Back to Journals » Patient Preference and Adherence » Volume 13
A discrete choice experiment on preferences of patients with low back pain about non-surgical treatments: identification, refinement and selection of attributes and levels
Authors Poder TG ![]() , Beffarat M, Benkhalti M, Ladouceur G, Dagenais P
, Beffarat M, Benkhalti M, Ladouceur G, Dagenais P
Received 13 January 2019
Accepted for publication 13 April 2019
Published 12 June 2019 Volume 2019:13 Pages 933—940
DOI https://doi.org/10.2147/PPA.S201401
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Johnny Chen
Thomas G Poder,1,2 Marion Beffarat,3 Maria Benkhalti,1 Ginette Ladouceur,2 Pierre Dagenais1
1UETMISSS, CIUSSS de l’Estrie-CHUS, Sherbrooke, QC, Canada; 2CRCHUS, CIUSSS de l’Estrie-CHUS, Sherbrooke, QC, Canada; 3CERDI, Université d’Auvergne, Clermont-Ferrand, France
Objectives: Hospital-based health technology assessment (HB-HTA) needs to consider all relevant data to help decision making, including patients’ preferences. In this study, we comprehensively describe the process of identification, refinement and selection of attributes and levels for a discrete choice experiment (DCE).
Methods: A mixed-methods design was used to identify attributes and levels explaining low back pain (LBP) patients’ choice for a non-surgical treatment. This design combined a systematic literature review with a patients’ focus group, one-on-one interactions with experts and patients, and discussions with stakeholder committee members. Following the patient’s focus group, preference exercises were conducted. A consensus about the attributes and levels was researched during discussions with committee members.
Results: The literature review yielded 40 attributes to consider in patients’ treatment choice. During the focus group, one additional attribute emerged. The preference exercises allowed selecting eight attributes for the DCE. These eight attributes and their levels were discussed and validated by the committee members who helped reframe two levels in one of the attributes and delete one attribute. The final seven attributes were: treatment modality, pain reduction, onset of treatment efficacy, duration of efficacy, difficulty in daily living activities, sleep problem, and knowledge about their body and pain.
Conclusion: This study is one of the few to comprehensively describe the selection process of attributes and levels for a DCE. This may help ensure transparency and judge the quality of the decision-making process. In the context of a HB-HTA unit, this strengthens the legitimacy to perform a DCE to better inform decision makers in a patient-centered care approach.
Keywords: low back pain, preference, treatment, choice
Introduction
The consideration of patient preferences in health technology assessment (HTA) has increasingly gained importance in recent years.1–3 In hospital-based HTA, this is all the more relevant since there is a need to consider the whole range of available data to help decision makers select a technology or an intervention that best fits the needs of patients in their specific context.4,5 Indeed, what is important for patients is not only access to a safe and effective technology, but also to one that is accepted and preferred by them.3,6,7 Collecting data about patients’ preferences can be performed in very different ways, from qualitative studies8,9 to quantitative ones.10,11 While quantitative methods may appear to be very sophisticated and require specific skills, they allow to consider more people in surveys at a relatively lower cost per unit and to capture more heterogeneity in patients’ preferences, thus providing additional information.12 As such, quantitative methods are becoming more popular but are not routinely used in HTA.12,13 Quantitative and qualitative approaches are also complementary since there is a need to perform qualitative studies before conducting a quantitative one.14,15
Frequent examples of quantitative methods are the best-worst scaling (BWS) and discrete choice experiment (DCE). Both methods belong to choice experiment’s studies and are increasingly used to elicit patients’ preferences.16 These methods are rooted in the random utility theory17 and are based on the assumption that a treatment can be described by its characteristics or attributes, which in turn are specified by several levels (eg, effectiveness is a characteristic of a treatment and a 90% effectiveness is one of its levels). Typically, a DCE consists in a series of choice tasks where a respondent is asked to perform a choice between two or more treatments defined by the same attributes but with varying levels. Patients’ choices provide information about the relative importance of these attributes and levels through statistical modeling. In this study, we report our experience in drawing a DCE using a mixed qualitative and quantitative approach in the context of a hospital-based HTA unit project on low back pain (LBP) treatments. All steps, from identification to final selection, will be comprehensively described.
