Back to Journals » Drug Design, Development and Therapy » Volume 20
A Comprehensive Review on the Cardioprotective and Nephroprotective Effects of Semaglutide, and Its Therapeutic Efficacy and Mechanisms in Cardiorenal Syndrome
Authors Ye L, Tang P, Wan H, Zhong X, Chen X ![]() , Liu C, Huang R
, Liu C, Huang R
Received 14 November 2025
Accepted for publication 28 February 2026
Published 24 March 2026 Volume 2026:20 581491
DOI https://doi.org/10.2147/DDDT.S581491
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Solomon Tadesse Zeleke
Lu Ye,1– 3,* Pusong Tang,1– 3,* Haixu Wan,1– 3,* Xing Zhong,2– 4 Xin Chen,2– 4 Changzhao Liu,2– 4 Rui Huang2– 4
1Health Science Center, Hubei Minzu University, Enshi, Hubei, People’s Republic of China; 2Hubei Selenium and Human Health Institute, The Central Hospital of Enshi Tujia and Miao Autonomous Prefecture, Enshi, Hubei, People’s Republic of China; 3Hubei Provincial Key Laboratory of Selenium Resources and Bio applications, Enshi, Hubei, People’s Republic of China; 4Cardiovascular Disease Center, The Central Hospital of Enshi Tujia and Miao Autonomous Prefecture, Enshi, Hubei, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Changzhao Liu, Email [email protected] Rui Huang, Email [email protected]
Abstract: Semaglutide (SEM), a GLP-1 receptor agonist (GLP-1RA), is commonly used to manage blood glucose and weight in type 2 diabetes mellituspatients (T2DM). Research indicates that SEM protects the kidneys and heart by slowing estimated glomerular filtration rate (eGFR) decline, reducing proteinuria, enhancing cardiac outcomes, and lowering cardiovascular risk. These benefits are linked to various mechanisms, including reduced oxidative stress and inflammation, anti-fibrotic effects, modulation of metabolism, inhibition of apoptosis, suppression of ferroptosis, and improved mitochondrial function for energy regulation. However, some studies have also found that SEM may potentially lead to renal impairment or even promote the progression of cardiorenal syndrome (CRS). Due to conflicting results, more animal studies and large-scale clinical trials are needed to understand SEM’s effects on CRS and its side effects, aiding in personalized treatment strategies. This review summarizes the functions and mechanisms of SEM in CRS, and highlights current research limitations and proposed directions for future studies.
Keywords: semaglutide, cardiorenal syndrome, GLP-1RA, cardiovascular outcomes
Introduction
Cardiorenal syndrome (CRS) involves heart or kidney dysfunction causing damage to the other organ. CRS is classified into five subtypes based on its pathological origin and clinical progression: Type 1 is characterized by acute kidney injury (AKI) resulting from acute cardiac dysfunction; Type 2 involves chronic kidney disease (CKD) arising from chronic cardiac dysfunction; Acute cardiac dysfunction induced by AKI defines type 3; Type 4 involves chronic cardiac impairment due to the progression of CKD; and Type 5 is characterized by the concurrent occurrence of cardiac and renal damage due to systemic conditions such as sepsis.1,2 In clinical practice, CRS is associated with high prevalence and mortality rates: a large clinical study found CRS prevalence at 0.40% in the general population, rising to 2.3% in type 2 diabetes patients.3 Research shows 60% of acute decompensated heart failure (HF) patients also have CKD, a major mortality risk. An acute estimated glomerular filtration rate (eGFR) decline occurs in 20–30% of patients,4 straining healthcare systems and emphasizing the need for early detection and intervention. Thus, developing new treatments offering cardiorenal protection with good safety is crucial in cardiovascular and renal disease research.
Semaglutide (SEM), a GLP-1 receptor agonist (GLP-1RA), shows promise for treating CRS due to its protective effects on the heart and kidneys. Numerous clinical studies reveal that SEM enhances cardiac function, reduces HF hospitalizations, and lowers cardiovascular mortality.5,6 Recent large-scale studies have further indicated that SEM also provides distinct renal benefits, effectively slowing the progression of CKD, improving eGFR, and reducing the risk of major cardiovascular events in high-risk populations.7–9 Animal experiments confirm these findings, implying that SEM’s positive effects are linked to its anti-inflammatory and anti-apoptotic actions, metabolic reprogramming, and better mitochondrial efficiency.10,11 Additionally, SEM helps manage type 2 diabetes mellitus (T2DM) by activating the GLP-1 receptor, which boosts insulin secretion and suppresses glucagon, improving glycemic control and reducing metabolic risks linked to cardiorenal diseases.12,13 Simultaneously, SEM is more effective than liraglutide for weight loss,14,15 renal protection in patients with T2DM,16 glycemic control, and cardiovascular outcomes.17 Importantly, SEM can be used regardless of renal function.18 In contrast, drugs like finerenone, angiotensin receptor-neprilysin inhibitors (ARNI), and angiotensin-converting enzyme inhibitors (ACEI), which are often used for cardiorenal protection, are restricted by renal function, especially in advanced kidney disease. Therefore, SEM offers distinct advantages for managing CRS and T2DM.
Recognizing SEM’s cardiorenal benefits, it’s crucial to consider its potential adverse effects, including impaired renal function,19 diabetic retinopathy progression,20 thyroid tumors,21 and psychiatric symptoms like depression,22 which raise concerns about its clinical safety. Thus, this article systematically searched databases, including PubMed, Science Direct, Google Scholar, and Web of Science to review the role and mechanisms of SEM in different subtypes of CRS, as well as its potential adverse effects. The aim is to provide theoretical and practical guidance for the therapeutic application of SEM in CRS.
The Mechanisms Underlying the Cardioprotective and Nephroprotective Effects of SEM
Research indicates that SEM’s cardioprotective benefits stem from enhancing heart structure and function, reducing inflammation, oxidative stress, and fibrosis, and regulating energy metabolism. It also offers renoprotective effects by slowing renal dysfunction, managing tubular and glomerular functions, and decreasing oxidative stress and inflammation. Tables 1 and 2 summarize clinical and basic research on SEM’s cardiorenal protection.
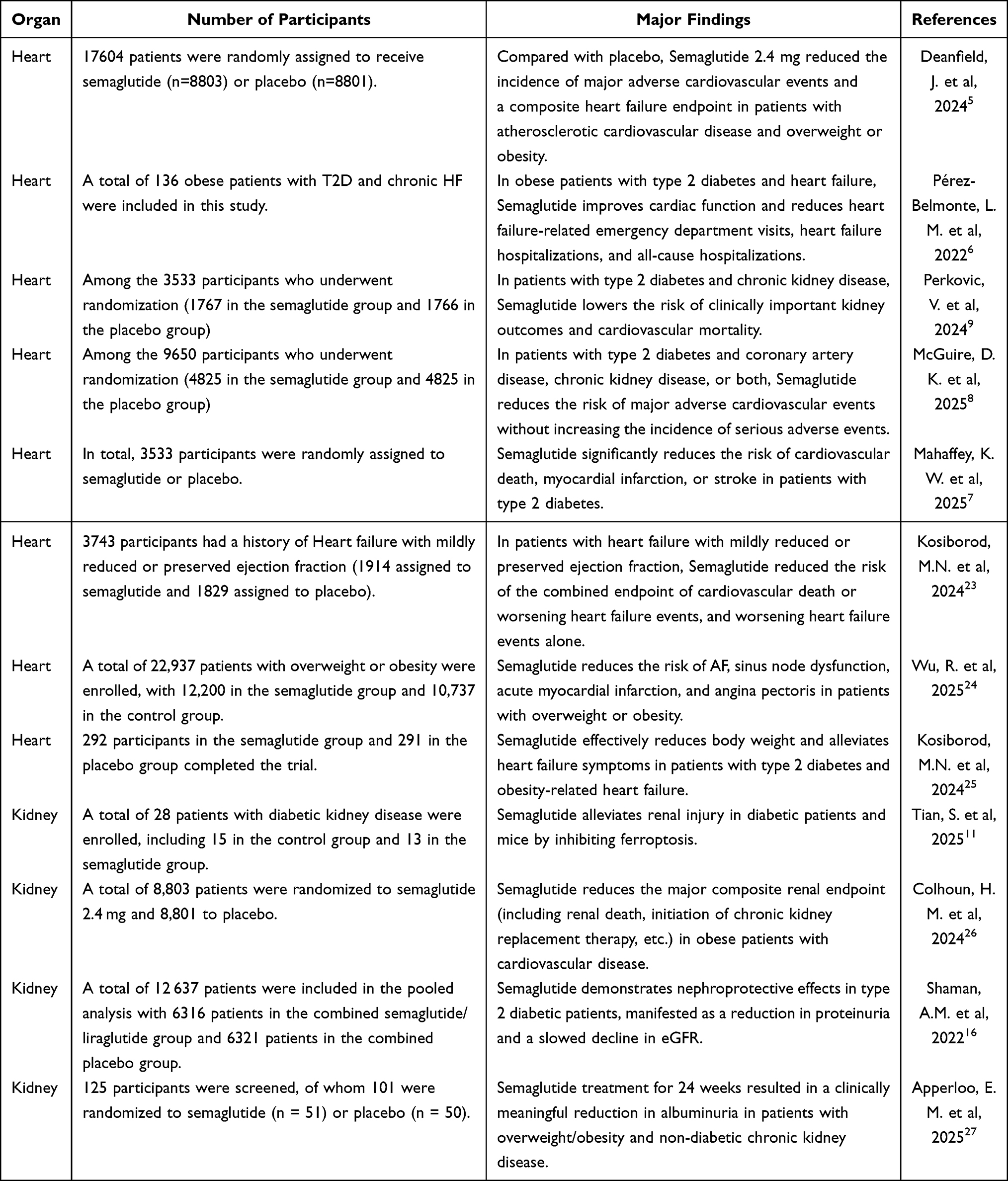 |
Table 1 Clinical Investigations on the Cardiorenal Protective Effects of SEM |
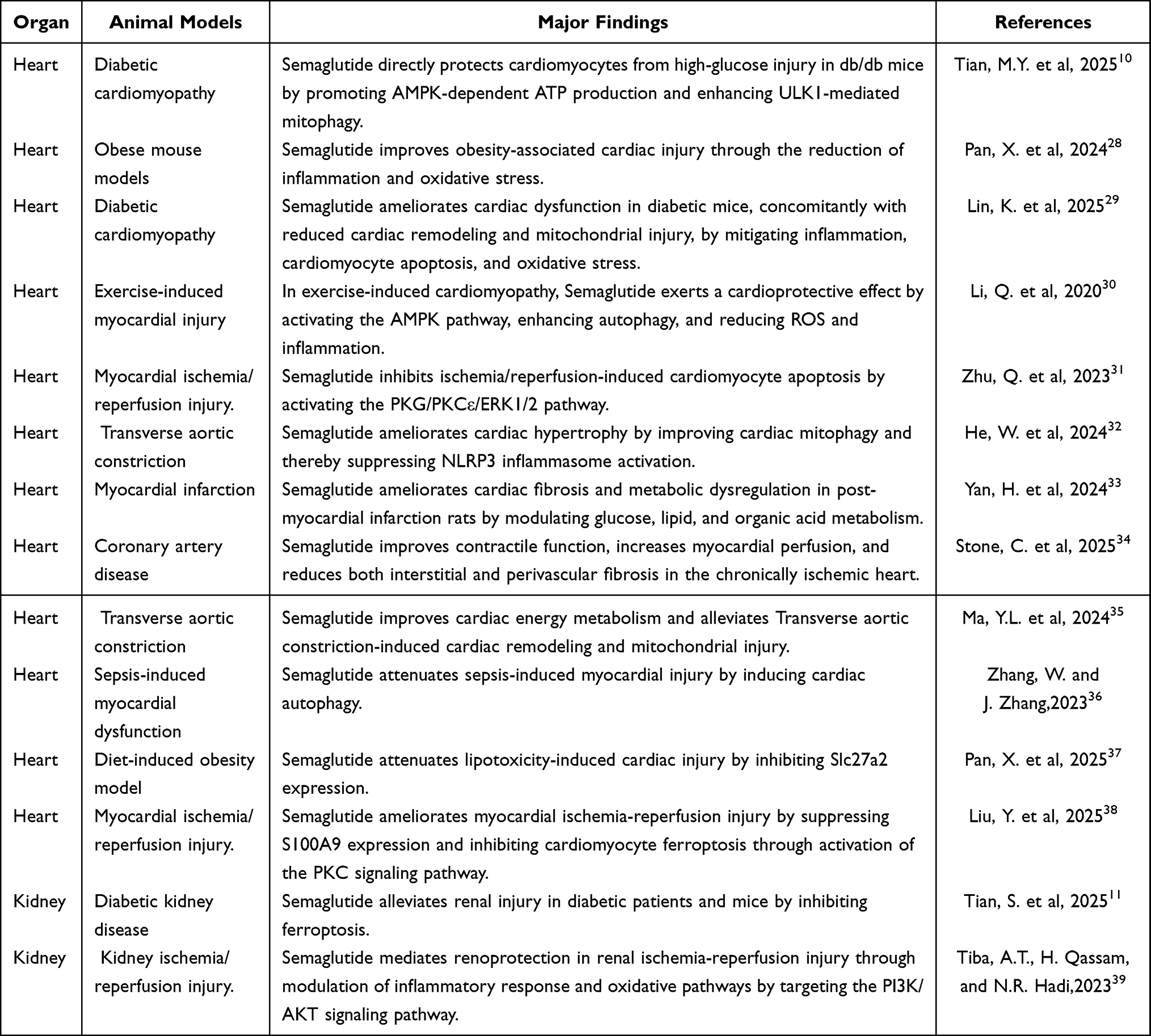 |
Table 2 Basic Research on the Cardiorenal Protective Effects of SEM |
Cardioprotective Mechanisms of SEM
SEM Exerts Cardioprotective Effects Through Anti-Inflammatory and Anti-Oxidative Stress Mechanisms
SEM is extensively used for type 2 diabetes treatment and is gaining attention for its cardiovascular protection benefits. As demonstrated in a previous clinical study, SEM can reduce the risk of cardiovascular death and worsening in patients with HF.23 The specific mechanisms may be related to SEM’s abilities to alleviate inflammatory responses, preserve mitochondrial function, mitigate oxidative stress, and inhibit cellular apoptosis.28–31,40 The NOD-like receptor thermal protein domain-associated protein 3(NLRP3) inflammasome is linked to cardiac injuries like myocardial ischemia and fibrosis.41–43 A study by He et al32 demonstrated that SEM can ameliorate impaired mitophagy induced by transverse aortic constriction (TAC) and suppress NLRP3 inflammasome activation, thereby attenuating cardiac hypertrophy. This finding uncovers the link between SEM and the NLRP3 pathway, emphasizing its strong anti-inflammatory effects. Further validation in a diabetic model demonstrated that SEM treatment attenuates inflammation-induced cardiac injury by upregulating RKIP expression and suppressing the TBK1/NF-κB signaling pathway. These effects were evidenced by improved cardiac function and reduced myocardial injury biomarkers,29 providing a theoretical foundation for expanding the clinical applications of SEM.
