Back to Journals » Clinical Ophthalmology » Volume 20
A Five-Step Approach to Acute Vision Loss: A Practical Narrative Review for Clinicians
Authors Maher C ![]() , Guo B, Yek J
, Guo B, Yek J
Received 21 December 2025
Accepted for publication 19 February 2026
Published 26 February 2026 Volume 2026:20 590753
DOI https://doi.org/10.2147/OPTH.S590753
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Dr Scott Fraser
Clare Maher,1 Brad Guo,2,* John Yek3,*
1Ophthalmology Department, John Hunter Hospital, Newcastle, NSW, 2305, Australia; 2Department of Medicine, The University of Adelaide, Adelaide, SA, 5005, Australia; 3Ophthalmology Department, Westmead Hospital, Westmead, NSW, 2145, Australia
*These authors contributed equally to this work
Correspondence: Clare Maher, Ophthalmology Department, John Hunter Hospital, Newcastle, Lookout Road, New Lambton Heights, Westmead, NSW, 2305, Australia, Tel +61448866450, Email [email protected]
Background: Acute vision loss is a time-critical presentation that requires rapid evaluation to differentiate benign conditions from ophthalmic and neurologic emergencies. Early recognition and appropriate triage are essential to prevent irreversible visual impairment. In many cases, the initial evaluation is performed by non-ophthalmic clinicians, where diagnostic uncertainty can delay appropriate referral and management.
Purpose: To present a practical, stepwise framework for the assessment of acute vision loss that supports rapid clinical localization, early identification of red-flag features, and timely escalation of care.
Methods: A targeted review of recent literature was performed using PubMed and MEDLINE, focusing on major causes of acute vision loss, established clinical algorithms, and evidence-based emergency management strategies. Relevant guidelines and high-impact review articles published between 2015 and 2025 were included.
Findings: A structured five-step approach—(1) determination of laterality, (2) assessment for pain, (3) targeted history-taking, (4) focused chairside examination with identification of red flags, and (5) action through timely escalation, investigation, and referral, enables clinicians to rapidly triage pathology, prioritise urgency and identify vision-threatening conditions. Presentations such as central retinal artery occlusion, acute angle-closure glaucoma, retinal detachment, optic neuritis, and giant cell arteritis require immediate recognition and specialist involvement. Fundamental chairside assessment remains central to early decision-making and safe triage.
Conclusion: A five-step diagnostic framework provides a clear, clinically intuitive approach to acute vision loss that is applicable across emergency, primary care, and general ophthalmic settings. By prioritising early localization and risk stratification, this approach may reduce diagnostic delays and support safer triage of vision-threatening disease.
Plain Language Summary: Sudden loss of vision is a medical emergency. Some causes are harmless and temporary, but others can lead to permanent vision loss or serious illness if not recognised and treated quickly. Many people with sudden vision problems first seek help from doctors or healthcare workers who are not eye specialists, which can make early decision-making difficult.
This review was written to help clinicians assess sudden vision loss in a clear, practical way. The authors reviewed current medical literature and developed a simple five-step approach that mirrors how clinicians think in real-world settings. The steps focus on whether vision loss affects one or both eyes, whether there is pain, key questions to ask in the medical history, important examination findings, and when to urgently refer for specialist care.
The review highlights warning signs that suggest serious conditions such as blocked blood vessels in the eye, inflammation of the optic nerve, retinal detachment, acute glaucoma, and giant cell arteritis, an inflammatory condition that can cause permanent blindness if missed. The framework emphasises the value of careful chairside assessment and early recognition of high-risk features rather than relying on tests alone.
This five-step approach is designed to support faster, safer decision-making in emergency departments, general practice, and hospital settings. By helping clinicians identify vision-threatening conditions earlier, this framework has the potential to reduce delays in care and improve outcomes for people presenting with sudden vision loss.
Keywords: acute vision loss, emergency ophthalmology, triage
Introduction
Acute vision loss is a high-risk clinical presentation that requires rapid and accurate assessment to prevent irreversible visual impairment.1 It represents a relatively common reason for emergency department presentation, accounting for up to approximately 2% of emergency visits.2 The underlying causes vary widely in urgency, ranging from benign conditions such as migraine aura to ophthalmic emergencies including central retinal artery occlusion (CRAO), acute angle-closure glaucoma (AACG), and retinal detachment.3 Failure to recognise these time-critical conditions may result in permanent visual morbidity.1,4 Given that many patients with sudden vision loss present first to emergency departments or primary care providers, clinicians across a wide range of specialties require a clear, structured approach to differentiate urgent from non-urgent causes.1,3–5
In contemporary clinical practice, patients with sudden vision loss frequently present first to emergency departments, primary care, or general medical services, where the initial assessment is often performed by clinicians without formal ophthalmic training. In this setting, diagnostic uncertainty is common and can lead to delayed referral or unnecessary investigations. Although existing literature provides detailed discussions of individual diagnoses and subspecialty pathways, there remains a need for a unified, practical framework that supports rapid chairside decision-making across diverse clinical environments.