Context
Our institution represents a regional group of public hospitals, community health care and social services points of care located in the province of Quebec, Canada. It supplies health care services ranging from public and primary health care all the way to tertiary hospital care to approximately half a million people. In our institution, patients with chronic LBP have access to a range of treatment options, of which corticosteroid injections are one of the most frequently prescribed. Considering the high costs generated by this procedure and the increasingly questionable benefit provided to patients, a committee was set up to consider and revise the patient’s health care pathway when experiencing non-cancerous chronic pain. This committee subsequently asked the hospital-based HTA unit to undertake an HTA on the safety and efficacy of corticosteroid injections as well as the optimal organization of care, while considering other recommended treatment options. This led to the constitution of a HTA consultative committee with stakeholders involved in the LBP health care pathway (eg, health care professionals, patients, managers, HTA experts). The hospital-based HTA unit was in charge of animating this committee.
In doing so, the hospital-based HTA unit performed three systematic reviews. The first was on the safety and efficacy of corticosteroid injections, with or without anesthetic, for various types of chronic LBP. The second was about the other treatments currently recommended for chronic LBP by clinical practice guidelines. The third was about patients’ preferences for factors underlying the choice of non-surgical treatment. The unit also conducted a survey on the health care services currently offered in our region and collected data about patients’ preferences. The need to assess patients’ preference in our institution was influenced by the numerous non-surgical treatments offered and their relatively low efficacy.18 It was therefore important to identify which factors are most important to patients when choosing a treatment. In doing so, patients’ preferences will inform the design of the services offered in our institution. This is all the more important within the context of the patient-centered care approach adopted by our institution.19
Methods
The use of qualitative methods alongside a DCE is highly recommended by experts in the field.20–22 In this study, we used a mixed-methods design combining a systematic literature review with a patients’ focus group, one-on-one interactions with experts and patients, as well as discussions with HTA consultative committee members.
Literature review
A systematic literature search has been conducted up to June 2018 in PubMed, Sciencedirect and Scopus. The objective of the literature review was to identify which attributes and levels were already reported in the literature as being important to patients. This would serve to answer the DCE aim to identify which attributes are important to LBP patients in their decision to choose a non-surgical treatment. The methodology of this systematic review is comprehensively described elsewhere.23 In brief, two reviewers independently selected the articles according to inclusion and exclusion criteria, one reviewer then extracted the data while the other verified and completed it when necessary. Any disagreements were arbitrated by a third reviewer. The quality of each included study was evaluated by each reviewer using the Mixed Methods Appraisal Tool (MMAT).24
Patients’ focus group
One focus group with chronic LBP patients was conducted in August 2018. To be eligible, participants had to be aged 18 years or older and to be chronic LBP patients. Patients were recruited through a provincial patients’ association on chronic pain (Association québécoise de la douleur chronique). This was a convenience sample. The focus group lasted 2 hrs. Its aim was to identify which attributes and levels to consider for the DCE. For this DCE, the modality treatment is considered as an attribute and thus each level in this attribute corresponds to a non-surgical treatment (eg, corticosteroid injection, psychotherapy). The focus group was conducted in 4 steps. First, the aim of the study and the necessity for conducting the DCE were presented to the focus group participants. To do so, a synthesis factsheet was provided to them a few days before the session and was subsequently used for discussion. Second, two brainstorming conversations took place, where each patient spontaneously indicated: 1) their list of preferred non-surgical treatments, and 2) their list of preferred attributes to explain their treatment choice. Each conversation was followed by the third step whereby the HB-HTA team presented the results of the systematic reviews conducted. For the first brainstorming conversation, it was explained that only non-surgical treatments which are either not currently offered at our institution or for which there are challenges in access and for which scientific or experiential evidence of efficacy is available were being considered. Since drugs are routinely prescribed to patients, this treatment option was not included in our discussion. After the first brainstorming conversation, we thus presented the results of the two systematic reviews conducted to determine the efficacy and safety of non-surgical treatment as stated in the context section. Results of these systematic reviews were very close to those published by the NICE.25 The results of the systematic review on preferences were presented after the second brainstorming conversation. In a fourth step, we discussed with patients the results of these systematic reviews, compared them with the attributes and levels they spontaneously listed, and finally asked them to indicate to us which treatments and attributes were the most important in their decision to choose a non-surgical treatment.
Preference exercises
Following the focus group, we asked patients to complete 2 ranking exercises and 2 scoring exercises at home to express their preferences. Two ranking exercises were completed for each theme addressed in the focus group, that is non-surgical treatments and other attributes that may explain their choice. The first exercise consisted in ordering all items from the most preferred (1) to the least preferred (n). The second exercise was to complete a Likert scale for each item using the following levels: very important (1), important (2), somewhat important (3) and of little importance (4). Results for the four patients were summed up and a final ranking was provided. These two types of exercises were conducted in order to check the consistency of results.
