Back to Journals » Journal of Healthcare Leadership » Volume 17
A Framework for Leadership in Organizational Development: A Novel Approach for Advancing Women Administrative and Faculty Leaders in Academic Medicine
Authors Williams WE, Baker MK ![]() , Denton L, Andreski P, Jacobs SR, Wooten LP, Singer K
, Denton L, Andreski P, Jacobs SR, Wooten LP, Singer K
Received 8 August 2024
Accepted for publication 18 June 2025
Published 5 August 2025 Volume 2025:17 Pages 355—364
DOI https://doi.org/10.2147/JHL.S490623
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Pavani Rangachari
Whitney E Williams,1,2 Michaella K Baker,3 Laura Denton,1 Patricia Andreski,4 Sonya R Jacobs,5 Lynn Perry Wooten,6 Kanakadurga Singer3,7,8
1Office of Faculty Development, University of Michigan Medical School, Ann Arbor, MI, USA; 2School of Social Work, University of Michigan, Ann Arbor, MI, USA; 3Department of Pediatrics, University of Michigan Medical School, Ann Arbor, MI, USA; 4Health Advancement, Michigan Medicine, Ann Arbor, MI, USA; 5Organizational Learning, University of Michigan, Ann Arbor, MI, USA; 6The President’s Office, Simmons University, Boston, MA, USA; 7Department of Molecular and Integrative Physiology, University of Michigan Medical School, Ann Arbor, MI, USA; 8Office of Faculty Affairs, University of Michigan Medical School, Ann Arbor, MI, USA
Correspondence: Whitney E Williams, Office of Faculty Development, University of Michigan Medical School, 6319 Med Sci 1, A-Wing, 1301 Catherine St, Ann Arbor, MI, 48109, USA, Tel +1 734-764-2307, Email [email protected]
Introduction: Despite achieving gender parity among medical and graduate students, women remain underrepresented in academic medical center leadership. This highlights a need for inclusive leadership development programs which impact both individuals and the organization. In response, we developed and evaluated a novel, comprehensive, and collaborative training designed for both mid-career to senior faculty and administrative leaders which addresses leader development and institutional culture.
Methods: A novel 18-month program for faculty and administrative leaders which includes 14 days of immersive workshops, a 360° assessment, personalized executive coaching, and an institutional group project was implemented and evaluated. Pre- and post-program assessments were analyzed using factor analysis to create seven composite scales defining various aspects of leadership competencies. Analysis of survey data used a t-test to determine significantly different scores pre- and post-test for each composite measure.
Results: Participants in this intensive program reported increased agreement with skill development across all competencies except for personal growth, where there was no statistically significant increase, and increased expectations about the program’s ability to enhance recognition, visibility, and opportunities to impress institutional leadership. Over 80% of participants in a five-year follow-up survey found the program beneficial for leadership development, and half of the participants felt the program influenced their decision to stay at their institution long-term. Ninety-four percent of faculty received promotions or new leadership roles within eight years.
Discussion: Determining the impact of leadership programming is difficult but institutional immersive leadership programs have demonstrated significant impact through the advancement of core leadership competencies, faculty and administrative staff promotion, and long-lasting collaborations across the academic medical center. Future comparative studies are needed to look across institutions to determine which elements of the program are most effective.
Keywords: leadership, academic medicine, faculty development, evaluation, women, mid-career, senior leadership
Introduction
Although we have reached gender parity in medical and graduate school student bodies, a persistent paucity of women in academic medical center leadership remains.1,2 Having leadership that represents the overall makeup of the academic health care system is important for representing varying perspectives and creating a group of leaders equipped to better solve problems in health care.3 Supportive measures for mid-career to senior leaders are needed, as female faculty in academic medicine often report lower career satisfaction, higher attrition, and are less likely to hold leadership positions compared to their counterparts.4,5 Training focused on expanding advancement for women at the individual level is often insufficient to create diversification of leadership and oftentimes is focused on faculty or administrative leaders separately.6 In order to address this gap, an expansive leadership model of development is needed which includes intentionality at both the individual and organizational levels. As an academic medical center, we recognized that to address issues of gender equity and the need for leadership training for diverse audiences, we needed to create various leadership training programs. A unique attribute of these programs is that both faculty and administrative leaders intentionally learn together by experiencing the training simultaneously and through peer coaching and/or group projects. While many of our programs are hours to days long, we saw an opening for comprehensive longitudinal training allowing for a depth of leadership concepts and variety of programmatic components while simultaneously evaluating outcomes of this institutional leadership program.
