Back to Journals » International Journal of Chronic Obstructive Pulmonary Disease » Volume 11 » Issue 1
A comparison of synchronized intermittent mandatory ventilation and pressure-regulated volume control ventilation in elderly patients with acute exacerbations of COPD and respiratory failure
Authors Chang SC, Shi JD, Fu CP, Wu X, Li S
Received 26 October 2015
Accepted for publication 7 March 2016
Published 17 May 2016 Volume 2016:11(1) Pages 1023—1029
DOI https://doi.org/10.2147/COPD.S99156
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Prof. Dr. Richard Russell
Suchi Chang,1 Jindong Shi,2 Cuiping Fu,1 Xu Wu,1 Shanqun Li1
1Department of Respiratory Medicine, Zhongshan Hospital, Fudan University, Shanghai, 2Department of Respiratory Medicine, The Fifth People’s Hospital of Shanghai, Fudan University, Shanghai, People’s Republic of China
Background: COPD is the third leading cause of death worldwide. Acute exacerbations of COPD may cause respiratory failure, requiring intensive care unit admission and mechanical ventilation. Intensive care unit patients with acute exacerbations of COPD requiring mechanical ventilation have higher mortality rates than other hospitalized patients. Although mechanical ventilation is the most effective intervention for these conditions, invasive ventilation techniques have yielded variable effects.
Objective: We evaluated pressure-regulated volume control (PRVC) ventilation treatment efficacy and preventive effects on pulmonary barotrauma in elderly COPD patients with respiratory failure.
Patients and methods: Thirty-nine intubated patients were divided into experimental and control groups and treated with the PRVC and synchronized intermittent mandatory ventilation – volume control methods, respectively. Vital signs, respiratory mechanics, and arterial blood gas analyses were monitored for 2–4 hours and 48 hours.
Results: Both groups showed rapidly improved pH, partial pressure of oxygen (PaO2), and PaO2 per fraction of inspired O2 levels and lower partial pressure of carbon dioxide (PaCO2) levels. The pH and PaCO2 levels at 2–4 hours were lower and higher, respectively, in the test group than those in the control group (P<0.05 for both); after 48 hours, blood gas analyses showed no statistical difference in any marker (P>0.05). Vital signs during 2–4 hours and 48 hours of treatment showed no statistical difference in either group (P>0.05). The level of peak inspiratory pressure in the experimental group after mechanical ventilation for 2–4 hours and 48 hours was significantly lower than that in the control group (P<0.05), while other variables were not significantly different between groups (P>0.05).
Conclusion: Among elderly COPD patients with respiratory failure, application of PRVC resulted in rapid improvement in arterial blood gas analyses while maintaining a low peak inspiratory pressure. PRVC can reduce pulmonary barotrauma risk, making it a safer protective ventilation mode than synchronized intermittent mandatory ventilation – volume control.
Keywords: COPD, respiratory failure, invasive mechanical ventilation, pressure-regulated volume control, synchronized intermittent mandatory ventilation
Introduction
The clinical manifestations of acute exacerbations of COPD (AECOPD) with hypercapnic respiratory failure include a partial pressure of carbon dioxide (PaCO2) in the arterial blood >45 mmHg and pH <7.35.1 Ventilatory support is one of the main interventions for AECOPD with respiratory failure in the intensive care unit. It is indicated when patients do not tolerate or fail to respond to treatment, or have contraindications to noninvasive ventilation support.1–3
Synchronized intermittent mandatory ventilation (SIMV) is a ventilation mode commonly used in the treatment of COPD respiratory failure. Many clinical trials have demonstrated that this ventilation mode can effectively improve hypoxemia, mitigate hypercapnia, and correct excessive respiratory acidosis. However, when SIMV without pressure support is applied in elderly patients with lung infection and bronchial and lung damage, barotrauma can be caused by increased peak pressure from increased airway resistance, resulting from their weakened systematic functions and multiple preexisting diseases.4,5 Synchronized intermittent mandatory ventilation – volume control (SIMV-VC), another volume control (VC) form of ventilation, can reduce barotrauma.6
Pressure-regulated volume control (PRVC) is a ventilation mode that is timed and pressure controlled with continuous airflow and continuous capacity control. It combines the advantages of both VC and pressure control (PC). While ensuring an improvement in ventilation, it can simultaneously lower inspiratory positive airway pressure and peak airway pressure, thereby reducing the incidence of barotrauma.7 Our aim was to evaluate the effects of treating respiratory failure by comparing the PRVC ventilation mode to the SIMV mode in elderly COPD patients with respiratory failure.