Interactions with experts and patients
We consulted two economists specialized in preference-based studies, one ethicist, one medical doctor in rheumatology, one public health professional with expertise in equity and two patients. With the exception of the two patients and for one economist, the remaining participants all have extensive experience in HTA methodology. All were consulted one-on-one and provided inputs about the validity, univocity and relevance of attributes and levels selected by patients from the focus group. Discussions about the feasibility of the DCE considering these attributes and levels were also conducted, specifically about the overlap of some attributes and the number of attributes and levels. These consultations were held before and after the meetings with stakeholder committee members described below.
Discussion with HTA consultative committee members
As indicated in the context section, a committee has been set up in our institution to improve the health care pathway and to revise the services delivery for chronic pain treatment. This committee will benefit from the recommendations provided by the HTA consultative committee consulted, which consisted in two medical doctors, one HB-HTA specialist, one ethicist, one social worker, two managers, two occupational therapists, one knowledge broker and two patients. All steps of the creation process of the DCE were presented to HTA consultative committee members during two sessions in September 2018. Results of the systematic literature review on preferences were also presented, as well as the results of the focus group and the preference exercises. All attributes were discussed around two main themes: 1) are the attributes and levels selected by patients and experts meaningful to you? and 2) which attributes and levels should be considered? During the discussion, it was explained that there should be a maximum of 7–8 attributes and 5–6 levels. An iterative process was used to get a consensus on attributes and levels. Following these two sessions, a questionnaire was developed by the HB-HTA unit.
Face validity of the questionnaire for the DCE
The questionnaire for the DCE was developed in accordance with the Common Sense Model (CSM) of illness representations.26 This model stipulates that when confronted with a medical problem, patients develop cognitive and emotional representations of their condition and beliefs about possible treatments, which may guide their choice. A preliminary version of the questionnaire was sent to all patients from the focus group, one medical doctor, two patient representatives and one public health expert. We asked them to indicate if the questionnaire was easy to complete, if some questions were unclear and needed to be rephrased and whether some questions were inappropriate. For patients, we also asked them to revise again the choice of attributes and levels to ensure that they consider these as important and appropriate and that they adequately reflected their previous input. We specifically asked the medical doctor and the public health expert to suggest potential new questions and to validate the epidemiological and clinical aspects of the questionnaire (ie, some questions were about the clinical aspect of LBP).
Ethics
This study was approved by the ethics committee of the CIUSSS de l’Estrie - CHUS. All participants were informed that the results will be used to design a DCE that will inform decision makers and that it may be published in a peer-reviewed journal.
Results
As indicated above, the study used a mixed-methods approach and consisted of different consecutive steps. To illustrate the whole process, the results are described step by step.
Literature review
Search engines identified 390 articles after the removal of duplicates. Thirty-seven articles were fully read to assess their eligibility. A total of 13 articles were included for analysis. Details of the process and results can be found elsewhere.23 This literature review provided a list of 40 attributes, each specified including one to seven levels. The most cited and most important attribute for LBP patients was pain reduction. Other important attributes were capacity to realize daily life activities, fit to patient’s life, providers’ attitudes and characteristics, frame/design of the treatment (eg, supervised or not, in groups or individually), credibility of treatment, capacity to return to work, treatment frequency, onset of treatment efficacy, content of program/treatment, energy/ability to sleep, etc. The full list of attributes and levels was discussed with patients during the focus group as described in the following section.
Focus group
Four patients aged 40–71 years were recruited in a patient discussion group. All were female and suffered from chronic LBP. The non-surgical treatments emerging from the brainstorming conversation were almost the same as those retrieved by the literature reviews (ie, corticosteroid infiltration, physical exercise, physical manipulation, psychotherapy, self-management), with the exception of acupuncture. Other non-surgical treatments were also identified, such as complementary and alternative medicine (CAM) (ie, gray clay and self-hypnosis), and the external neurostimulator. Considering the high heterogeneity in physical exercise activities available, it was decided to consider mind–body–spirit (eg, yoga, tai-chi, Pilates) and active sport activities (eg, walking, swimming, riding). In total, nine non-surgical treatments were selected and subsequently ranked. From the brainstorming conversation about attributes explaining the choice of a non-surgical treatment, eight attributes spontaneously emerged from the patients (ie, pain reduction, daily life activities, biomechanical functioning, have a social life and traveling, energy/sleep problem, out-of-pocket cost, knowledge/listening of body and pain, and alertness). Then, after discussing the full list of 40 attributes from the literature, another list of 8 attributes were considered important and further selected (ie, treatment frequency, risk of relapse, onset of treatment efficacy, duration of efficacy, side-effects risks, sensation during treatment, size group and distance to treatment). This led to 16 attributes to be ranked. The only attribute that was not cited in the literature review and which emerged from the discussion as being important was alertness. The focus group also led to consider 3 levels in most attributes: same as before, a little bit less than before, and much more than before.