This narrative review presents a five-step clinical assessment and triage framework for acute vision loss. The framework is designed to mirror real-world clinical reasoning, emphasising early localization and risk stratification before investigation. By synthesising contemporary evidence into a structured, clinician-friendly algorithm, this review aims to support timely diagnosis, reduce preventable delays, and improve outcomes in both ophthalmic and non-ophthalmic practice.
Framework for Evaluation
A structured, stepwise approach assists clinicians in rapidly triaging acute vision loss and identifying vision-threatening disease. Each step progressively narrows the differential diagnosis and informs the urgency of investigation and referral. This framework (Figure 1) is intended to support initial localization and triage rather than provide a definitive diagnosis. Paediatric causes and chronic/progressive vision loss are outside the scope of this review.
 |
Figure 1 Five-step clinical assessment and triage framework for acute vision loss. Note ± indicates plus or minus, IOP (intra-ocular pressure), RAPD (relative afferent pupillary defect). Bold formatting is used to highlight important headings. |
Step 1: Determine Laterality: Monocular vs Binocular Vision Loss
The first discriminator in the assessment of acute vision loss is laterality. Establishing whether symptoms are monocular or binocular immediately localises pathology and narrows the differential diagnosis, as depicted in Table 1. Monocular vision loss typically reflects disease anterior to the optic chiasm, involving the ocular media, retina, or optic nerve.5 In contrast, binocular visual disturbance suggests retro chiasmal pathology or a systemic neurologic process.6
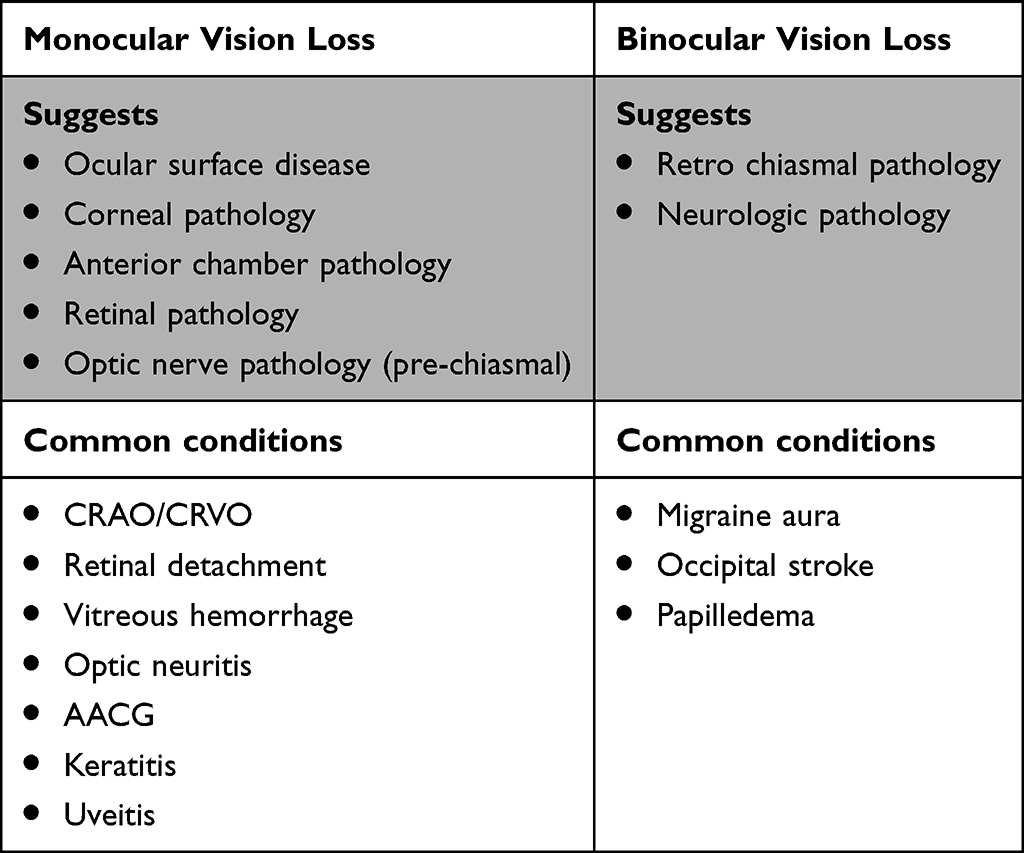 |
Table 1 Diagnostic Implications of Monocular versus Binocular Acute Vision Loss. Bold Formatting is Used to Highlight Important Headings |
It is important to note that patients may misinterpret binocular visual blur as monocular loss. Each eye should therefore be tested individually to confirm true laterality. Accurate determination at this early stage facilitates appropriate triage.
