Back to Journals » Journal of Asthma and Allergy » Volume 10
A framework for measuring self-management effectiveness and health care use among pediatric asthma patients and families
Authors Rangachari P ![]()
Received 29 January 2017
Accepted for publication 17 March 2017
Published 12 April 2017 Volume 2017:10 Pages 111—122
DOI https://doi.org/10.2147/JAA.S133481
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Luis Garcia-Marcos
Pavani Rangachari
College of Allied Health Sciences, Augusta University, Augusta, GA, USA
Abstract: Asthma is associated with substantial health care expenditures, including an estimated US$56 billion per year in direct costs. A recurring theme in the asthma management literature is that costly asthma symptoms, including hospitalizations and multiple emergency department (ED)/outpatient visits, can often be prevented through patient/family adherence to the national (National Institutes of Health Expert Panel Report-3) guidelines for effective self-management of asthma, specifically 1) medication adherence and 2) environmental trigger avoidance, as outlined in the patient’s personalized Asthma-Action Plan. It is important to note however that while effective self-management of asthma is known to reduce ED visits and hospitalizations, the relationship between asthma self-management effectiveness and outpatient visit frequency remains ambiguous, reflecting a gap in the literature. For instance, do patients/families who self-manage effectively visit outpatient clinics more frequently for asthma care (compared to those who do not self-manage effectively), after accounting for differences in asthma severity, demographic characteristics, and risk factors? Do patients/families who visit outpatient clinics more frequently for asthma care, in turn have fewer ED and inpatient encounters for asthma? On the other hand, do patients/families who do not revisit outpatient clinics regularly have higher ED visits and hospitalizations? It is important to address these gaps, in order to reduce the costs and public health burden of asthma. This paper provides a foundation for addressing these gaps, by conducting an integrative review of the asthma management literature, to develop a conceptual framework for measuring self-management effectiveness and health care use among pediatric asthma patients/families. In doing so, the paper lays the groundwork for future research seeking to explicate the relationship between asthma self-management effectiveness and health care use, which in turn has potential to engage asthma providers in promoting ideal self-management and optimal health care use for pediatric asthma, in accordance with national evidence-based guidelines for asthma management.
Keywords: pediatric asthma, self-management, health care use, evidence-based guidelines, patient-and-family-centered care, population health management
Introduction
The US Centers for Disease Control and Prevention (CDC) reports a 4.3 million increase in the number of individuals diagnosed with asthma, from 2001 to 2010. In 2010, there were over 450,000 asthma-related hospitalizations, nearly 2 million emergency department (ED) visits, over 1 million visits to outpatient clinics, and over 3,000 deaths associated with asthma, resulting in approximately US$56 billion in direct health care costs nationwide.1–3 A recurring theme in the asthma management literature is that costly symptoms of asthma, including hospitalization and multiple ED or outpatient visits, can often be prevented through patient/family adherence to the national guidelines for effective self-management of asthma.4–10
The National Institutes of Health (NIH) National Asthma Education and Prevention Program (NAEPP) Expert Panel Report-3 (EPR-3) Guidelines for the Diagnosis and Management of Asthma, originally released in 2007, is the most current set of national evidence-based guidelines for asthma management. A central recommendation of the NAEPP EPR-3 is the use of an Asthma-Action Plan (AAP) by asthma patients/families and their providers. The AAP is a written personalized (patient-specific) plan that explains which medicines to take and when to take them, which types of environmental triggers to avoid, and how to deal with the signs and symptoms of an asthma episode.11,12
In effect, the AAP serves to reinforce to asthma patients/families and their providers two key components of effective self-management of asthma, described in the EPR-3 guidelines: 1) adherence to medication or pharmacotherapy and 2) avoidance of environmental triggers. Additionally, the AAP includes a personalized plan for ongoing monitoring of symptoms and instructions for when the patient/family should seek medical attention. According to EPR-3, the AAP should be developed collaboratively by the patient and provider, and represent a partnership between provider and patient, emphasizing education and reinforcement, to encourage effective asthma self-management.4,6,11–16 Since 2009, hospitals across the nation have been required to provide all asthma patients with an AAP, regardless of the care setting.13
Turning our attention to the substantial costs and public health burden of asthma can serve to underscore the crucial role of effective self-management of asthma in 1) preventing avoidable health care visits for asthma, 2) optimizing both self-management and health care use, and 3) reducing the overall costs of asthma. At this juncture, however, a key distinction needs to be made between ED/inpatient visits and outpatient visits for asthma. In other words, while effective asthma self-management is known to be associated with lower ED and inpatient visits for asthma, the relationship between self-management effectiveness and outpatient visit frequency for asthma remains ambiguous, reflecting a gap in the literature. For example:
- Do patients/families who self-manage effectively visit outpatient clinics for asthma care, more frequently or less frequently, compared to those who do not self-manage effectively, after accounting for differences in asthma severity, demographic characteristics, and other socioeconomic risk factors?
- Do patients/families who visit outpatient clinics more frequently for asthma care in turn have fewer ED and inpatient encounters for asthma?
- On the other hand, do “no-shows” and those who do not revisit outpatient clinics even once in over six months, that is, “non-revisits”, have higher ED and inpatient encounters?