There is very little literature available pertaining to interventions for advancing mid- to senior career women physicians in academic medicine and no identified research on institutional programs with combined administrative and faculty offerings. Recently, Purkey et al published a scoping review of 2,813 existing studies for this population, and when narrowed down to 64 articles, only two of the studies focused on mid- to late-career women physicians.7 Of those two studies, one focused on the Executive Leadership in Academic Medicine (ELAM) Program for Women and the other was a career development program for mid-career women at the University of Rochester School of Medicine and Dentistry.8,9 While ELAM is a nationally known program, enrollment is highly competitive which limits the number of women faculty who can attend. Each academic institution can only send two faculty members per cohort to attend.10 Rochester’s program was developed internally and while it covers a variety of topics such as career planning, communication skills, self-promotion and negotiation skills, the program is only four days long over a six-month period which seems it might prove difficult to cover each topic with significant depth in that timeframe. Additionally, the Association of American Medical Colleges (AAMC) hosts a three-day seminar for mid-career women faculty; however, it also limits how many faculty can attend from the same institution and may be cost-prohibitive for some.11
It appears there is not a similar internally developed, and thus, accessible, program for mid- to senior career women leaders that exists in other academic medical centers where faculty and administrator leaders learn together within the same cohort in the literature. We saw these training gaps as an opportunity with the objective of being innovative and creating collective training where administrators and faculty could learn together, given their focus on the same primary mission of the academic medical institution. We also saw an opportunity to evaluate the program impact as well as capture the evaluation of the program through COVID as a hybrid longitudinal program. We believe an approach that is inclusive of diverse participants, integrates teamwork, 360° leadership evaluations, and a range of learning approaches can have a sustained impact for individuals and academic medical institutions alike. This type of training not only educates leaders but also builds a supportive network that can enable participants to advance in their careers while also creating a positive culture shift within their institution. In this paper, we describe a novel leadership program with these aspects, and analyze outcomes of the program, including career progression of those participants who graduated from the longitudinal program. This study highlights key positive outcomes for participants’ individual leadership journeys including increased confidence in core competencies, overall satisfaction with the program, impact on decisions related to retention, and promotion to advanced leadership positions. Through this data-driven approach, we were able to determine the study’s impact and how this could be scalable at other institutions.
Methods
Rudi Ansbacher Advancing Women in Academic Medicine Leadership Scholars Program (Ansbacher Program)
The Ansbacher Program was designed on the foundation of the Morgan McCall and the Centre for Creative Leadership 70–20-10 learning and development model.12 The 70–20-10 development model emphasizes that 70% of learning comes from experiential or on-the-job learning, 20% comes from mentoring/coaching or developmental relationships, and 10% of learning comes from formal training such as learning experienced in a classroom, reading, podcasts, etc. Recognizing the impact and necessity in diversifying one’s modalities of development, it was critical for learning to occur within these domains in the Ansbacher Program curriculum through 14-days of immersive classroom training (10%), one-on-one executive coaching (20%), and institutional group projects (70%).
The Ansbacher Program is open to all in leadership roles at or above the director level for administrators or associate or higher professor level for faculty, who have a demonstrated commitment to supporting the advancement of women. Since its inception, the program has been open to all genders, however our first male participants joined in the fourth cohort. We began to see male allies show interest in participating once the program gained more recognition. Since the program’s launch in 2014, there have been six cohorts with a total of 142 participants including 111 female and 4 male faculty and 27 female administrative leaders from the University of Michigan (Schools of Medicine, Dentistry, Nursing, Engineering, and Public Health), Wayne State University, The Ohio State University, University of Nevada-Reno, Indiana University, University of Illinois-Chicago, Medical College of Wisconsin, Henry Ford Health, and Virginia Mason Medical Center.
To be considered for the program, interested participants must be nominated by their leader, preferably their department chair. The nomination serves as the leader’s commitment to support the participant through mentorship and sponsorship, while also agreeing to release the potential participant’s time and allow them to fully engage in all the programmatic components. This nomination also allows the review committee to learn how the participants’ leaders may view their future impact within their institution; it provides insight as to whether the participant is being considered a part of a future succession plan and ultimately their broader impact in academic medicine. Qualified participants are invited to complete an application that includes the applicants’ long-term goals, opportunities for growth, demonstrated commitment to equity, their overall interest in participating in the program, a summary of prior leadership training, and two additional recommendation letters from individuals who can speak to the participants’ leadership attributes and impact. In order to mitigate selection bias, each application is reviewed by two members of a selection committee composed of various faculty and administrative leaders who have demonstrated their own investment towards creating an equitable organization as well as previous Ansbacher Program participants. Reviewers are provided a scoring rubric that assesses the strength of applicant’s leadership statement, relevant leadership experience, demonstrated commitment towards equity in alignment with the passion of our program’s donor, overall impression of application materials, and strength of letters of recommendation.