Patients and methods
We conducted a prospective, double-blind, randomized controlled trial. The participants were randomly assigned to the “control” SIMV or “experimental” PRVC mode groups. Randomization was performed by using sealed envelopes containing a piece of paper with either “A” (for SIMV) or “B” (for PRVC), which were opened by the physician in charge at the beginning of the trial. The study was approved by the ethics committee of The Fifth People’s Hospital of Shanghai. Written informed consent was obtained from all the individual participants included in the study and their family members.
Patients
Patients selected for the study were those older than 80 years from February 2007 to February 2010 and treated on the respiratory intensive care unit of The Fifth People’s Hospital of Shanghai. A total of 42 cases, including 24 men and 18 women, aged 80–102 years (average, 86.4±6.0 years), who matched the COPD diagnosis and treatment standards of the 2007 Chinese Medical Association for respiratory diseases8 and type II respiratory failure diagnostic criteria with a blood oxygen partial pressure (PaO2) <60 mmHg and blood carbon dioxide partial pressure (PaCO2) >50 mmHg were included. The COPD patients recruited responded poorly to noninvasive ventilation. All cases were severe enough to warrant immediate implementation of endotracheal intubation and mechanical ventilation and met the criteria for intubation at the time of presentation.
All patients had a variety of comorbidities, with up to four kinds of underlying diseases, mainly including high blood pressure, coronary heart disease, cerebral infarction, diabetes, arthritis, and fractures. We screened 864 patients, and 42 patients were enrolled in our study. They were randomly divided into the experimental group (21 cases) and the control group (21 cases). We excluded patients with serious heart, liver, or kidney failure; severe arrhythmia or acute myocardial ischemia; pneumothorax or mediastinal emphysema; intracranial hypertension; severe multiple organs dysfunction; end-stage malignant carcinoma; and immunosuppression conditions. We also excluded three patients in the control group: one because of death caused by pneumothorax and two because of withdrawal.
Thirty-nine study subjects with AECOPD and respiratory failure were finally recruited, as shown in Figure 1. The differences between the sex ratios; average ages; course of the diseases; Acute Physiology and Chronic Health Evaluation II scores; pH, PaCO2, PaO2, and bicarbonate (HCO3−) levels; and respiratory rates (f) of the two groups were not statistically significant (P>0.05), as shown in Table 1.
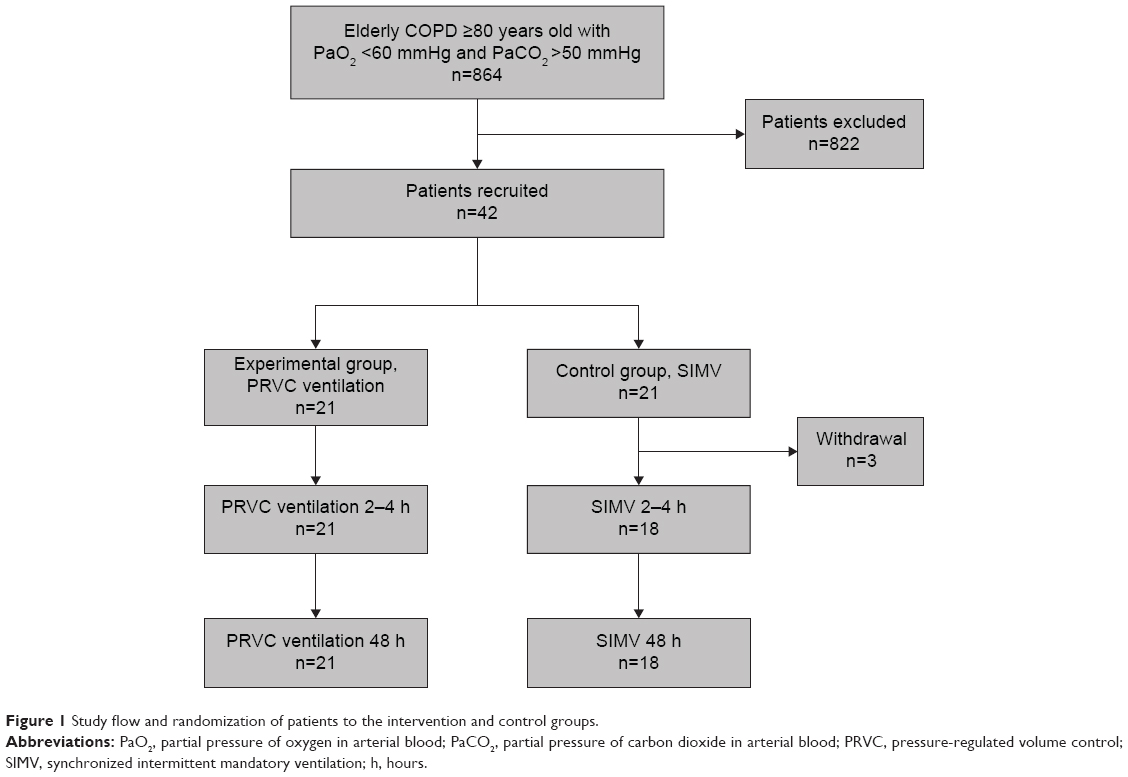 | Figure 1 Study flow and randomization of patients to the intervention and control groups. |