The importance of addressing these gaps is heightened by the variation in provider opinion on this topic. For example, at one children’s hospital in Georgia, some asthma providers believe that while multiple (three or more) revisits over a six-month period to general pediatric clinics for “acute asthma exacerbation” may be indicative of low self-management effectiveness, multiple revisits to specialty (e.g., allergy) clinics may not, because new patients or patients recently discharged from the hospital may need to be seen frequently in specialty clinics. Other providers however are of the opinion that multiple sick revisits over a six-month period even to specialty clinics may be indicative of low self-management effectiveness. On the other hand, some providers believe that “non-revisits” and/or no-shows for asthma outpatient care over a six-month period may be a better indicator of low self-management effectiveness, reflecting a level of nonchalance among these patients/families to seek regular treatment, which may in turn place them at a greater risk for future ED visits and hospitalizations for asthma.17
Significance and importance
Since both primary care physicians (PCPs) and asthma subspecialists play a crucial role in asthma management, particularly with respect to influencing patient/family adherence to the AAP, these providers could greatly benefit from resources for measuring asthma self-management effectiveness among patients/families, including key risk factors associated with low self-management effectiveness. Additionally, it would be important for asthma providers to understand the relationship between asthma self-management effectiveness and health care use (including outpatient visit frequency), while adjusting for asthma severity, demographics, and risk factors. This type of information in turn could aid providers in:
- identifying strategies for promoting ideal self-management and optimal health care use at the individual patient/family level; and
- developing interventions for promoting asthma self-management effectiveness, at the community level, where applicable.
For example, if low asthma self-management effectiveness is found to be related to a lack of self-management education by PCPs, resulting in more outpatient visits than necessary, then asthma subspecialists could develop interventions to increase the adoption of asthma self-management education by community PCPs. Similarly, if low self-management effectiveness is found to be associated with the child’s school environment, including the absence of trigger reduction education in the school, then providers could work with school and county officials to raise awareness and resources for asthma education and support in schools. On the other hand, if low self-management effectiveness is traced back to younger parents/guardians not refilling prescriptions for required medication with their pharmacy, leading to preventable asthma episodes and ED visits for their children, then asthma providers may be prompted to work with community pharmacies to increase the rate of prescription refills and medication adherence for asthma patients/families in the community.
There are other important reasons to address the gap in the literature with respect to the relationship between self-management effectiveness and health care use, particularly, outpatient visit frequency for asthma. Outpatient visits are known to constitute the largest expense of asthma, accounting for nearly 60% of direct costs.1–3 Importantly, while outpatient visits for asthma are known to encompass multiple revisits over short time frames, they are also known to have a number of no-shows and “non-revisits”, that is, asthma patients/families who do not return for outpatient care even once over a six-month period. For example, analysis of asthma encounter data at one children’s hospital in the state of Georgia revealed that hospital outpatient clinic revisits for pediatric asthma were over 200% greater than unique patient visits, over a six-month period. To elaborate, the hospital had 1,227 unique visits to outpatient clinics for pediatric asthma, between July and December 2013. However, when individual patients/families were tracked for a six-month window following their initial visit to the outpatient clinics, we found a total of 2,468 revisits to the outpatient clinic for this population. While, on the one hand, 363 (30%) patients/families did not revisit the hospital outpatient clinics even once over a six-month period (i.e., “non-revisits”), on the other, 353 (30%) revisited the hospital outpatient clinics three or more times. At the extreme, we found that 130 (10%) patients/families revisited five or more times, and 23 (2%) revisited ten or more times, over a six-month period.17 Therefore, outpatient clinics can provide access to both extremes in the asthma patient population, in addition to providing access to “low-hanging fruits”, that is, patients/families with moderate-to-high asthma severity and considerable potential to improve self-management effectiveness.
In summary, the outpatient setting can serve as a unique venue for conducting impactful interventions to promote asthma self-management effectiveness in the community. To this effect, efforts to develop a framework for measuring self-management effectiveness and health care use for pediatric asthma would be significant for the following reasons:
- Accelerating the adoption of patient-and-family-centered care for pediatric asthma management: the variation in provider opinion regarding self-management effectiveness and health care use (including outpatient visit frequency) for pediatric asthma suggests that providers do not yet have the resources/tools for measuring asthma self-management effectiveness, and discerning its impact on health care use. On a related note, this suggests that providers may be playing a more reactive rather than a proactive role in asthma management, thereby implying that pediatric asthma management is presently being driven largely by patients/families, with providers playing more of a supporting rather than an influential role. In order to begin playing a more proactive role in optimizing self-management and health care use for asthma, in accordance with the NIH EPR-3 national guidelines, providers may need additional resources/tools for measuring asthma self-management effectiveness and its impact on health care use. Therefore, efforts to develop resources/tools for measuring pediatric asthma self-management effectiveness would have potential to increase the engagement of asthma providers in delivering patient-and-family-centered care, to promote ideal self-management and optimal health care use for pediatric asthma, at the patient/family (individual) level and at the community level.
- Enabling successful implementation of national evidence-based (EPR-3) guidelines for asthma management: the proactive involvement and engagement of health care providers in asthma management is important now more than ever because of the availability of national guidelines for asthma management. To elaborate, a landmark report, “Crossing the Quality Chasm”, by the Institute of Medicine in 2001, stressed the need for “evidence-based management” to accompany “evidence-based guidelines”.18,19 While there is no paucity of evidence-based guidelines for a variety of conditions, these guidelines need to be accompanied by actionable strategies for successful implementation, to realize their full benefit. For example, while the Central Line Bundle (CLB) is widely known to include five key evidence-based practices for preventing catheter-related bloodstream infections (CRBSIs), the implementation of the CLB by health care providers is known to be inconsistent. This gap has been addressed through health services research endeavors that have strived to generate evidence-based management strategies for successfully implementing the CLB in hospitals, which in turn has enabled sustained reduction of CRBSIs at a national level.20–25 In a similar vein, efforts to measure asthma self-management effectiveness and its impact on health care use have the potential to create “evidence for action”, that is, a resource base of strategies for effective implementation of evidence-based (EPR-3) guidelines for asthma management, by health care providers.
- Facilitating a focus on “population health management” by hospitals and providers in a new era of value-based reimbursement: the efforts described in this paper are highly significant from the perspective of enabling asthma providers (including hospitals and physicians) to address the “Triple Aim” challenge, that is, 1) optimize health care delivery, 2) promote population health, and 3) reduce health care costs.26 In a new era of “value-based reimbursement” for providers, health care organizations must now manage disease within the community by concentrating on wellness instead of sickness. As such, hospitals, often the initial point of care, are increasingly becoming centers for promoting population health. Therefore, any efforts to measure asthma self-management effectiveness (and its impact on health care use) would provide a foundation for enabling asthma providers to address the growing challenges of community health promotion and population health management.