Preference exercises
Results of the preference exercises are provided in Tables 1 and 2. Among non-surgical treatments, psychotherapy always ranked first, followed by mind–body–spirit physical activities, and physical manipulation. To the contrary, acupuncture, CAM and corticosteroid infiltration always ranked last. Among the other attributes that may explain the choice of patients toward non-surgical treatment, pain reduction was ranked first, as it was in the scientific literature. It was followed by daily life activities and sleep problem. Interestingly, knowledge of body and pain was well ranked, as much as onset of treatment efficacy and duration of efficacy. The least important attributes were the size of the group and distance to treatment.
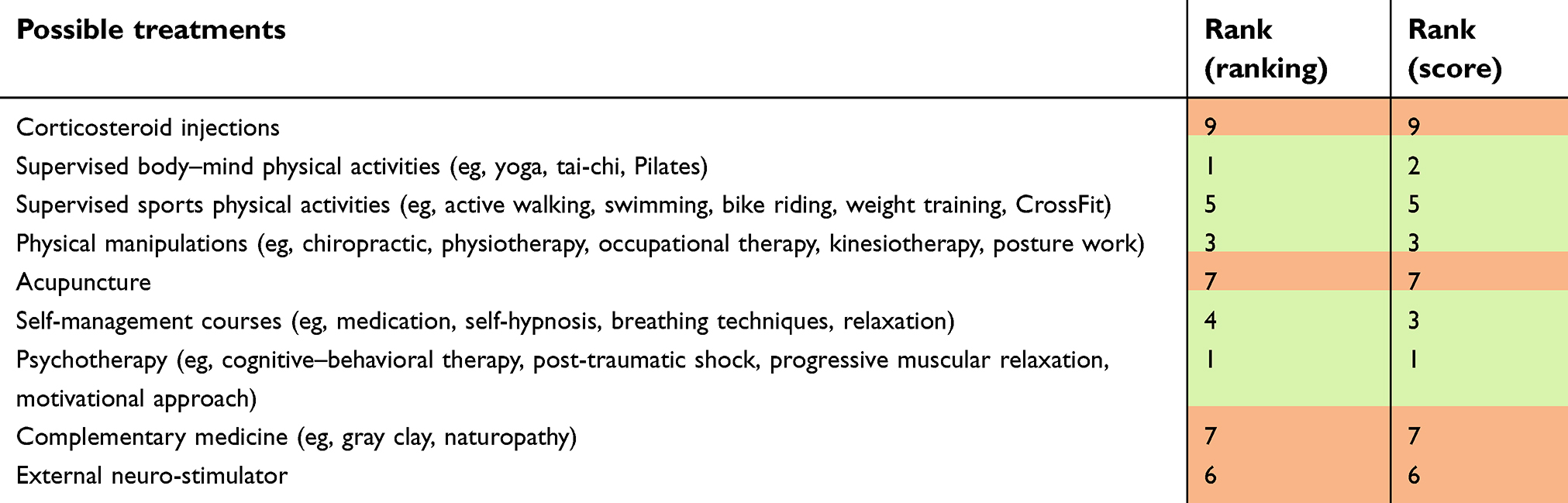 | Table 1 Ranking of treatments |
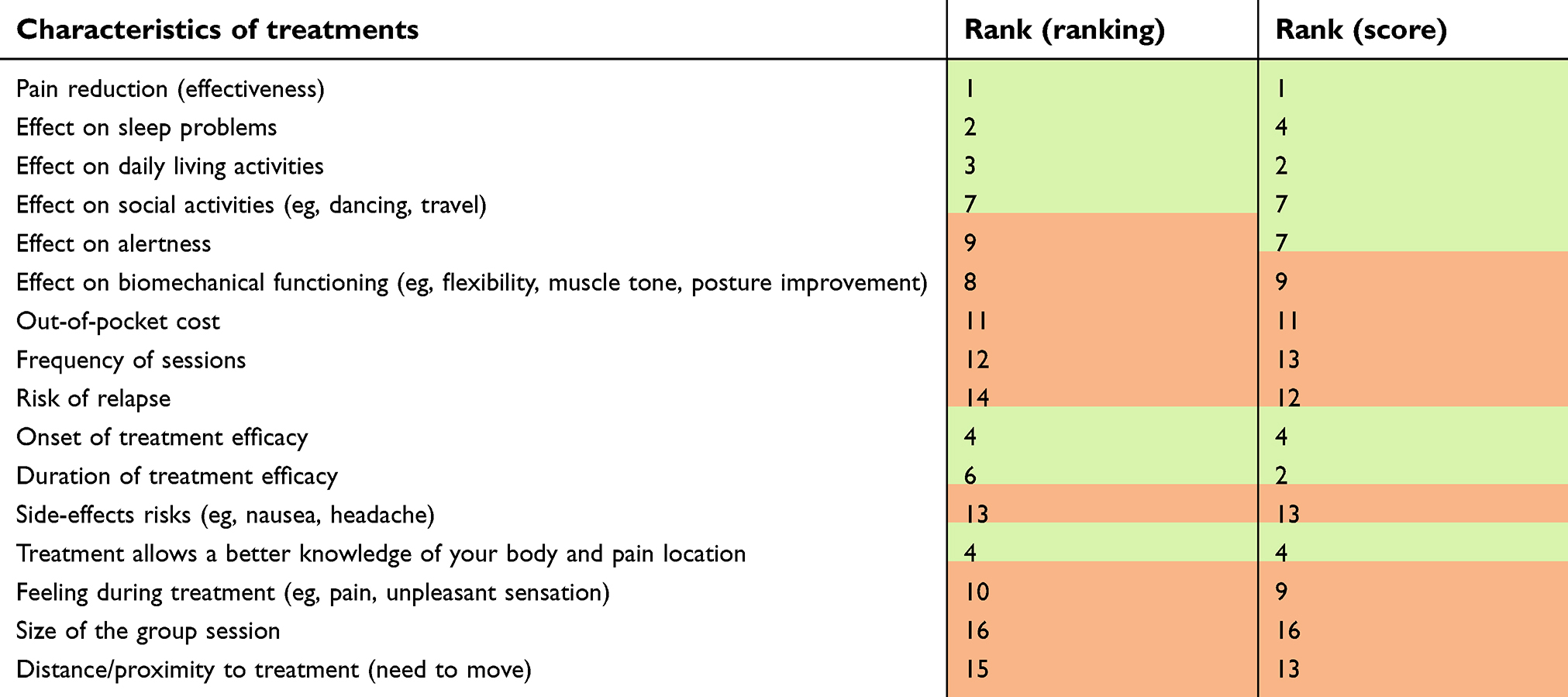 | Table 2 Ranking of treatments’ characteristics |
Considering that in a DCE it is recommended not to have more than 7 attributes or levels, it was decided to keep the 5 most preferred treatments plus corticosteroid infiltration. Indeed, even if corticosteroid infiltration was the least preferred treatment from our 4 patients, this treatment was the main concern leading to the HTA requested by our institution.
Interactions with experts and patients
One-on-one discussions with experts and patients allowed validating a first set of 8 attributes with varying levels to present to the committee members and subsequently to provide adjustments. The discussions also allowed refining the phrasing of the attributes and levels, as well as the number of attributes to retain.
Discussion with committee members
Each session with stakeholder committee members lasted 2 hrs. The iterative process allowed to discuss each of the attributes and levels from the preference exercises, as well as those most frequently cited in the literature review and others that emerged from the discussion with committee members. This led to reframe two levels in one of the attributes (ie, physical manipulation and psychotherapy in the modality treatment attribute) and to delete one attribute (ie, alertness). At this step, it was also confirmed that an overlapping risk was present between the attribute of daily living activities and the attribute of social activities, thus justifying keeping only seven attributes. These final attributes were: treatment modality, pain reduction, onset of treatment efficacy, duration of efficacy, difficulty in daily living activities, sleep problem and knowledge about their body and pain. Their associated levels are presented in Table 3.