Once admitted to the program, participants experience 14-days of immersive formal workshops focused on developing four fundamental and three differentiating competencies over the course of 18-months (Table 1). Fundamental competencies are core leadership competencies and Differentiators are leadership competencies specific to women in academic medicine.13 Throughout the 18-months of participation, a variety of topics are covered by subject matter experts from the business, higher education, and healthcare fields. The program is broken up into three main sections – leading self, leading others and leading an organization. Each section covers corresponding development that aligns with these sections. The goal of the leading-self portion of the program is to increase participants’ leadership self-awareness and create opportunities in setting intentions on how they want to show up as a leader. This is achieved through a variety of assessments including a 360° leadership evaluation and communication and social styles instruments to provide insights and language on participants’ current behaviors and attitudes. Topics of facilitated sessions include establishing your leadership agenda, emotional intelligence, and creating a leadership vision. The goal for the leading others portion of the program is to build upon the knowledge gained about oneself and apply those learnings in how to lead others. This portion heavily involves experts from the business world, covering topics such as business and financial acumen, conflict management, strategic thinking and crisis management. Participants engage in a virtual simulation, that requires them to assume the role of healthcare executives whose health system is experiencing a significant crisis. The simulation requires participants to apply their learning such as strategic decision making, crisis communication, and teamwork. Lastly, the third portion of the program, leading an organization, allows participants to elevate their learning to think more broadly about leadership and their future impact. The program components associated with this portion include hosting invited leaders to speak with participants about their experiences, pivoting their attention towards their institutional group projects, executive presence and leading change.13
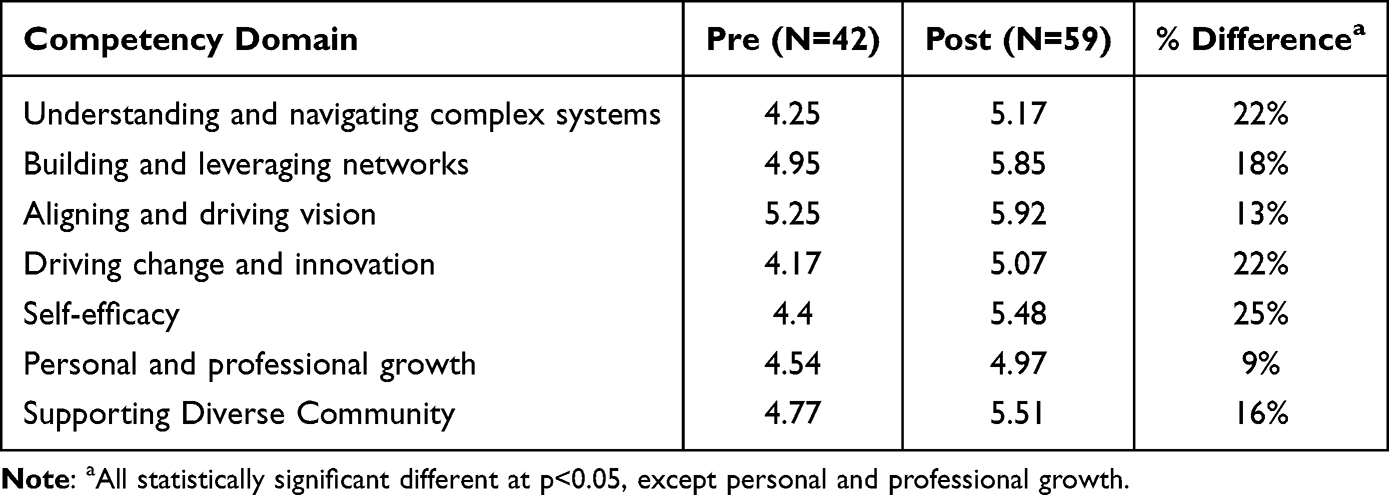 |
Table 1 Mean Scores and Percent Change in Scores for Each Competency Domain Before and After Participation in Ansbacher Program |
In addition to engaging in the 14-days of formal learning, participants each have access to their own executive coach. Executive coaches are senior leaders, both faculty and administrators, who undergo extensive training and certification, whose goal is to engage participants in a customized, tailored way to accelerate participants’ growth and performance.14 The University of Michigan Medical School has been fortunate in developing an executive coaching training program that allows us the ability to train our own senior faculty and administrative leaders to serve as coaches for various leadership development programs. In the Ansbacher Program, the executive coaches’ main role is to analyze participants’ individual leadership 360° assessment, increase participants’ self-awareness, outline participants’ personalized journey for growth while leveraging and implementing the skills learned throughout the training program. Executive coaches are used as catalysts and guides to facilitate the participants’ learning from the classroom into application within their work environments. Participants are typically introduced to their executive coach 3–4 months following the program’s kick-off. This is done intentionally so that participants have familiarity with the program and the initial modules that focus on leading self.