Purpose and objectives
Following from the above discussion, this paper seeks to develop a conceptual framework for measuring self-management effectiveness and health care use for pediatric asthma. The broader purpose of this endeavor is to lay a foundation for future research seeking to:
- develop methods for measuring self-management effectiveness among pediatric asthma patients and families;
- develop methods for evaluating health care use for pediatric asthma, including outpatient visits and revisits (routine and sick), ED and inpatient visits and revisits, primary care visits and revisits, urgent care visits and revisits, “non-revisits” and no-shows for outpatient care, and health care costs associated with these visits; and
- develop methods for explicating the relationship between self-management effectiveness and health care use for pediatric asthma.
The availability of national guidelines for asthma management reflects support for a self-agency model of asthma management, at the federal policy level, that is, support for a collaborative provider–patient partnership, leading up to the patient/family being in a position of control of their asthma management, through behavioral and other lifestyle changes.11,27 On the other hand, at the provider level, the variation in provider perspectives related to asthma self-management effectiveness suggests that a medical approach to asthma management may be more prevalent among health care professionals.17,28 Under the medical model, low self-management effectiveness is often viewed as the result of noncompliance in following doctors’ orders, which in turn could be attributed to a variety of socioecological constraints that may make effective asthma management beyond the control of the patient/family, including socioeconomic, institutional, health system, environmental, community-level, and policy-level constraints.29,30 In other words, providers’ perspectives on self-management effectiveness reflect support for a socioecological model of asthma management, rather than a self-agency model of asthma management.
Therefore, while the national guidelines assert the importance of provider–patient collaboration and self-agency in asthma management, asthma providers’ perspectives indicate that there may be several factors beyond patients/families’ control at play in impacting self-management effectiveness. This dichotomy in turn points to the importance of viewing asthma self-management effectiveness as a byproduct of both factors within the control of asthma patients/families and factors beyond their control.
Accordingly, the three objectives of this paper are as follows:
- Conduct an integrative review of the literature on asthma management, including an exploration of the essential tenets of the medical, collaborative, self-agency, and socioecological models of asthma management, with the goal of developing a conceptual framework for measuring the self-management effectiveness of pediatric asthma.
- Articulate the importance of incorporating “health care use” for pediatric asthma into the framework. Adding health care use into the model would enable explication of the relationship between self-management effectiveness and health care use (including outpatient visit frequency) for pediatric asthma, which in turn has potential to provide actionable information for asthma providers to use in developing strategies and interventions for promoting ideal self-management and optimal health care use among pediatric asthma patients and families.
- Develop a holistic conceptual framework for measuring self-management effectiveness and health care use among pediatric asthma patients and families.
Parameters of the literature review
This paper performs an integrative review of the asthma management literature, to address the stated problem of interest, that is, the absence of sufficient resources for asthma providers (PCPs and subspecialists) to assess self-management effectiveness of pediatric asthma. This gap in turn makes it challenging for asthma providers to be more proactively engaged in promoting optimal self-management and health care use for pediatric asthma (which in turn is not in alignment with the national EPR-3 guidelines for asthma management, and likewise, is known to result in growing costs and public health burden of pediatric asthma).
Correspondingly, the goal of this paper is to develop a conceptual framework for measuring self-management effectiveness and health care use for pediatric asthma. The literature review in turn is driven by this goal and informed by the background (provided earlier), with regard to the dichotomy of perspectives between policymakers and asthma providers, on the potential of patients/families to be in control of their asthma.
This background information in turn serves to determine the parameters of the literature review, that is, a focus on understanding the key tenets of the collaborative vs. medical models of asthma management, with a view to developing a framework for measuring self-management effectiveness and health care use for pediatric asthma. Specifically, the paper examines two decades of literature on asthma management (mid-90s to current), including the period leading up to the development and publication of the national EPR-3 guidelines for asthma management in 2007. The review is conducted through PubMed/NCBI databases using broad search terms including “asthma self-management”, “medical models”, “collaborative models”, and “pediatric asthma”. All articles (resulting from the search) that provided insight into factors (barriers and facilitators) influencing asthma management behaviors and practices (for pediatric and adult asthma) were included in the review. On the other hand, articles which focused exclusively on clinical and biologic interventions for asthma prevention were excluded from the review.
The next section summarizes the results of an integrative review of the asthma management literature, culminating in the development of a holistic conceptual framework for measuring self-management effectiveness and health care use for pediatric asthma. The remaining sections of the paper discuss key implications of the conceptual framework, for asthma management research and practice, while Figures 1 and 2 provide a figurative depiction of the evolution of the framework.
