Back to Journals » Journal of Asthma and Allergy » Volume 15
A Cross-Sectional Study on Prescription Patterns of Short-Acting β2-Agonists in Patients with Asthma: Results from the SABINA III Colombia Cohort
Authors Pedrozo-Pupo JC, Pacheco Gallego MC ![]() , Baños Álvarez IDJ, Jaller Raad RA, Caballero Pinilla AC, Reynales Londoño H, Bernal Villada L, Beekman M
, Baños Álvarez IDJ, Jaller Raad RA, Caballero Pinilla AC, Reynales Londoño H, Bernal Villada L, Beekman M ![]()
Received 4 March 2022
Accepted for publication 20 August 2022
Published 26 August 2022 Volume 2022:15 Pages 1167—1178
DOI https://doi.org/10.2147/JAA.S365009
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Amrita Dosanjh
John Carlos Pedrozo-Pupo,1 Manuel Conrado Pacheco Gallego,2 Iván de Jesús Baños Álvarez,3 Rodolfo Antonio Jaller Raad,4 Andrea Carolina Caballero Pinilla,5 Humberto Reynales Londoño,6 Laura Bernal Villada,7 Maarten Beekman8
1PREVICARE LTDA. Programa de Medicina, Facultad de Ciencias de la Salud, Universidad del Magdalena, Santa Marta, Colombia; 2División de Neumología y Endoscopia Respiratoria, Departamento de Medicina Interna, Universidad Tecnológica de Pereira, Universidad Visión de las Américas, RESPIREMOS Centro de Neumología y Endoscopia Respiratoria, Pereira, Colombia; 3Centro de Rehabilitación Pulmonar Integral S.A.S., Cartagena, Colombia; 4Department of Allergy and Immunology, Centro de Investigación Médico Asistencial S.A.S, Barranquilla, Colombia; 5Centro de Investigación Clínica, Caja de Compensación Familiar CAFAM, Sede Centro de Atención en Salud CAFAM Floresta, Bogotá, Colombia; 6Clinical Research Department, Centro de Atención e Investigación Médica - CAIMED, Chía, Colombia; 7Andean Cluster - Respiratory & Immunology, AstraZeneca, Bogotá, Colombia; 8Respiratory & Immunology AstraZeneca, The Hague, the Netherlands
Correspondence: John Carlos Pedrozo-Pupo, PREVICARE LTDA. Programa de Medicina, Facultad de Ciencias de la Salud, Universidad del Magdalena, Santa Marta, Colombia, Tel +57 603017384712, Email [email protected]
Purpose: Overuse of short-acting β2-agonists (SABAs) for asthma is associated with a significant increase in exacerbations and healthcare resource use. However, limited data exist on the extent of SABA overuse outside of Europe and North America. As part of the multi-country SABA use IN Asthma (SABINA) III study, we characterized SABA prescription patterns in Colombia.
Patients and Methods: This observational, cross-sectional cohort study of SABINA III included patients (aged ≥ 12 years) with asthma recruited from seven sites in Colombia. Demographics, disease characteristics (including investigator-defined asthma severity guided by the 2017 Global Initiative for Asthma report), and asthma treatments prescribed (including SABAs and inhaled corticosteroids [ICS]) in the 12 months preceding the study were recorded using electronic case report forms during a single study visit.
Results: Of 250 patients analyzed, 50.4%, 33.2%, and 16.4% were enrolled by pulmonologists, general medicine practitioners, and allergists, respectively. Most patients were female (74.0%) and had moderate-to-severe asthma (67.6%). Asthma was partly controlled or uncontrolled in 57.6% of patients, with 15.6% experiencing ≥ 1 severe exacerbation 12 months before the study visit. In total, 4.0% of patients were prescribed SABA monotherapy and 55.6%, SABA in addition to maintenance therapy. Overall, 39.2% of patients were prescribed ≥ 3 SABA canisters in the 12 months before the study visit; 25.2% were prescribed ≥ 10 canisters. Additionally, 17.6% of patients purchased SABAs over the counter, of whom 43.2% purchased ≥ 3 canisters. Maintenance medication in the form of ICS or ICS/long-acting β2-agonist fixed-dose combination was prescribed to 36.0% and 66.8% of patients, respectively.
Conclusion: Our findings suggest that prescription/purchase of ≥ 3 SABA canisters were common in Colombia, highlighting a public health concern. There is a need to improve asthma care by aligning clinical practices with the latest evidence-based treatment recommendations to improve asthma management across Colombia.
