Back to Journals » Patient Preference and Adherence » Volume 20
A Four-Year Monocenter Epidemiological Analysis of 30-Day Unplanned Readmission Patients
Authors Chen Q, Rao D, Liang Y, Li Y, Wang H, Liu A, Huang J
Received 2 January 2026
Accepted for publication 2 May 2026
Published 19 May 2026 Volume 2026:20 593242
DOI https://doi.org/10.2147/PPA.S593242
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Johnny Chen
Qiuchan Chen,1 Dongping Rao,2 Yuanhao Liang,3 Yongfeng Li,2 Haiqin Wang,1 Ai Liu,1 Jing Huang1
1Nursing Department, Jiangmen Central Hospital, Jiangmen, Guangdong, People’s Republic of China; 2Medical Quality Management Division, Jiangmen Central Hospital, Jiangmen, Guangdong, People’s Republic of China; 3Clinical Experimental Center, Jiangmen Engineering Technology Research Center of Clinical Biobank and Translational Research, Jiangmen Central Hospital, Jiangmen, Guangdong, People’s Republic of China
Correspondence: Jing Huang, Nursing Department, Jiangmen Central Hospital, Jiangmen, Guangdong, 529000, People’s Republic of China, Tel +8607503365067, Email [email protected]
Purpose: Describe the distribution and clinical characteristics of unplanned readmission patients.
Patients and methods: This study employed a retrospective observational design to investigate patients who were unplanned readmissions at a general hospital in Guangdong Province between January 2016 and December 2019. It compared and analyzed the distribution patterns and clinical characteristics of patients readmitted unplanned across different subgroups.
Results: We collected data on 15,585 patients. Among unplanned readmissions, patients aged 41 or older (10,618, 68.13%), females (8243, 52.89%), married individuals (10,660, 68.4%), and employees (3834, 24.6%) had higher proportions. Most patients had some form of insurance (12,026, 77.16%). Significant differences were observed in the sociodemographic statistics of unplanned readmission patients across different time periods. The average duration of unplanned readmission was approximately two weeks. Among patients aged 41 and above, nearly half (6803; 43.65%) had unplanned readmissions lasting more than 2 weeks. Most patients had undergone surgery (11,395, 73.12%), with the highest proportions undergoing urological (2575, 16.5%) and gynecological (2437, 15.6%) surgery.
Conclusion: Unplanned readmission patients are primarily middle-aged and older adults aged 40 and above, women, married individuals, and employed persons. They bear a heavy disease burden, and while most have health insurance, a significant proportion remain uninsured. These patients are mainly referred from surgical departments, particularly urology and obstetrics and gynecology. Unplanned readmissions most frequently occur within two weeks of discharge, and hospitalization costs rise significantly with age; therefore, greater attention should be paid to this issue in discharge instructions.
Keywords: unplanned, readmission, insurance, hospital, epidemiological analysis
Background
Recent research in the medical field has increasingly focused on strategies to reduce unplanned readmission rates. Short-term unplanned readmissions have become a key global indicator of healthcare quality. This metric not only directly reflects the quality of medical services but also plays a crucial role in strengthening hospital service management and identifying and improving deficiencies in medical procedures.1 An unplanned readmission refers to a readmission to the hospital within 30 days for any unplanned reason, excluding planned readmissions.2 Unplanned readmissions are closely linked to poor outcomes, excessive use of healthcare resources, and pressure on health insurance payments. Unplanned readmissions are a widespread phenomenon worldwide. A systematic review indicates that approximately one-quarter of readmissions in medical, surgical, and geriatric care could be prevented by optimizing care processes.3 In Australia, for example, there are more than 600,000 potentially avoidable unplanned readmissions each year.4 Under US health insurance coverage, the readmission rate is approximately 17.5%, and such readmissions result in annual losses of over $17 billion for health insurers.5,6 To address this challenge, many countries have incorporated 30-day readmission rates into their hospital performance evaluation and payment systems, such as the Hospital Readmission Reduction Program (HRRP) in the United States and the German Diagnosis-Related Groups (G-DRG) system, with the aim of curbing inappropriate early discharges and strengthening continuity of care.7,8
Currently, North America has established hospital-wide readmission metrics covering multiple specialties to drive systematic quality improvement. However, epidemiological studies of unplanned readmissions in large populations remain relatively limited in other countries, with most focusing on specific diseases or surgical populations.9,10 There is a lack of systematic epidemiological descriptions of unplanned readmissions to inpatient care across all age groups. In particular, there is a lack of systematic analysis of non-surgical departments and regional healthcare networks. Therefore, conducting an in-depth examination of the incidence and distribution patterns of unplanned readmissions is of significant practical importance for optimizing post-discharge management strategies and reducing the risk of avoidable readmissions.