 | Figure 1 A conceptual framework for measuring self-management effectiveness among pediatric asthma patients and families. |
 | Figure 2 A holistic conceptual framework for measuring self-management effectiveness and health care use among pediatric asthma patients and families. |
Literature on asthma management
The availability of national asthma management guidelines suggests that US policymakers have embraced self-management programs as one way to decrease health costs (by reducing health care utilization through patient empowerment). A review of the literature indicates considerable attention to asthma self-management over the past two decades.31–44 Additionally, during this time frame, various federal agencies, including the CDC and the NIH NAEPP, have sponsored multiple national reports and conferences on asthma management.3,11,13
However, a closer review suggests that a medical model of asthma management may be more rampant.28,45–53 Under the medical model, an emphasis is placed on adherence to directions given by health care professionals; in other words, patients/families are expected to take prescribed medications and follow doctors’ orders. Consequently, the patient/family must learn to trust the doctor’s medical knowledge, which in turn is the essence of the medical management approach. Patients/families who do not comply with doctors’ orders are labeled as noncompliant. Noncompliance with prescribed treatment in turn is viewed as a result of not only behavioral issues but also a consequence of socioecological constraints that neither the patient nor the doctor can control, for example, socioeconomic issues, insurance barriers, low health literacy, health system limitations, environmental issues, and policy-level constraints.29,30,45,54
Despite the widespread emphasis on a medical approach to asthma management, efforts have been made in recent years, at the policy and industry levels, to move toward more collaborative models of asthma management. For example, as discussed earlier, a central component of the NIH EPR-3 guidelines for asthma management is the development of an AAP, by asthma patients/families and their providers, in an effort to emphasize the importance of a collaborative approach to asthma management by providers and their patients/families.11,13 The essence of the collaborative approach is a partnership between providers and patients in chronic disease management, with providers extending education, support, and resources for monitoring, to enhance self-management by patients/families.55–58 According to Bodenheimer et al, self-management is crucial in enabling a rewarding lifestyle for individuals living with chronic disease, since it enables patients to be informed and educated to participate in their own care (including decisions related to their treatment options), to gain a sense of control over their lives, which in turn can serve to reduce the frequency of physician visits, and improve quality of life.59–62
Under the self-agency model, an extension of the collaborative model of asthma management, patients are proactive in understanding how they respond to illness and planning day-to-day routines as a way of creating a sense of order.39,42,59,62 Developing alternative lifestyle habits and taking control of their own lives are important for patients (asthmatics) who have embraced the self-agency paradigm. This includes initiating discussions with one’s doctor on which medications work and which do not work, within the context of one’s life, keeping informed about alternate approaches to managing their condition, and monitoring changes in treatment with vigilance.59,62 Therefore, taking control of one’s own asthma management is the essence of the self-agency paradigm.
In summary, while both the collaborative and self-agency models of asthma management tend to emphasize patient empowerment and control as the key to effective asthma management, the medical model places doctors in charge, with patients/families being expected to follow doctors’ orders in taking prescribed medication. Importantly, under the medical model, any lapses in following prescribed asthma management practices are often ascribed to socioecological constraints that may be beyond the control of the patient or the doctor.
The above discussion highlights the importance of considering the socioecological model of asthma prevention and management, which has been embraced by public health agencies (such as the CDC), as a framework for guiding interventions for chronic disease prevention and management.63,64 According to the socioecological model, people exist within a system of relationships, within complex layers of environments that impact on their lives. Changes or impacts in one layer tend to ripple throughout other layers.63,65–68 The model views individual behavior as being influenced, while also influencing the environment. Environmental influences on individual behaviors are divided into micro-, meso-, exo-, and macro-systems.
The micro-system is the layer closest to the individual and contains the structures with which one has direct contact: family, school, neighborhood, and work environments. The meso-system is the layer where connections are made between structures within the micro-system. Beyond this layer is the exo-system that consists of the larger social system, in which the individual does not function directly. The structures within this layer impact the individual by interacting with one or more structures of the meso-system. Finally, the macro-system is the outermost layer, comprising cultural values, customs, and laws that indirectly impact the individual. The effect of the larger principles defined by the macro-system has a cascading influence throughout the interactions of all other layers.63,65–68
Based on the above framework, the socioecological model for health promotion posits that individual behavior is influenced by five categories of factors: intrapersonal factors (individual characteristics such as knowledge, skills, behavior, and beliefs), interpersonal factors (social networks including family, professional peers, and friends), institutional factors (rules and regulations of social institutions), community and environmental factors (relationships among the various institutions), and public policy (all levels of government). This model can be utilized to guide planning and interventions across each level. Research suggests that efforts to target all levels of the socioecological model may be important in improving intervention effectiveness.69,70
A framework for measuring pediatric asthma self-management effectiveness
The above review reveals a dichotomy of perspectives in the asthma management literature with regard to the best approach to achieving effective asthma self-management. While the collaborative model and the self-agency model place the patient/family in a position of control in ensuring effective asthma management, the medical approach places the doctor in control of disease management, with the patient/family being expected to follow doctor’s orders. Moreover, any lapses in following the prescribed course of treatment are often attributed to socioecological influences and constraints that are beyond the control of the patient/family.
These gleanings from the asthma management literature point to the importance of considering both perspectives in any effort to measure asthma self-management effectiveness:
- Factors that are within the control of the individual patient/family, for example, asthma behaviors and self-management practices, such as regularity of refilling prescriptions for medication adherence or use of air purifiers in the indoor/home environment to mitigate exposure to environmental triggers for asthma.
- Factors that are beyond the control of the individual patient/family, for example, individual biologic factors such as asthma severity and comorbidities; individual cultural factors including beliefs related to asthma illness and treatment; socioeconomic risk factors, for example, child/patient’s living arrangements, insurance coverage for asthma controller medications, and so on; health system (institutional) risk factors, for example, self-management education received from asthma providers, including subspecialists and primary care providers; community-level risk factors, for example, support for self-management education in schools, daycares, and community at large; environmental risk factors, for example, ownership of indoor pets, exposure to tobacco smoke, and so on; policy-level risk factors, for example, state support/reimbursement for asthma education by community health workers.
In other words, self-management effectiveness for pediatric asthma needs to be a composite measure of factors within patient’s control, for example, medication adherence and environmental trigger avoidance (as outlined in the patient’s AAP), while accounting for factors beyond patient/family’s control, including 1) the multiple levels of risk factors (mentioned above), 2) severity of asthma (e.g., EPR-3 severity classification of “mild-persistent asthma” or higher), and 3) demographic characteristics (e.g., age, gender, race, household income, insurance, caregiver employment status, family history of asthma, number of smokers in household, and so on). This conceptualization of self-management effectiveness would incorporate key tenets of both the self-agency model of asthma management and the socioecological model of asthma management (while accounting for various risk factors and demographic characteristics impacting self-management behaviors at the patient/family level).