Keywords: exacerbations, inhaled corticosteroids, over-prescription, practice patterns, prescriptions
Introduction
Latin America is a highly diverse region which is reflected in the variability in rates, determinants, and burden of asthma among its countries.1,2 Nevertheless, asthma has a substantial disease burden in the region, with results from the 2011 Latin America Asthma Insight and Management (LA AIM) survey reporting high rates of uncontrolled asthma (35.0%) and insufficient use of maintenance medication.1 Although there is a paucity of country-specific data from Colombia on asthma epidemiology and treatment patterns, currently available evidence suggests that asthma places a significant burden on both patients and healthcare systems in Colombia. Indeed, a cross-sectional, population-based survey, conducted in six Colombian cities (Barranquilla, Bogotá, Bucaramanga, Cali, Medellín, and San Andrés Island) from 2009 to 2010, reported an overall asthma prevalence of 12.0%.3 Moreover, disease severity was high among patients reporting asthma symptoms, with 43.0% of symptomatic patients requiring an emergency department visit or hospitalization in the year prior to taking the survey.3 This finding is likely attributable to suboptimal asthma control1 and a general lack of awareness of current treatment guidelines amongst healthcare practitioners (HCPs).4 In addition, another cross-sectional study of patients (aged ≥12 years) with asthma from specialist ambulatory centers across Colombia, Chile, Argentina, and Mexico reported that only 43.4% of patients had controlled asthma, underscoring the high rate of uncontrolled asthma in parts of Latin America, including Colombia, even at the tertiary level of care.5
Despite asthma being a chronic variable inflammatory disease,6 many patients rely on SABAs for symptomatic relief at the expense of daily maintenance medication, thereby not treating the underlying inflammation of asthma. As a result of growing evidence that SABA overuse is associated with an increased risk of exacerbations, hospitalizations, and mortality,7,8 in 2019, the Global Initiative for Asthma (GINA) updated its report to no longer recommend SABA monotherapy, and now instead recommends as-needed low-dose ICS-formoterol as the preferred reliever for adults and adolescents with mild asthma, and for those with moderate-to-severe asthma who are prescribed ICS-formoterol maintenance therapy.9,10
In light of GINA updated treatment recommendations, an examination of the prevalence of SABA use and its consequences is required to provide clinicians and healthcare policymakers with a clear picture on the extent of SABA overuse and to advocate for changes in clinical practice to ensure that treatment practices align with the latest evidence-based treatment recommendations. However, whilst several surveys have been conducted across Latin American populations (Argentina, Brazil, Mexico, Venezuela, and Puerto Rico),1,11 examining the use of controller and reliver medications, data from Colombia on trends in asthma medication use, including SABA use, are lacking. Therefore, to fill this gap, Colombia was included in the SABA use IN Asthma (SABINA) III pillar12 of the SABINA Programme,13 which was designed to capture clinical information, including SABA prescription data, in local healthcare settings using electronic case report forms (eCRFs) to overcome the lack of healthcare databases as central repositories of clinical information in a large part of the world. The primary objective of SABINA Colombia was to describe the prevalence and pattern of SABA prescriptions and other asthma treatments to provide real-world evidence on asthma management practices in the country.
Patients and Methods
Study Design and Data Source
Detailed methodology for SABINA III has been published previously.12 In brief, this was an observational, cross-sectional study conducted at seven centers across Colombia. Patients were recruited from August 2019 to December 2019. The study sites were selected using purposive sampling with the aim of obtaining a nationally representative sample of both physicians (primary care physicians and respiratory specialists) and patients. Retrospective data were obtained from existing medical records, and patient data, including an assessment of current asthma symptom control, were collected during a study visit and entered into an electronic eCRF. Physicians entered data on exacerbation history, comorbidities, and information on medication prescriptions for asthma in the eCRF based on patient medical records.
Study Population
At each site, patients aged ≥12 years with a diagnosis of asthma in their medical records, with ≥3 consultations with an HCP or practice, and medical records containing data for ≥12 months before the study visit were enrolled. Patients with other chronic respiratory diseases, such as chronic obstructive pulmonary disease, or a diagnosis of an acute or chronic condition that, in the investigator’s opinion, would limit the patients’ ability to participate in the study, were excluded. Signed informed consent was obtained from patients or their legal guardians.
Variables
Patients were categorized by sociodemographic characteristics (age, number of comorbid conditions, body mass index [BMI], smoking status, educational level, and medication reimbursement status), practice type (primary or specialist care), and asthma characteristics (investigator-defined asthma severity guided by GINA 2017 treatment steps14 [GINA treatment steps 1–2, mild asthma; GINA treatment steps 3–5, moderate-to-severe asthma], time since asthma diagnosis, and number of severe exacerbations in the 12 months before the study visit). Asthma symptom control was evaluated using the GINA 2017 assessment of asthma control14 and categorized as well controlled, partly controlled, or uncontrolled.