A recent clinical trial revealed that SEM improves cardiovascular outcomes by enhancing vascular endothelial function and reducing inflammation, independent of weight loss.44 In an obesity-related cardiac injury model, its anti-inflammatory effect was confirmed. SEM significantly reduced body weight in obese mice while simultaneously downregulating the expression of inflammation- and oxidative stress-related genes (such as S100A8, S100A9, and Cxcl2) in neutrophils, thereby mitigating cardiac injury.28,45 Clinical studies indicate that SEM’s anti-inflammatory properties may prevent atrial fibrosis and alleviate atrial fibrillation symptoms in obese individuals.24 When used with antihypertensive and lipid-lowering drugs, SEM lowered high-sensitivity C-reactive protein by 37.8%.46 These findings support SEM’s potential use in treating heart injuries from inflammation.
SEM Mitigates Myocardial Ischemia-Reperfusion Injury (MIRI)
In addition, SEM has demonstrated protective effects against myocardial injury caused by acute myocardial infarction(AMI), coronary artery perfusion, and ischemia-reperfusion injury.33,38 The mechanisms primarily include alleviating cellular injury, modulating metabolism and vascular function, and inhibiting apoptosis, among others. For example, in animal models of AMI, SEM not only significantly alleviated myocardial cell edema, necrosis, and fibrous tissue hyperplasia but also effectively reduced residual risks post-infarction by modulating energy metabolism, lowering blood glucose, lipid levels, and body weight.33,47 In Yorkshire swine with myocardial ischemia, SEM treatment markedly enhanced the activation and expression of AMPK, AKT, and eNOS, improved vascular diastolic function, and increased coronary perfusion in ischemic areas.34 Previous studies have confirmed that the AMPK/AKT/eNOS signaling pathway plays a critical role in regulating vasodilation and promoting angiogenesis,28,48 which may be one of the key mechanisms through which SEM alleviates myocardial ischemia. Additionally, SEM exerts cardioprotective effects by inhibiting ferroptosis38 and activating the PKG/PKCε/ERK1/2 signaling pathway,31 thereby reducing cellular apoptosis and decreasing infarct size. Meanwhile, subsequent clinical studies have further confirmed that the combined use of GLP-1RA (such as SEM) and SGLT-2 inhibitors after PCI can increase myocardial salvage during the peri-infarction period,49 highlighting its potential clinical application value. Clinical studies indicate that SEM significantly lowers the risk of myocardial infarction and heart failure more than sitagliptin and shows a numerical advantage over tirzepatide in reducing major adverse cardiovascular events (MACE).50
Therefore, based on the current research, we posit that SEM can exert protective effects in myocardial infarction and MIRI. However, the specific role of SEM in the long-term prognosis of AMI warrants further clinical investigation for confirmation.
Evidence for SEM’s Improvement of Cardiometabolic Function
Another significant mechanism through which SEM enhances cardiovascular health is by improving cardiac metabolic function. Myocardial injury is primarily associated with mitochondrial damage and disorders of glucose and lipid metabolism, leading to the accumulation of toxic lipids.51–53 For example, SEM can improve mitochondrial function through the PI3K/AKT/CREB5/NR4A1 axis, thereby alleviating TAC-induced myocardial injury.35 Slc27a2 is associated with HF of metabolic origin.54 Recent studies show that SEM can lower Slc27a2 expression and reduce cardiac injury by enhancing lipid metabolism and reducing lipid buildup in heart cells. While Slc27a2 levels are higher in the blood of obese individuals,37 confirmation in human heart tissue is lacking due to ethical constraints. Despite this, the research strongly supports SEM’s cardioprotective effects in obesity. Studies by Yan et al33 and Stone et al34 further demonstrated, in models of AMI and chronic cardiac injury, respectively, that SEM modulates glucose and lipid metabolism to optimize myocardial energy utilization. Therefore, the mitochondrial protective and metabolic regulatory effects of SEM underscore its potential therapeutic value in both acute and chronic cardiac injury, presenting promising avenues for future cardiovascular disease treatment.
In conclusion, SEM alleviates cardiac injury through various mechanisms, including anti-inflammatory and anti-apoptotic pathways, as well as enhanced vascular function and maintaining mitochondrial structure and function to regulate glucose and lipid metabolism in cardiomyocytes. Early clinical studies indicate its protective role in ischemic myocardium, offering new strategies for myocardial infarction and reperfusion injury treatment. However, most evidence comes from animal studies, with limited clinical research, particularly in acute myocardial injury cases. Thus, high-quality clinical trials are urgently needed to confirm these findings.
Nephroprotective Mechanisms of SEM
The nephroprotective effects of SEM, particularly in patients with CKD, have garnered significant attention in recent years. Studies indicate that long-term administration of SEM can delay the progression of CKD through multiple mechanisms, including attenuating the decline in eGFR, reducing proteinuria, and alleviating renal fibrosis.16,26,27
SEM Alleviates Renal Injury in CRS: Insights from Mechanisms, Preclinical and Clinical Evidence
Despite limited direct investigation, existing data indicate that SEM’s renoprotection may operate through a proposed mechanism that entails mitigating renal fibrosis and inflammation, thereby lowering proteinuria and ultimately resulting in improved renal function—effects that have received preliminary confirmation in clinical research. Initially, SEM was confirmed to have nephroprotective properties in experimental models of CKD. Researchers such as Tian et al55 showed that the GLP-1 RA liraglutide can reduce renal fibrosis in CKD animal models by inhibiting the TGF-β1/Smad3 and ERK1/2 pathways, thus decreasing extracellular matrix secretion and deposition. Based on this mechanism, it is hypothesized that SEM may exert similar effects. Our team’s investigations have shown that in a rodent model of unilateral ureteral obstruction (UUO), SEM improves renal injury and fibrosis by modulating tubulo-glomerular signaling, as indicated by lower creatinine levels and preserved renal structure. In models of renal ischemia-reperfusion injury, SEM reduced the release of inflammatory mediators through activation of the PI3K/Akt signaling pathway, leading to decreased serum creatinine and blood urea nitrogen levels, as well as significant suppression of inflammatory and oxidative stress markers such as TNF-α, IL-6, and F2-isoprostane.39 Thus, it is suggested that SEM’s renoprotection may be linked to its anti-inflammatory and anti-fibrotic properties. A clinical study has shown that, compared with placebo, GLP-1RA can significantly reduce mortality, MACE, and major adverse kidney events (MAKE) in patients with T2DM and AKI.56 The mechanisms may be related to its anti-inflammatory,57 blood pressure, and lipid-regulating effects.58 Given that the most common causes of AKI are sepsis and CRS,56,59 and based on the etiology of AKI as well as the therapeutic effects and mechanisms of GLP-1RA, it is reasonable to speculate that SEM may play an important role in the treatment of AKI and holds great potential in the management of CRS1 and CRS5.
