymphatic blockage secondary to surgery, trauma, infections, and neoplasms.6 Finally, it has been suggested that non-fusion of the leaves of mesentery results in the accumulation of lymphatic fluid within this space.6
Mesenteric chylous cysts are usually asymptomatic and are found incidentally during investigations for another pathology or other surgical procedures.6 They can also present with vague abdominal pain, bulging or abdominal distension, constipation or diarrhea, intestinal obstruction, and palpation of a lump.8 Non-specific symptoms such as nausea, vomiting, weight loss, anorexia, and bloating may not be severe enough for patients to seek medical help.9 They can also present with symptoms and signs arising from compression of adjacent structures, resulting in pyelonephritis, due to ureteral obstruction; acute abdomen because of infection, rupture or torsion of the cyst; jaundice due to biliary compression and anemia due to intratumoral bleeding.10
The specific diagnosis of mesenteric chylous cyst is difficult before operation as there are no pathognomonic symptoms or imaging findings.6 Deferent diagnostic modalities are used to diagnose mesenteric chylous cysts, but ultrasonography, CT-scan, and MRI are preferred.11
The differential diagnosis of mesenteric cysts includes ovarian cysts, pancreatic cysts, renal cysts, splenic cysts, as well as hydronephrosis, ascites, periappendicular abscesses, and even septic ascites.10
The treatment of choice for mesenteric chylous cysts in symptomatic patients is complete excision (enucleation) by either laparoscopic or open technique.12 Whenever enucleation is not safely possible, due to the adhesion of the cyst wall to adjacent mesenteric tissues or other organs, a resection of adjacent organs may be necessary.13 In 20 to 60% of cases, resection and anastomosis of the surrounding intestine may be required in addition to the removal of the cysts.8 Other surgical procedures include drainage, deroofing, and partial excision with marsupialization which are associated with a higher chance of recurrence and therefore are best avoided.13 In a few cases, mesenteric cysts are treated by ultrasound drainage and ethanol sclerotherapy.8
The indication for surgery in mesenteric cysts is symptom-related. In the case of asymptomatic patients, follow-up can be maintained while for those with clinical manifestations, surgery is suggested.3
The prognosis of completely excised mesenteric cysts is generally good.1 These cysts are benign and have a very low recurrence rate with recurrences usually within a year.1 Malignant transformation is reported in 3% of cases.5
Conclusion
Mesenteric chylous cysts are rare benign abdominal pathologic entities that possess the risk of malignant transformation in 3% of cases as reported. Mesenteric chylous cysts are usually asymptomatic and are found incidentally during investigations for another pathology or during other surgical procedures. Mesenteric cysts should be kept in the differential diagnosis of patients with abdominal pain. Indication for surgery in mesenteric cysts is symptom-related.
Ethical Approval
This report does not contain any personal information that could lead to the identification of the patient. Therefore, it is exempt from the ethical approval of our institution.
Consent
Written informed consent was obtained from the patient for publication of this case report and accompanying images.
Acknowledgment
The authors would like to express their sincere gratitude to the patient’s guardians for providing consent to include the case details and photographs in this publication.
Funding
The authors declare that his work is not funded by any institution, organ, or government and he has no financial support.
Disclosure
The authors have no potential conflicts of interest to disclose for this work.
References
1. Sah RP, Bhusal A, Yogi TN, et al. Mesenteric cyst in a toddler: a case report. J Pediatr Surg Case Rep. 2023;99:102735. doi:10.1016/j.epsc.2023.102735
2. Razi K, Al-Asaad O, Milind R. Case report: elective removal of a large mesenteric. J Surg Case Rep. 2017;1–3. doi:10.1093/jscr/rjx063
3. Zavala RAB, García Cerda AE, Calderon UC, et al. Surgical treatment of type 2 giant mesenteric cyst: case report and literature review. Int J Res Med Sci. 2024;12(1):243–245. doi:10.18203/2320-6012.ijrms20234009
4. Yeh BM, Joe BN, Sirlin CB, et al. Vascular contact with soft tissue: a sign of mesenteric masses at computed tomography. J Comput Assist Tomogr. 2008;32:185–190. doi:10.1097/RCT.0b013e3181507557
5. Alqurashi HE, Alaryni AA, Alsairafi RA, et al. Mesenteric cyst: a case report. Cureus. 2023;15(1). doi:10.7759/cureus.34325
6. Paramythiotis D, Bangeas P, Karakatsanis A, et al. Ideal treatment strategy for chylous mesenteric cyst: a case report. J Med Case Rep. 2018;12(317):1–6. doi:10.1186/s13256-018-1716
7. Al-Harfoushi R, Stevenson L, Binnie N. Mesenteric cyst: drained and marsupialised laparoscopically avoiding enterectomy. BMJ Case Rep. 2012;1–2. doi:10.1136/bcr.03.2012.6013
8. Rezaee-Azandaryani A, Ghorbanpour M, Taghipour M, Yamini A. A case report of a huge mesenteric cyst in a 5-year-old girl: a rare and challenging finding in radiological Assessment. Adv J Emerg Med. 2020;4(2):e31. doi:10.22114/ajem.v0i0.201
9. Nguyen M, Faul P, Naqvi SA. Giant mesenteric cyst–cause of abdominal distension managed with laparotomy-a case report. J Case Rep Studies. 2014;2(3):303. doi:10.15744/2348-9820.1.603
10. Carmon IC, Trebollé JF, García DM, et al. A case report: acute abdominal pain caused by a mesenteric cyst in a 20-year-old female patient. Ann Med Surg. 2019;50:28–30.
11. Dalgıç D, Ince E, Ciftci E, et al. Infected mesenteric cyst: a case report. J Ankara Univ Faculty Med. 2005;58(3):139–141.
12. Rajendran S, Khan A, Murphy M, O’Hanlon D. The diagnosis and treatment of a symptomatic mesenteric cyst. BMJ Case Rep. 2014;1–2. doi:10.1136/bcr-2013-202410
13. Abiyere O, Rosiji OB, Adewara O, et al. Huge mesenteric cyst: case report. Int J Surg Res Pract. 2021;8(2):128–131. doi:10.23937/2378-3397/1410128
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.