Methods
Between January 2016 and December 2019, this study included 15,585 cases of unplanned readmissions, which were verified by the Medical Records Department of a hospital in Guangdong Province. The data for this study were derived from four years (2016–2019) of complete inpatient data from the hospital’s electronic medical record system. The integrity of case inclusion was ensured through a standardized data extraction process conducted by the hospital’s information technology department. Given that patients who voluntarily discharged lacked a complete treatment history and that deceased patients no longer faced the risk of readmission, this study excluded patients who voluntarily discharged (n = 320) and deceased patients (n = 270).
We identified all patients admitted to a Grade A Level 3 general hospital in Guangdong Province between January 1, 2016, and January 1, 2020, who experienced a first unplanned readmission within 30 days of discharge. Doctors had already decided whether to admit each patient for an unplanned readmission. Excludes scheduled readmissions (such as chemotherapy, follow-up surgery, or postoperative suture removal). Inpatients of all ages and from all clinical departments were included. We developed a medical utilization data collection form covering multiple dimensions, including patients’ sociodemographic characteristics, length of stay, medical costs, and insurance status. Surgery was defined as a procedure performed during the patient’s previous hospitalization, identified using ICD-9-CM-3 coding. Resuscitation was defined as life-saving interventions received during the previous hospitalization, identified through temporary physician orders for “resuscitation of critically ill patients” or by searching for the keyword “resuscitation” in the patient’s medical records. All data were sourced from electronic medical records. To ensure data completeness and comprehensiveness, the hospital’s electronic medical record system enforces mandatory entry and logical validation rules for all key fields relevant to the study; incomplete records cannot be submitted. We used ICD-10 codes to identify patients with co-coded hypertension and diabetes. For patients with multiple hospitalizations during the study period, this study defined the first admission as the reference event and limited the analysis to the first unplanned readmission occurring within 30 days of discharge. This approach ensured the completeness of all patient records included in the analysis. In addition, patients who were readmitted for specific planned purposes, discharged through an automated process, or were still recovering; as well as those for whom key variables such as age, gender, hospitalization costs, and health insurance type could not be extracted from the electronic medical records were excluded from the study.
Ethical Aspects
This study was conducted in accordance with the ethical standards of the Jiangmen Central Hospital Ethics Committee (approval number: [2023–262]) and with the Declaration of Helsinki. We engaged a diverse group of participants and stakeholders, instructing them to align with the guidelines on patient records while ensuring the confidentiality of patient identities. The findings were published only after all patient identity information had been anonymized. As this was a retrospective analysis of de-identified data, no consent was required following ethical approval.
Statistical Analysis
Statistical analysis was performed using SPSS version 25.0. Continuous variables were expressed as mean ± SD, and data distributions were illustrated using pie charts. Categorical data were described as frequency and percentage. Comparisons between groups were conducted using the chi-square test or Fisher’s exact test, as appropriate. All data were entered after the patient was admitted to the hospital, so no missing data were found.
Results
This study included a cohort of 15,585 patients, distributed across 34 wards. Over the four-year period from 2016 to 2019, the annual patient numbers were as follows: 3869 in 2016, 4336 in 2017, 3414 in 2018, and 3966 in 2019. Using 2016 as the baseline, the subsequent rates of change were 12.07% increase, 11.76% decline, and 2.51% increase.
Table 1 presents the sociodemographic characteristics of patients categorized by the number of days until unplanned readmission. The average age was recorded as 50.26 ± 20.31 years. Women constituted a higher proportion of the sample (8243; 52.9%). The largest demographic within this patient group was those who were married (10,660; 68.4%). Regarding occupational distribution, employees formed the largest segment, followed by those who were retired or unemployed. The majority of patients had medical insurance. Hypertension and diabetes were the most frequently represented chronic conditions in this cohort. The analysis revealed that most unplanned readmission patients did not suffer from these conditions. Significant statistical differences were observed in the sociodemographic characteristics of patients across different readmission intervals, including age, gender, marital status, occupation, medical insurance status, presence of chronic conditions (hypertension/diabetes), length of hospital stay, costs associated with two hospitalizations, rescue interventions, and surgical procedures.