According to Kidney Disease: Improving Global Outcomes (KDIGO) risk stratification analysis, treatment with SEM resulted in a general reduction in KDIGO risk categories. Regardless of baseline CKD severity, patients exhibited a slower decline in eGFR and a reduced rate of increase in urinary albumin-to-creatinine ratio (UACR), indicating significant nephroprotective effects.60 Furthermore, this nephroprotective effect was independent of blood pressure, blood glucose, and UACR levels.61 The SUSTAIN 6 trial was limited to T2DM patients with concomitant cardiovascular disease or risk, excluding a wider spectrum of patients; thus, future research requires finer patient stratification to assess SEM’s renoprotection across distinct subgroups.
Animal and clinical studies indicate that SEM’s nephroprotective benefits go beyond lowering glucose and weight. In AKI and CKD, SEM may reduce proteinuria, inhibit renal fibrosis, and slow renal dysfunction. However, more research is needed on SEM’s role in AKI. Overall, evidence suggests SEM could be a key therapeutic agent for glycemic control and kidney protection.
Mechanisms of SEM in Regulating Tubular and Glomerular Function
The reduction of damage to renal tubules and glomeruli might be another way SEM contributes to mitigating kidney injury. For example, in renal ischemia-reperfusion models, SEM significantly lowers injury scores and improves kidney function39. Furthermore, in chronic conditions like diabetic nephropathy, by inhibiting ferroptosis, SEM ameliorates renal structural damage, including tubular epithelial cell detachment, glomerular hypertrophy, mesangial expansion, and podocyte foot process effacement.11 These effects decrease proteinuria and slow CKD progression, demonstrating SEM’s role in mitigating kidney injury through various mechanisms in both AKI and CKD models. Slc27a2 is associated with structural damage, increased proteinuria, and decreased eGFR in diabetic kidney disease (DKD).62 As mentioned earlier, SEM can alleviate high-lipid-induced cardiac injury by inhibiting Slc27a2.37 Therefore, SEM may potentially reduce renal structural damage and proteinuria levels while maintaining eGFR in DKD through the inhibition of Slc27a2. Consequently, SEM decreases the incidence of end-stage renal disease, postpones the necessity for renal replacement therapy, enhances patients’ quality of life, and alleviates the economic burden on families and healthcare systems associated with long-term dialysis or transplantation.
The Protective Role of SEM in Regulating Purine Metabolism in the Heart and Kidneys
As a GLP-1RA, SEM has been shown to reduce serum uric acid concentrations in diabetic animal models,63 and clinical studies have also observed a certain uric acid-lowering effect.64 Chen et al’s65 metabolomic analysis links SEM’s effects to purine metabolism, specifically adenosine and NAD+. This finding provides a theoretical basis for related basic and clinical research. Further investigations by our team have demonstrated that in UUO-induced CRS4, SEM reduces uric acid production by downregulating xanthine oxidase activity, thereby mitigating cardiac and renal tissue damage. However, a randomized controlled clinical trial conducted by Lennart Tonneijck et al66 showed that GLP-1 Ra did not significantly reduce serum uric acid levels in patients. The discrepancy between this clinical outcome and preclinical findings may be attributed to the relatively normal baseline uric acid levels of the enrolled patients, limited sample size, and short follow-up duration.
Hyperuricemia is a key indicator of purine metabolism disorder and is closely associated with an increased risk of cardiovascular diseases and CKD.67–69 High serum uric acid levels predict all-cause mortality, major cardiovascular events, and heart failure hospitalizations in patients with heart or kidney problems.70,71 Managing uric acid levels is crucial due to its impact on cardiorenal health. The effect of SEM on lowering uric acid is debated, with unclear mechanisms. Future research should focus on detailed investigations and extensive clinical trials to understand SEM’s impact on uric acid metabolism.
SEM May Exert Cardioprotective Effects by Modulating the Gut Microbiota
Dysbiosis of gut microbiota is closely associated with the progression of cardiovascular disease72 and the worsening of CKD.73 GLP-1, an enteric peptide, can serve as a prognostic indicator in patients with AMI complicated by cardiogenic shock and is a strong predictor of adverse outcomes in AMI patients.74 This suggests a potential close relationship between the heart and the gut. Relevant studies have confirmed that SEM alleviates β-cell dysfunction by modulating the gut microbiota, notably by significantly reducing the abundance of Proteobacteria.75 This finding is consistent with our team’s experimental results in a CRS4 model. Furthermore, increased levels of Proteobacteria have been observed in patients with HF,76,77 and the involvement of Proteobacteria in the production of trimethylamine (TMA) and trimethylamine N-oxide (TMAO) is associated with an elevated risk of CKD and cardiovascular diseases.76,78 These findings indicate a link between SEM, gut microbiota, and the heart and kidneys, potentially explaining SEM’s cardiorenal protective effects. However, direct proof of SEM’s role in cardiorenal protection through gut microbiota is absent, necessitating further animal studies as a future research priority.
Role of SEM in Different Subtypes of CRS
Current research indicates that SEM exhibits protective effects across various types of CRS. The mechanisms may involve its anti-inflammatory, anti-fibrotic properties, and inhibition of ferroptosis and apoptosis, suggesting that SEM could be a potential therapeutic agent for different subtypes of CRS. However, some studies have found that SEM may lead to AKI and even exacerbate the progression of CRS. The following section reviews the research progress on SEM in each subtype of CRS.
Research Progress on SEM in Type 1 Cardiorenal Syndrome (CRS1)
CRS1 refers to AKI secondary to acute worsening of cardiac function, with an incidence ranging from 25% to 40%. One clinical study reported an associated mortality rate of 20.5%.79,80 Although current research on SEM in CRS1 remains limited, existing studies indicate its protective effects in both acute cardiac and renal injury. In an animal model of myocardial infarction, four-week SEM treatment ameliorated myocardial fibrosis and significantly improved left ventricular ejection fraction (LVEF) after infarction.33 A clinical study by Filippo Trombara et al81 demonstrated that diabetic patients on long-term GLP-1RA therapy who experienced AMI had lower rates of in-hospital mortality, acute HF, and AKI. The findings indicate a potentially significant role for GLP-1RAs in CRS1. A recent study demonstrated that the addition of GLP-1RA or sodium-glucose co-transporter-2 inhibitors (SGLT2-i) to treatment regimens after percutaneous coronary intervention (PCI) for AMI resulted in enhanced myocardial salvage during the peri-infarction period compared to SGLT2-i monotherapy.49 Despite these findings, the study did not evaluate renal outcomes, leaving the extension of cardioprotective benefits to CRS1 uncertain. While evidence for SEM in treating AKI and CRS1 is limited, GLP-1RAs have been proven to enhance mortality rates and long-term cardiorenal outcomes in T2DM patients with AKI. Given SEM’s protective effects in acute cardiac injury, it shows promise for CRS1 treatment. More clinical and animal studies are needed to investigate its mechanisms and efficacy, offering additional treatment options for CRS1.
Recent Advances in SEM for Type 2 Cardiorenal Syndrome (CRS2)
CRS2 is defined as chronic kidney injury resulting from chronic cardiac dysfunction. Previous studies have indicated that nearly half of all patients with chronic HF exhibit some degree of renal impairment, with approximately one-third experiencing moderate to severe renal dysfunction.82,83 Current research demonstrates that SEM offers significant advantages in the treatment of patients with chronic HF and CKD, including a reduced incidence of HF, improved exercise tolerance in HF patients, decreased proteinuria, and slowed progression of renal impairment. A network meta-analysis showed that type 2 diabetes patients treated with GLP-1RA experienced an 11% reduction in HF hospitalization risk and a 21% decrease in composite kidney outcomes—primarily consisting of renal function deterioration and the need for renal replacement therapy,84 highlighting the therapeutic potential of GLP-1RAs in CRS2.SEM has been shown to attenuate plaque progression in murine models of atherosclerosis through its anti-inflammatory effects, concurrently reducing systemic inflammatory markers and cardiovascular risk.85 In rat models of CRS2, elevated levels of pro-inflammatory cytokines have been observed, which may be closely associated with chronic kidney injury secondary to congestive HF.86 The ability of SEM to mitigate systemic inflammatory responses represents one potential mechanism through which it may ameliorate cardiorenal damage in CRS2. In a randomized controlled trial involving patients with T2DM and ASCVD, SEM reduced the number of adverse kidney outcomes compared with placebo. Although not statistically significant, it significantly slowed the decline in eGFR.87 Although direct evidence for SEM in the treatment of CRS2 is currently lacking, ongoing research into the pathogenesis of CRS2 and the pharmacological effects of SEM is expected to elucidate its efficacy and detailed mechanisms of action in this specific context.
SEM in Type 3 Cardiorenal Syndrome (CRS3): Current Research Perspectives
CRS3 occurs when AKI leads to acute cardiac dysfunction. The incidence of CRS3 is notably increased in critically ill patients. AKI-induced disturbances in water and electrolyte balance, volume overload, and activation of the sympathetic nervous and renin–angiotensin–aldosterone systems contribute to the development of acute HF and malignant arrhythmias, resulting in varying degrees of cardiac injury.88 Recent research indicates that SEM exerts synergistic protective effects on acute cardiac and renal injuries. In models of renal ischemia–reperfusion injury, SEM has been shown to reduce the release of inflammatory mediators, including TNF-α and IL-6, through the PI3K/Akt signaling pathway. This modulation leads to a reduction in renal damage, highlighting SEM’s potential efficacy in the treatment of AKI.39 A clinical study by Pan et al56 reported significant benefits in diabetic patients with AKI treated with GLP-1RAs, including notable reductions in MACE, major adverse kidney events, and all-cause mortality, indicating concurrent cardiorenal protection. The cardiorenal protective effects of SEM may be attributed to its potent anti-inflammatory properties, which mitigate organ damage, and its ability to ameliorate fluid retention caused by acute renal dysfunction.