In terms of asthma treatments, patients were categorized by SABA canister prescriptions (0, 1–2, 3–5, 6–9, 10–12, and ≥13 canisters) and ICS canister prescriptions (categorized according to the prescribed average daily dose as low, medium, or high14) in the 12 months preceding the study visit. Prescription of ≥3 SABA canisters per year was defined as over-prescription.13 Data were also collected on prescriptions for asthma treatments, including ICS monotherapy, fixed-dose combinations of ICS with long-acting β2-agonists (LABAs), short-course oral corticosteroids (OCS), OCS maintenance treatment, and antibiotics prescribed for asthma. Data on SABA purchases over the counter (OTC) without a prescription in the 12 months before the study visit were obtained directly from patients during the study visit.
Statistical Analysis
Descriptive analyses were used to characterize patients according to baseline demographics and clinical characteristics. Continuous variables were summarized by the number of non-missing values, mean, standard deviation (SD), median, and range. Categorical variables were summarized by frequency counts and percentages.
Results
Patient Disposition
Of 250 patients analyzed in this study, 50.4% were enrolled by pulmonologists, 33.2% by general medicine practitioners, and 16.4% by allergists (Figure 1). Overall, 32.4% of patients had investigator-classified mild asthma (GINA treatment steps 1–2) and 67.6%, moderate-to-severe asthma (GINA treatment steps 3–5). Patients treated by pulmonologists had predominantly moderate-to-severe asthma (92.9%), while the majority treated by allergists had mild asthma (92.7%). A total of 41.0% and 59.0% of patients treated by general medicine practitioners had mild and moderate-to-severe asthma, respectively.
 |
Figure 1 Patient population by practice type and asthma severity. |
Patient Characteristics
The median (minimum, maximum) age of patients was 53.0 (18.0, 81.0) years, with more than half of the patients (54.0%) aged 18–54 years (Table 1). Most patients were female (74.0%), had never smoked (85.2%), and were overweight or obese (65.2%). In total, 32.8% of patients had received university and/or post-graduate education. Almost all patients (97.6%) had received fully reimbursed healthcare.
 |
Table 1 Demographics and Baseline Characteristics by Asthma Severity in the SABINA III Colombia Cohort |
Disease Characteristics
Patients had a mean (SD) duration of asthma of 23.1 (19.5) years (Table 2). Most patients were at GINA treatment step 4 (28.0%) or step 2 (24.4%). Approximately 45.2% and 22.4% of patients had 1–2 and ≥3 comorbidities, respectively. Patients reported a mean (SD) of 0.3 (1.0) severe exacerbations, with 15.6% of patients experiencing ≥1 severe exacerbation in the 12 months before the study visit. Overall, the level of asthma symptom control was assessed as well controlled in 42.4%, partly controlled in 30.0%, and uncontrolled in 27.6% of patients. A total of 76.5% of patients with mild asthma had partly or well-controlled asthma compared with 70.4% of those with moderate-to-severe asthma.
 |
Table 2 Asthma Characteristics According to Investigator-Classified Asthma Severity in the SABINA III Colombia Cohort |
Asthma Treatments in the 12 Months Before the Study Visit
SABA Prescription Categorization
Overall, 39.2% of patients were prescribed ≥3 SABA canisters; 25.2% were prescribed ≥10 canisters (Figure 2). Approximately 40.0% of patients had not been prescribed SABAs. A higher proportion of patients with mild asthma vs those with moderate-to-severe asthma were prescribed ≥3 SABA canisters (54.3% vs 32.0%).
 |
Figure 2 SABA prescription categorization in the 12 months before the study visit. Abbreviations: SABA, short-acting β2 agonist. |
SABA Monotherapy and SABA in Addition to Maintenance Therapy
Only 4.0% of patients were prescribed SABA monotherapy, with a mean (SD) of 11.3 (11.1) SABA canisters (Table 3). As expected, all of these patients were classified as having mild asthma. Over half of all patients (55.6%) were prescribed SABA in addition to maintenance therapy, with this occurring in a higher proportion of patients with mild asthma vs those with moderate-to-severe asthma (71.6% vs 47.9%). These patients were prescribed a mean (SD) of 8.7 (8.7) SABA canisters, with 66.2% prescribed ≥3 SABA canisters and 42.4% prescribed ≥10 SABA canisters.
 |
Table 3 SABA Prescriptions in the 12 Months Before the Study Visit in the SABINA III Colombia Cohort |
SABA Purchase Without a Prescription
A total of 17.6% of patients purchased SABA OTC, of whom 43.2% purchased ≥3 SABA canisters (Table 4).