Binocular vision loss, particularly homonymous visual field loss, should be considered retro chiasmal and treated as cerebrovascular disease until proven otherwise. In this context, normal pupillary responses and a normal anterior segment examination increase suspicion for neurologic pathology, particularly occipital lobe infarction.5,6 Acute homonymous field defects with associated neurologic symptoms should prompt immediate stroke evaluation.1 In contrast, transient binocular visual disturbance with positive visual phenomena, such as scintillations or zig-zag lines, is more characteristic of migraine aura, particularly in younger patients with a normal examination.7
Step 2: Assess for Pain: Painful vs Painless Vision Loss
The presence or absence of ocular pain provides a critical second layer of diagnostic discrimination, particularly in cases of monocular vision loss (Table 2). Severe ocular pain accompanied by nausea, vomiting, or halos strongly suggests acute angle-closure glaucoma.8 Pain exacerbated by eye movement is characteristic of optic neuritis,9 while surface irritation with photophobia raises concern for keratitis or anterior uveitis.10 In contrast, sudden painless visual loss should prompt urgent consideration of retinal vascular occlusion, retinal detachment, vitreous hemorrhage, or ischemic optic neuropathy, all of which are potentially vision-threatening.5,6
 |
Table 2 Diagnostic Implications of Painful versus Painless Acute Vision Loss. Bold Formatting is Used to Highlight Important Headings |
Step 3: Obtain a Targeted History
A concise but focused history provides essential diagnostic context and should be obtained early. The onset of vision loss is particularly informative. Vision loss that reaches maximal severity within seconds is suggestive of vascular occlusion or trauma, whereas progression over hours to days is more typical of inflammatory or infectious conditions.
Associated ocular symptoms further refine the differential diagnosis, as shown in Table 3. Flashes, floaters, or a descending curtain strongly indicate retinal detachment.11 Halos around lights are characteristic of acute angle-closure glaucoma, while transient visual dimming may reflect amaurosis fugax.8,12 Pain with eye movement is highly suggestive of optic neuritis.9 Systemic symptoms such as headache, jaw claudication, or constitutional features should raise suspicion for giant cell arteritis, particularly in patients over 50 years of age.13
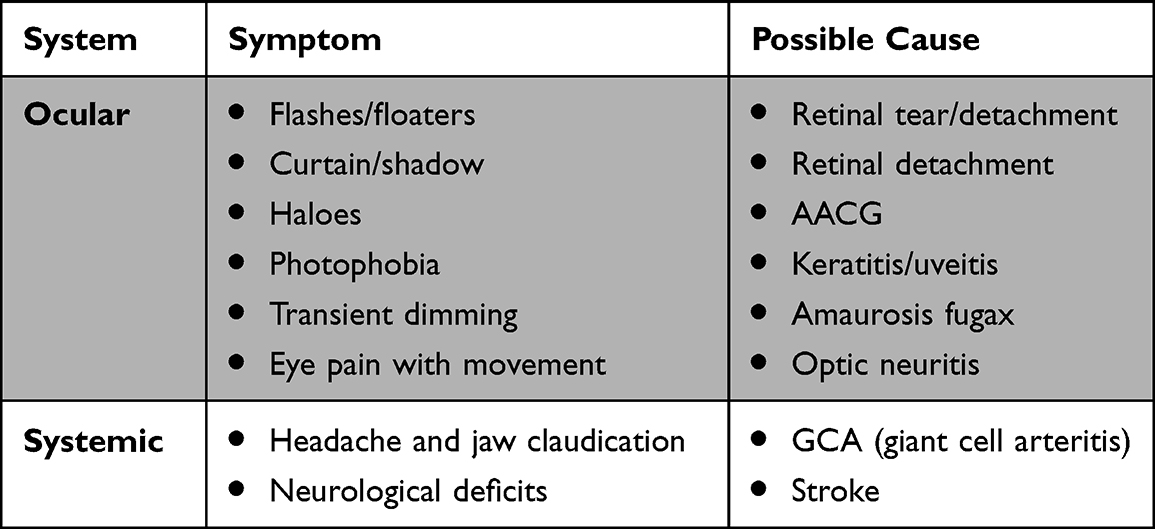 |
Table 3 Key Ocular and Systemic Symptoms in Acute Vision Loss and Their Diagnostic Implications. Bold Formatting is Used to Highlight Important Headings |
A history of recent ocular surgery or intraocular procedures is critical in patients presenting with acute vision loss. Post-operative endophthalmitis most commonly presents within 3–5 days following cataract surgery or intravitreal injection and should be suspected in any patient with acute visual decline, ocular pain, redness, or hypopyon in this timeframe. Endophthalmitis represents an ophthalmic emergency requiring immediate specialist referral.14
A focused medical history provides essential diagnostic clues in the evaluation of acute vision loss. Systemic comorbidities are strongly associated with specific ophthalmic pathologies, and recognising these relationships can help clinicians rapidly narrow the differential diagnosis.