However, while SEM demonstrates protective potential, some reports have associated its use with adverse renal outcomes such as AKI and acute interstitial nephritis (AIN).89 Case reports have documented elevated serum urea nitrogen and creatinine levels, interstitial inflammation, tubulitis, and tubular injury following SEM use.90 In another case, renal biopsy demonstrated focal segmental glomerulosclerosis (FSGS), AIN with mild interstitial fibrosis and tubular atrophy, variable thickening of the glomerular basement membrane lamina densa, and segmental foot process effacement (25%).19 Therefore, SEM-related AKI has the potential to aggravate the further progression of CRS. However, current evidence suggests that the overall cardiorenal benefits of SEM surpass the risks associated with its rare adverse events. As SEM use increases, monitoring renal function is essential for early detection and management of potential issues, ensuring optimal treatment outcomes. Given the conflicting evidence on SEM use in CRS3, further research is needed to clarify its safety and efficacy, explore its mechanisms in CRS3-related AKI, and confirm its potential for cardiorenal protection.
Advances in SEM for Type 4 Cardiorenal Syndrome (CRS4)
CRS4 describes a condition in which CKD leads to chronic myocardial injury. CKD is recognized as an independent risk factor for cardiovascular disease, not only increasing the incidence of various cardiovascular disorders but also worsening cardiovascular outcomes as eGFR declines.91,92 CKD contributes to the accumulation of uremic toxins and impairs vascular endothelial function through mechanisms such as chronic inflammation and oxidative stress, leading to arterial stiffness, increased cardiac load, and relative cardiac hypoperfusion. These pathological changes further promote coronary artery disease, myocardial infarction, and cardiac remodeling, ultimately resulting in life-threatening complications and reduced quality of life.93,94 Given that SEM has been shown to ameliorate vascular remodeling in various injury models,95–97 it may similarly alleviate CKD-induced endothelial dysfunction and arterial stiffness, thereby mitigating cardiac impairment in CRS4. Current research on the mechanisms by which SEM alleviates CRS4-induced myocardial injury is limited. The anti-inflammatory and nephroprotective effects of SEM are likely among the key mechanisms contributing to its beneficial role in CRS4. During CKD, cardiorenal crosstalk occurs wherein Toll-like receptors, the NLRP3 inflammasome, and other inflammatory pathways are activated, leading to the production of chemokines and subsequent chronic inflammatory damage.98 As previously mentioned, SEM can attenuate pressure overload-induced myocardial hypertrophy mediated by NLRP3 inflammasome activation,32 suggesting that the NLRP3 inflammasome may be one of the targets through which SEM exerts its anti-inflammatory effects and mitigates CRS4-related cardiac injury.
Furthermore, in the CRS4 model induced by UUO, SEM demonstrated efficacy in improving cardiac function, suppressing myocardial apoptosis, and alleviating cardiorenal fibrosis. Separately, a clinical study involving patients with type 2 diabetes and chronic renal failure confirmed that SEM treatment significantly reduced the risk of major kidney outcomes - including renal replacement therapy and death from renal causes - by 24%, and lowered the risk of MACE by 18%.9 Moreover, this cardioprotective effect was independent of CKD severity.7 These findings collectively indicate the therapeutic potential of SEM for CRS4. Currently available cardiorenal protective agents (such as ARNI, SGLT2i, and finerenone) are often limited by renal function. In contrast, SEM can be used in patients with all stages of renal impairment, including those with end-stage uremia, offering broader clinical applicability.18,99 Therefore, SEM holds considerable promise and may provide optimized treatment options for patients with CRS4.
Research Progress on SEM in Type 5 Cardiorenal Syndrome (CRS5)
CRS5 is characterized by concurrent cardiac and renal dysfunction resulting from systemic disorders, such as sepsis, septic shock, diabetes, amyloidosis, and systemic lupus erythematosus. Among these, sepsis is a leading cause of death in CRS5 patients, with an in-hospital mortality rate reaching 100% in severe cases.100–103 The pathogenesis of CRS5 may involve systemic inflammatory responses, cytokine dysregulation,104 and direct cardiac and renal injury mediated by endotoxins and other inflammatory mediators. As demonstrated in a previous clinical study, in patients with diabetes complicated by cardiovascular disease, CKD, or both, treatment with SEM was associated with a lower incidence of new-onset or worsening kidney disease and a significant reduction in cardiovascular mortality.20 Furthermore, SEM also reduces the risk of sepsis, prosthetic joint infections, and hospital readmissions in obese or diabetic patients undergoing joint arthroplasty.89,105 In a mouse model of sepsis-induced myocardial dysfunction (SIMD), SEM treatment significantly lowered levels of inflammatory cytokines and cardiac injury markers compared to untreated controls.36 As the primary cause of CRS5, sepsis can be effectively prevented and its associated cardiac injury mitigated by SEM, offering novel insights for the prevention and treatment of CRS5. While the cornerstone of CRS5 prevention remains the treatment of underlying systemic diseases,2 SEM may mitigate common predisposing factors, thereby reducing the incidence of CRS5 at its source. However, the mechanisms through which SEM may confer cardiorenal protection in established CRS5 remain unclear; elucidating these mechanisms represents an important direction for future research and could reveal further pharmacological applications of SEM.
Adverse Effects and Management of SEM
SEM is generally well-tolerated, with a safety profile comparable to other GLP-1RA. It has demonstrated both safety and efficacy not only in adult patients but also in children with obesity.6,106,107 Despite its favorable overall safety profile, treatment initiation with SEM can lead to certain adverse effects, and longer-term observation is still required to fully characterize its adverse reaction spectrum. Early recognition of these reactions and appropriate management strategies are essential to maximize the clinical benefits of SEM.
Gastrointestinal Symptoms
Gastrointestinal symptoms are among the most common adverse effects of SEM, primarily including nausea, vomiting, and diarrhea during the initial treatment phase. These symptoms are generally transient, occurring mainly in the early stages of treatment and during dose escalation. They are closely related to the administration method and dosage.108 In most cases, these symptoms resolve spontaneously over time. Strategies such as dietary adjustments, gradual dose titration, careful timing of administration, and minimizing concomitant use of medications with known gastrointestinal side effects can help manage these reactions.
Hypoglycemia
Although hypoglycemia is a well-known adverse effect of glucose-lowering medications, the insulinotropic action of SEM is glucose-dependent, and glucagon secretion remains unimpaired under hypoglycemic conditions. Consequently, SEM is associated with a relatively low risk of hypoglycemia.109–111 A meta-analysis further indicated that SEM does not significantly increase the incidence of hypoglycemic events.112 Cases of hypoglycemia in patients using SEM often occur in the context of concomitant use of insulin or other antihyperglycemic agents.109 Studies suggest that the dosage of concomitant glucose-lowering medications may require reduction or adjustment following SEM initiation.6 Regular monitoring of blood glucose levels, patient education regarding recognition of hypoglycemia signs, periodic glycated hemoglobin (HbA1c) testing, and treatment adjustment by specialists based on glycemic profiles are essential to minimize or prevent hypoglycemia.
Cholelithiasis
The formation of gallstones may result from direct effects of SEM on bile secretion, alterations in gallbladder motility, or drug dosage-related factors,106 though the precise mechanisms remain unclear. Studies have indicated a linear relationship between the rate of weight loss and the risk of cholelithiasis development. Specifically, when obese individuals lose weight at a rate of 1.5 kg/week, the risk of gallstone formation increases significantly.113 For patients with a history of cholelithiasis or those possessing high-risk factors, regular imaging follow-up is recommended. Additional measures include controlling the dosage, moderating the rate of weight loss, and considering pharmacological prophylaxis when appropriate. In cases where necessary, laparoscopic cholecystectomy may be performed.
Depression
Two case reports have indicated a potential association between SEM and the induction or recurrence of depression. In both cases, depressive symptoms emerged approximately one month after initiating SEM treatment and resolved following drug discontinuation. One of the patients had a prior history of depression.22 Additionally, the European Medicines Agency reviewed approximately 150 reports of self-harm and suicidal ideation among users of liraglutide or SEM. As a result, patients with a history of depression or suicidal ideation were excluded from subsequent clinical trials of SEM.114 However, a fundamental experiment observed opposite results: in a mouse model of type 2 diabetes-associated depression, SEM not only effectively alleviated depression- and anxiety-like behaviors and enhanced cognitive function but also exhibited neuroprotective effects.115 Due to conflicting findings, further research on SEM’s role in neuropsychiatric disorders is needed. While psychiatric side effects from SEM are rare, caution is recommended when prescribing it to patients with a history of depression or other psychiatric conditions to prevent symptom relapse or worsening.
Thyroid Tumors
A study by Julien Bezin et al suggested that treatment with GLP-1RAs for 1–3 years may increase the risk of thyroid tumors.21 However, a meta-analysis examining the association between SEM and cancer yielded contrasting results.116 Interestingly, a preclinical study even observed an inhibitory effect of SEM on thyroid cancer cells.117 Furthermore, multiple studies have not established a causal relationship between SEM and the development of thyroid tumors.118 Although the association between SEM and thyroid cancer remains controversial, clinical vigilance is still warranted. Physicians are advised to evaluate thyroid function and perform thyroid ultrasonography before initiating SEM therapy to mitigate this potentially serious, though rare, adverse effect.
Retinopathy
The SUSTAIN-6 trial indicated that while SEM improves renal function, it is associated with an increased risk of diabetic retinopathy complications.20 However, a meta-analysis on this topic found no overall correlation between SEM and retinopathy in the unstratified analysis. Yet, subgroup analyses based on age and duration of diabetes revealed a significantly elevated risk of SEM-associated retinopathy in patients with a mean age of≥ 60 years and a diabetes duration of≥ 10 years.119 Additionally, a more rapid reduction in glycated hemoglobin (HbA1c) was correlated with a higher incidence of retinal complications.120 These findings provide valuable clinical guidance: caution is advised when prescribing SEM to elderly patients with long-standing diabetes or pre-existing retinopathy. It is recommended to achieve glycemic control gradually, schedule regular ophthalmologic follow-up, and implement early intervention to mitigate potential vision-threatening outcomes.
Renal Adverse Events
In recent years, the expanding clinical use of SEM—driven by its demonstrated efficacy in weight control and cardiorenal protection—has been accompanied by increased reporting of renal adverse events. Farhana Begum et al identified 2,375 renal adverse events associated with GLP-1RA reported to the U.S. Food and Drug Administration Adverse Event Reporting System (FAERS) over 12 years, including 17 cases of proteinuria and one case of glomerulonephritis specifically linked to SEM.19 Mark M. Smits et al proposed that SEM-related renal impairment may be precipitated by dehydration secondary to drug-induced vomiting, diarrhea, and increased urinary sodium excretion.109 In contrast, Richeek Pradhan and Farhana Begum et al hypothesized that SEM, as a peptide-based therapeutic, may possess immunogenic properties capable of triggering autoimmune-mediated renal injury. Notably, such injury often showed reversibility following drug discontinuation and corticosteroid therapy.19,121 Although SEM-related kidney injury is rare compared to its therapeutic benefits, monitoring for renal issues is crucial in clinical practice. If patients experience severe gastrointestinal side effects, dose reduction or discontinuation should be considered, along with managing symptoms and regularly checking kidney function and urinary protein levels. Future research should aim to clarify the mechanisms and risk factors of SEM-related kidney injury to create targeted prevention strategies.