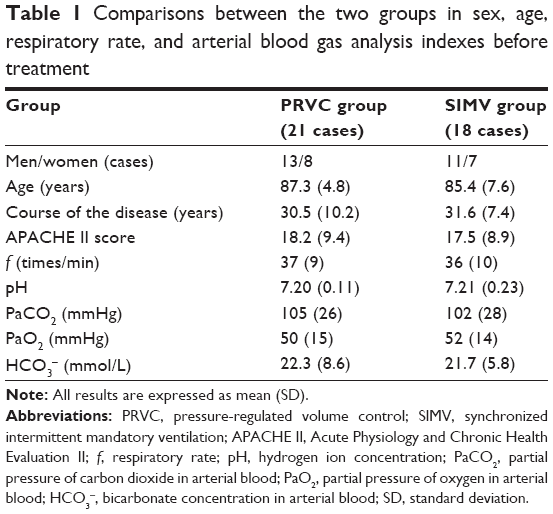 | Table 1 Comparisons between the two groups in sex, age, respiratory rate, and arterial blood gas analysis indexes before treatment |
Methods
General management
All patients admitted to the respiratory intensive care unit were managed with electrocardiographic monitoring, blood pressure monitoring, and transcutaneous pulse oxygen saturation (SpO2) monitoring, followed by zealous treatment for infection, bronchospasm, and mucolysis. A complete history was obtained, and physical examination was performed. Maintenance of water and electrolyte balances, optimal nutritional support, and airway humidification were also administered promptly.
Mechanical ventilation
All patients who were treated with the above general management therapy because of their critical condition were simultaneously in need of oral (nasal) intubation using a Maquet Servo-i (Maquet Medical Equipment, Shanghai, People’s Republic of China) ventilator for mechanical ventilation.
The experimental group was treated with the PRVC method, while the control group was treated with SIMV-VC mode without pressure support. The preset values for both groups were as follows: a tidal volume (VT) of 6–10 mL/kg, respiratory frequency (f) of 12–16 times/min, inspiratory time (Tinsp) of 1.0–1.3 seconds, inhaled gas oxygen concentration (fraction of inspiration O2 [FiO2]) of 0.3–0.6, and positive end-expiratory pressure of 3–5 cmH2O.
Sedative use
For patients who showed significant irritation and could not cooperate with the ventilator and for whom assisted breathing by bag valve mask proved ineffectual during the intubation and mechanical ventilation process, a small amount of short-term intravenous sedatives can guarantee an effective collaboration between them and the ventilator. The use of sedation or analgesia may help to reduce a patient’s respiratory rate and dyspnea. Moreover, they may improve patient comfort and reduce breathing work during mechanical ventilation. However, the long-term, heavy use of sedatives should be avoided.9
Observation index
The vital signs, including heart rate, systolic blood pressure, diastolic blood pressure, and respiratory rate, and respiratory mechanics, including peak inspiratory pressure (PIP), mean airway pressure, pulmonary dynamic compliance, ventilator for power, VT, and minute ventilation (MV), of the two groups were observed during mechanical ventilation treatment for 2–4 hours and 48 hours. Simultaneously, the pH, PaCO2, PaO2, and HCO3− levels of arterial blood were determined (GEM Premier 3000 blood gas analyzer; GEM Premier 3000, Shanghai, People’s Republic of China), and then, the oxygenation index (PaO2/FiO2) was calculated.