Diabetes mellitus is a major risk factor for several causes of acute visual deterioration, including diabetic macular oedema (DME), vitreous hemorrhage secondary to proliferative diabetic retinopathy, tractional retinal detachment and central retinal vein occlusion (CRVO). Diabetic eye disease remains one of the most common systemic contributors to acute and subacute vision loss, and its prevalence increases with duration of disease and poor glycaemic control.15
Vascular risk factors such as hypertension, hyperlipidaemia, carotid disease, and smoking are closely linked with retinal arterial and venous occlusions. Central retinal artery occlusion (CRAO) is now considered a stroke equivalent, and up to two-thirds of patients have underlying cardiovascular or cerebrovascular disease.6 Non-arteritic ischaemic optic neuropathy (NAION) also shares systemic associations, particularly nocturnal hypotension, diabetes, and obstructive sleep apnoea.16
Autoimmune and inflammatory disorders substantially increase the likelihood of uveitis, scleritis, and optic neuropathies. Conditions such as rheumatoid arthritis, granulomatosis with polyangiitis, sarcoidosis, and HLA-B27–associated diseases often present initially with ocular inflammation, sometimes before systemic symptoms declare themselves.10 These disorders can produce acute painful vision loss and require urgent ophthalmic assessment and systemic workup.
Pharmacological or systemic immunosuppression, including corticosteroids, chemotherapy, biologic agents, human immunodeficiency virus (HIV) infection, or recent systemic sepsis, substantially increases the risk of severe ocular infection and atypical presentations.10,17,18 In immunocompromised patients, ocular infections may progress rapidly and present with muted inflammatory signs, necessitating a lower threshold for urgent ophthalmology involvement.17,19
Step 4: Perform a Focused Eye Examination and Identify Red Flags
Step 4a: Focused Chairside Examination
A structured chairside eye examination is central to the assessment of acute vision loss and can be performed in most clinical settings with minimal equipment (Table 4).
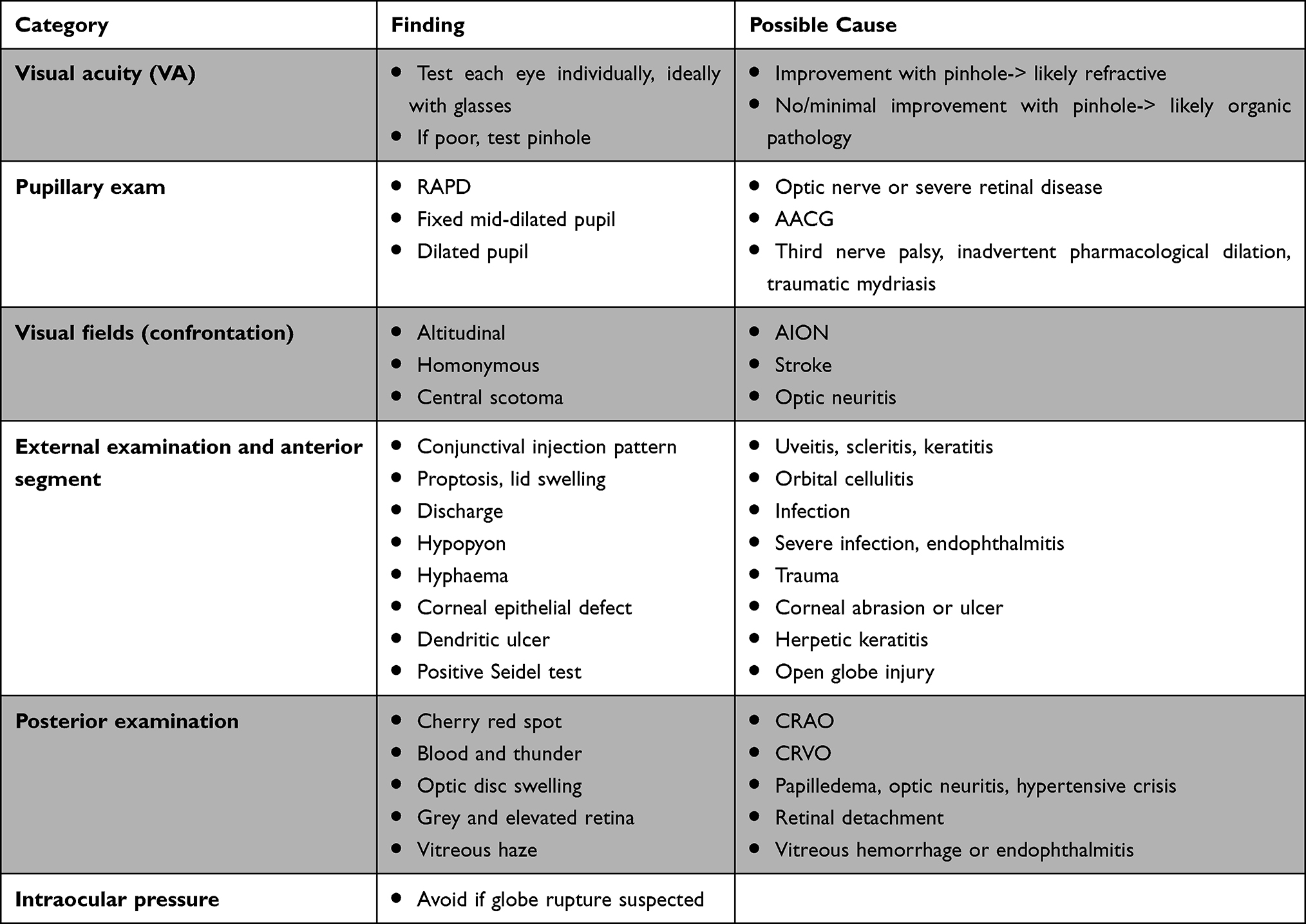 |
Table 4 Focused Chairside Eye Examination Findings in Acute Vision Loss and Their Diagnostic Implications. Bold Formatting is Used to Highlight Important Headings |
General inspection may reveal periocular or facial findings that localise pathology, including a vesicular rash in the ophthalmic division of the trigeminal nerve with Hutchinson sign suggestive of herpes zoster ophthalmicus,20 or eyelid oedema, erythema, and proptosis concerning for orbital cellulitis.21
Visual acuity should be measured in each eye individually and documented accurately. Poor visual acuity that improves with pinhole testing suggests refractive or media-related causes, whereas lack of improvement indicates organic pathology.1
Pupillary examination is essential, with particular attention to the presence of a relative afferent pupillary defect, which indicates optic nerve or severe retinal disease.22 Confrontation visual field testing may reveal altitudinal defects suggestive of ischaemic optic neuropathy or homonymous deficits indicating retro chiasmal pathology.23