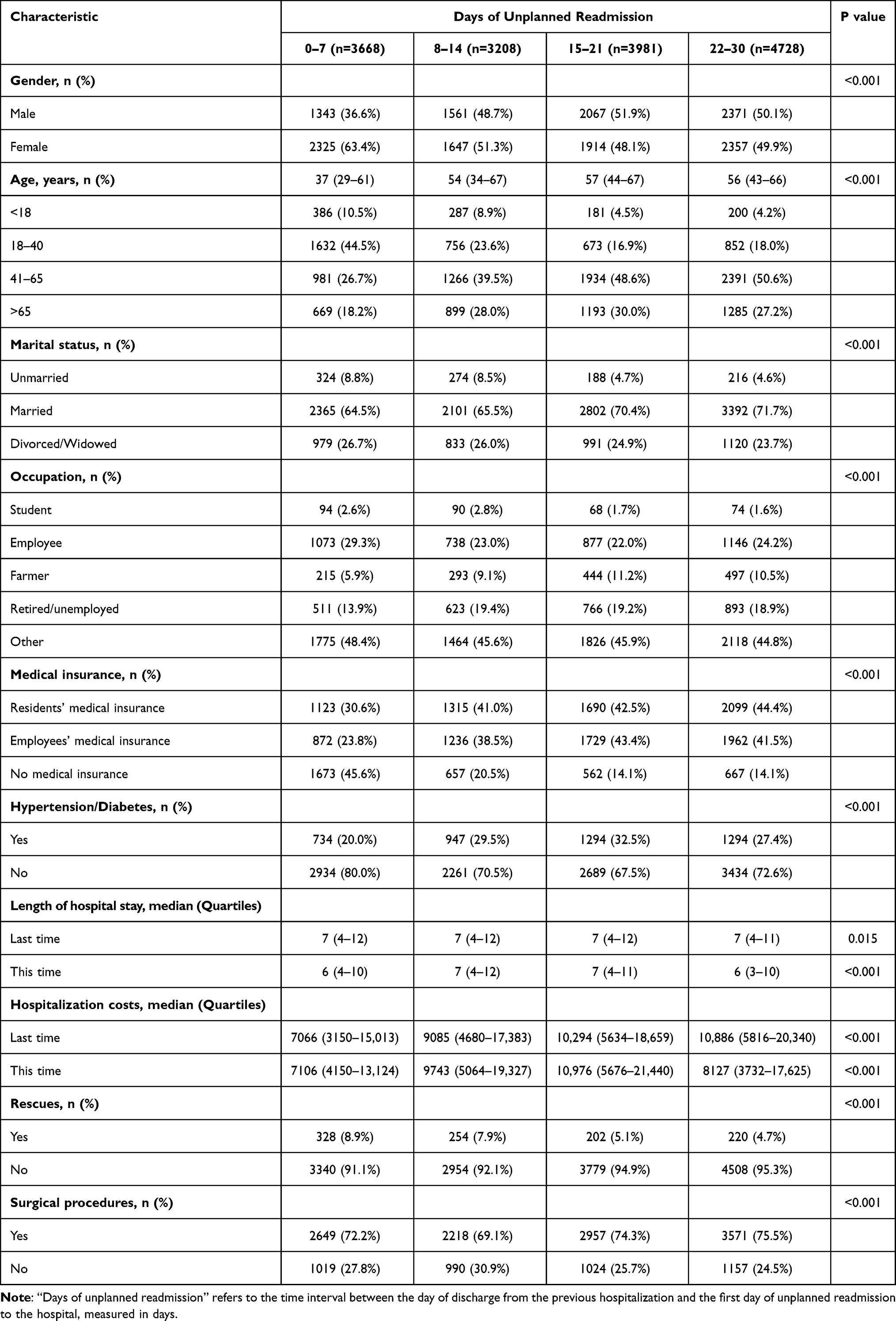 |
Table 1 Sociodemographic Characteristics of Patients with Different days of Unplanned Readmission |
To further elucidate the distribution patterns of patients with unplanned readmissions, an in-depth analysis was conducted focusing on age groups and surgical conditions (refer to Tables 2 and 3). The findings reveal that the majority of readmissions occur within two weeks. The median hospitalization cost increases with age, particularly among individuals aged 41 and older, where it has exceeded 10,000 yuan. The majority of these patients have undergone surgical procedures. There are substantial statistical differences in the distributions of gender, marital status, occupation, days of unplanned readmission, medical insurance coverage, chronic disease prevalence, the number of patients readmitted within four years, length of hospital stay, hospitalization costs, rescue efforts, and surgical history across different age groups.