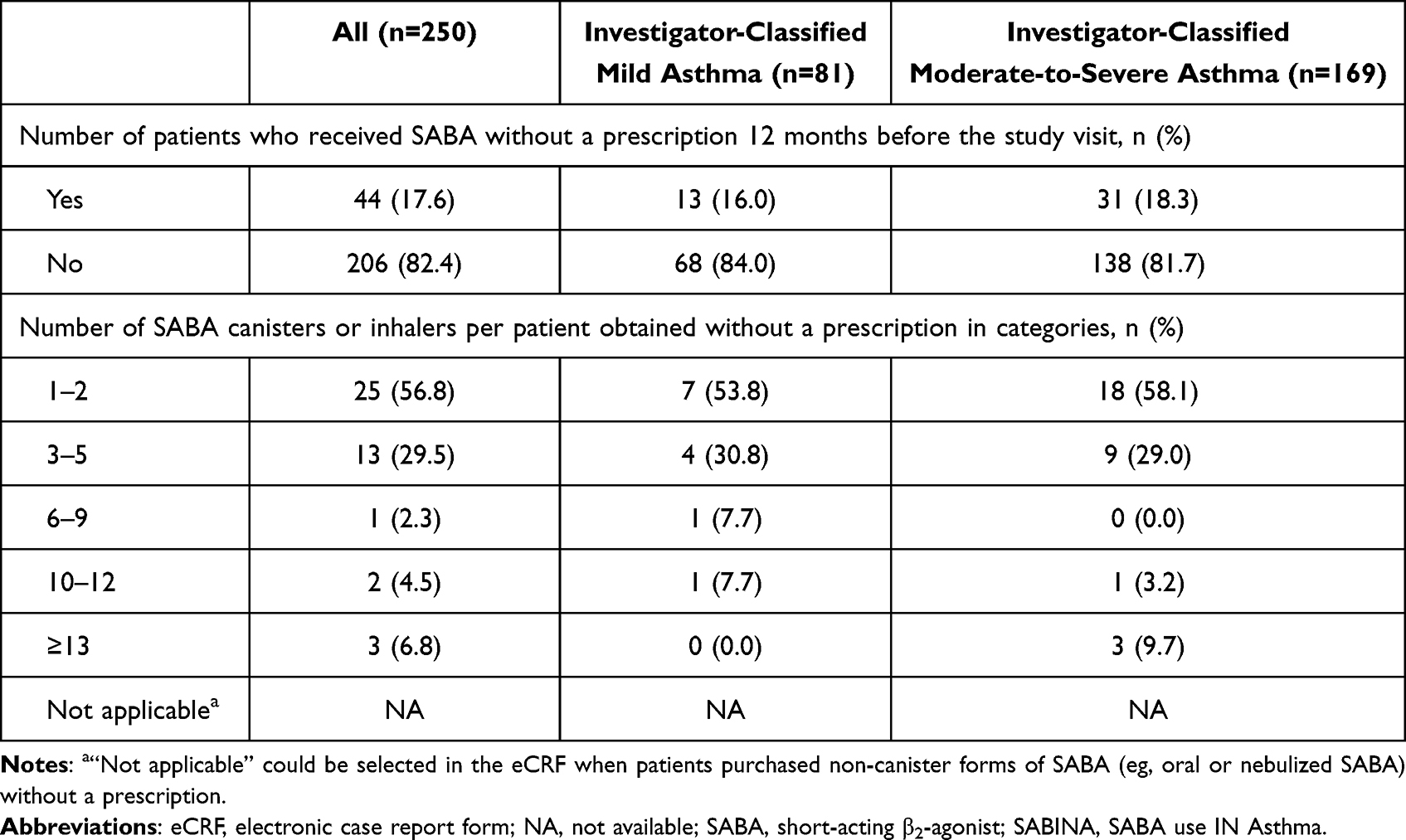 |
Table 4 Patients Who Received SABA Without a Prescription in the 12 Months Before the Study Visit in the SABINA III Colombia Cohort |
Maintenance Medication, OCS Bursts and Antibiotics
Overall, maintenance medication in the form of ICS was prescribed to 36.0% of patients, with a mean (SD) of 7.2 (4.8) ICS canisters per patient in the 12 months before the study visit. Most of these patients (77.8%) had mild asthma (Table 5). A fixed-dose combination of an ICS/LABA was prescribed to approximately two-thirds (66.8%) of patients, almost all of whom had moderate-to-severe asthma. Of these patients, 22.8% were prescribed low-dose ICS, 41.3% medium-dose ICS, and 35.9% high-dose ICS.
 |
Table 5 Other Categories of Asthma Treatment Prescribed in the 12 Months Before the Study Visit in the SABINA III Colombia Cohort |
Short-course OCS were prescribed to 11.6% of patients, while 5.2% of patients were prescribed antibiotics for asthma (Table 5). A marginally higher proportion of patients with moderate-to-severe asthma versus those with mild asthma received ≥1 OCS burst (12.4% vs 9.9%) or antibiotic (6.5% vs 2.5%) prescriptions.