Prior to initiating coaching, participants complete their 360° leadership assessment. This evaluates participants’ leadership competencies and skills (referred to as the Michigan Leadership Assessment, or 360° assessment). The 360° assessment tests for the domains and expectations contained in the Michigan Expectations Model (Figure 1).15 The model is designed to allow University of Michigan leaders to achieve organizational vision and attain organizational goals. It consists of four leadership domains: Mission, People, Self, and Execution. Each domain contains three expectations made up of behavioral indicators. Participants select individuals in manager, direct report, peer, and “other” categories to complete the evaluation. Assessment results are provided to participants during session one. Participants then use this feedback to create their leadership agenda and individual development plan and inform the remainder of their time in the program.16,17 Participants can use this evaluation tool to better guide their utilization of their 6–9 month executive coaching engagement. Participant and executive coach matching is based upon the skill development needs indicated on the participant’s application as well as observable behaviors/opportunities during the training sessions. That data is used to compare the expertise of available coaches to provide the participants with the most aligned and compatible match.
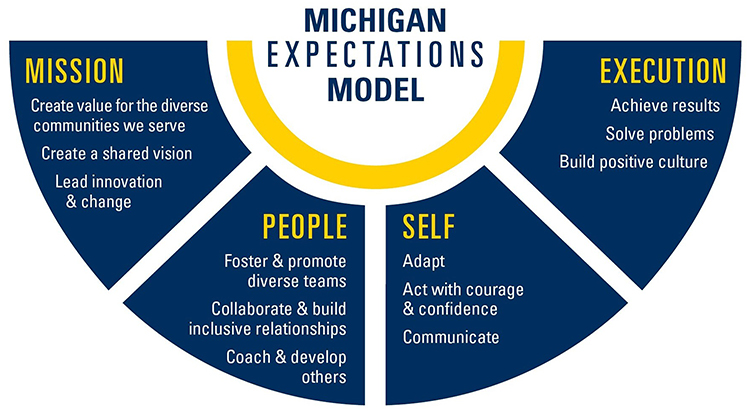 |
Figure 1 Michigan Expectations Model. |
For the experiential learning portion of the curriculum, all participants complete an Institutional Group Project (IGP).18 The literature shows when considering advancement and developmental opportunities for leaders, that action-based learning is one impactful approach.19 The IGP guide was adopted by components utilized through ELAM and a previously hosted University of Michigan Masters Leadership Program. The primary goal of the IGP is to pinpoint an institutional need, address that need by applying their Ansbacher Program learning, and concurrently gain self-exposure within the organization amongst senior leaders. Participants are given the following criteria to consider when brainstorming project ideas early in the program:
- Projects should create visibility both vertically and horizontally across their institutions.
- Projects should demonstrate complexity and are valued to be important.
- Project goals should be SMART (Specific, Measurable, Attainable, Realistic and Timely).
- Projects should be transferable from one academic institution to another.
- Projects should be mindful of what is important to key stakeholders.
Groups are created based upon common project interest, as we have found over the years that when participants were assigned a project, excitement and passion towards the project dropped over time. Group size is between 4 and 7 participants, who begin meeting within the first few months of the program. During the earlier stages of the program, groups are provided feedback from program leadership to help define impact, narrow scope and clarify realistic goals that can be achieved throughout the program. Once an IGP has a defined scope, participants are provided with potential collaborators and/or other leaders who may have a vested interest in this project. During the clarification process of the IGP, groups are encouraged to consider how their projects will improve or impact others, as that can assist in the group’s success in broader adoption. Groups work together for almost 12-months in defining, collecting data, and in some instances, piloting their projects all in anticipation of presenting their final results to a group of institutional executives in hopes of gaining support – both social capital and monetary, towards institutional implementation/adoption of their projects.
IGPs over the years have included: short- and long-term mentoring programs, community building for underrepresented minority faculty, standardizing critical communication channels, and quality improvement for patient care.18 The IGP allows participants a chance to connect with senior and executive leaders, practice skills of communication and influence while improving an organizational need. Under the guidance of Michigan Medicine alumni of the ELAM program, these projects provided much-needed exposure to senior leaders thus providing visibility that is otherwise unobtainable.
Survey Design
Assessment of this leadership training program was based on data acquired in pre- and post-program surveys, as well as real-world outcomes. Example outcomes we sought to identify included 1) stability and advancement in the target profession; and 2) measures of leadership competency and skill development. The pre- and post-survey instruments used were a modification of a questionnaire incorporated in ELAM cohorts.20 It consisted of 44 questions with a seven-point scaled response, plus a set of questions to assess the following: satisfaction with current job and leadership opportunities; expectations of the extent that each program will assist with leadership goals; and current leadership roles applied for, offered, and accepted.20 We created seven composite scales defining various aspects of leadership competencies from the 44 scaled-response items: understanding and navigating complex systems (6 items), building and leveraging networks (10 items), aligning and driving vision (3 items), driving change and innovation (9 items), self-efficacy (8 items), personal and professional growth (4 items), and supporting a diverse community (3 items). Promotions for faculty and staff were assessed by the Board of Regents faculty rank promotion approvals, promotional announcements from participants, and internet searches of previous titles versus current titles.