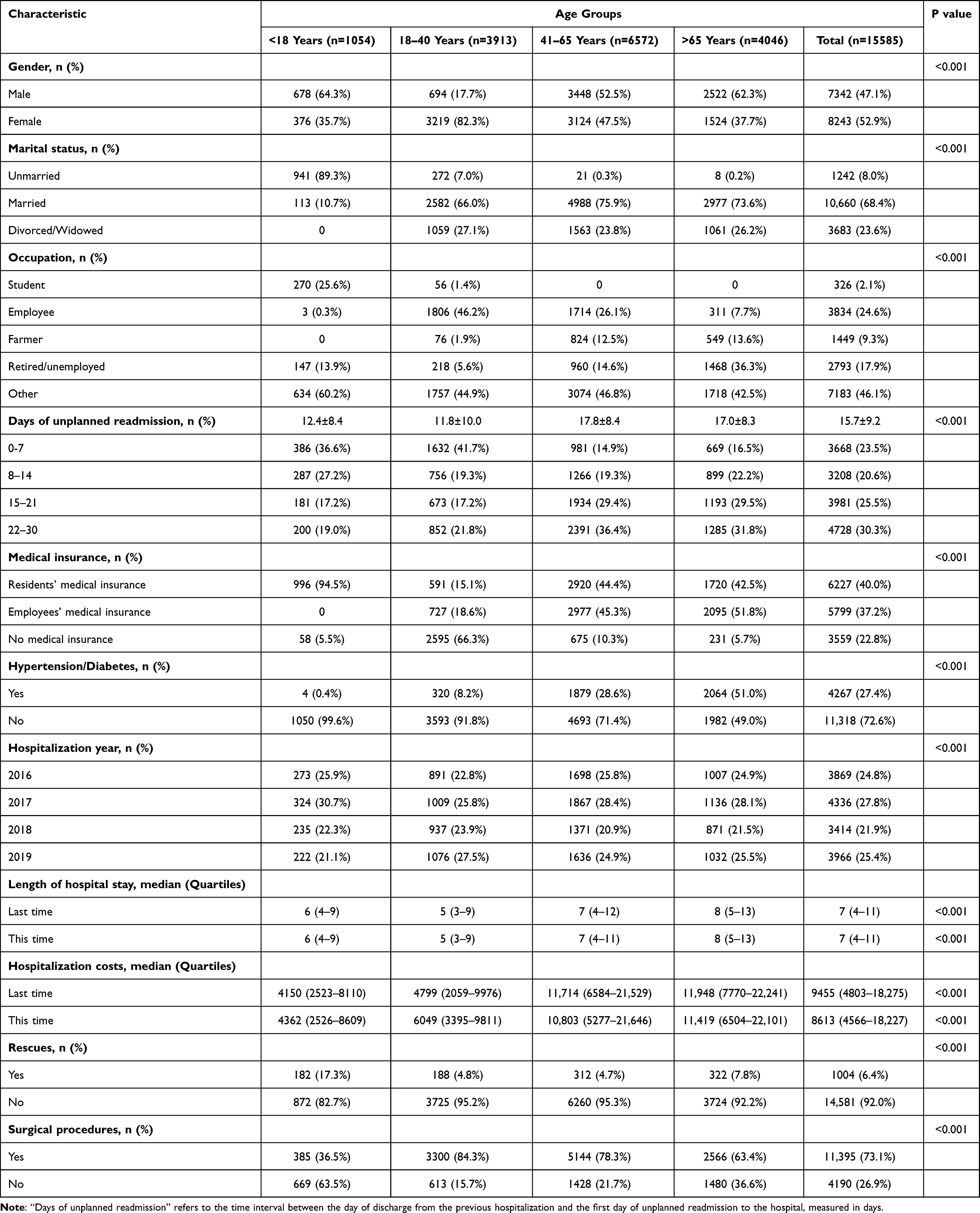 |
Table 2 Sociodemographic Characteristics and Admission Status of Unplanned Readmission Patients by Different Age Groups |
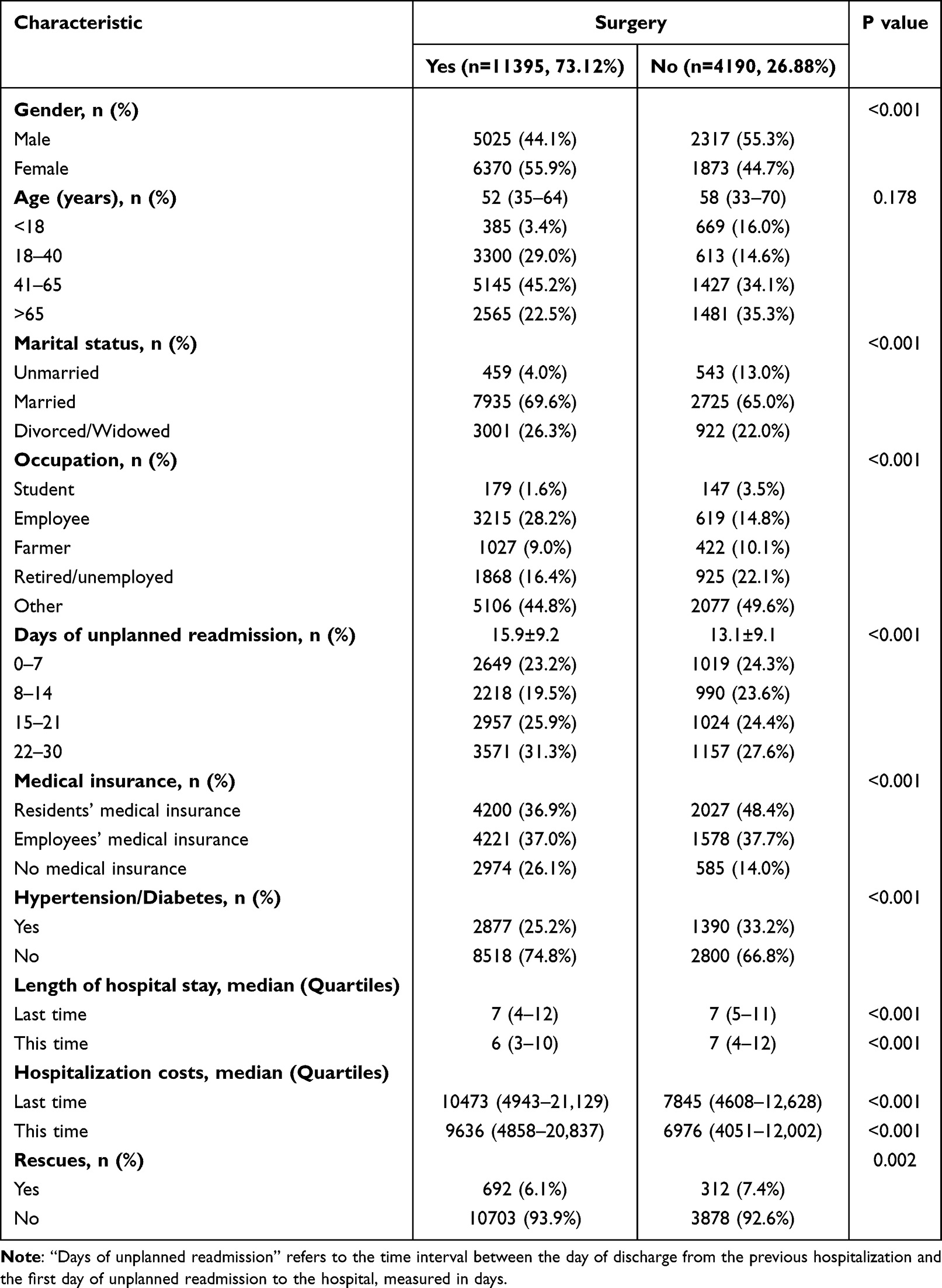 |
Table 3 Sociodemographic Characteristics and Admission Status of Unplanned Readmission Patients by Surgery |
Between 2016 and 2019, a total of 211 patients died following unplanned readmissions, with annual death tolls of 69, 36, 24, and 83, respectively. Over this period, the average and median durations from unplanned readmission to death were 18.49 days and 12 days, respectively. The annual breakdown of these figures is as follows: 20.68 days average and 14 days median in the first year; 15.11 days average and 10.5 days median in the second year; 11.61 days average and 7 days median in the third year; and 20.05 days average and 12 days median in the fourth year. The all-cause mortality rates per thousand for the four years were 13.54‰, with annual rates of 17.83‰, 8.3‰, 7.03‰, and 20.96‰, respectively.
Additionally, this study examined the sociodemographic characteristics of both surgical and non-surgical patients, categorizing individuals based on their surgical history. Significant statistical differences were observed between the two groups for gender, marital status, occupation, days of unplanned readmission, medical insurance coverage, chronic disease prevalence, length of hospital stay, hospitalization costs, and rescue interventions.
Figure 1 illustrates the distribution of patients with unplanned readmissions across various departments. More than 70% of these patients originate from surgical departments, with urology and obstetrics accounting for the highest proportions, representing 17% (2575 patients) and 16% (2437 patients) respectively.