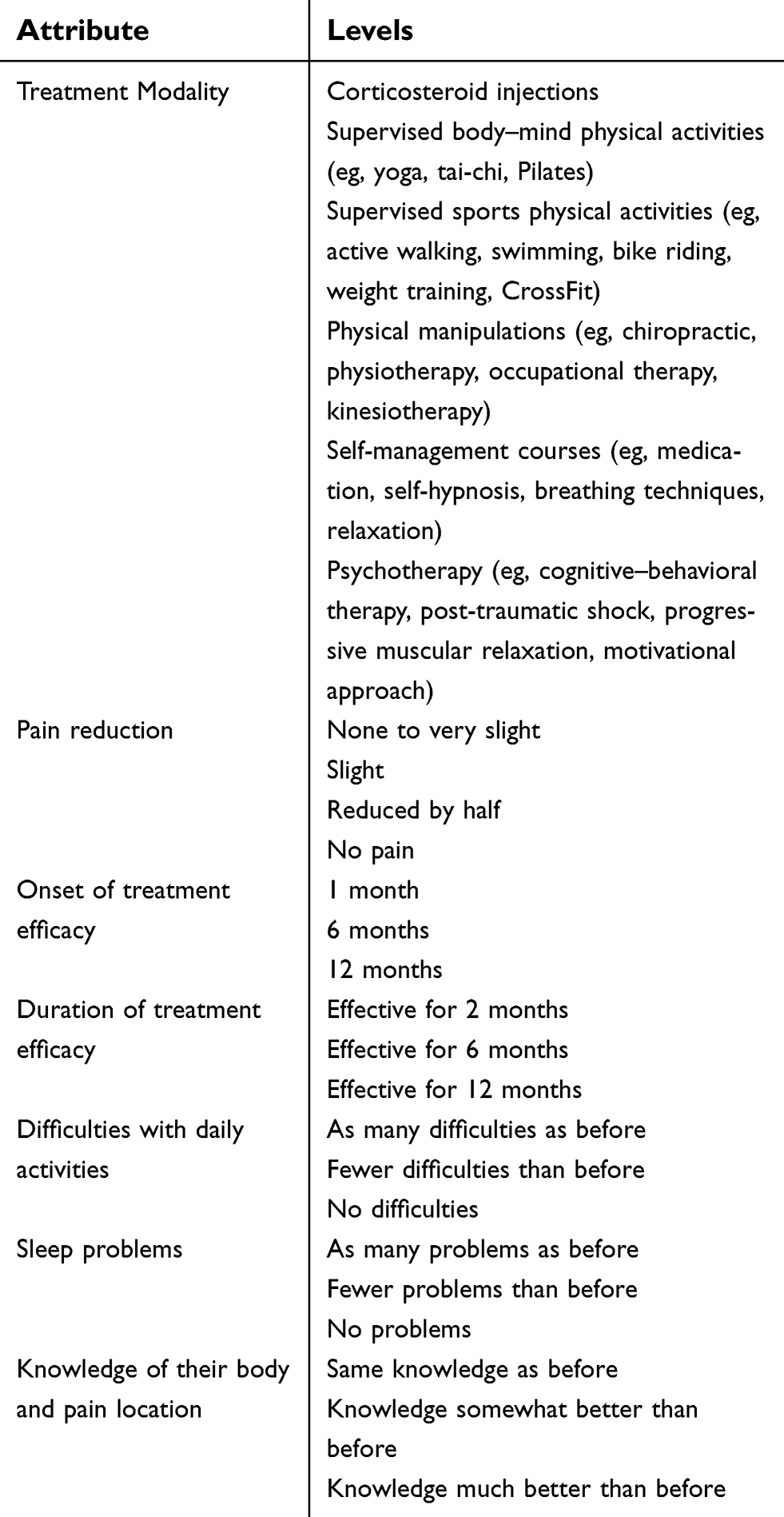 | Table 3 Attributes and levels for the DCE |
Validity of the questionnaire for the DCE
To assess the validity of the questionnaire with respect to its univocity, the relevance of its content and its easiness to complete allowed refining five questions (ie, gender, height and weight, identification of LBP, list of available diagnosis) and to improve the visual presentation of the DCE. At this step, all participants were confident that the attributes and levels selected were the most appropriate to assess the preferences of LBP patients for non-surgical treatments in our context.
Discussion
This study comprehensively describes the process of identification, refinement and selection of attributes and levels for a DCE on non-surgical treatments for LBP patients. This was the first step in the process to conduct a DCE and this was done in reference to the CSM of illness representations. It should help in the next step to elicit preferences of LBP patients towards their treatment and subsequently for our institution to offer services in line with their needs and preferences.
The novelty of our DCE is that it will consider up to six different non-surgical treatments in LBP and that these treatments are intrinsically very different from another. To our knowledge, this had not been done and existing DCE only compare a few treatments in the same family of treatment (eg, physical activities, CAM). In addition, we will also consider the attribute of “knowledge of body and pain”, which was frequently cited in the literature, but never tested in a DCE. This exercise will thus provide experiential data from patients that will complete existing data in LBP treatment (eg, clinical trials, expert consensus).