Statistical analysis
Using the Statistical Program for Social Sciences Version 17.0 software (SPSS Inc., Chicago, IL, USA), all data were expressed as mean ± standard deviation (SD) by using the independent samples t-test. A P-value of ≤0.05 was considered to be statistically significant.
Results
The changes in vital signs, blood gas analysis, and indexes of breathing mechanics 2–4 hours and 48 hours after treatment are shown in Table 2. The pH, PaCO2, and PIP of the experimental group showed significant improvements compared with those of the control group 2–4 hours after treatment, as shown in Figures 2–4. However, only the PIP of the experimental group significantly improved 48 hours after treatment (P<0.05).
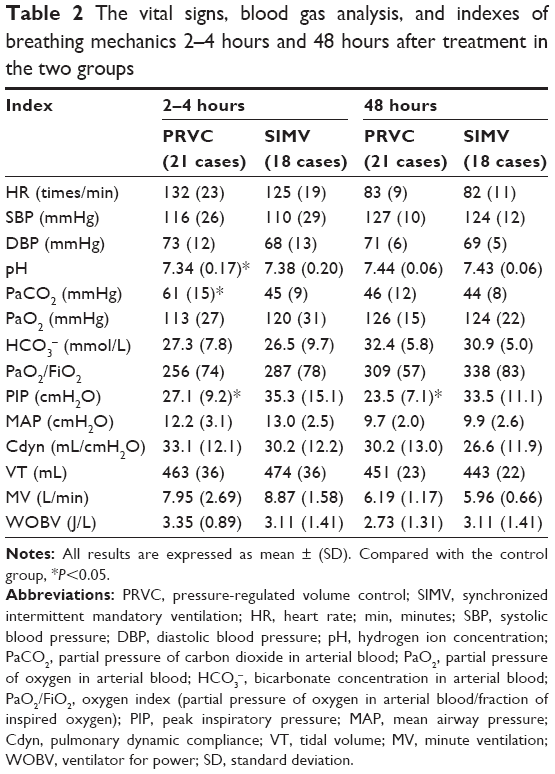 | Table 2 The vital signs, blood gas analysis, and indexes of breathing mechanics 2–4 hours and 48 hours after treatment in the two groups |
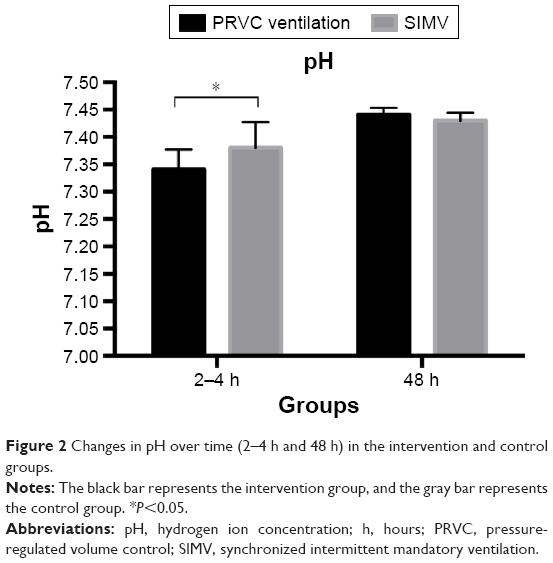 | Figure 2 Changes in pH over time (2–4 h and 48 h) in the intervention and control groups. |
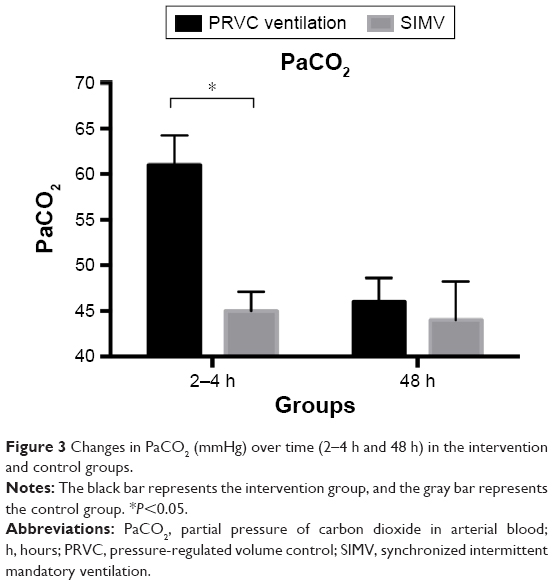 | Figure 3 Changes in PaCO2 (mmHg) over time (2–4 h and 48 h) in the intervention and control groups. |
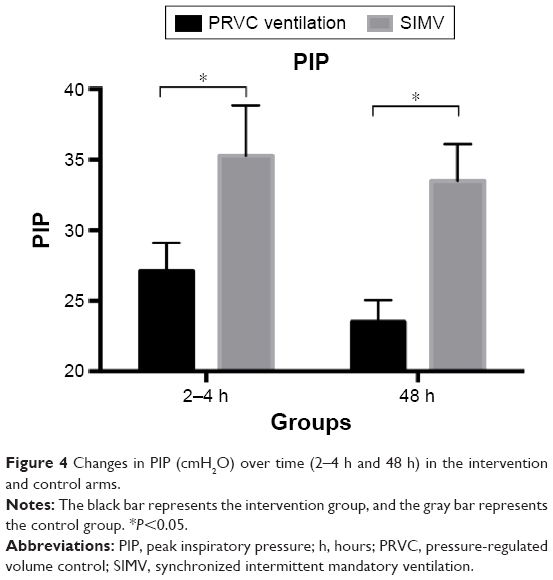 | Figure 4 Changes in PIP (cmH2O) over time (2–4 h and 48 h) in the intervention and control arms. |
Complications
During mechanical ventilation, hyperinflation should be prevented while improving oxygenation and reducing the work of breathing. Hyperinflation can induce barotrauma and further injury to the lungs, which may prolong the duration of mechanical ventilation.10 Barotrauma is a type of lung damage caused by the application of high airway pressure.11 The most common form of barotrauma is pneumothorax, which can be detected on a chest radiograph when the lateral lung regions collapse.12 Other forms of barotrauma include gaseous embolism and pneumomediastinum, which may extend to the neck, face, trunk, and scrotum.13 In our study, there was one case of pneumothorax in the control group and no case of barotrauma in the treatment group.