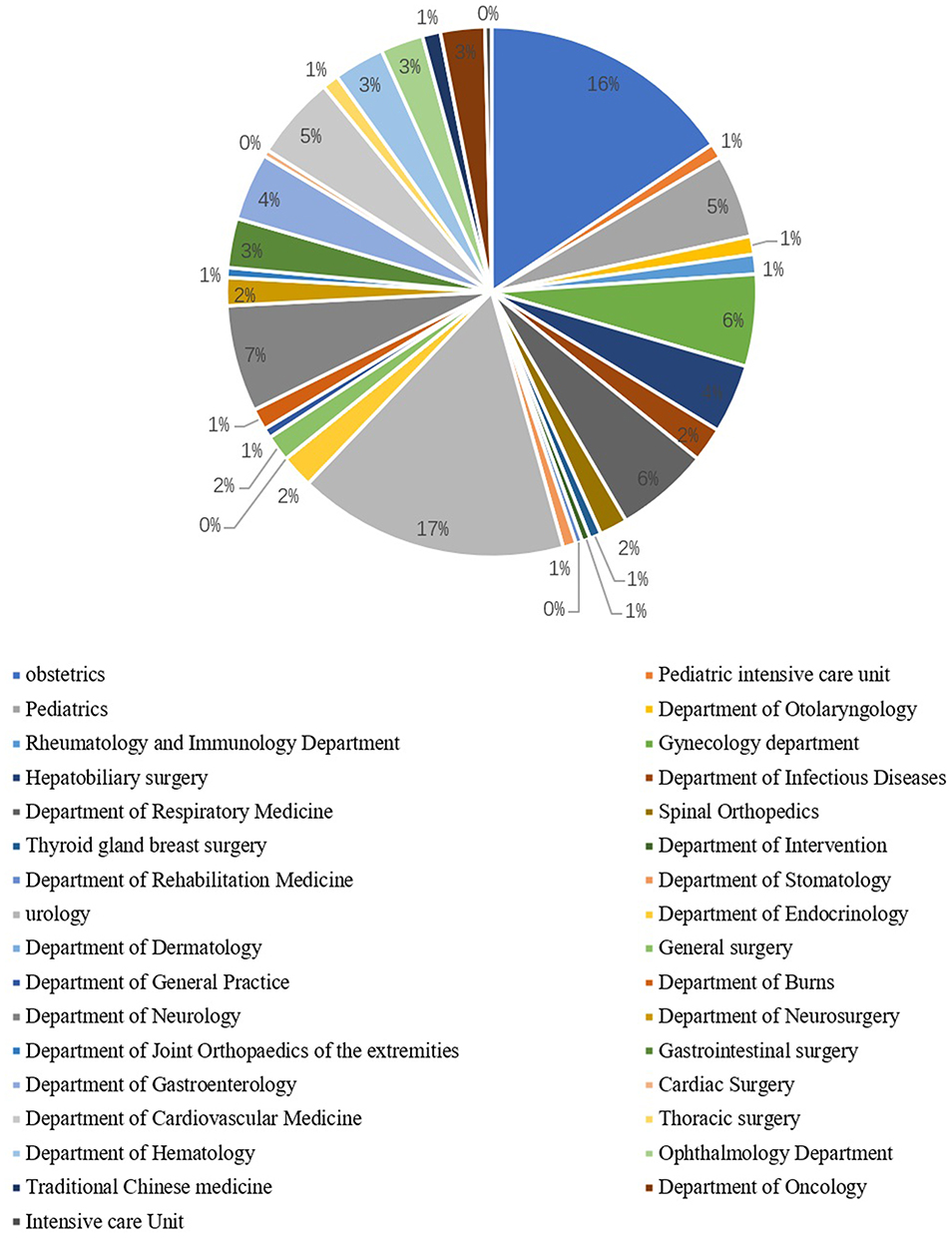 |
Figure 1 Department distribution of unplanned readmission patients. Among the unplanned readmission patients included in this study, the departments with the highest proportions were urology (17%) and obstetrics (16%). The other departments were more evenly distributed, with most having a proportion of less than 5%. |
Discussion
Among patients experiencing unplanned readmissions, those aged 41 and older tend to have more complex medical conditions, which may increase the risk of subsequent readmissions. There are significant differences in sociodemographic characteristics among patients across age groups and unplanned readmission durations. The largest proportion of these patients falls within the 41–65 age group, followed by those aged 65 and older, and then those aged 18–40. This observation is consistent with previous studies’ findings.11–13 Patients under the age of 41 typically experience an unplanned readmission within two weeks. In contrast, for patients aged 41 and older, the duration of hospitalization often exceeds two weeks, and hypertension and diabetes are common comorbidities. Patients with a history of surgery tend to have longer hospital stays, which may result in higher medical costs. Furthermore, the incidence of physical complications increases with age, underscoring the importance of providing personalized medical guidance for elderly patients. Medical care for the elderly requires close attention.
It is worth noting that nearly half of patients who experience unplanned readmissions within seven days lack health insurance. Health insurance plays a crucial role as a risk-sharing mechanism in the healthcare system, underpinning the provision of essential medical services. China’s health insurance system covers the majority of residents and employees, safeguarding the health of both urban and rural populations. A large body of research indicates that medical costs have a significant impact on patients’ healthcare decisions and overall health status.14–16 Under current conditions, basic health insurance meets the medical needs of insured individuals to a certain extent. However, it does not cover all medical needs that fall outside its scope. In light of this, it is essential to acknowledge the diverse needs of patients and establish a multi-tiered insurance framework that prioritizes basic health coverage while allowing commercial health insurance to provide additional support.
Our study shows that more than half of people aged 18 to 40 lack health insurance, suggesting that the young workforce and the uninsured may be at a relative disadvantage among those experiencing unplanned readmissions. This disparity may stem from issues such as healthcare billing models, reimbursement criteria, and insufficient behavioral guidance, resulting in an excessively high out-of-pocket cost burden for this age group.17–19 Consequently, there is an urgent need for policy and welfare systems to enhance support in this area. This group is not only pivotal to the societal labor force but also a cornerstone of household income.