Future Research Directions for SEM in CRS
As SEM’s cardiorenal protective effects become clearer, key research areas are emerging to better understand its mechanisms, optimize treatments, and improve patient outcomes. Table 3 summarizes current knowledge gaps and future research directions.
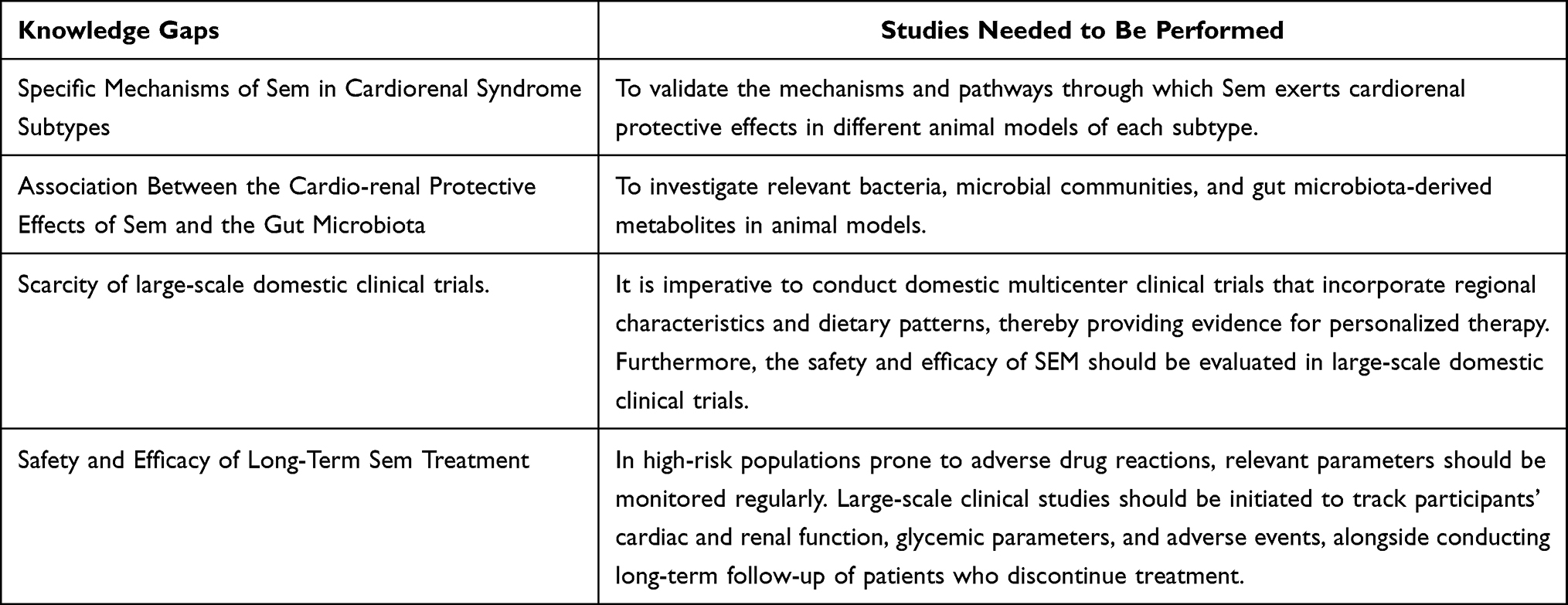 |
Table 3 Knowledge Gaps and Studies Needed to Be Performed |
Mechanistic Exploration, Particularly in Animal Models
Future research should continue to utilize animal models to gain deeper insights into the underlying pharmacological mechanisms of SEM. Studies involving transgenic mice or other suitable animal models could help elucidate the specific pathways through which SEM exerts its cardioprotective and nephroprotective effects. Integrating findings from basic research with clinical data will enable a more comprehensive exploration of how SEM interacts with various metabolic, renal, and cardiac processes in humans, as well as its direct impact on cardiorenal function. Such efforts will provide stronger evidence to support the effective, reliable, and broad application of SEM.
With CRS having five subtypes, it’s crucial to study SEM’s impact on each. Understanding its varied effects on HF types and renal impairments will help clinicians create tailored treatments. Future research should focus on SEM’s mechanisms in each subgroup.
Association Between the Microbiome and SEM
In recent years, the gut microbiota has become a major focus of scientific research. Current studies have shown that microbial-derived metabolites-such as trimethylamine N-oxide (TMAO), N, N, N-trimethyl-5-aminovaleric acid (TMAVA), indoxyl sulfate (IS), indole-3-acetic acid (IAA), and p-cresyl sulfate (PCS)—contribute to cardiac and renal injury by influencing lipid metabolism, inflammation, oxidative stress, and mitochondrial function, thereby promoting reciprocal dysfunction across both organs.122 Whether and how the gut microbiota interacts with SEM remains an important open question for future investigation. A study by Duan et al demonstrated that SEM reduces body weight, fat mass, and insulin resistance in mice by increasing the abundance of Akkermansia, Faecalibaculum, and Allobaculum.123 Furthermore, SEM modulates the relative abundance of gut bacteria and reduces food intake,124 providing compelling evidence for its role in metabolic regulation via the gut microbiome. However, based on current research findings, it remains unclear whether SEM can exert cardiorenal protective effects by modulating the gut microbiota. The outcomes and underlying mechanisms require further elucidation in future animal studies. Given the influential role of the gut microbiota in the onset and progression of various diseases, the interaction between Sem and the gut microbiome will constitute a key research direction for our team.
Potential for Individualized Treatment Approaches
As research advances, opportunities are emerging to develop personalized treatment plans tailored to individual patient profiles. The creation of algorithms incorporating biomarkers, genetic variations, and metabolic characteristics could assist clinicians in optimizing drug selection, dosing, and combination therapies. Such an approach would aim to enhance therapeutic efficacy while minimizing side effects and reducing the financial burden on patients. Additionally, dynamic monitoring of cardiac and renal function, along with metabolic changes, would allow for treatment adjustments—such as dose modification and combination regimens—based on the evolving pathophysiological state during the disease course. This strategy is especially promising for optimizing management in patients with multiple underlying comorbidities.
Importance of Multicenter Clinical Trials
Multicenter clinical trials are essential for validating outcomes across diverse populations and healthcare settings. Such trials enhance the generalizability of findings by including a broader representation of demographic backgrounds, socioeconomic statuses, and comorbid conditions. This inclusivity helps ensure that the results are widely applicable and effective across varied clinical contexts, ultimately promoting greater health equity in the management of CRS. Furthermore, treatment efficacy and optimal dosing of SEM—both as monotherapy and in combination with other drugs—may vary among CRS subtypes, underlying diseases, and concomitant medications. Large-scale, long-term clinical studies are needed to analyze these variables, clarify therapeutic effects, establish evidence-based dosing strategies, and achieve optimal treatment outcomes. Currently, there is a lack of large-scale clinical studies on SEM within China. Most existing clinical evidence is derived from international data. It is therefore imperative to collect and analyze data specific to the Chinese population—considering factors such as dietary habits, genetic predispositions, and environmental exposures—in order to develop more tailored treatment approaches and conclusively establish its therapeutic efficacy for Chinese patients.
Long-Term Safety and Efficacy Monitoring
Long-term follow-up studies are urgently needed to evaluate the sustained efficacy and safety of SEM in the context of CRS. Such studies should monitor cardiovascular health, renal function, and potential long-term adverse effects to comprehensively assess the outcomes of prolonged treatment.
Although SEM shows promise in the treatment of CRS, further research is essential to fully realize its therapeutic potential. By elucidating its mechanisms of action, conducting multicenter clinical trials, and advancing personalized treatment strategies, future studies will not only improve patient outcomes but also refine our understanding of this innovative agent. Such investigations are crucial for exploring SEM’s pharmacological foundations and evaluating its long-term safety and efficacy across different CRS subtypes.
Conclusion
This article reviews SEM’s cardiorenal protective effects and therapeutic strategies for CRS, focusing on mechanisms, clinical evidence, and future prospects. In T2DM, SEM reduces cardiorenal risk factors like blood glucose, blood pressure, and lipids through metabolic regulation. Its anti-inflammatory properties decrease cardiorenal injury and the risk of MACE and MARE. SEM protects the heart by reducing cardiac injury, preserving function, and improving mitochondrial function, energy metabolism, and inhibiting ferroptosis. In kidney disease, SEM prevents inflammatory damage, oxidative stress, fibrosis, and ferroptosis, maintaining renal integrity and slowing disease progression. Figures 1 and 2 illustrate these mechanisms.
 |
Figure 1 The Cardiac Protective Mechanism of SEM. |
 |
Figure 2 The Renal Protective Mechanism of SEM. |
While SEM may offer therapeutic benefits for CRS, its side effects, such as thyroid tumors, kidney issues, depression, and retinopathy progression, must be considered. The risk of SEM-induced AKI needs further clinical validation, and alternative treatments to reverse kidney damage should be actively pursued. Future research should focus on understanding the subtype-specific mechanisms of SEM in different CRS subtypes. Rigorous evaluation of SEM’s efficacy and safety in real-world CRS populations is needed through multicenter trials and long-term studies. Clinically, improved monitoring and personalized risk management are crucial for the effective use of SEM. These steps will help integrate SEM into precision therapy for CRS.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This work was funded by the National Natural Science Foundation of China (No.82160072, No.82360085), the Natural Science Foundation of Hubei Province (No.2023AFD073), and the Science and Technology Support Project of Enshi Prefecture Science and Technology Bureau (No. D20230079, D20230075).