Discussion
This nationwide cross-sectional study was conducted as part of SABINA III to characterize the asthma patient population and describe the extent of SABA prescriptions in Colombia. Although most patients were prescribed maintenance therapy in the form of either ICS or ICS/LABA fixed-dose combination, SABA over-prescription was common across Colombia, with almost 40% of patients prescribed ≥3 SABA in the 12 months before the study visit. Overall, these findings are consistent with previous studies from Latin America that have also reported over-reliance on SABAs,1,11 as well as the aggregated data of all 24 SABINA III countries, wherein 38.0% of patients with asthma were prescribed ≥3 SABA canisters annually.12 Taken together, these results corroborate the recent position statement on asthma management in Latin America that noted that SABA over-reliance is an important health concern.15
Previously, the 2003 Asthma Insights and Reality in Latin America (AIRLA) survey, which interviewed 2184 patients with asthma across 11 Latin American countries, including Colombia, reported that within a 4-week time period, 37.0% of patients reported receiving prescriptions for maintenance medication, while 54.0% reported using prescription reliever medication,4 suggesting underuse of maintenance therapy and potential overuse of SABA. Similarly, results from the LA AIM survey in 2169 patients with asthma from 5 Latin America countries (Argentina, Brazil, Mexico, Venezuela, and Puerto Rico) reported that whilst almost half of all patients used reliever medication in the last 4 weeks, only 32% of patients had used maintenance medication during this time period.1 Therefore, our results, almost 20 years later, suggest that improvements in asthma management in Colombia may be minimal with respect to the pervasiveness of SABA use and ICS underuse. Notably, any improvements appear to have been primarily driven by increased maintenance medication use, with nearly all patients from this Colombian cohort prescribed maintenance medication, and more than two-thirds prescribed fixed-dose combination ICS/LABA; this was considerably higher than that observed in previous reports from Latin America and may reflect access to specialists care.16 Nevertheless, patients prescribed ICS monotherapy received a mean of 7.2 canisters for 12 months, suggesting potential ICS underuse. Importantly, not all SABAs were obtained with prescriptions, with unregulated SABA medication obtained OTC further compounding SABA overuse. In Colombia, beclomethasone and salbutamol are the only two asthma medications included in the national formulary.17 To prescribe other asthma medications, such as ICS/LABA, and ensure that patients continue to receive healthcare reimbursement, physicians use MIPRES, an online tool implemented by the Ministry of Health and Social Protection in Colombia in 2016, to facilitate centralized prescription of medications that cannot be paid for through the capitation payment unit.18 While this tool has proven effective at delivering medications to patients in a timely manner,19 it is possible that physicians may be more inclined to prescribe SABAs as it is more convenient to arrange reimbursement for these therapies. Our data suggest the need for a change in the national formulary in Colombia to include additional maintenance medications in order to improve availability and accessibility to these treatments. There is also a need for regulations that limit physicians from over-prescribing SABA. Furthermore, since the Ministry of Health and Social Protection does not intervene in the process of prescription through MIPRES,20 regulations may be required to ensure that patients receive optimal medication and SABA over-prescription is prevented.
In Colombia, evidence linking SABA use to asthma burden and costs has been previously reported. Indeed, results from a study conducted in 2018 involving >20,000 patients with asthma in Colombia concluded that health service utilization was directly linked to asthma severity and that hospitalizations, general physician visits, and SABA medications had the greatest impact on rising healthcare resource utilization costs.21 Taken together with findings from the SABINA III study,12 which indicated that ≥3 SABA prescriptions/year (versus 1−2 SABA prescriptions) were associated with significantly increased rate of severe exacerbations and increasingly lower odds of controlled or partly controlled asthma across many countries, healthcare settings and asthma severities, there is a clear need to ensure that clinical practices are aligned with current asthma treatment guidelines in Colombia. The updated GINA report now recommends eliminating SABA monotherapy,10 and country-specific guidelines in Latin America have started to follow suit. For instance, the 2020 Brazilian Thoracic Association guidelines prohibit SABA monotherapy and recommend an ICS/SABA combination due to its affordability compared with an ICS/LABA combination.22 The Colombian Ministry of Health and Social Protection developed an evidence-based national guideline for pediatric asthma treatment.23 However, there are currently no national guidelines, consensus, or recommendations available for the treatment of adult asthma in Colombia, which may hinder evidence-based treatment practices in the country.