Discussion
Since elderly patients often suffer from multiple organ dysfunction, malnutrition, and many other complications during AECOPD, they have a higher risk for asphyxia. In addition, in patients with severe pulmonary infection, the possibilities of respiratory failure and pulmonary encephalopathy increase.
As a main method for rescuing patients with respiratory failure, noninvasive mechanical ventilation is always difficult to implement in elderly patients with COPD because of the increased occurrence of tooth loss, facial marasmus due to severe malnutrition, and subsequent facial anomalies or partial defects leading to poor sealing of the mask.14 Therefore, establishing an artificial airway with assistive ventilation needs to be prioritized to make the most of an early treatment and diagnostic plan and reduce the mortality rate in these patients.15
The viewpoints of articles on mechanical ventilation for severely obstructed patients are controversial. Some authors prefer pressure-controlled ventilation,16–18 some favor volume-controlled ventilation,19 and others suggest that both VC and PC have similar outcomes in COPD patients with acute respiratory failure.20 Nevertheless, the latest trends recommend that newer modes such as PRVC ventilation may be the most favorable option, as it allows patients to receive the most desired VT at the lowest attainable PIP. In addition, PRVC could provide the advantages of both PC and VC, including minimizing airway pressure and providing excellent inspiratory flow and a guaranteed VT.21
Thus far, SIMV-VC is still the most commonly used ventilation mode in treating COPD patients with respiratory failure, and a large number of clinical studies have proven its reliability.22 This mode ensures that patients receive a sufficiently effective ventilatory capacity or ventilation volume through respiratory support by mechanical ventilation and an organic combination of two different ventilation modes: spontaneous breathing and intermittent positive pressure ventilation.