Disclosure
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
References
1. Rangaswami J, Bhalla V, Blair JEA. et al. Cardiorenal syndrome: classification, pathophysiology, diagnosis, and treatment strategies: a scientific statement from the American Heart Association. Circulation. 2019;139(16):e840–18. doi:10.1161/CIR.0000000000000664
2. Ronco C, Haapio M, House AA, et al. Cardiorenal syndrome. J Am Coll Cardiol. 2008;52(19):1527–1539. doi:10.1016/j.jacc.2008.07.051
3. Schechter M, Melzer Cohen C, Yanuv I, et al. Epidemiology of the diabetes-cardio-renal spectrum: a cross-sectional report of 1.4 million adults. Cardiovasc Diabetol. 2022;21(1):104. doi:10.1186/s12933-022-01521-9
4. Norhammar A, Bodegard J, Vanderheyden M, et al. Prevalence, outcomes and costs of a contemporary, multinational population with heart failure. Heart. 2023;109(7):548–556. doi:10.1136/heartjnl-2022-321702
5. Deanfield J, Verma S, Scirica BM, et al. Semaglutide and cardiovascular outcomes in patients with obesity and prevalent heart failure: a prespecified analysis of the SELECT trial. Lancet. 2024;404(10454):773–786. doi:10.1016/S0140-6736(24)01498-3
6. Pérez-Belmonte LM, Sanz-Cánovas J, García de Lucas MD, et al. Efficacy and safety of semaglutide for the management of obese patients with type 2 diabetes and chronic heart failure in real-world clinical practice. Front Endocrinol. 2022;13:851035. doi:10.3389/fendo.2022.851035
7. Mahaffey KW, Tuttle KR, Arici M, et al. Cardiovascular outcomes with semaglutide by severity of chronic kidney disease in type 2 diabetes: the FLOW trial. Eur Heart J. 2025;46(12):1096–1108. doi:10.1093/eurheartj/ehae613
8. McGuire DK, Marx N, Mulvagh SL, et al. Oral semaglutide and cardiovascular outcomes in high-risk type 2 diabetes. N Engl J Med. 2025;392(20):2001–2012. doi:10.1056/NEJMoa2501006
9. Perkovic V, Tuttle KR, Rossing P, et al. Effects of semaglutide on chronic kidney disease in patients with type 2 diabetes. N Engl J Med. 2024;391(2):109–121. doi:10.1056/NEJMoa2403347
10. Tian MY, Yang J-Q, Hu J-C, et al. Semaglutide administration protects cardiomyocytes in db/db mice via energetic improvement and mitochondrial quality control. Acta Pharmacol Sin. 2025;46(5):1250–1261. doi:10.1038/s41401-024-01448-9
11. Tian S, Zhou S, Wu W, et al. GLP-1 receptor agonists alleviate diabetic kidney injury via β-klotho-mediated ferroptosis inhibition. Adv Sci. 2025;12(4):e2409781. doi:10.1002/advs.202409781
12. Aroda VR, Blonde L, Pratley RE. A new era for oral peptides: SNAC and the development of oral semaglutide for the treatment of type 2 diabetes. Rev Endocr Metab Disord. 2022;23(5):979–994. doi:10.1007/s11154-022-09735-8
13. Hall S, Isaacs D, Clements JN. Pharmacokinetics and clinical implications of semaglutide: a new glucagon-like peptide (GLP)-1 receptor agonist. Clin Pharmacokinet. 2018;57(12):1529–1538. doi:10.1007/s40262-018-0668-z
14. Rubino DM, Greenway FL, Khalid U, et al. Effect of weekly subcutaneous semaglutide vs daily liraglutide on body weight in adults with overweight or obesity without diabetes: the STEP 8 randomized clinical trial. JAMA. 2022;327(2):138–150. doi:10.1001/jama.2021.23619
15. Karimi MA, Gholami Chahkand MS, Dadkhah PA, et al. Comparative effectiveness of semaglutide versus liraglutide, dulaglutide or tirzepatide: a systematic review and meta-analysis. Front Pharmacol. 2025;16:1438318. doi:10.3389/fphar.2025.1438318
16. Shaman AM, Bain SC, Bakris GL, et al. Effect of the glucagon-like peptide-1 receptor agonists semaglutide and liraglutide on kidney outcomes in patients with type 2 diabetes: pooled analysis of SUSTAIN 6 and LEADER. Circulation. 2022;145(8):575–585. doi:10.1161/CIRCULATIONAHA.121.055459
17. Peng ZY, Lee Y-H, Ou H-T, et al. Temporal and subgroup disparities in mediation effects on cardiovascular outcomes with liraglutide and semaglutide: a post-hoc analysis of LEADER and SUSTAIN-6 trials. Cardiovasc Diabetol. 2025;24(1):465. doi:10.1186/s12933-025-03007-w
18. Thethi TK, Pratley R, Meier JJ. Efficacy, safety and cardiovascular outcomes of once-daily oral semaglutide in patients with type 2 diabetes: the PIONEER programme. Diabetes Obes Metab. 2020;22(8):1263–1277. doi:10.1111/dom.14054
19. Begum F, Chang K, Kapoor K, et al. Semaglutide-associated kidney injury. Clin Kidney J. 2024;17(9):fae250. doi:10.1093/ckj/sfae250
20. Marso SP, Bain SC, Consoli A, et al. Semaglutide and cardiovascular outcomes in patients with type 2 diabetes. N Engl J Med. 2016;375(19):1834–1844. doi:10.1056/NEJMoa1607141
21. Bezin J, Gouverneur A, Pénichon M, et al. GLP-1 receptor agonists and the risk of thyroid cancer. Diabetes Care. 2023;46(2):384–390. doi:10.2337/dc22-1148
22. Li JR, Cao J, Wei J, et al. Case report: semaglutide-associated depression: a report of two cases. Front Psychiatry. 2023;14:1238353. doi:10.3389/fpsyt.2023.1238353
23. Kosiborod MN, Deanfield J, Pratley R, et al. Semaglutide versus placebo in patients with heart failure and mildly reduced or preserved ejection fraction: a pooled analysis of the SELECT, FLOW, STEP-HFpEF, and STEP-HFpEF DM randomised trials. Lancet. 2024;404(10456):949–961. doi:10.1016/S0140-6736(24)01643-X
24. Wu R, Xing B, Zhou Z, et al. Effect of semaglutide on arrhythmic, major cardiovascular, and renal outcomes in patients with overweight or obesity: a systematic review and meta-analysis. Eur J Med Res. 2025;30(1):835. doi:10.1186/s40001-025-03124-y
25. Kosiborod M N et al. (2024). Semaglutide in Patients with Obesity-Related Heart Failure and Type 2 Diabetes. N Engl J Med, 390(15), 1394–1407. 10.1056/NEJMoa2313917
26. Colhoun HM, Lingvay I, Brown PM, et al. Long-term kidney outcomes of semaglutide in obesity and cardiovascular disease in the SELECT trial. Nat Med. 2024;30(7):2058–2066. doi:10.1038/s41591-024-03015-5
27. Apperloo EM, Gorriz JL, Soler MJ, et al. Semaglutide in patients with overweight or obesity and chronic kidney disease without diabetes: a randomized double-blind placebo-controlled clinical trial. Nat Med. 2025;31(1):278–285. doi:10.1038/s41591-024-03327-6
28. Pan X, Yang L, Wang S, et al. Semaglutide ameliorates obesity-induced cardiac inflammation and oxidative stress mediated via reduction of neutrophil Cxcl2, S100a8, and S100a9 expression. Mol Cell Biochem. 2024;479(5):1133–1147. doi:10.1007/s11010-023-04784-2
29. Lin K, Wang A, Zhai C, et al. Semaglutide protects against diabetes-associated cardiac inflammation via Sirt3-dependent RKIP pathway. Br J Pharmacol. 2025;182(7):1561–1581. doi:10.1111/bph.17327
30. Li Q, Tuo X, Li B, et al. Semaglutide attenuates excessive exercise-induced myocardial injury through inhibiting oxidative stress and inflammation in rats. Life Sci. 2020;250:117531. doi:10.1016/j.lfs.2020.117531
31. Zhu Q, Luo Y, Wen Y, et al. Semaglutide inhibits ischemia/reperfusion-induced cardiomyocyte apoptosis through activating PKG/PKCε/ERK1/2 pathway. Biochem Biophys Res Commun. 2023;647:1–8. doi:10.1016/j.bbrc.2023.01.049
32. He W, Wei J, Liu X, et al. Semaglutide ameliorates pressure overload-induced cardiac hypertrophy by improving cardiac mitophagy to suppress the activation of NLRP3 inflammasome. Sci Rep. 2024;14(1):11824. doi:10.1038/s41598-024-62465-6
33. Yan H, Yao W, Li Y, et al. Cardiometabolic Modulation by Semaglutide Contributes to Cardioprotection in Rats with Myocardial Infarction. Drug Des Devel Ther. 2024;18:5485–5500
34. Stone C, Harris DD, Broadwin M, et al. Semaglutide improves myocardial perfusion and performance in a large animal model of coronary artery disease. Arterioscler Thromb Vasc Biol. 2025;45(2):285–297. doi:10.1161/ATVBAHA.124.321850
35. Ma YL, Kong C-Y, Guo Z, et al. Semaglutide ameliorates cardiac remodeling in male mice by optimizing energy substrate utilization through the Creb5/NR4a1 axis. Nat Commun. 2024;15(1):4757. doi:10.1038/s41467-024-48970-2
36. Zhang W, Zhang J. Semaglutide pretreatment induces cardiac autophagy to reduce myocardial injury in septic mice. Discov Med. 2023;35(178):853–860. doi:10.24976/Discov.Med.202335178.80
37. Pan X, Wang S, Yang X, et al. Semaglutide attenuates lipotoxicity-induced cardiac injury by inhibiting Slc27a2 expression. Chem Biol Interact. 2025;418:111583. doi:10.1016/j.cbi.2025.111583
38. Liu Y, Li Z, Xu X, et al. Semaglutide attenuates myocardial ischemia-reperfusion injury by inhibiting ferroptosis of cardiomyocytes via activation of PKC-S100A9 axis. Front Pharmacol. 2025;16:1529652. doi:10.3389/fphar.2025.1529652
39. Tiba AT, Qassam H, Hadi NR. Semaglutide in renal ischemia-reperfusion injury in mice. J Med Life. 2023;16(2):317–324. doi:10.25122/jml-2022-0291
40. Butler J, Shah SJ, Petrie MC, et al. Semaglutide versus placebo in people with obesity-related heart failure with preserved ejection fraction: a pooled analysis of the STEP-HFpEF and STEP-HFpEF DM randomised trials. Lancet. 2024;403(10437):1635–1648. doi:10.1016/S0140-6736(24)00469-0
41. Duan Y, Li Q, Wu J, et al. A detrimental role of endothelial S1PR2 in cardiac ischemia-reperfusion injury via modulating mitochondrial dysfunction, NLRP3 inflammasome activation, and pyroptosis. Redox Biol. 2024;75:103244. doi:10.1016/j.redox.2024.103244
42. Lv SL, Zeng Z-F, Gan W-Q, et al. Lp-PLA2 inhibition prevents Ang II-induced cardiac inflammation and fibrosis by blocking macrophage NLRP3 inflammasome activation. Acta Pharmacol Sin. 2021;42(12):2016–2032. doi:10.1038/s41401-021-00703-7
43. Zhang J, Huang L, Shi X, et al. Metformin protects against myocardial ischemia-reperfusion injury and cell pyroptosis via AMPK/NLRP3 inflammasome pathway. Aging. 2020;12(23):24270–24287. doi:10.18632/aging.202143
44. Deanfield J, Lincoff AM, Kahn SE, et al. Semaglutide and cardiovascular outcomes by baseline and changes in adiposity measurements: a prespecified analysis of the SELECT trial. Lancet. 2025;406(10516):2257–2268. doi:10.1016/S0140-6736(25)01375-3
45. Gavini MP, Mahmood A, Belenchia AM, et al. Suppression of inflammatory cardiac cytokine network in rats with untreated obesity and pre-diabetes by AT2 receptor agonist NP-6A4. Front Pharmacol. 2021;12:693167. doi:10.3389/fphar.2021.693167