The essence of the conceptual framework therefore is that asthma is the manifestation of multiple individual, interpersonal, socioeconomic, community, health system, and environmental determinants. While the self-agency model places an emphasis on individual behavioral and lifestyle influences on asthma management, the socioecological model recognizes the interdependent relationship between individual (patients/families) and their environment, with respect to asthma management. While individual patients/families are responsible for making lifestyle changes appropriate for optimal health, their behavior is also considerably influenced by social, community, and environmental factors. The most suitable approach to changing individual health behavior therefore may be a combination of individual-, organizational-, and community-level interventions. Figure 1 articulates the conceptual framework discussed above.
Incorporating “health care use for pediatric asthma” into the framework
An important goal of this paper is to articulate what could be done to facilitate successful adoption and implementation of the national (EPR-3) guidelines for asthma management by asthma providers and their patients/families. As discussed earlier, while the national guidelines reflect support for patient–provider collaboration and patient self-agency in asthma management, asthma providers’ perspectives indicate support for a socioecological model, that is, multiple levels of influences on patients/families that may be constraining them from gaining control over their asthma. Importantly, the latter implies that asthma providers do not yet have the resources/tools for measuring pediatric asthma self-management effectiveness, as well as the specific risk factors associated with low self-management effectiveness (among asthma patients/families they serve).
Since both asthma subspecialists and PCPs play a crucial role in impacting patient/family self-management effectiveness, and influencing adherence to the AAP (in accordance with EPR-3 national guidelines), these providers could greatly benefit from resources for measuring self-management effectiveness among pediatric asthma patients/families. However, in addition to being able to measure asthma self-management effectiveness, it would be important for asthma providers to understand the impact of asthma self-management effectiveness on health care use (particularly, outpatient visit frequency), as discussed earlier. For example, do patients/families who self-manage effectively visit outpatient clinics more frequently for asthma care, compared to those who do not self-manage effectively after accounting for differences in asthma severity, demographic characteristics, and risk factors? And do these patients in turn have fewer emergency room (ER) and inpatient encounters? On the other hand, do those who do not revisit outpatient clinics even once in over six months have higher ER and inpatient encounters? Therefore, it would be important to conceptualize “health care use for pediatric asthma” broadly, to include
- primary care visits and revisits;
- outpatient (subspecialty) clinic visits and revisits (routine and sick);
- urgent care visits and revisits;
- ED and inpatient visits and revisits (general admission and pediatric intensive care unit stay);
- “non-revisits” and no-shows for asthma outpatient (subspecialty) care; and finally yet importantly,
- health care costs (provider charges and reimbursement) associated with all pediatric asthma care visits, to obtain a broader measure of health care use.
In summary, efforts to measure the relationship between self-management effectiveness and health care use for pediatric asthma would help to create “evidence for action” for asthma providers to be more proactively involved in promoting ideal self-management and optimal health care use for pediatric asthma, in accordance with national guidelines (EPR-3) for asthma management. In effect, the development of resources/tools for measuring pediatric asthma self-management effectiveness and health care use would have the potential to engage health care providers in 1) providing patient-and-family-centered care for pediatric asthma to individual patients/families and 2) developing interventions to promote asthma self-management effectiveness at the community level, as applicable.
A holistic framework for measuring self-management effectiveness and health care use for pediatric asthma
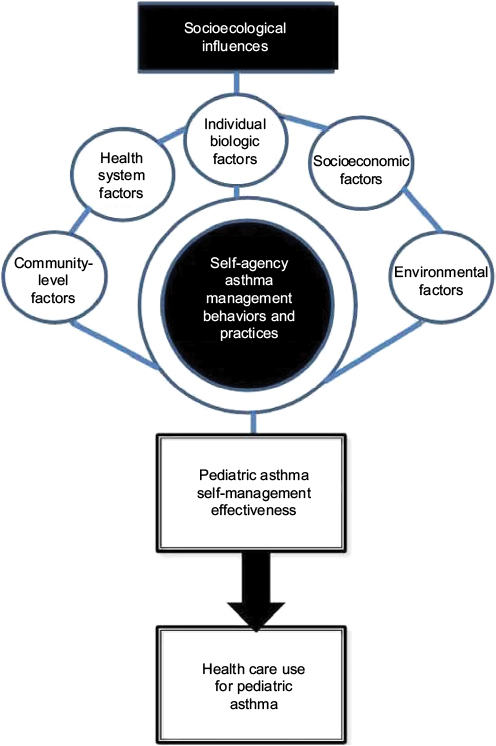
The above discussion enables us to put forth a holistic framework for measuring self-management effectiveness and health care use among pediatric asthma patients/families (summarized in Figure 2). Following from the rationale discussed earlier, “health care use” for pediatric asthma would be a function of patient/family “self-management effectiveness” (self-agency model), while adjusting for various patient/family demographic characteristics, severity of illness, and multiple levels of risk factors (socioecological model).
A key innovation of this conceptual framework is its integration of the self-agency model for defining self-management effectiveness, as patient/family adherence to EPR-3 guidelines for asthma management, with the socioecological model for identifying risk factors impacting self-management behaviors at the patient/family level, to put forth a holistic model for predicting health care use for pediatric asthma. This comprehensive approach to measuring both self-management effectiveness and health care use in turn has potential to not only address a gap in the asthma management literature but also pave the way for future research in chronic disease self-management, in general.
It would be relevant to note at this juncture that the purpose of this paper is to develop a holistic conceptual framework for measuring self-management effectiveness and health care use for pediatric asthma. The discussion leading to the development of this framework included several implicit assumptions about the directionality or relationships among variables in the framework. For example, the various levels of socioecological influences, when viewed as constraints (i.e., “socioeconomic”, “individual biologic”, “health system”, “environmental”, and “community-level” constraints), would be expected to have an inverse relationship with self-management effectiveness, that is, the greater the constraints (e.g., lack of insurance coverage for controller medications under “socioeconomic” factors), the stronger the negative impact on asthma self-management behaviors and practices, leading to lower asthma self-management effectiveness.