One strength of our study is that it involved a great variety of participants, which allowed to better consider the stakes in our institution alongside the needs and preferences of patients. This ensured that this exercise was not disconnected from our context and avoid unrealistic expectations from patients and health care professionals.27,28 Also, given that the focus was on patients’ needs and preferences, this facilitated the emergence of a consensus. Indeed, all participants were working together to revise a service delivery of treatments that will create a real value added for the patients.
From an HB-HTA unit point of view, this is the first time that such a unit will conduct a DCE to elicit the preferences of patients. Furthermore, this study was explicitly requested by our institution’s health care pathway animation committee. This is in line with an international tendency to consider these preferences through different ways to better inform decision making in health care.3 In this setting, the HTA consultative committee will have more data to provide contextualized recommendations to our institution. As such, the results will be directly input into the development of the organization of care. This clearly illustrates the move in our institution toward a greater consideration of patients’ needs and preferences. It is expected that this patient-centered approach will bring them more satisfaction and ultimately better services and improved outcomes. However, considering the significant amount of resources needed and the skills required to conduct such a study, it will not be possible to reproduce this process for each HB-HTA endeavor. This situation echoes another work in a HB-HTA unit where specific skills (eg, failure and mode effects analysis, technical features tests, computer sciences) were necessary to facilitate a procurement process.29 As such, it will be of greater importance to prioritize the projects in which the inclusion of a DCE will provide the most value-added for both the patient and our institution.
Finally, one limit of our study is that we could have recruited more patients in the focus group or conduct more than one focus group. This may have improved the representativeness of our sample of patients, especially since no male patients attended. However, this is counterbalanced by the numerous and various participants involved in the process of identification and selection of attributes and levels. Also, our selection is consistent with what was found in the literature. In addition, even if LBP patients are willing to participate in such activities, this may be hard for them to participate considering the cognitive effort requested during the focus group and the potential impact on their emotions, which could have potential ethical ramifications on the extent of their involvement.
Conclusion
This study is one of the few to comprehensively describe the process of identification, refinement and selection of attributes and levels for a DCE. This is also one of the first to be conducted in the context of a HB-HTA unit. This was done in a favorable context where our institution decided to go further in the development of a patient-centered care approach. The results of our study led to a balanced choice of seven attributes to be used in a DCE that will contribute to a better understanding of LBP patients’ preferences and the production of recommendations adapted both to their needs and the capacities of our institution.
Key points
This is the first study describing how patients were involved in the preparation of a discrete choice experiment in the context of a health technology assessment unit. Patients’ participation allowed to select the most important attributes and to revise the questionnaire for the discrete choice experiment.
Ethical approval
All participants were voluntary and were members of the research team.
Written Informed consent
All participants agreed to participate and were informed that the results will be analyzed anonymously before being made public.
Acknowledgments
We would like to thank all those who participated in this study, particularly members of the Association québécoise de la douleur chronique (AQDC) and professionals from the CIUSSS de l’Estrie – CHUS. This work was supported by the HB-HTA unit of the CIUSSS de l’Estrie – CHUS.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Facey KM, Hansen HP. Patient-focused HTAs. Int J Technol Assess Health Care. 2011;27:273–274. doi:10.1017/S0266462311000572