46. Lincoff AM, Brown-Frandsen K, Colhoun HM, et al. Semaglutide and cardiovascular outcomes in obesity without diabetes. N Engl J Med. 2023;389(24):2221–2232. doi:10.1056/NEJMoa2307563
47. Ajmera R, Karim H, Fegan PG, et al. Eligibility for semaglutide 2.4 mg in patients with acute myocardial infarction and overweight or obesity without diabetes: a real-world analysis. Heart Lung Circ. 2025;34(9):977–979. doi:10.1016/j.hlc.2025.01.011
48. Wang S, Miao J, Qu M, et al. Adiponectin modulates the function of endothelial progenitor cells via AMPK/eNOS signaling pathway. Biochem Biophys Res Commun. 2017;493(1):64–70. doi:10.1016/j.bbrc.2017.09.073
49. Marfella R, Prattichizzo F, Sardu C, et al. GLP-1 receptor agonists-SGLT-2 inhibitors combination therapy and cardiovascular events after acute myocardial infarction: an observational study in patients with type 2 diabetes. Cardiovasc Diabetol. 2024;23(1):10. doi:10.1186/s12933-023-02118-6
50. Krüger N, Schneeweiss S, Desai RJ, et al. Cardiovascular outcomes of semaglutide and tirzepatide for patients with type 2 diabetes in clinical practice. Nat Med. 2026;32(1):342–352. doi:10.1038/s41591-025-04102-x
51. Ritterhoff J, Tian R. Metabolic mechanisms in physiological and pathological cardiac hypertrophy: new paradigms and challenges. Nat Rev Cardiol. 2023;20(12):812–829. doi:10.1038/s41569-023-00887-x
52. Da Dalt L, Cabodevilla AG, Goldberg IJ, et al. Cardiac lipid metabolism, mitochondrial function, and heart failure. Cardiovasc Res. 2023;119(10):1905–1914. doi:10.1093/cvr/cvad100
53. Lopaschuk GD, Karwi QG, Tian R, et al. Cardiac energy metabolism in heart failure. Circ Res. 2021;128(10):1487–1513. doi:10.1161/CIRCRESAHA.121.318241
54. Chakraborty P, Niewiadomska M, Farhat K, et al. Effect of Low-level tragus stimulation on cardiac metabolism in heart failure with preserved ejection fraction: a transcriptomics-based analysis. Int J Mol Sci. 2024;25(8):4312. doi:10.3390/ijms25084312
55. Li YK, Ma D-X, Wang Z-M, et al. The glucagon-like peptide-1 (GLP-1) analog liraglutide attenuates renal fibrosis. Pharmacol Res. 2018;131:102–111. doi:10.1016/j.phrs.2018.03.004
56. Pan HC, Chen J-Y, Chen H-Y, et al. GLP-1 receptor agonists’ impact on cardio-renal outcomes and mortality in T2D with acute kidney disease. Nat Commun. 2024;15(1):5912. doi:10.1038/s41467-024-50199-y
57. Shah FA, Mahmud H, Gallego-Martin T, et al. Therapeutic effects of endogenous incretin hormones and exogenous incretin-based medications in sepsis. J Clin Endocrinol Metab. 2019;104(11):5274–5284. doi:10.1210/jc.2019-00296
58. Tommerdahl KL, Kendrick J, Bjornstad P. The role of glucagon-like peptide 1 (GLP-1) receptor agonists in the prevention and treatment of diabetic kidney disease: insights from the AMPLITUDE-O trial. Clin J Am Soc Nephrol. 2022;17(6):905–907. doi:10.2215/CJN.00020122
59. Liu J, Zheng J, Xu Y, et al. The role of mitochondrial dysfunction in sepsis-associated acute kidney injury: a narrative review. Drug Des Devel Ther. 2025;19:9545–9558. doi:10.2147/DDDT.S553838
60. Tuttle KR, Bain SC, Bosch-Traberg H, et al. Effects of once-weekly semaglutide on kidney disease outcomes by KDIGO risk category in the SUSTAIN 6 trial. Kidney Int Rep. 2024;9(7):2006–2015. doi:10.1016/j.ekir.2024.04.028
61. Apperloo EM, Cherney DZI, Kuhlman AB, et al. Effect of semaglutide on kidney function across different levels of baseline HbA1c, blood pressure, body weight and albuminuria in SUSTAIN 6 and PIONEER 6. Nephrol Dial Transplant. 2025;40(2):352–359. doi:10.1093/ndt/gfae150
62. Khan S, Gaivin R, Abramovich C, et al. Fatty acid transport protein-2 regulates glycemic control and diabetic kidney disease progression. JCI Insight. 2020;5(15). doi:10.1172/jci.insight.136845.
63. Lotfy M, Singh J, Rashed H, et al. The effect of glucagon-like peptide-1 in the management of diabetes mellitus: cellular and molecular mechanisms. Cell Tissue Res. 2014;358(2):343–358. doi:10.1007/s00441-014-1959-9
64. Okamoto A, Yokokawa H, Nagamine T, et al. Efficacy and safety of semaglutide in glycemic control, body weight management, lipid profiles and other biomarkers among obese type 2 diabetes patients initiated or switched to semaglutide from other GLP-1 receptor agonists. J Diabetes Metab Disord. 2021;20(2):2121–2128. doi:10.1007/s40200-021-00899-9
65. Chen X, Chen S, Ren Q, et al. Metabolomics provides insights into renoprotective effects of semaglutide in obese mice. Drug Des Devel Ther. 2022;16:3893–3913. doi:10.2147/DDDT.S383537
66. Tonneijck L, Muskiet MHA, Smits MM, et al. Effect of immediate and prolonged GLP-1 receptor agonist administration on uric acid and kidney clearance: post-hoc analyses of four clinical trials. Diabetes Obes Metab. 2018;20(5):1235–1245. doi:10.1111/dom.13223
67. Saito Y, Tanaka A, Node K, et al. Uric acid and cardiovascular disease: a clinical review. J Cardiol. 2021;78(1):51–57. doi:10.1016/j.jjcc.2020.12.013
68. Li N, Li Y, Cui L, et al. Uric acid and risk of incident heart failure in individuals with cardiovascular disease. Nutr Metab Cardiovasc Dis. 2024;34(12):2763–2770. doi:10.1016/j.numecd.2024.09.012
69. Luo Q, Xia X, Li B, et al. Serum uric acid and cardiovascular mortality in chronic kidney disease: a meta-analysis. BMC Nephrol. 2019;20(1):18. doi:10.1186/s12882-018-1143-7
70. Ndrepepa G. Uric acid and cardiovascular disease. Clin Chim Acta. 2018;484:150–163. doi:10.1016/j.cca.2018.05.046
71. Borghi C, Agabiti-Rosei E, Johnson RJ, et al. Hyperuricaemia and gout in cardiovascular, metabolic and kidney disease. Eur J Intern Med. 2020;80:1–11. doi:10.1016/j.ejim.2020.07.006
72. Tang WHW, Li DY, Hazen SL. Dietary metabolism, the gut microbiome, and heart failure. Nat Rev Cardiol. 2019;16(3):137–154. doi:10.1038/s41569-018-0108-7
73. Rysz J, Franczyk B, Ławiński J, et al. The impact of CKD on uremic toxins and gut microbiota. Toxins. 2021;13(4):252. doi:10.3390/toxins13040252
74. Lehrke M, Fuernau G, Jung C, et al. GLP-1 in patients with myocardial infarction complicated by cardiogenic shock-an IABP-SHOCK II-substudy. Clin Res Cardiol. 2024;113(8):1211–1218. doi:10.1007/s00392-023-02366-2
75. Luo Y, Yang S, Zeng H, et al. Both subcutaneous semaglutide and calorie restriction improves pancreatic cell hyperplasia and gut microbiota in high-fat diet-induced obese mice. Nutr Metab. 2025;22(1):95. doi:10.1186/s12986-025-00987-0
76. Cienkowski K, Cienkowska A, Kupczynska K, et al. The role of gut microbiota and its metabolites in patients with heart failure. Biomedicines. 2024;12(4):894. doi:10.3390/biomedicines12040894
77. Huang J, Lin Y, Ding X, et al. Alteration of the gut microbiome in patients with heart failure: a systematic review and meta-analysis. Microb Pathog. 2024;192:106647. doi:10.1016/j.micpath.2024.106647
78. Shoukry AEA, Rahhal A, Constantinou C. The role of the gut microbiota and metabolites in heart failure and possible implications for treatment. Heart Fail Rev. 2025;30(6):1251–1263. doi:10.1007/s10741-025-10546-7
79. Fu K, Hu Y, Zhang H, et al. Insights of worsening renal function in type 1 cardiorenal syndrome: from the pathogenesis, biomarkers to treatment. Front Cardiovasc Med. 2021;8:760152. doi:10.3389/fcvm.2021.760152
80. Wang C, Pei -Y-Y, Ma Y-H, et al. Risk factors for acute kidney injury in patients with acute myocardial infarction. Chin Med J. 2019;132(14):1660–1665. doi:10.1097/CM9.0000000000000293
81. Trombara F, Cosentino N, Bonomi A, et al. Impact of chronic GLP-1 RA and SGLT-2I therapy on in-hospital outcome of diabetic patients with acute myocardial infarction. Cardiovasc Diabetol. 2023;22(1):26. doi:10.1186/s12933-023-01758-y
82. Smith GL, Lichtman JH, Bracken MB, et al. Renal impairment and outcomes in heart failure: systematic review and meta-analysis. J Am Coll Cardiol. 2006;47(10):1987–1996. doi:10.1016/j.jacc.2005.11.084
83. Damman K, Valente MAE, Voors AA, et al. Renal impairment, worsening renal function, and outcome in patients with heart failure: an updated meta-analysis. Eur Heart J. 2014;35(7):455–469. doi:10.1093/eurheartj/eht386
84. Sattar N, Lee MMY, Kristensen SL, et al. Cardiovascular, mortality, and kidney outcomes with GLP-1 receptor agonists in patients with type 2 diabetes: a systematic review and meta-analysis of randomised trials. Lancet Diabetes Endocrinol. 2021;9(10):653–662. doi:10.1016/S2213-8587(21)00203-5
85. Rakipovski G, Rolin B, Nøhr J, et al. The GLP-1 analogs liraglutide and semaglutide reduce atherosclerosis in ApoE(-/-) and LDLr(-/-) mice by a mechanism that includes inflammatory pathways. JACC Basic Transl Sci. 2018;3(6):844–857. doi:10.1016/j.jacbts.2018.09.004
86. Angelini A, Castellani C, Virzì GM, et al. The role of congestion in cardiorenal syndrome type 2: new pathophysiological insights into an experimental model of heart failure. Cardiorenal Med. 2015;6(1):61–72. doi:10.1159/000440775
87. Mann JFE, Marx N, Deanfield JE, et al. Impact of oral semaglutide on kidney outcomes in people with type 2 diabetes: results from the SOUL randomized trial. Diabetes Care. 2026;49(2):257–265. doi:10.2337/dc25-1080
88. Ronco C, McCullough PA, Anker SD, et al. Cardiorenal Syndromes: An Executive Summary From the Consensus Conference of the Acute Dialysis Quality Initiative (ADQI). Contrib Nephrol; 2010;165:54–67
89. Magruder ML, Yao VJH, Rodriguez AN, et al. Does semaglutide use decrease complications and costs following total knee arthroplasty? J Arthroplasty. 2023;38(11):2311–2315.e1. doi:10.1016/j.arth.2023.05.071
90. Borkum M, Lau W, Blanco P, et al. Semaglutide-associated acute interstitial nephritis: a case report. Kidney Med. 2022;4(12):100561. doi:10.1016/j.xkme.2022.100561
91. Uduman J. Epidemiology of cardiorenal syndrome. Adv Chronic Kidney Dis. 2018;25(5):391–399. doi:10.1053/j.ackd.2018.08.009
92. Shen Y, Peng X, Ji H, et al. Dapagliflozin protects heart function against type-4 cardiorenal syndrome through activation of PKM2/PP1/FUNDC1-dependent mitophagy. Int J Biol Macromol. 2023;250:126116. doi:10.1016/j.ijbiomac.2023.126116
93. Zanoli L, Lentini P, Briet M, et al. Arterial stiffness in the heart disease of CKD. J Am Soc Nephrol. 2019;30(6):918–928. doi:10.1681/ASN.2019020117