Because of severe pulmonary infection, elderly patients with COPD can have complications of hypoxemia and/or hypercapnic acidosis, in which case the application of SIMV-VC can improve hypoxemia and/or hypercapnic acidosis by triggering the ventilator and enhancing ventilation through spontaneous breathing.
During the acute stage of COPD (AECOPD), the presence of airway inflammation exacerbates airway resistance through airway spasm and sputum retention. Meanwhile, if large VTs are utilized during SIMV-VC mechanical ventilation, they tend to cause hyperventilation and overly high pressure in the local airway, resulting in mediastinal emphysema, subcutaneous emphysema, pneumothorax, and, ultimately, barotrauma.
PRVC can effectively correct acute respiratory failure while simultaneously protecting lung tissue from barotrauma and was proven to be effective in patients with AECOPD and respiratory failure.23 During the application of PRVC, the ventilator calculates the volume and pressure measurements for each respiration and modulates the next inspiratory pressure level according to the measurement results to shorten the gap between the actual VT and the preset VT.
Compared with the SIMV-VC mode, the VT in the PRVC mode can change within a certain range with changes in lung compliance and airway resistance. However, the actual VT ultimately remains relatively stable at the preset level through the microcomputer’s pressure regulation. When severe airway obstruction occurs, the application of a deceleration wave in the PRVC mode increases laminar airflow components and reduces pressure consumption; thus, it requires lower pressure to maintain the same VT.24
The subjects of this research were elderly AECOPD patients with respiratory failure. The results showed a rapid, effective improvement in hypoxemia and oxygenation and reduction in PaCO2 in the experimental group and the control group in both ventilation modes within 2–4 hours. There was no significant difference in vital signs between the two groups after treatments of 2–4 hours and 48 hours.
The improvements in pH and PaCO2 within 2–4 hours of treatment in the experimental group were significantly lower than those in the control group; however, blood gas analysis indices in both groups returned to normal after 48 hours of treatment. This phenomenon may be due to the presence of respiratory rhythm disturbances and subsequent patient–ventilator asynchrony in the early stage of endotracheal intubation in mechanically ventilated patients, who may present additionally with inflammatory airway spasm, sputum retention, and increased airway resistance. During the application of the PRVC mode, a large change in the estimation of ventilation capacity makes it difficult to reach the preset VT, causing the alveolar ventilation volume to be lower than that in the control group. The improvement in ventilation in the first 2–4 hours of PRVC ventilation is not as obvious as it is in SIMV, but as airway pressure is simultaneously controlled while maintaining clinical efficacy, it prevents the occurrence of pulmonary barotrauma and thus has the advantage of being safer.
The PIP in the experimental group was distinctly lower than that in the control group during mechanical ventilation at 2–4 hours and 48 hours, while differences in mean airway pressure, pulmonary dynamic compliance, VT, MV, and ventilator for power were not statistically significant between the two groups, which illustrates that under the condition of ensuring a preset VT and MV volume, PRVC ventilation can effectively reduce PIP, thereby reducing the risk of barotrauma. During treatment, one case of death caused by pneumothorax was observed in the control group, while no case of barotrauma was observed in the experimental group.
Conclusion
This study showed that using PRVC ventilation as a treatment in elderly COPD respiratory failure patients can rapidly improve arterial blood gas analyses and simultaneously maintain a lower PIP, which effectively reduces the risk of barotrauma during 48 hours of mechanical ventilation. It is a safe and effective protective ventilation mode that should be prioritized in clinical practice.
However, the observation duration of this study was restricted to the implementation of mechanical ventilation intervention over 48 hours, which is considered the early stage of mechanical ventilation and does not cover the entire mechanical ventilation process. Therefore, clinical efficacy and barotrauma could not be fully observed in all phases of the mechanical ventilation process. It is vital to continue to evaluate new concepts in invasive mechanical ventilation in larger and long-term studies to optimize outcomes in COPD patients. Further clinical trials or meta-analyses are desired to determine the optimal management for AECOPD, particularly in severely ill patients admitted to the intensive care unit.
Acknowledgment
This study was funded by Shanghai Committee of Science and Technology (No. 13430720500), and National Natural Science Foundation of China (No. 81472175, 81570081, 81500058, 81400043).
Disclosure
The authors report no conflicts of interest in this work.