Patients with a history of surgery are more prone to unplanned readmissions, with obstetric and urological patients identified as key demographic groups. Several studies have suggested that the severity of the condition and surgical complications are principal factors contributing to high rates of readmission.20–22 Inadequate assessment of a patient’s condition by the attending physician at discharge can increase the risk of unplanned readmission, often due to premature discharge or poor compliance with post-discharge treatment protocols. To mitigate this issue, hospitals should improve their clinical management practices by accurately assessing whether patients meet the discharge criteria and implementing effective communication strategies before discharge.23 Additionally, enhancing the whole cycle of discharge readiness work in hospital, actively utilizing internet resources for early disease recognition and home care guidance, and optimizing community healthcare resource allocation are crucial.24–26 These measures will improve service capacity and quality, effectively guiding patients in seeking appropriate medical care and thus reducing the incidence of unplanned readmissions due to inadequate or improper treatment post-discharge.27–30
Limitations
This retrospective study does not allow for causal conclusions due to its design. Certain factors were excluded from the analysis due to limitations in the available data. Since we do not have access to certain information on patients’ hospital stays at other hospitals, we did not include the number of readmitted patients from those hospitals into our statistics; this may introduce a bias in our estimates. Future research should aim to further refine and expand the dataset. The initial survey was conducted before the COVID-19 pandemic; forthcoming studies will incorporate pandemic-era data to evaluate the influence of uncontrollable factors. Additionally, future investigations will expand the sample size and include a causal analysis of selected predictive factors.
Conclusions
In summary, patients readmitted for unplanned reasons are primarily middle-aged and elderly individuals over 41 years of age, women, married individuals, and employed persons. They bear a heavy disease burden, and while the majority have health insurance, a significant proportion remain uninsured. Patients primarily come from surgical departments, particularly urology and obstetrics and gynecology, and a history of surgery is a key characteristic. Although hypertension and diabetes are common comorbidities, they do not constitute the main group of readmitted patients. Readmissions most frequently occur within two weeks of discharge, and hospitalization costs rise significantly with age. This suggests that discharge instructions and the allocation of medical resources should be strengthened for the elderly, postoperative patients, and those without health insurance to reduce the risk of unplanned readmissions.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; All authors took part in drafting, revising or critically reviewing the article; All authors gave final approval of the version to be published; All authors have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This work was supported by the Jiangmen Association for Science and Technology [grant numbers 7, 2024]. The funder did not participate in the study concept and design, data collection and analysis, interpretation of results, the drafting of the manuscript, or the decision to submit the manuscript for publication.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Horwitz LI, Bernheim SM, Ross JS, et al. Hospital characteristics associated with risk-standardized readmission rates. Med Care. 2017;55(5):528–11. doi:10.1097/MLR.0000000000000713
2. Australian Consortium for Aged CARE. Hospital-wide all-cause unplanned readmission measure (HWR). 2013. Available from: https://agedcareconsortium.com.au/quality-indicators/indrr029.
3. van Walraven C, Bennett C, Jennings A, Austin PC, Forster AJ. Proportion of hospital readmissions deemed avoidable: a systematic review. CMAJ. 2011;183(7):E391–402. doi:10.1503/cmaj.101860
4. Hamar GB, Coberley C, Pope JE, et al. Effect of post-hospital discharge telephonic intervention on hospital readmissions in a privately insured population in Australia. Aust Health Rev. 2018;42(3):241–247. doi:10.1071/AH16059
5. Rohr R. Rehospitalizations among patients in the medicare fee-for-service program. New Engl J Med. 2009;361(3):311–312. author reply 312.
6. McIlvennan CK, Eapen ZJ, Allen LA. Hospital readmissions reduction program. Circulation. 2015;131(20):1796–1803. doi:10.1161/CIRCULATIONAHA.114.010270
7. Desai NR, Ross JS, Kwon JY, et al. Association between hospital penalty status under the hospital readmission reduction program and readmission rates for target and nontarget conditions. JAMA. 2016;316(24):2647–2656. doi:10.1001/jama.2016.18533
8. Busse R, Geissler A, Aaviksoo A, et al. Diagnosis related groups in Europe: moving towards transparency, efficiency, and quality in hospitals? BMJ. 2013;346(jun07 3):f3197. doi:10.1136/bmj.f3197