94. Sessa C, Granata A, Gaudio A, et al. Vascular dysfunction in cardiorenal syndrome type 4. G Ital Nefrol. 2020;37(1).
95. Jensen DM, Skovsted GF, Bonde MFB, et al. Semaglutide treatment attenuates vessel remodelling in ApoE-/- mice following vascular injury and blood flow perturbation. Atheroscler Plus. 2022;49:32–41. doi:10.1016/j.athplu.2022.05.004
96. Mouhammad ZA, Rombaut A, Bermúdez MYG, et al. Systemic semaglutide provides a mild vasoprotective and antineuroinflammatory effect in a rat model of ocular hypertensive glaucoma. Mol Brain. 2025;18(1):54. doi:10.1186/s13041-025-01224-8
97. Bonaca MP, Catarig A-M, Houlind K, et al. Semaglutide and walking capacity in people with symptomatic peripheral artery disease and type 2 diabetes (STRIDE): a phase 3b, double-blind, randomised, placebo-controlled trial. Lancet. 2025;405(10489):1580–1593. doi:10.1016/S0140-6736(25)00509-4
98. Amador-Martínez I, Aparicio-Trejo OE, Bernabe-Yepes B, et al. Mitochondrial impairment: a link for inflammatory responses activation in the cardiorenal syndrome type 4. Int J Mol Sci. 2023;24(21). doi:10.3390/ijms242115875.
99. Mosenzon O, Blicher TM, Rosenlund S, et al. Efficacy and safety of oral semaglutide in patients with type 2 diabetes and moderate renal impairment (PIONEER 5): a placebo-controlled, randomised, phase 3a trial. Lancet Diabetes Endocrinol. 2019;7(7):515–527. doi:10.1016/S2213-8587(19)30192-5
100. Shah HR, Singh NP, Aggarwal NP, et al. Cardiorenal syndrome: clinical outcome study. J Assoc Physicians India. 2016;64(12):41–46.
101. Ronco C, McCullough P, Anker SD, et al. Cardio-renal syndromes: report from the consensus conference of the acute dialysis quality initiative. Eur Heart J. 2010;31(6):703–711. doi:10.1093/eurheartj/ehp507
102. Clementi A, Virzì GM, Brocca A, et al. The role of endotoxin in the setting of cardiorenal syndrome type 5. Cardiorenal Med. 2017;7(4):276–283. doi:10.1159/000475846
103. Virzì GM, Clementi A, Brocca A, et al. Cardiorenal syndrome type 5 in sepsis: role of endotoxin in cell death pathways and inflammation. Kidney Blood Press Res. 2016;41(6):1008–1015. doi:10.1159/000452602
104. Brocca A, Virzì GM, Pasqualin C, et al. Cardiorenal syndrome type 5: in vitro cytotoxicity effects on renal tubular cells and inflammatory profile. Anal Cell Pathol. 2015;2015:469461. doi:10.1155/2015/469461
105. Magruder ML, Miskiewicz MJ, Rodriguez AN, et al. Semaglutide use prior to total hip arthroplasty results in fewer postoperative prosthetic joint infections and readmissions. J Arthroplasty. 2024;39(3):716–720. doi:10.1016/j.arth.2023.12.023
106. Song CE, Wang Y, Dai XM, Wu HY. Efficacy and safety of semaglutide in weight loss of non-diabetic people. Endocr Metab Immune Disord Drug Targets, 2024;25.
107. van Boxel EJ, Rahman S, Lai K, et al. Semaglutide treatment for children with obesity: an observational study. Arch Dis Child. 2024;109(10):822–825. doi:10.1136/archdischild-2023-326687
108. Cleto AS, Schirlo JM, Beltrame M, et al. Semaglutide effects on safety and cardiovascular outcomes in patients with overweight or obesity: a systematic review and meta-analysis. Int J Obes. 2025;49(1):21–30. doi:10.1038/s41366-024-01646-9
109. Smits MM, Van Raalte DH. Safety of semaglutide. Front Endocrinol. 2021;12:645563. doi:10.3389/fendo.2021.645563
110. Meier JJ. Efficacy of semaglutide in a subcutaneous and an oral formulation. Front Endocrinol. 2021;12:645617. doi:10.3389/fendo.2021.645617
111. Nauck MA, Quast DR, Wefers J, et al. GLP-1 receptor agonists in the treatment of type 2 diabetes - state-of-the-art. Mol Metab. 2021;46:101102. doi:10.1016/j.molmet.2020.101102
112. Andreadis P, Karagiannis T, Malandris K, et al. Semaglutide for type 2 diabetes mellitus: a systematic review and meta-analysis. Diabetes Obes Metab. 2018;20(9):2255–2263. doi:10.1111/dom.13361
113. Weinsier RL, Wilson LJ, Lee J. Medically safe rate of weight loss for the treatment of obesity: a guideline based on risk of gallstone formation. Am J Med. 1995;98(2):115–117. doi:10.1016/S0002-9343(99)80394-5
114. Ruder K. As semaglutide’s popularity soars, rare but serious adverse effects are emerging. JAMA. 2023;330(22):2140–2142. doi:10.1001/jama.2023.16620
115. de Paiva IHR, da Silva RS, Mendonça IP, et al. Semaglutide attenuates anxious and depressive-like behaviors and reverses the cognitive impairment in a type 2 diabetes mellitus mouse model via the microbiota-gut-brain axis. J Neuroimmune Pharmacol. 2024;19(1):36. doi:10.1007/s11481-024-10142-w
116. Nagendra L, BG H, Sharma M, et al. Semaglutide and cancer: a systematic review and meta-analysis. Diabetes Metab Syndr. 2023;17(9):102834. doi:10.1016/j.dsx.2023.102834
117. Wang L, Zhang L, Ma R, et al. Semaglutide reprograms macrophages via the GLP-1R/PPARG/ACSL1 pathway to suppress papillary thyroid carcinoma growth. J Clin Endocrinol Metab. 2025;110(10):2777–2789. doi:10.1210/clinem/dgaf053
118. Feier CVI, Vonica R, Faur A, et al. Assessment of thyroid carcinogenic risk and safety profile of GLP1-RA semaglutide (Ozempic) therapy for diabetes mellitus and obesity: a systematic literature review. Int J Mol Sci. 2024;25(8):4346. doi:10.3390/ijms25084346
119. Wang F, Mao Y, Wang H, et al. Semaglutide and diabetic retinopathy risk in patients with type 2 diabetes mellitus: a meta-analysis of randomized controlled trials. Clin Drug Investig. 2022;42(1):17–28. doi:10.1007/s40261-021-01110-w
120. Vilsbøll T, Bain SC, Leiter LA, et al. Semaglutide, reduction in glycated haemoglobin and the risk of diabetic retinopathy. Diabetes Obes Metab. 2018;20(4):889–897. doi:10.1111/dom.13172
121. Pradhan R, Patorno E, Tesfaye H, et al. Glucagon-Like peptide 1 receptor agonists and risk of anaphylactic reaction among patients with type 2 diabetes: a multisite population-based cohort study. Am J Epidemiol. 2022;191(8):1352–1367. doi:10.1093/aje/kwac021
122. Lai Y, Zhu Y, Zhang X, et al. Gut microbiota-derived metabolites: potential targets for cardiorenal syndrome. Pharmacol Res. 2025;214:107672. doi:10.1016/j.phrs.2025.107672
123. Duan X, Zhang L, Liao Y, et al. Semaglutide alleviates gut microbiota dysbiosis induced by a high-fat diet. Eur J Pharmacol. 2024;969:176440. doi:10.1016/j.ejphar.2024.176440
124. Da Silva RS, de Paiva IHR, Mendonça IP, et al. Anorexigenic and anti-inflammatory signaling pathways of semaglutide via the microbiota-gut--brain axis in obese mice. Inflammopharmacology. 2025;33(2):845–864. doi:10.1007/s10787-024-01603-y
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.