Surveys were sent to the first four cohorts of Ansbacher participants each averaging 21 participants, for a total of 87 subjects composed of faculty (66 female, 2 male) and 19 female administrative leaders. The University of Michigan Institutional Review Board (IRBMED) determined that this evaluation does not require IRB approval because it does not satisfy the definition of research under 45 CFR 46.102(d), 21 CFR 56.102(c), or U-M policy as described in Human Research Protection Program Operations Manual Part 4. Additionally, IRBMED stated that in accordance with the United States Department of Health and Human Services Office for Human Research Protection (OHRP) FAQ about quality improvement activities, there is no requirement for such activities to undergo review by an IRB, or for these activities to be conducted with provider or patient informed consent.
Survey Analysis
We assessed the internal consistency utilizing power analyses for the seven leadership competencies for both the pre- and post-tests and all Cronbach alphas exceeded.86. Analysis of survey data used t-tests to determine significantly different scores for pre- and post-test groups. Tests for normality and homoscedasticity were performed for both groups. Since there were minor deviations from normality for some scales, the Wilcoxon rank-sum test was performed as an alternative to the independent two-sample t-test to confirm the results. For all scales, the nonparametric tests confirmed the results from the original t-tests.
Results
The response rate for the combined Ansbacher Program cohorts was 68%. Table 1 shows the mean scores and percent change in scores for each competency domain before and after the program. Scores ranged from 1 (strongly disagree) to 7 (strongly agree). Participants in the Ansbacher Program reported increased agreement with skill development across all competencies except for personal growth, where there was no statistically significant increase in confidence level.
Participants were also asked about their expectations of the program using a Likert scale of 1 (strongly disagree) to 7 (strongly agree). In comparing pre- vs post-test responses, Ansbacher Program participants reported significantly higher program expectations at post-test that the program would provide them with skills necessary to attain recognition, would help them become more visible at their institution, and would create opportunities to impress institutional leadership (Table 2). A recent alum of the Ansbacher Program was quoted in their institutional newsletter as saying, “This experience has been invaluable at this stage of my career and during the pandemic to hone new skills for the benefit of those that I serve.”21
 |
Table 2 Mean Scores for Program Expectations Before and After Participation in Ansbacher Program |
Promotions in rank and the appointment to leadership positions by faculty and staff were also tracked for up to eight years post participation. Among the 68 faculty members who attended the Ansbacher Program, 94% (n=64) received a promotion in rank or held a new leadership position up to eight years following participation (Table 3).
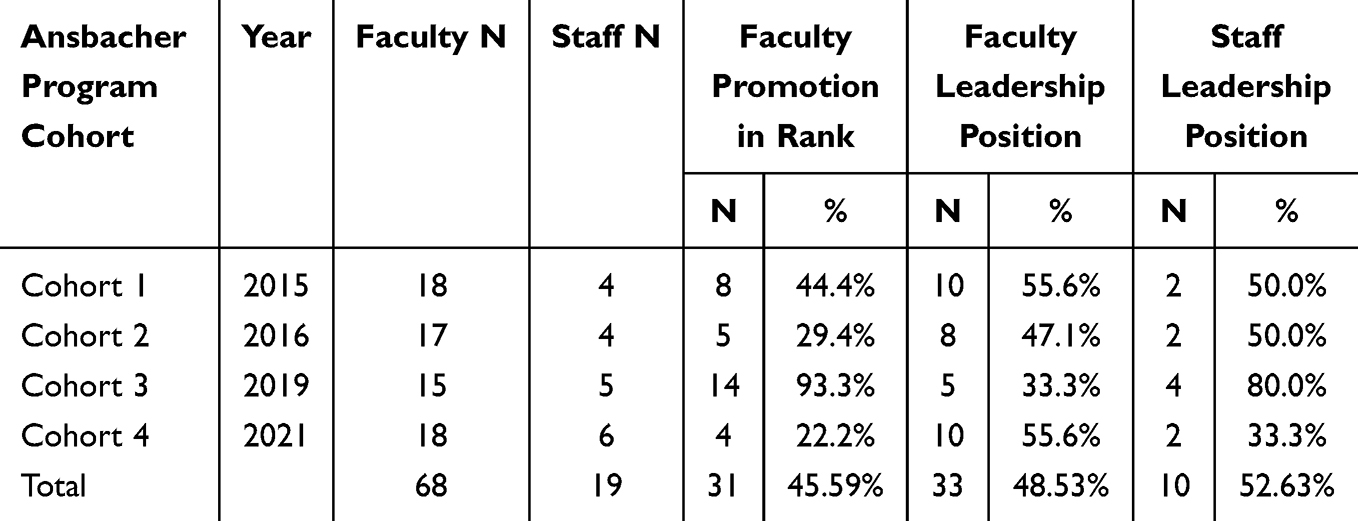 |
Table 3 Change in Position and/or Status for Ansbacher Program Participants |
Five-Year Follow-Up
In addition to examining promotion and leadership rates, a five-year follow-up survey was sent to the initial Ansbacher Program cohort (2015) to further understand the impact of the program on skills gained. The response rate for this survey was 76%. Table 4 shows the percentage of participants from the 2015 cohort who agreed that the program added value to their leadership journey. Over 80% of participants agreed that the program helped support their career advancement, taught them skills on how to attain recognition, gave them strategies for achieving leadership aspirations, and improved interpersonal skills related to team leadership. One participant stated, “It was a wonderful experience, and I still treasure the friendships and professional growth I attained by participating.” Another participant mentioned “The program is excellent (content, skill development, networking, etc). It definitely helped me develop as a leader.” Almost 90% of surveyed participants utilized techniques learned in the program to gain support for new ideas. Establishing collaborations with peer leaders across the institution and maintaining contact with their program cohort were the only areas where participants had less than 60% agreement. The survey asked participants if their involvement in the Ansbacher Program influenced their decision to remain at their organization for at least 5 years, and 50% responded positively that the program did contribute in some capacity in their decision.