Patients may describe “vision loss” despite normal or near-normal central visual acuity, reflecting visual field loss rather than macular involvement. This presentation should raise suspicion for pathology affecting the visual pathways rather than the eye itself. Important causes include compressive lesions of the optic chiasm (including pituitary adenoma or pituitary apoplexy), retro chiasmal vascular events involving the visual pathways,24 and raised intracranial pressure resulting in an enlarged blind spot, as seen in idiopathic intracranial hypertension or hypertensive crisis.25 Macula-on retinal detachment may present early with peripheral field loss before central acuity is affected, while non-arteritic anterior ischaemic optic neuropathy commonly produces altitudinal visual field defects with relatively preserved central vision.26 Normal visual acuity does not exclude vision- or life-threatening disease.6
Anterior segment inspection can identify corneal opacity, hypopyon, keratic precipitates, or a shallow anterior chamber. Fluorescein staining of the ocular surface is an essential component of the focused chairside examination. It facilitates identification of corneal epithelial defects, including dendritic ulcers characteristic of herpetic keratitis, punctate epithelial erosions suggestive of severe ocular surface disease, and focal staining associated with corneal ulceration.27 A positive Seidel test, indicated by aqueous leakage diluting fluorescein dye, confirms an open-globe injury and mandates immediate eye protection and urgent ophthalmology referral.28
Fundus examination may reveal retinal detachment, retinal vascular occlusion, optic disc swelling, or vitreous hemorrhage.
Step 4b: Red Flag Features Requiring Urgent Escalation
Red-flag findings must be actively sought, as their presence mandates urgent specialist involvement. These include sudden profound painless vision loss, severe ocular pain, a relative afferent pupillary defect, neurologic deficits, jaw claudication, corneal ulceration in contact lens wearers, suspected globe rupture, hypopyon, and proptosis with systemic features of infection.6,21 Any visual symptoms in a patient over 50 years of age accompanied by headache, jaw claudication, scalp tenderness, or raised inflammatory markers should prompt strong clinical suspicion for giant cell arteritis, even in the presence of normal erythrocyte sedimentation rate and C-reactive protein.13,29 Identification of any red-flag feature should prompt immediate escalation of care.
Step 5: ACT — Initiate Targeted Investigations, Escalate, and Refer
This final step emphasizes that, in acute vision loss, timely escalation and referral are often more critical than definitive diagnosis at first presentation. Once laterality, pain, targeted history, and focused examination findings have been integrated, clinicians should act decisively to initiate appropriate investigations, escalate care, and arrange timely referral. Investigations should support clinical localization and risk stratification and should not delay urgent specialist involvement when red-flag features are present.
Targeted Investigations
Diagnostic testing should be purposeful and guided by the suspected pathology, as summarised in Table 5. Ocular imaging modalities such as optical coherence tomography and fundus photography are valuable for confirming retinal and optic nerve disease when available. B-scan ultrasonography is particularly useful when the fundus view is obscured, allowing assessment for retinal detachment, vitreous pathology or T-sign in posterior scleritis.30 Intraocular pressure measurement may assist in identifying acute angle-closure glaucoma, provided globe rupture has been excluded.