Prevention of SABA over-prescription should also involve targeting patient-centered drivers of poor adherence to maintenance medication, particularly since failure to treat the underlying inflammation of asthma with ICS will drive patient reliance on SABA for rapid symptom relief. Results from a targeted review of qualitative studies indicated that key drivers affecting medication adherence in asthma were high costs of asthma medication, suboptimal knowledge about asthma treatment, and poor patient-physician communication.24 Notably, due to operational challenges in conducting such studies at a primary care level, a substantial proportion of patients were enrolled by pulmonologists and/or allergists. Primary care centers are often the first points of contact for most patients with asthma in Colombia.25 Primary care physicians may be less likely to follow asthma treatment guidelines, in part due to lack of awareness and time,26–30 and thus the current study may have underestimated SABA over-prescription. The Colombian healthcare system, which previously favored hospital-based and highly specialized care, enacted Law 1438 in 2011 to reinforce the role of primary care centers in addressing the country’s health priorities.25,30 This is a step in the right direction; however, educating patients about globally recommended asthma treatment regimens through primary healthcare centers in addition to paving the way for a robust healthcare infrastructure are needed to reduce reliance on SABAs for symptom relief.
Despite the fact that two-thirds of patients in this study had moderate-to-severe asthma, approximately three-quarters had well-controlled or partly controlled asthma, which was considerably better than that observed from previous reports from Latin America.1,4,11,31,32 Thus, patients had a relatively low exacerbation burden compared with other countries included in the SABINA III study.12 However, the lower exacerbation burden despite prevalent SABA over-prescription may potentially be due to incomplete medical records and/or underreporting of exacerbation data by patients, combined with stockpiling of SABA by patients as a precautionary measure. Of note, 15.0% of patients with mild asthma were seeking treatment from allergists, potentially suggesting the presence of comorbidities such as rhinitis, which is prevalent in at least 32.0% of patients in Colombia.3
To our knowledge, this is the first study to assess SABA prescriptions patterns in Colombia. Moreover, the use of a standardized threshold for defining high SABA use will enable comparison of SABA use both across neighboring regions and countries and globally. However, certain limitations should be considered. Firstly, this study was descriptive in nature and no statistical analyses were performed. In addition, due to low patient numbers, it was not feasible to examine the association between SABA prescriptions and asthma-related clinical outcomes. Moreover, the recruitment of a greater number of patients with moderate-to-severe asthma precluded comparisons across asthma severities. As data entry into the eCRF relied on a physician’s assessment as well as patient recall, these findings may be impacted by response/recall bias. Furthermore, SABA prescriptions were used as a proxy for SABA use; therefore, it is entirely possible that patients did not use all the SABAs they were prescribed, potentially leading to an over- or underestimation of SABA use. Data also do not fully capture over-prescription of other forms of SABA administration, such as oral (tablets) and nebulized SABA. Lastly, due to the exclusion of adolescents or children, the study may not sufficiently reflect the demographics of the asthma population in Colombia. Indeed, the aforementioned cross-sectional, population-based study across six Colombian cities found that the prevalence of asthma symptoms was 12.0%, of which 46.3% was contributed by patients aged ≤17 years.3 Nevertheless, these real-world data on SABA prescription patterns can provide the starting point for clinicians and policy makers to make targeted changes to improve treatment outcomes in patients with asthma in Colombia.
Conclusions
Results from SABINA Colombia demonstrated that SABA over-prescription was widely prevalent in patients with asthma who were treated by pulmonologists, general medicine practitioners, and allergists. A similar assessment of prescription trends targeted exclusively at primary care may reveal that actual SABA use in Colombia is greater than that documented in our study. Overall, these findings highlight that SABA over-prescription remains a public health concern in Colombia, necessitating healthcare providers, policymakers, and government stakeholders to work together to ensure that clinical practices are aligned with the latest evidence-based treatment recommendations to improve asthma management across Colombia.
Abbreviations
AIRLA, Asthma Insights and Reality in Latin America; BMI, Body mass index; CI, Confidence interval; eCRF, Electronic case report form; GINA, Global Initiative for Asthma; HCP, Healthcare practitioner; ICS, Inhaled corticosteroids; LA AIM, Latin America Asthma Insight and Management; LABA, Long-acting β2-agonist; OCS, Oral corticosteroids; OTC, Over the counter; SABA, Short-acting β2-agonist; SABINA, SABA use IN Asthma; SD, Standard deviation.