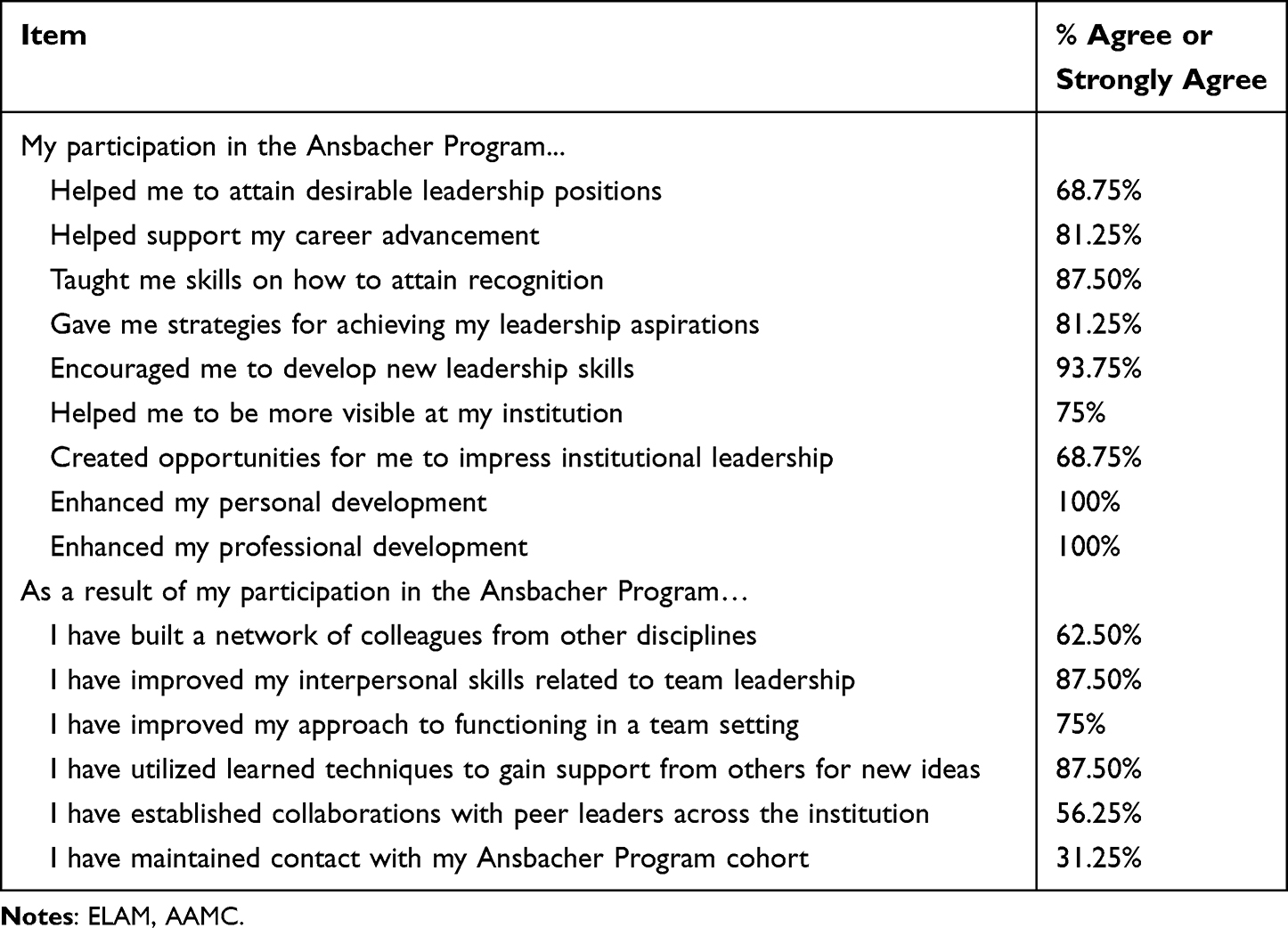 |
Table 4 % of Participants in the Original Ansbacher Program Cohort That Agreed or Strongly Agreed with the Following Statements Regarding Their Participation (N=16) |
Discussion
The leadership development journey we have taken with collaborative learning amongst cohorts of combined faculty and administrative leaders in academic medicine has been highly successful. By aligning participants’ 360 assessments with our institutional competency model, we have cultivated leadership practices and behaviors that create an ideal organizational culture and allow participants to advance in diverse areas of academic medicine. This was demonstrated by key positive outcomes including increased confidence in core competencies, overall satisfaction with the program, impact on decisions related to retention, and promotion to advanced leadership positions.