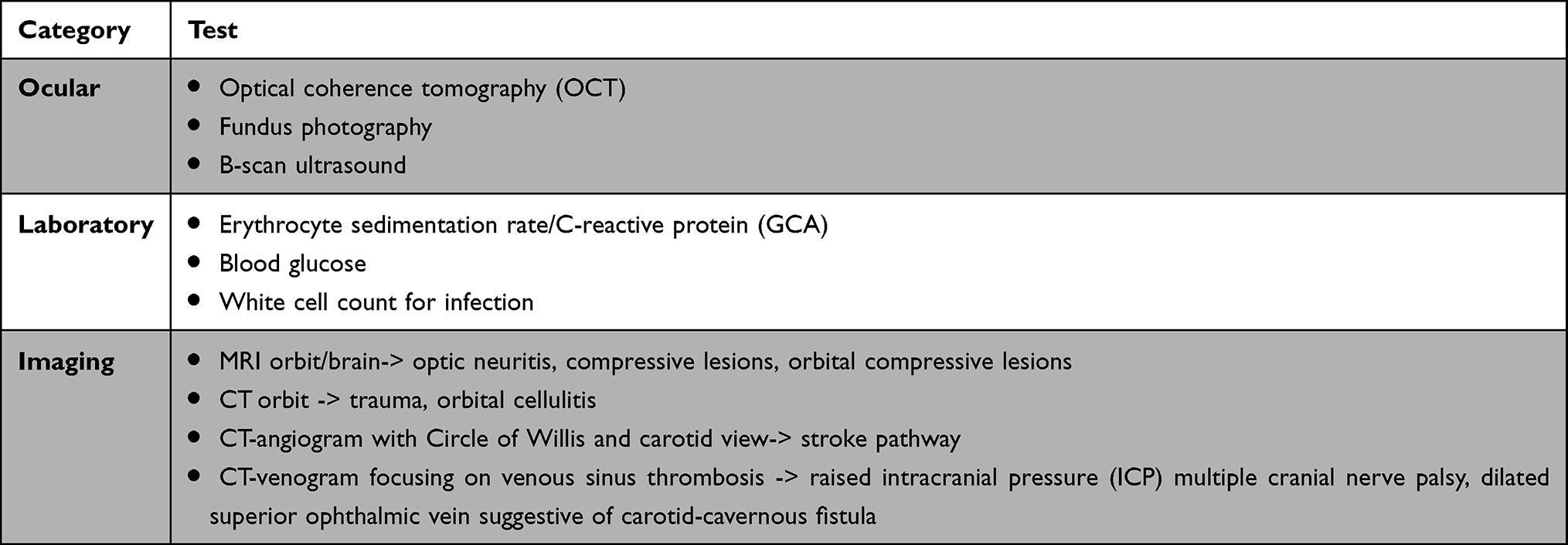 |
Table 5 Targeted Investigations in the Evaluation of Acute Vision Loss. Bold Formatting is Used to Highlight Important Headings |
Laboratory investigations should be obtained selectively. Erythrocyte sedimentation rate and C-reactive protein are essential in patients over 50 years of age with symptoms suggestive of giant cell arteritis and should not delay initiation of corticosteroid therapy when clinical suspicion is high.13,29 Contemporary non-invasive diagnostic pathways for suspected giant cell arteritis increasingly incorporate temporal artery Doppler ultrasonography and positron emission tomography (PET) to support diagnosis and disease assessment.29 Inflammatory markers may also support the presence of underlying systemic autoimmune or inflammatory disease, such as rheumatoid arthritis, systemic lupus erythematosus, or granulomatosis with polyangiitis, which are associated with ocular manifestations including uveitis, scleritis, and optic neuropathy.29,31 Additional blood tests, including blood glucose levels and full blood count, may be considered in selected cases to aid risk stratification but are not routinely required.
Neuroimaging is indicated when optic neuritis, compressive optic neuropathy, or retro chiasmal pathology or stroke is suspected. Magnetic resonance imaging of the brain and orbits is preferred in these scenarios with gadolinium to identify demyelination,32 while computed tomography of the orbits is appropriate for trauma, suspected orbital cellulitis, or acute proptosis. Suspected central retinal artery or cerebral ischemia should prompt immediate activation of local stroke pathways.33
Investigations
Referral and Initial Management
Several causes of acute vision loss require immediate ophthalmology involvement, listed in Table 6, early specialist input is critical to preserving vision and, in some cases, life.
 |
Table 6 Time-Critical Causes of Acute Vision Loss Requiring Immediate Escalation. Bold Formatting is Used to Highlight Important Headings |
Initial management priorities include prompt treatment of reversible emergencies where indicated, protection of the eye in cases of trauma, avoidance of topical corticosteroids or mydriatic agents unless advised by ophthalmology, and provision of adequate analgesia and antiemetics as required.
Clinical pearls:
- Do not patch painful red eye with vision loss.
- Do not dilate until AACG excluded.
- Do shield suspected globe rupture.
- Do start steroids immediately if high suspicion GCA (after bloods, do not delay).
Discussion
Acute vision loss represents a diagnostic challenge across a wide range of clinical settings, owing to its broad differential diagnosis and the potential for irreversible visual morbidity if time-critical conditions are not promptly recognised. Rather than proposing a novel diagnostic algorithm, this review synthesises established principles from emergency medicine, ophthalmology, and neuro-ophthalmology into a single, structured triage framework designed for rapid chairside use by non-ophthalmic clinicians. By emphasising high-yield clinical discriminators rather than exhaustive diagnostic lists, the proposed approach aligns with real-world practice and is applicable to both ophthalmic and non-ophthalmic environments.