However, the framework by itself does not seek to explicitly comment on the directionality or relationships among the variables, since the goal is to develop a broad conceptual model that can provide a foundation for future research seeking to generate empirical evidence on the relationships among variables (in the framework). In summary, the emphasis of this paper is on developing a broad conceptual framework. The framework emanates from integrating a variety of literature streams to develop a conceptual model that is intended to lead to future research (on the nature of relationships among the key variables in the framework).
Implications for practice
If efforts to measure the relationship between self-management effectiveness and health care use for pediatric asthma (using the framework summarized in Figure 2) indicate that patients with younger parents (<25 years) are at greater risk for low self-management effectiveness, and low medication adherence, due to not regularly refilling prescription medications, then asthma providers may wish to explore prospects for conducting a pharmacy-led community-based intervention to increase the rate of refills for required medications, and thereby improve medication adherence and self-management of pediatric asthma in the community. On the other hand, if results indicate that patients/families at risk for insurance coverage denial are prone to “non-revisits” and later end up in the ED at other community hospitals, then asthma specialists, in collaboration with other community asthma providers, may wish to explore the possibility of investing in a community-based case manager to assist families in obtaining alternate controller medications covered by insurance, prevent no-shows, and promote optimal health care use for pediatric asthma among patients/families in the community.
Therefore, the framework (and future research generated by the framework) would engage asthma providers in identifying strategies to promote ideal asthma management among individual patients and families and in developing interventions to promote self-management effectiveness at a community level. In summary, the framework would have considerable potential to impact practice by promoting patient-and-family-centered care for pediatric asthma management, enabling successful implementation of EPR-3 guidelines by asthma providers, and enabling asthma providers to rise to the challenge of population health management, in a changing environment of rising costs and value-based reimbursement.
Implications for future research
The conceptual framework developed in this paper is intended to provide a foundation for the following: measuring pediatric asthma self-management effectiveness, while adjusting for severity, demographics, and multiple levels of risk factors (including individual behavioral and biologic, socioeconomic, health system, community, and environmental levels); and measuring health care use for pediatric asthma, including the following: 1) outpatient visits and revisits (routine and sick); 2) ER, inpatient, primary care, and urgent care visits and revisits; 3) “non-revisits” and no-shows for outpatient care; and the 4) health care costs associated with these visits. Such a comprehensive conceptual framework therefore is expected to serve as a stepping stone for future research seeking to:
- develop methods for measuring self-management effectiveness and health care use for pediatric asthma;
- develop a systematic understanding of the relationship between self-management effectiveness and health care use among pediatric asthma patients/families;
- create comparative profiles of patients/families with high and low self-management effectiveness of pediatric asthma; and
- generate insight into individual- and community-based interventions and strategies for promoting ideal self-management and optimal health care use for pediatric asthma, in accordance with the national evidence-based (EPR-3) guidelines for asthma management.
Future research efforts of this nature in turn would have potential to lay groundwork for larger projects to evaluate generalizability of results through large-scale replications of study methods, across outpatient settings in rural and inner-city regions in the US, as well as projects seeking to implement community-based interventions (developed using the framework described in this paper), to promote ideal self-management and optimal health care use among pediatric asthma patients/families in the community. These types of research endeavors in turn would serve a dual purpose of 1) addressing gaps in the pediatric asthma management literature and 2) tackling the practical challenges of asthma management, thereby directly helping to alleviate the public health burden (including the growing health care costs and disparities) associated with pediatric asthma and other chronic diseases in the community.
Conclusion
This paper reviews the asthma management literature to put forth a holistic conceptual framework for measuring self-management effectiveness and health care use for pediatric asthma. In doing so, the study lays a foundation for future research seeking to explicate the relationship between asthma self-management effectiveness and health care use, which in turn has potential to engage asthma providers in identifying strategies for promoting ideal self-management and optimal health care use at the individual patient/family level, and developing interventions for promoting asthma self-management effectiveness, at the community level, where applicable.
In addition to accelerating the adoption of patient-and-family-centered care for asthma management, the framework would have potential to enable successful implementation of national evidence-based guidelines for asthma management, and facilitate a focus on “population health management” by asthma providers, in a new era of value-based reimbursement. Such a comprehensive conceptual framework therefore is expected to serve as a stepping stone for future research having potential to develop a systematic understanding of the relationship between self-management effectiveness and health care use for pediatric asthma, which in turn has considerable potential to generate insight into individual- and community-based interventions for promoting optimal self-management and health care use for pediatric asthma, in accordance with the national evidence-based (EPR-3) guidelines for asthma management.
Acknowledgments
The author would like to thank Dr Renuka Mehta and other providers and staff at the Children’s Hospital of Georgia at Augusta University, for their support in conducting a pilot study, which provided a foundation for this review article. The pilot study in turn, emanated from a Community Health Partnership Grant sponsored by the Institute of Public and Preventive Health (IPPH) at Augusta University.
Disclosure
The author has no conflicts of interest to declare in this work.