Our intensive Ansbacher Program has had significant positive gains in leadership competency development, personal career trajectories, and networking (Table 2). Along with these quantitative survey data pieces, we have been impressed with the number, diversity, and impact of the roles our participants have taken on in the health care system and medical school. Another aspect that is captured through participant feedback is the impact of the alumni network created through this collaborative learning amongst faculty and administrative leaders. Further, we have been able to maintain the integrity of the program while pivoting to a virtual platform that opens the possibility of offering future cohorts a hybrid in-person/virtual model, while also remaining nimble to the needs of leaders in academic medicine.
Theoretical Implications
National programs for women leaders demonstrate the impact on personal skills and network-based learning that drives career advancement. A similar program for women faculty leaders at Drexel University College of Medicine, ELAM found similar results in that participants showed gains in their leadership skills, career trajectory, networking, and increased visibility at their respective institutions.20 Given that such resources are limited to a few nominations and are oftentimes intensive, institutional programs are important to expand the development of emerging and future leaders as we continue to build the bench of experienced women leaders within academic medicine. Another identified benefit of this program was shared learning of administrative leaders and faculty across the health system. Over the years, we have heard from our participants how they feel there is a significant impact and value in having both faculty and administrative leaders together in the program – the learning space created frequent and safe opportunities to learn about others’ perspectives and identify ways to improve collaboration. The more we explore leadership development in academic medicine, the clearer we see how our program stands out. In addition, assessments of participants engaged in leadership development programs are critical in understanding learning and promotion outcomes. It is important for faculty development offices in academic medical centers to understand outcomes for programming. There is something to be said in allowing leaders ample time to not only become aware of a concept but to also have a space and community to apply that learning, receive feedback about their experience and experiment again on their learned skill. The Ansbacher Program was designed to allow participants to increase their confidence in their ability to behave like a leader, not only how to think as one – in conjunction with the program’s longitudinal nature, incorporation of executive coaching, and the strong emphasis on network building, we have been able to make a difference on the 100+ leaders who have attended the program over the last decade. This model over the six cohorts of this program with evaluation and responding to feedback and needs is what allowed us to pivot during COVID and continue to have impactful programming.
Practical Implications
In addition to greater numbers of participants, an institutional program can be more cost effective than sending faculty to a national program where they must pay for lodging, meals, travel, and tuition. It also allows for better work-life integration to stay local while bringing in outside attendees helps to grow their network and can alleviate some internal costs. We recognize and have benefitted tremendously by having other organizations sponsor their leaders to attend. We want to share with organizations, that no matter if you are sponsoring a leader to attend a development program or considering creating your own institutional program, we must continue to invest, develop and sponsor women leaders within academic medicine. We also recognize that a practical implication of our institutional program is the ability to align with specific institutional priorities and to build leadership skills towards those priorities. Lastly, another outcome resulted in building new, long-lasting collaborations across the health system as demonstrated in our five-year outcomes.
Limitations and Future Research
Evaluation of programs is critical to understand the impact for both individual careers and the institution. By surveying our participants we identified key areas where our program can evolve. We identified opportunities in learning related to how to improve personal and professional growth scores and for participants to lead at the institution instead of having to go elsewhere. While our group has identified possible solutions including enhanced institutional sponsorship, these are limitations of our program and future areas of focus. Although our data shows that participants find the Ansbacher Program impactful, our survey design limits our ability to specifically identify what components of the program directly contribute to participant outcomes. In terms of true evaluation of outcomes, we also recognized through this process of evaluation there were difficulties determining an appropriate control group to survey given that selected individuals were mid-level to senior leaders and had their leadership’s support and nomination. For future studies, we plan to look at comparative studies across institutions to determine program effectiveness. Currently, there are few similar programs to act as comparators. We also identified difficulties in measuring incremental role advancement to new opportunities that may have a similar level of leadership. An opportunity for future evaluation would be to explicitly capture data on the impact each cohort’s network has on participants, both in the short and long term. Lastly, we identified that many of our participants felt the need to leave the institution to advance, which made tracking advancement difficult, and meant that our institutional investment would impact the field more than just our institution directly.