Data Sharing Statement
Data underlying the findings described in this article may be obtained in accordance with AstraZeneca’s data sharing policy described at https://astrazenecagrouptrials.pharmacm.com/ST/Submission/Disclosure.
Ethics Approval and Informed Consent
The study was approved by the ethics committee of Comfamiliar Clinic in Pereira, Universidad Tecnológica de Pereira in Pereira, CAIMED in Chía, Comité de Ética Caja de Compensación Familiar CAFAM in Bogota, and Centro de Rehabilitación Pulmonar Integral S.A.S. in Cartagena and conducted in accordance with the study protocol and the Declaration of Helsinki.
Acknowledgments
Medical writing support was provided by Niraj Babu, PhD, of Cactus Life Sciences (part of Cactus Communications), Mumbai, India in accordance with the Good Publication Practice (GPP3) guidelines (http://www.ismpp.org/gpp3) and funded by AstraZeneca.
Funding
AstraZeneca funded the SABINA studies and was involved in designing the program, developing the study protocol, conducting the studies, and performing the analyses. AstraZeneca was given the opportunity to review the manuscript before submission and funded medical writing support.
Disclosure
Dr Andrea Carolina Caballero Pinilla reports personal fees from SANOFI, personal fees from GLAXO SMITHKLINE, personal fees from NOVARTIS, outside the submitted work. LBV is an employee of AstraZeneca and is the R&I Manager for the Andean Cluster. MB was an employee of AstraZeneca at the time this study was conducted. All other authors have no conflicts of interest to disclose.
References
1. Maspero JF, Jardim JR, Aranda A, et al. Insights, attitudes, and perceptions about asthma and its treatment: findings from a multinational survey of patients from Latin America. World Allergy Organ J. 2013;6(1):19. doi:10.1186/1939-4551-6-19
2. Forno E, Gogna M, Cepeda A, et al. Asthma in Latin America. Thorax. 2015;70(9):898–905. doi:10.1136/thoraxjnl-2015-207199
3. Dennis RJ, Caraballo L, García E, et al. Prevalence of asthma and other allergic conditions in Colombia 2009–2010: a cross-sectional study. BMC Pulm Med. 2012;12:17. doi:10.1186/1471-2466-12-17
4. Neffen H, Fritscher C, Schacht FC, et al. Asthma control in Latin America: the Asthma Insights and Reality in Latin America (AIRLA) survey. Rev Panam Salud Publica. 2005;17(3):191–197. doi:10.1590/S1020-49892005000300007
5. Neffen H, Chahuan M, Hernandez DD, et al. Key factors associated with uncontrolled asthma - The Asthma Control in Latin America Study. J Asthma. 2020;57(2):113–122. doi:10.1080/02770903.2018.1553050
6. Holgate ST, Wenzel S, Postma DS, Weiss ST, Renz H, Sly PD. Asthma. Nat Rev Dis Primers. 2015;1:15025. doi:10.1038/nrdp.2015.25
7. FitzGerald JM, Tavakoli H, Lynd LD, Al Efraij K, Sadatsafavi M. The impact of inappropriate use of short acting beta agonists in asthma. Respir Med. 2017;131:135–140. doi:10.1016/j.rmed.2017.08.014
8. Stanford RH, Shah MB, D’Souza AO, Dhamane AD, Schatz M. Short-acting β-agonist use and its ability to predict future asthma-related outcomes. Ann Allergy Asthma Immunol. 2012;109(6):403–407. doi:10.1016/j.anai.2012.08.014
9. Global Initiative for Asthma (GINA). Global strategy for asthma management and prevention; 2019. Available from: https://ginasthma.org/.
10. Global Initiative for Asthma (GINA). Global strategy for asthma management and prevention; 2022. Available from: https://ginasthma.org/.
11. Alith MB, Gazzotti MR, Nascimento OA, Jardim JR. Impact of asthma control on different age groups in five Latin American countries. World Allergy Organ J. 2020;13(4):100113. doi:10.1016/j.waojou.2020.100113
12. Bateman ED, Price DB, Wang HC, et al. Short-acting β2-agonist prescriptions are associated with poor clinical outcomes of asthma: the multi-country, cross-sectional SABINA III study. Eur Respir J. 2022;59(5):2101402.