References
Akinbami LJ, Moorman JE, Bailey C, et al. Trends in asthma prevalence, health care use, and mortality in the United States, 2001–2010. NCHS data brief, no 94. Hyattsville, MD: National Center for Health Statistics; 2012. | ||
Bahadori K, Doyle-Waters MM, Marra C, et al. Economic burden of asthma: a systematic review. BMC Pulm Med. 2009;9:4. | ||
U.S. Centers for Disease Control and Prevention (CDC). Asthma self-management education and environmental management: approaches to enhancing reimbursement. 2013. Available from: http://www.cdc.gov/asthma/pdfs/Asthma_Reimbursement_Report.pdf. Accessed May 3, 2016. | ||
Bhogal S, Zemek R, Ducharme FM. Written action plans for asthma in children. Cochrane Database Syst Rev. 2006;(3):CD005306. | ||
Cloutier MM, Hall CB, Wakefield DB, Bailit H. Use of asthma guidelines by primary care providers to reduce hospitalization and emergency department visits in poor, minority, urban children. J Pediatr. 2005;146(5):591–597. | ||
Jones MA. Asthma self-management patient education. Respir Care. 2008;53(6):778–784; discussion 784–786. | ||
Rastogi D, Madhok N, Kipperman S. Caregiver asthma knowledge, aptitude, and practice in high healthcare utilizing children: effect of an educational intervention. Pediatr Allergy Immunol Pulmonol. 2013;26(3):128–139. | ||
Schultz A, Martin AC. Outpatient management of asthma in children. Clin Med Insights Pediatr. 2013;7:13–24. | ||
Stanton MW, Dougherty D, Rutherford MK. Chronic care for low-income children with asthma: strategies for improvement. AHRQ Publication No. 05-0073. Rockville, MD: Agency for Healthcare Research and Quality; 2005. | ||
Frey SM, Fagnano M, Halterman J. Medication identification among caregivers of urban children with asthma. Acad Pediatr. 2016;16(8):799–805. | ||
National Asthma Education and Prevention Program (National Heart, Lung, and Blood Institute) Third Expert Panel on the Management of Asthma. Expert Panel Report 3: Guidelines for the Diagnosis and Management of Asthma. NLM ID: 101474652. 2007. Available from: http://www.nhlbi.nih.gov/guidelines/asthma/asthgdln.pdf. Accessed May 31, 2016. | ||
Zemek RL, Bhogal SK, Ducharme FM. Systematic review of randomized controlled trials examining written action plans in children: what is the plan? Arch Pediatr Adolesc Med. 2008;162(2):157–163. | ||
Fassl BA, Nkoy FL, Stone BL, et al. The Joint Commission Children’s Asthma Care quality measures and asthma readmissions. Pediatrics. 2012;130(3):482–491. | ||
Espinoza-Palma T, Zamorano A, Arancibia F, et al. Effectiveness of asthma education with and without a self-management plan in hospitalized children. J Asthma. 2009;46(9):906–910. | ||
Ring N, Malcolm C, Wyke S, et al. Promoting the use of Personal Asthma Action Plans: a systematic review. Prim Care Respir J. 2007;16(5):271–283. | ||
Pinnock H, Epiphaniou E, Pearce G, et al. Implementing supported self-management for asthma: a systematic review and suggested hierarchy of evidence of implementation studies. BMC Med. 2015;13:127. | ||
Rangachari P, Mehta R, Rethemeyer RK, Ferrang C, Dennis C, Redd V. Short or long end of the lever? Associations between provider communication of the “Asthma-Action Plan” and outpatient revisits for pediatric asthma. J Hosp Adm. 2015;4(5):26–39. | ||
Institute of Medicine (US) Committee on Quality of Health Care in America. In: Kohn LT, Corrigan JM, Donaldson MS, editors. To Err is Human: Building a Safer Health System. Washington, DC: National Academies Press (US); 2000. | ||
Institute of Medicine (US) Committee on Quality of Health Care in America. Crossing the Quality Chasm: A New Health System for the 21st Century. Washington, DC: National Academies Press (US); 2001. | ||
Pronovost PJ, Berenholtz SM, Goeschel CA, et al. Creating high reliability in health care organizations. Health Serv Res. 2006;41(4 Pt 2):1599–1617. | ||
Pronovost PJ, Goeschel CA, Colantuoni E, et al. Sustaining reductions in catheter related bloodstream infections in Michigan intensive care units: observational study. BMJ. 2010;340:c309. | ||
Rangachari P. Knowledge sharing networks related to hospital quality measurement and reporting. Health Care Manage Rev. 2008;33(3):253–263. | ||
Rangachari P. Knowledge sharing and organizational learning in the context of hospital infection prevention. Qual Manag Health Care. 2010;19(1):34–46. | ||
Rangachari P, Madaio M, Rethemeyer RK, et al. The evolution of knowledge exchanges enabling successful practice change in two intensive care units. Health Care Manage Rev. 2015;40(1):65–78. | ||
Rangachari P, Madaio M, Rethemeyer RK, et al. Cumulative impact of periodic top-down communications on infection prevention practices and outcomes in two units. Health Care Manage Rev. 2015;40(4):324–336. | ||
Berwick DM, Nolan TW, Whittington J. The triple aim: care, health, and cost. Health Aff. 2008;27(3):759–769. | ||
Hoppin P, Jacobs M, Stillman L. Investing in Best Practices for Asthma: A Business Case for Education and Environmental Interventions. Asthma Regional Council; 2010. Available from: http://asthmaregionalcouncil.org/wp-content/uploads/2014/02/2010_Investing-in-Best-Practices-for-Asthma-A-Business-Case.pdf. Accessed January 10, 2017. | ||
Fish L, Lung CL; Antileukotriene Working Group. Adherence to asthma therapy. Ann Allergy Asthma Immunol. 2001;86(6 Suppl 1):24–30. | ||
Trueman JF. Non-adherence to medication in asthma. Prof Nurse. 2000;15(9):583–586. | ||
Nuss HJ, Hester LL, Perry MA, Stewart-Briley C, Reagon VM, Collins P. Applying the social ecological model to creating asthma-friendly schools in Louisiana. J Sch Health. 2016;86(3):225–232. | ||
Adams RJ, Smith BJ, Ruffin RE. Patient preferences for autonomy in decision making in asthma management. Thorax. 2001;56(2):126–132. | ||
Bailey WC, Kohler CL, Richards JM Jr, et al. Asthma self-management: do patient education programs always have an impact? Arch Intern Med. 1999;159(20):2422–2428. | ||