2. Poder TG. Editorial: better understanding health preferences. Int J Heal Prefer Res. 2016;1:1.
3. Mott DJ. Incorporating quantitative patient preference data into healthcare decision making processes: is HTA falling behind? Patient - Patient-Centered Outcomes Res. 2018;11:249–252. doi:10.1007/s40271-018-0305-9
4. Brooker A-S, Carcone S, Witteman W, Krahn M. Quantitative patient preference evidence for health technology assessment: a case study. Int J Technol Assess Health Care. 2013;29:290–300. doi:10.1017/S0266462313000329
5. Kievit W, Tummers M, van Hoorn R, et al. Taking patient heterogeneity and preferences into account in health technology assessments. Int J Technol Assess Health Care. 2017;33:562–569. doi:10.1017/S0266462317000885
6. Poder TG, Bellemare CA, Bédard SK, Lemieux R. Social acceptance and population confidence in telehealth in Quebec. BMC Health Serv Res. 2015;15:72. doi:10.1186/s12913-015-0718-2
7. Aboagye E. Valuing individuals’ preferences and health choices of physical exercise. Pain Ther. 2017;6:85–91. doi:10.1007/s40122-017-0067-4
8. Gardner T, Refshauge K, McAuley J, Goodall S, Hübscher M, Smith L. Patient led goal setting in chronic low back pain – what goals are important to the patient and are they aligned to what we measure? Patient Educ Couns. 2015;98:1035–1038. doi:10.1016/j.pec.2015.04.012
9. Ng-Mak DS, Poon JL, Rajagopalan K, et al. Qualitative study of patients’ preferences for bipolar depression treatment. Value Heal. 2015;18:A123. doi:10.1016/j.jval.2015.03.718
10. Craig BM, Lancsar E, Mühlbacher AC, Brown DS, Ostermann J. Health preference research: an overview. Patient - Patient-Centered Outcomes Res. 2017;10:507–510. doi:10.1007/s40271-017-0253-9
11. Marsh K, Caro JJ, Zaiser E, Heywood J, Hamed A. Patient-centered decision-making: lessons from multi-criteria decision analysis for quantifying patient preferences. Int J Technol Assess Health Care. 2018;34:105–110. doi:10.1017/S0266462317001118
12. Johnson FR, Zhou M. Patient preferences in regulatory benefit-risk assessments: a US perspective. Value Heal. 2016;19:741–745. doi:10.1016/j.jval.2016.04.008
13. Egbrink MO, IJzerman M. The value of quantitative patient preferences in regulatory benefit-risk assessment. J Mark Access Heal Policy. 2014;2:22761. Availble from:
14. Vass C, Rigby D, Payne K. The role of qualitative research methods in discrete choice experiments. Med Decis Making. 2017;37:298–313. doi:10.1177/0272989X16683934
15. Mathijssen E, van Heuckelum M, van Dijk L, et al. A discrete choice experiment on preferences of patients with rheumatoid arthritis regarding disease-modifying antirheumatic drugs: the identification, refinement and selection of attributes and levels. Patient Prefer Adherence. 2018;12:1537–1555. doi:10.2147/PPA.S176067
16. Mühlbacher A, Johnson FR. Choice experiments to quantify preferences for health and healthcare: state of the practice. Appl Health Econ Health Policy. 2016;14:253–266. doi:10.1007/s40258-016-0232-7
17. McFadden D. Conditional logit analysis of qualitative choice behavior. In: Zarembka P, editor. Front Economy. New Ork: Academic Press; 1974:105–142.
18. Haldeman S, Dagenais S. A supermarket approach to the evidence-informed management of chronic low back pain. Spine J. 2008;8:1–7. doi:10.1016/j.spinee.2007.10.009
19. Roy M, Ganache I, Dagenais P. Advocating for a better engagement of patients, users, caregivers, and citizens in healthcare and social services technology assessment (HSTA). Int J Hosp-Based Health Technol Assess. 2018;1:15–18.
20. Louvière JJ, Lancsar E. Choice experiments in health: the good, the bad, the ugly and toward a brighter future. Heal Econ Policy Law. 2009;4:527. doi:10.1017/S1744133109990193
21. Coast J, Al-Janabi H, Sutton EJ, et al. Using qualitative methods for attribute development for discrete choice experiments: issues and recommendations. Health Econ. 2012;21:730–741. doi:10.1002/hec.1739
22. Bridges JFP, Hauber AB, Marshall D, et al. Conjoint analysis applications in health – a checklist: a report of the ISPOR good research practices for conjoint analysis task force. Value Heal. 2011;14:403–413. doi:10.1016/j.jval.2010.11.013
23. Poder TG, Beffarat M. Factors underlying the choice of Low Back Pain (LBP) patients in non-surgical treatments: a systematic review. J Patient Experience. In press 2019.
24. Pluye P, Robert E, Cargo M, Bartlett G. Proposal: A Mixed Methods Appraisal Tool for Systematic Mixed Studies Reviews. Montréal McGill Univ; 2011:1–8.
25.
26. Leventhal HA, Brissette I, Leventhal EA. The common-sense model of self-regulation of health and illness. In: Cameron LD, Leventhal HA, editors. The Self-Regulation of Health and Illness Behaviour. London: Routledge; 2003:42–65.
27. Poder TG, Bellemare CA. Importance of contextual data in producing health technology assessment recommendations: a case study. Int J Technol Assess Health Care. 2018;34:63–67. doi:10.1017/S0266462317004469
28. Poder TG, Carrier N, Bédard SK. Health technology assessment unit processes for the validation of an information tool to involve patients in the safety of their care. Int J Technol Assess Health Care. 2018;34:378–387. doi:10.1017/S0266462318000375
29. Poder TG. Using the health technology assessment toolbox to facilitate procurement: the case of smart pumps in a Canadian hospital. Int J Technol Assess Health Care. 2017;33:54–62. doi:10.1017/S0266462317000125
 © 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.