9. Rippe W, Dittberner A, Boeger D, et al. 30-day unplanned readmission rate in otolaryngology patients: a population-based study in Thuringia, Germany. PLoS One. 2019;14(10):e0224146. doi:10.1371/journal.pone.0224146
10. Evans K, Makar T, Miles LF. Associations between postoperative anaemia and specific drivers of unplanned readmission. Anaesthesia. 2025;80(8):1000–1001. doi:10.1111/anae.16677
11. Zeng Y, Wan Y, Yuan Z, Fang Y. Healthcare-seeking behavior among chinese older adults: patterns and predictive factors. Int J Environ Res Public Health. 2021;18(6):2969. doi:10.3390/ijerph18062969
12. Li CY, Karmarkar A, Adhikari D, Ottenbacher K, Kuo YF. Effects of age and sex on hospital readmission in traumatic brain injury. Arch Phys Med Rehabil. 2018;99(7):1279–1288e1271. doi:10.1016/j.apmr.2017.12.006
13. Rothenberg KA, Stern JR, George EL, et al. Association of frailty and postoperative complications with unplanned readmissions after elective outpatient surgery. JAMA Network Open. 2019;2(5):e194330. doi:10.1001/jamanetworkopen.2019.4330
14. Pu X, He S, Lin X. The effect of urban-rural resident basic medical insurance on physical health of the rural older adult in China. Front Public Health. 2024;12:1319697. doi:10.3389/fpubh.2024.1319697
15. Jung DH, DuGoff E, Smith M, Palta M, Gilmore-Bykovskyi A, Mullahy J. Likelihood of hospital readmission in medicare advantage and fee-for-service within same hospital. Health Serv Res. 2020;55(4):587–595. doi:10.1111/1475-6773.13315
16. Cooper J, Asti L, Metzger G, Xiang H, Deans K, Chisolm D. Effects of the affordable care act medicaid expansion on in‐hospital mortality, access to rehabilitation, and readmission rates among young adult trauma patients. Health Serv Res. 2021;56(S2):21–22. doi:10.1111/1475-6773.13747
17. Tonse R, Townsend A, Rubens M, et al. Factors associated with unplanned readmissions and costs following resection of brain metastases in the United States. Sci Rep. 2021;11(1):22152. doi:10.1038/s41598-021-01641-4
18. Tong L, Erdmann C, Daldalian M, Li J, Esposito T. Comparison of predictive modeling approaches for 30-day all-cause non-elective readmission risk. BMC Med Res Methodol. 2016;16(1):26. doi:10.1186/s12874-016-0128-0
19. Handa S, Gupta K, Sidhu JS, Petrone G, Rajeeve S, Jatwani K. Etiologies and predictors of 30-day readmission in patients undergoing induction chemotherapy for acute myeloid leukemia. Blood. 2019;134(Supplement_1):4759. doi:10.1182/blood-2019-132180
20. Maali Y, Perez-Concha O, Coiera E, Roffe D, Day RO, Gallego B. Predicting 7-day, 30-day and 60-day all-cause unplanned readmission: a case study of a Sydney hospital. BMC Med Inform Decis Mak. 2018;18(1):1. doi:10.1186/s12911-017-0580-8
21. Kim Y, Gani F, Canner JK, et al. Hospital readmission after multiple major operative procedures among patients with employer provided health insurance. Surgery. 2016;160(1):178–190. doi:10.1016/j.surg.2016.01.025
22. Makar T, Hezkial M, Vasudeva M, et al. Associations between postoperative anaemia and unplanned readmission to hospital after major surgery: a retrospective cohort study. Anaesthesia. 2024;79(8):839–848. doi:10.1111/anae.16291
23. Vaqueriza Cubillo D, Dominguez Munoa M, Beltran Herrera C, et al. A multidisciplinary program based on early care in a day hospital after heart failure hospitalizations. Reduction of 30-day readmissions in patients discharged from cardiology departments. Eur Heart J. 2022;43(Supplement_2):ehac544–1033.
24. Rich AO. Nurse-led inpatient heart failure program in a community hospital improves initiation of heart failure guideline directed medication therapy and reduces readmission rates. Heart Lung. 2023;61:170. doi:10.1016/j.hrtlng.2023.06.019
25. Weinstein JM, Kiselnik DS, Sidi A, Hemo Z, Guterman E, Refaelovich E. The “Triage” clinic: close communication between hospital and community heart failure unit reduces readmissions. Eur Heart J. 2023;44(Supplement_2). doi:10.1093/eurheartj/ehad655.1053
26. John G, Payrard L, Donze J. Associations between post-discharge medical consultations and 30-day unplanned hospital readmission: a prospective observational cohort study. Eur J Intern Med. 2022;99:57–62. doi:10.1016/j.ejim.2022.01.013
27. Becker C, Zumbrunn S, Beck K, et al. Interventions to improve communication at hospital discharge and rates of readmission: a systematic review and meta-analysis. JAMA Network Open. 2021;4(8):e2119346. doi:10.1001/jamanetworkopen.2021.19346
28. Schultz BE, Corbett CF, Hughes RG, Bell N. Scoping review: social support impacts hospital readmission rates. J Clin Nurs. 2022;31(19–20):2691–2705. doi:10.1111/jocn.16143
29. Yen HY, Chi MJ, Huang HY. Effects of discharge planning services and unplanned readmissions on post-hospital mortality in older patients: a time-varying survival analysis. Int J Nurs Stud. 2022;128:104175. doi:10.1016/j.ijnurstu.2022.104175
30. Marsall M, Hornung T, Bauerle A, Weigl M. Quality of care transition, patient safety incidents, and patients’ health status: a structural equation model on the complexity of the discharge process. BMC Health Serv Res. 2024;24(1):576. doi:10.1186/s12913-024-11047-3
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.