A central strength of this framework is its prioritisation of chairside clinical assessment. Determination of laterality, assessment of pain, careful evaluation of symptom onset, and focused examination findings collectively provide substantial diagnostic information and often obviate the need for indiscriminate testing. While advances in ocular imaging and neuroimaging have transformed diagnostic capabilities, this review reinforces that timely recognition of vision-threatening conditions continues to depend on foundational clinical skills that are accessible in most care settings.
The framework also highlights the importance of early risk stratification through identification of red-flag features. Profound sudden vision loss, severe ocular pain, the presence of a relative afferent pupillary defect, neurologic deficits, and symptoms suggestive of giant cell arteritis reliably indicate conditions requiring urgent specialist involvement. Failure to recognise these features remains a significant contributor to delayed referral and preventable vision loss, particularly in emergency departments and regional or resource-limited settings. By integrating red flags directly into the diagnostic pathway, this approach supports safer triage and more efficient escalation of care. Transient vision loss should be approached with similar urgency to persistent loss, particularly when vascular causes are suspected.
This framework is intended to complement, not replace, specialist assessment and condition-specific management guidelines. Instead, it provides a structured framework for initial evaluation, ensuring that high-risk presentations are recognised early and that investigations are targeted rather than reflexive. Variability in access to ophthalmic expertise and diagnostic resources may limit the immediate applicability of certain investigations, underscoring the need for clinical judgment and local adaptation of the pathway.
This review is narrative in nature and does not represent a systematic appraisal of all available evidence. The proposed framework is intended to support initial localization, risk stratification, and triage rather than provide definitive diagnosis or replace specialist assessment. Access to ophthalmic examination tools and imaging modalities may vary across clinical settings, which may limit immediate application of certain components of the pathway. Paediatric presentations and chronic or progressive vision loss are outside the scope of this review. Future studies evaluating the impact of this framework on diagnostic accuracy, referral patterns, and patient outcomes would be valuable.
Conclusion
Acute vision loss requires rapid, structured assessment to distinguish benign presentations from time-critical, vision-threatening disease. The five-step framework presented in this review provides a practical, clinically intuitive approach that supports early localization, identification of red-flag features, and timely escalation of care across a range of clinical settings. By reinforcing the value of focused chairside assessment and risk stratification, this approach has the potential to reduce diagnostic delays and improve outcomes for patients presenting with acute visual symptoms.
Abbreviations
AACG, acute angle-closure glaucoma; AION, arteritic anterior ischaemic optic neuropathy; CRAO, central retinal artery occlusion; CRVO, central retinal vein occlusion; CT, computed tomography; CTA, computed tomography angiography; DME, diabetic macular oedema; GCA, giant cell arteritis; HIV, human immunodeficiency virus; HLA, human leukocyte antigen; ICP, intra-cranial pressure; IOP, intra-ocular pressure; IV, intra-venous; NAION, non-arteritic anterior ischaemic optic neuropathy; OCT, optical coherence tomography; PET, positive emission tomography; RAPD, relative afferent pupillary defect.
Data Sharing Statement
This study did not generate or analyze original datasets. All information used in this review was obtained from previously published sources.
Ethics and Informed Consent
Ethics approval and informed consent: Not applicable (narrative review of published literature).
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
No external funding was received for the preparation of this manuscript.
Disclosure
The authors declare no competing interests or financial relationships relevant to this manuscript.
References
1. Edlow JA, Hoffmann B. Managing patients with acute visual loss. Ann Emerg Med. 2022;79(5):474–11. doi:10.1016/j.annemergmed.2021.10.019
2. Lindsay H. Point-of-care emergency clinical summary. 2018. Available from: https://emergencycarebc.ca/clinical_resource/clinical-summary/acute-vision-loss/.