Conclusion
While this evaluation has played a role in our revisions of these programs, there are several limitations to our study. While we had considered a control group, the competitive application for this program makes participant bias likely and random assessment infeasible. Several participants received leadership promotions outside of the organization. We view these promotions as an organizational success and hope to continue to build our reputation in developing women leaders in academic medicine broadly.
As we think about continued expansion for the program, one consideration is how to intentionally bring men along as participants and measuring what difference, if any, the program has on their leadership development. We also recognize that we are building women leaders at the individual level and yet, to make a significant impact in gender equity, there must be systematic level changes and the dismantling of hierarchical practices that disproportionately impact women advancing in academic medicine.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Bates C, Gordon L, Travis E, et al. Striving for gender equity in academic medicine careers: a call to action. Acad Med. 2016;91(8):1050–1052. doi:10.1097/ACM.0000000000001283
2. Lautenberger DM, Dandar VM, Raezer CL, Sloane RA. The State of Women in Academic Medicine: The Pipeline and Pathways to Leadership, 2013-2014. 2014.
3. Page S, Cantor N, Lewis E. The diversity bonus: how great teams pay off in the knowledge economy. 2019.
4. Cropsey KL, Masho SW, Shiang R, Sikka V, Kornstein SG, Hampton CL. Why do faculty leave? Reasons for attrition of women and minority faculty from a medical school: four-year results. J Women's Health. 2008;17(7):1111–1118. doi:10.1089/jwh.2007.0582
5. Peterson NB, Friedman RH, Ash AS, Franco S, Carr PL. Faculty self-reported experience with racial and ethnic discrimination in academic medicine. J Gen Intern Med. 2004;19(3):259–265. doi:10.1111/j.1525-1497.2004.20409.x
6. Kossek EE, Buzzanell PM. Women’s Career Equality and Leadership in Organizations: Creating an Evidence‐based Positive Change. Wiley Online Library; 2018:813–822.
7. Purkey NJ, Han P, Woodward A, et al. Advancing women physicians in academic medicine: a scoping review. Acad Med. 2024;
8. Dannels SA, Yamagata H, McDade SA, et al. Evaluating a leadership program: a comparative, longitudinal study to assess the impact of the Executive Leadership in Academic Medicine (ELAM) Program for Women. Acad Med. 2008;83(5):488–495. doi:10.1097/ACM.0b013e31816be551
9. Chaudron LH, Anson E, Bryson Tolbert JM, Inoue S, Cerulli C. Meeting the needs of mid-career women in academic medicine: one model career development program. J Women’s Health. 2021;30(1):45–51. doi:10.1089/jwh.2019.8062
10. Drexel University College of Medicine. Executive leadership in academic medicine application information. Available from: https://drexel.edu/medicine/academics/womens-health-and-leadership/elam/how-to-apply/.
11. AAMC. Mid-career women faculty leadership development seminar. Available from: https://www.aamc.org/career-development/leadership-development/midwims.
12. Center for Creative Leadership. The 70-20-10 rule for leadership development. Available from: https://www.ccl.org/articles/leading-effectively-articles/70-20-10-rule/.
13. Lantz PM. Gender and leadership in healthcare administration: 21st century progress and challenges. J Healthc Manag Sep-Oct. 2008;53(5):291–301.
14. Schidlow DV, Siders CT. executive coaching in academic medicine - the net under the tightrope. Physician Leadersh J. 2014;1(2):60–2,64.
15. University of Michigan Organizational Learning. Michigan expectations model. 2023. Available from: https://hr.umich.edu/working-u-m/professional-development/learning-development-models/michigan-expectations-model.
16. University of Michigan Organizational Learning. Individual development plan. 2023. Available from: https://hr.umich.edu/sites/default/files/final-idp.pdf.
17. University of Michigan Organizational Learning. Individual Development Plan Faculty Edition. Available from: https://hr.umich.edu/sites/default/files/faculty-idp.pdf.
18. University of Michigan Office of Faculty Affairs & Faculty Development. AWIAML Projects. Available from: https://docs.google.com/document/d/1pe9Rz_f-Q7lAkXssoPYMHdzgKAgwxlYtLL8v3loSTnw/edit?usp=sharing.
19. Tichy NM, DeRose C. Action Learning: Simultaneous Development and Succession Planning. In: ATD Talent Management handbook. ATD Press; 2016:275–290.
20. Jagsi R, Spector ND. Leading by design: lessons for the future from 25 years of the Executive Leadership In Academic Medicine (ELAM) program for women. Acad Med. 2020;95(10):1479–1482. doi:10.1097/ACM.0000000000003577
21. School of Medicine News. Three more letters behind M.D.: how a M.O.M. in medicine discovered the best of both worlds. 2021. https://today.wayne.edu/medicine/news/2021/03/22/three-more-letters-behind-md-how-a-mom-in-medicine-discovered-the-best-of-both-worlds-41965.
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.