Nieuwlaat R, Wilczynski N, Navarro T. Interventions for enhancing medication adherence. Cochrane Database Syst Rev. 2014;(11):CD000011. | ||
Barner JC, Mason HL, Murray MD. Assessment of asthma patients’ willingness to pay for and give time to an asthma self-management program. Clin Ther. 1999;21(5):878–894. | ||
Barlow JH, Sturt J, Hearnshaw H. Self-management interventions for people with chronic conditions in primary care: examples from arthritis, asthma and diabetes. Health Educ J. 2002;61(4):365–378. | ||
Bartholomew LK, Sockrider M, Abramson SL, et al. Partners in school asthma management: evaluation of a self-management program for children with asthma. J Sch Health. 2006;76(6):283–290. | ||
Costello F. Self-management of asthma. Nurs Stand. 2000;15:33. | ||
Lindgren B. The importance of self-management. Eur Respir Rev. 1996;6(35):108–112. | ||
Kralik D, Koch T, Price K, Howard N. Chronic illness self-management: taking action to create order. J Clin Nurs. 2004;13(2):259–267. | ||
Kolbe J. The influence of socioeconomic and psychological factors on patient adherence to self-management strategies: lessons learned in asthma. Dis Manag Health Out. 2002;10(9):551–570. | ||
Lorig K. Self-management in chronic illness. In: Funk S, Tornquist E, Leeman J, Miles M, Harrell J, editors. Key Aspects of Preventing and Managing Chronic Illness. New York, NY: Springer; 2001:35–41. | ||
Koch T, Jenkin P, Kralik D. Chronic illness self-management: locating the ‘self’. J Adv Nurs. 2004;48(5):484–492. | ||
Tattersall RL. The expert patient: a new approach to chronic disease management for the twenty-first century. Clin Med (Lond). 2002;2(3):227–279. | ||
Coleman MT, Newton KS. Supporting self-management in patients with chronic illness. Am Fam Physician. 2005;72(8):1503–1510. | ||
Bender B, Milgrom H, Rand C. Non-adherence in asthmatic patients: is there a solution to the problem? Ann Allergy Asthma Immunol. 1997;79(3):177–185. | ||
Brown R. Behavioral issues in asthma management. Allergy Asthma Proc. 2001;22(2):67–69. | ||
Conway A. Adherence and compliance in the management of asthma: 1. Br J Nurs. 1998;7(21):1313–1315. | ||
Fishwick D, D’Souza W, Beasley R. The asthma self-management plan system of care: what does it mean, how is it done, does it work, what models are available, what do patients want and who needs it? Patient Educ Couns. 1997;32(1 Suppl):S21–S33. | ||
Edwards AL. Asthma action plans and self-management: beyond the traffic light. Nurs Clin North Am. 2013;48(1):47–51. | ||
Milgrom H, Wamboldt F, Bender B. Monitoring adherence to the therapy of asthma. Curr Opin Allergy Clin Immunol. 2002;2(3):201–205. | ||
Watts RW, McLennan G, Bassham I, el-Saadi O. Do patients with asthma fill their prescriptions? A primary compliance study? Aust Fam Physician. 1997;26 Suppl 1:S4–S6. | ||
Haynes RB, Ackloo E, Sahota N, McDonald HP, Yao X. Interventions for enhancing medication adherence. Cochrane Database Syst Rev. 2008;(2):CD000011. | ||
Wraight JM, Cowan JO, Flannery EM, Town GI, Taylor DR. Adherence to asthma self-management plans with inhaled corticosteroid and oral prednisone: a descriptive analysis. Respirology. 2002;7(2):133–139. | ||
Stokols D. Translating social ecological theory into guidelines for community health promotion. Am J Health Promot. 1996;10(4):282–298. | ||
Holman H, Lorig K. Patients as partners in managing chronic disease. Partnership is a prerequisite for effective and efficient health care. BMJ. 2000;320(7234):526–527. | ||
Toelle BG, Ram FS. Written individualised management plans for asthma in children and adults. Cochrane Database Syst Rev. 2004;(2):CD002171. | ||
Sarver N, Murphy K. Management of asthma: new approaches to establishing control. J Am Acad Nurse Pract. 2009;21(1):54–65. | ||
Lorig K, Holman H. Arthritis self-management studies: a twelve year review. Health Educ Q. 1993;20(1):17–28. | ||
Bodenheimer T, Lorig K, Holman H, Grumbach K. Patient self-management of chronic disease in primary care. JAMA. 2002;288(19):2469–2475. | ||
Lindberg M, Ekström T, Möller M, Ahlner J. Asthma care and factors affecting medication compliance: the patient’s point of view. Int J Qual Health Care. 2001;13(5):375–383. | ||
Lorig K, González VM, Laurent DD, Morgan L, Laris BA. Arthritis self-management program variations: three studies. Arthritis Care Res. 1998;11(6):448–454. | ||
Kennedy I. Patients are experts in their own field. BMJ. 2003;326(7402):1276–1277. | ||
Bronfenbrenner U. The Ecology of Human Development. Cambridge, MA: Harvard University Press; 1979. | ||
Gillen EM, Hassmiller Lich K, Yeatts KB, Hernandez ML, Smith TW, Lewis MA. Social ecology of asthma: engaging stakeholders in integrating health behavior theories and practice-based evidence through systems mapping. Health Educ Behav. 2014;41(1):63–77. | ||
Golden SD, Earp JA. Social ecological approaches to individuals and their contexts: twenty years of health education & behavior health promotion interventions. Health Educ Behav. 2012;39(3):364–372. | ||
Kaugars AS, Klinnert MD, Bender BG. Family influences on pediatric asthma. J Pediatr Psychol. 2004;29(7):475–491. | ||
Miller BD, Wood BL. Childhood asthma in interaction with family, school, and peer systems: a developmental model for primary care. J Asthma. 1991;28(6):405–414. | ||
Wamboldt FS, Ho J, Milgrom H, et al. Prevalence and correlates of household exposures to tobacco smoke and pets in children with asthma. J Pediatr. 2002;141(1):109–115. | ||
McLeroy KR, Bibeau D, Steckler A, Glanz K. An ecological perspective on health promotion programs. Health Educ Q. 1998;15(4):351–377. | ||
Schölmerich VL, Kawachi I. Translating the socio-ecological perspective into multilevel interventions: gaps between theory and practice. Health Educ Behav. 2016;43(1):17–20. |
 © 2017 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2017 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.