3. Raharja A, Whitefield L. Clinical approach to vision loss: a review for general physicians. Clin Med. 2022;22(2):95–99. doi:10.7861/clinmed.2022-0057
4. Statham MO, Sharma A, Pane AR. Misdiagnosis of acute eye diseases by primary health care providers: incidence and implications. Med J Aust. 2008;189(7):402–404. doi:10.5694/j.1326-5377.2008.tb02091.x
5. Prasad S, Galetta SL. Approach to the patient with acute monocular visual loss. Neurol Clin Pract. 2012;2(1):14–23. doi:10.1212/CPJ.0b013e31824cb084
6. Newman N, Biousse V. Diagnostic approach to vision loss. Continuum. 2014;20(4 Neuro–ophthalmology):785–815. doi:10.1212/01.CON.0000453317.67637.46
7. Viana M, Linde M, Sances G, et al. Migraine aura symptoms: duration, succession and temporal relationship to headache. Cephalalgia. 2016;36(5):413–421. doi:10.1177/0333102415593089
8. Flores-Sánchez BC, Tatham AJ. Acute angle closure glaucoma. Br J Hosp Med. 2019;80(12):C174–c179. doi:10.12968/hmed.2019.80.12.C174
9. Corbett JJ, Thompson HS, Musser C, et al. The clinical profile of optic neuritis. Experience of the optic neuritis treatment trial. optic neuritis study group. Arch Ophthalmol. 1991;109(12):1673–1678. doi:10.1001/archopht.1991.01080120057025
10. Jabs DA. Immunosuppression for the Uveitides. Ophthalmology. 2018;125(2):193–202. doi:10.1016/j.ophtha.2017.08.007
11. Hollands H, Johnson D, Brox AC, Almeida D, Simel DL, Sharma S. Acute-onset floaters and flashes: is this patient at risk for retinal detachment? JAMA. 2009;302(20):2243–2249. doi:10.1001/jama.2009.1714
12. The amaurosis fugax study group. Current management of amaurosis fugax. Stroke. 1990;21(2):201–208. doi:10.1161/01.STR.21.2.201
13. Hayreh SS, Podhajsky PA, Raman R, Zimmerman B. Giant cell arteritis: validity and reliability of various diagnostic criteria. Am J Ophthalmol. 1997;123(3):285–296. doi:10.1016/S0002-9394(14)70123-0
14. Durand ML. Endophthalmitis. Clin Microbiol Infect. 2013;19(3):227–234. doi:10.1111/1469-0691.12118
15. Wong TY, Scott IU. Clinical practice. Retinal-vein occlusion. N Engl J Med. 2010;363(22):2135–2144. doi:10.1056/NEJMcp1003934
16. Arnold AC. Pathogenesis of nonarteritic anterior ischemic optic neuropathy. J Neuroophthalmol. 2003;23(2):157–163. doi:10.1097/00041327-200306000-00012
17. Kresloff MS, Castellarin AA, Zarbin MA. Endophthalmitis. Surv Ophthalmol. 1998;43(3):193–224. doi:10.1016/s0039-6257(98)00036-8
18. Jabs DA. Ocular manifestations of HIV infection. Trans Am Ophthalmol Soc. 1995;93:623–683.
19. Durand ML. Bacterial and fungal endophthalmitis. Clin Microbiol Rev. 2017;30(3):597–613. doi:10.1128/CMR.00113-16
20. Shaikh S, Ta CN. Evaluation and management of herpes zoster ophthalmicus. Am Fam Physician. 2002;66(9):1723–1730.
21. Chaudhry IA, Shamsi FA, Elzaridi E, et al. Outcome of treated orbital cellulitis in a tertiary eye care center in the Middle East. Ophthalmology. 2007;114(2):345–354. doi:10.1016/j.ophtha.2006.07.059
22. Thompson HS. Pupillary signs in retinal and optic nerve disease. In: Heijl A, Greve EL, editors. Sixth International Visual Field Symposium: Santa Margherita Ligure, May 27–31, 1984. Dordrecht: Springer Netherlands; 1985:223–225.
23. Liu GT, Volpe NJ, Galetta S. Neuro-ophthalmology: Diagnosis and Management.
24. Zhang X, Kedar S, Lynn MJ, Newman NJ, Biousse V. Homonymous hemianopias: clinical-anatomic correlations in 904 cases. Neurology. 2006;66(6):906–910. doi:10.1212/01.wnl.0000203913.12088.93
25. Wall M. Idiopathic intracranial hypertension. Neurol Clin. 2010;28(3):593–617. doi:10.1016/j.ncl.2010.03.003
26. Hayreh SS. Ischemic optic neuropathy. Prog Retin Eye Res. 2009;28(1):34–62. doi:10.1016/j.preteyeres.2008.11.002
27. Wilson SA, Last A. Management of corneal abrasions. Am Fam Physician. 2004;70(1):123–128.
28. Kuhn F, Morris R, Witherspoon CD, Heimann K, Jeffers JB, Treister G. A standardized classification of ocular trauma. Ophthalmology. 1996;103(2):240–243. doi:10.1016/S0161-6420(96)30710-0
29. Hellmich B, Agueda A, Monti S, et al. 2018 update of the EULAR recommendations for the management of large vessel vasculitis. Ann Rheum Dis. 2020;79(1):19–30. doi:10.1136/annrheumdis-2019-215672
30. Johnson TE. Ultrasound of the eye and orbit, 2nd ed. Ophthalmic Plastic Reconstructive Surg. 2003;19(2):171. doi:10.1097/00002341-200303000-00024
31. Patel SJ, Lundy DC. Ocular manifestations of autoimmune disease. Am Fam Physician. 2002;66(6):991–998.
32. Balcer LJ. Clinical practice. Optic neuritis. N Engl J Med. 2006;354(12):1273–1280. doi:10.1056/NEJMcp053247
33. Mac Grory B, Schrag M, Biousse V, et al. Management of central retinal artery occlusion: a scientific statement from the American Heart Association. Stroke. 2021;52(6):e282–e294. doi:10.1161/STR.0000000000000366
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.