13. Cabrera CS, Nan C, Lindarck N, Beekman MJ, Arnetorp S, van der Valk RJP. SABINA: global programme to evaluate prescriptions and clinical outcomes related to short-acting β 2 -agonist use in asthma. Eur Respir J. 2020;55(2):1901858.
14. Global Initiative for Asthma (GINA). Global strategy for asthma management and prevention; 2017. Available from: https://ginasthma.org/.
15. Nannini LJ, Luhning S, Rojas RA, et al. Position statement: asthma in Latin America. Is short-acting beta-2 agonist helping or compromising asthma management? J Asthma. 2021;58(8):991–994. doi:10.1080/02770903.2020.1777563
16. Rodrigo GJ, Plaza V, Bellido-Casado J, et al. The study of severe asthma in Latin America and Spain (1994–2004): characteristics of patients hospitalized with acute severe asthma. J Bras Pneumol. 2009;35(7):635–644. doi:10.1590/S1806-37132009000700004
17. National Formulary: resolution 2481 of 2020. Available from: https://www.minsalud.gov.co/Normatividad_Nuevo/Resoluci%C3%B3n%20No.%202481%20de%202020.pdf.
18. Agudelo-Londoño SM, Polyxeni V, Aanestad M. MIPRES grew like a snowball and took us with it: evolution of a health information infrastructure.
19. Ministry of Health and Social Protection. Survey reveals improvements in medicine delivery through Mipres [press release]; 2017.
20. What is the Mipres app. News Release. Ministry of Health and Social Protection; 2017. https://www.minsalud.gov.co/English/Paginas/What-is-The-Mipres-app.aspx.
21. Florez-Tanus A, Parra D, Zakzuk J, Caraballo L, Alvis-Guzman N. Health care costs and resource utilization for different asthma severity stages in Colombia: a claims data analysis. World Allergy Organ J. 2018;11(1):26. doi:10.1186/s40413-018-0205-4
22. Pizzichini MMM, Carvalho-Pinto RM, Cancado JED, et al. 2020 Brazilian Thoracic Association recommendations for the management of asthma. J Bras Pneumol. 2020;46(1):e20190307. doi:10.1590/1806-3713/e20190307
23. Asociación Colombiana de Neumología Pediátrica (ACNP). The national asthma guideline of pediatric asthma; 2013. Available from: http://portal.neumopediatriacolombia.com/wp-content/uploads/2017/03/GPC_Prest_Salu_Asma.pdf.
24. Amin S, Soliman M, McIvor A, Cave A, Cabrera C. Understanding patient perspectives on medication adherence in asthma: a targeted review of qualitative studies. Patient Prefer Adherence. 2020;14:541–551. doi:10.2147/PPA.S234651
25. World Health Organization. Primary health care systems (PRIMASYS) - Case study from Colombia. Available from: https://www.who.int/alliance-hpsr/projects/alliancehpsr_colombiaabridgedprimasys.pdf?ua=1.
26. Price C, Agarwal G, Chan D, et al. Large care gaps in primary care management of asthma: a longitudinal practice audit. BMJ Open. 2019;9(1):e022506. doi:10.1136/bmjopen-2018-022506
27. Abudahish A, Bella H. Adherence of primary care physicians in Aseer region, Saudi Arabia to the National Protocol for the Management of Asthma. East Mediterr Health J. 2010;16(2):171–175. doi:10.26719/2010.16.2.171
28. Grant EN, Moy JN, Turner-Roan K, Daugherty SR, Weiss KB. Asthma care practices, perceptions, and beliefs of Chicago-area primary-care physicians. Chicago Asthma Surveillance Initiative Project Team. Chest. 1999;116(4Suppl 1):145S–154S. doi:10.1378/chest.116.suppl_2.145S
29. Almutawa FN, Al-Mutairy G, Al-Arada N, Kamel MI. Perception of primary care physicians about guidelines of bronchial asthma. Alexandria J Med. 2014;50(1):17–24. doi:10.1016/j.ajme.2013.05.002
30. Hernandez-Rincon EH, Lamus-Lemus F, Carratala-Munuera C, Orozco-Beltran D, Jaramillo-Hoyos CL, Robles-Hernandez G. Building community capacity in leadership for primary health care in Colombia. MEDICC Rev. 2017;19(2–3):65.
31. Gold LS, Montealegre F, Allen-Ramey FC, Jardim J, Sansores R, Sullivan SD. Asthma control and cost in Latin America. Value Health Reg Issues. 2014;5:25–28. doi:10.1016/j.vhri.2014.06.007
32. Neffen H, Moraes F, Viana K, et al. Asthma severity in four countries of Latin America. BMC Pulm Med. 2019;19(1):123. doi:10.1186/s12890-019-0871-1
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.