References
Global Initiative for Chronic Obstructive Lung Disease (GOLD) [webpage on the Internet]. Global Strategy for the Diagnosis, Management, and Prevention of Chronic Obstructive Pulmonary Disease; 2015. Available from: http://www.goldcopd.org/Guidelines/guidelines-global-strategy-for-diagnosis-management.html. Accessed February 1, 2015. | ||
Stefan MS, Shieh MS, Pekow PS, Hill N, Rothberg MB, Lindenauer PK. Trends in mechanical ventilation among patients hospitalized with acute exacerbation of COPD in the United States, 2001 to 2011. Chest. 2015;147(4):959–968. | ||
Celli BR, MacNee W. ATS/ERS task force. Standards for the diagnosis and treatment of patients with COPD: a summary of the ATS/ERS position paper. Eur Respir J. 2004;23(6):932–946. | ||
100md.com [webpage on the Internet]. Manual for the Clinical Application of Mechanical Ventilation. China: Intensive Care Branch of the Chinese Medical Association; 2006. Available from: http://www.100md.com/html/201502/2551/5845.htm. Accessed March 1, 2016. | ||
Riley C, Pilcher J. Volume-guaranteed ventilation. Neonatal Netw. 2003;22(2):17–22. | ||
Valeron Lemaur ME, Lopez Alvarez JM, Gonzalez Jorge R, Manzano Alonso JL. [Intermittent mandatory ventilation]. An Pediatr. 2003;59(1):86–92. | ||
Holt SJ, Sanders RC, Thurman TL, Heulitt MJ. An evaluation of Automode, a computer-controlled ventilator mode, with the Siemens Servo 300A ventilation, using a porcine model. Respir Care. 2001;46(1):26–35. | ||
The Chinese Medical Association Respiratory Disease Branch of the Chronic Obstructive Pulmonary Disease Study Group. Chronic obstructive pulmonary disease diagnosis and treatment guidelines (2007 Revision). Chin Med J. 2007;46(3):254–261. | ||
Ranieri VM, Giuliani R, Cinnella G, et al. Physiologic effects of positive end-expiratory pressure in patients with chronic obstructive pulmonary disease during acute ventilatory failure and controlled mechanical ventilation. Am Rev Respir Dis. 1993;147(1):5–13. | ||
Parrilla FJ, Morán I, Roche-Campo F, Mancebo J. Ventilatory strategies in obstructive lung disease. Semin Respir Crit Care Med. 2014;35(4):431–440. | ||
Kumar A, Pontoppidan H, Falke KJ, Wilson RS, Laver MB. Pulmonary barotrauma during mechanical ventilation. Crit Care Med. 1973;1(4):181–186. | ||
Tagliabue M, Casella TC, Zincone GE, Fumagalli R, Salvini E. CT and chest radiography in the evaluation of adult respiratory distress syndrome. Acta Radiol. 1994;35(3):230–234. | ||
Marini JJ, Culver BH. Systemic gas embolism complicating mechanical ventilation in the adult respiratory distress syndrome. Ann Intern Med. 1989;110(9):699–703. | ||
Hitzl AP, Jörres RA, Heinemann F, Pfeifer M, Budweiser S. Nutritional status in patients with chronic respiratory failure receiving home mechanical ventilation: impact on survival. Clin Nutr. 2010;29(1):65–71. | ||
Añón JM, Lorenzo AG. Prognosis of patients with COPD admitted to the ICU. Thorax. 2009;64(10):916. | ||
Medoff BD. Invasive and noninvasive ventilation in patients with asthma. Respir Care. 2008;53(6):740–748. | ||
Stather DR, Stewart TE. Clinical review: mechanical ventilation in severe asthma. Crit Care. 2005;9(6):581–587. | ||
Ugurlucan M, Basaran M, Erdim F, et al. Pressure-controlled mechanical ventilation is more advantageous in the follow-up of patients with chronic obstructive pulmonary disease after open heart surgery. Heart Surg Forum. 2014;17(1):E1–E6. | ||
Oddo M, Feihl F, Schaller MD, Perret C. Management of mechanical ventilation in acute severe asthma: practical aspects. Intensive Care Med. 2006;32(4):501–510. | ||
Karakurt Z, Yarkin T, Altinoz H, et al. Pressure vs. volume control in COPD patients intubated due to ARF: a case-control study. Tuberk Toraks. 2009;57(2):145–154. | ||
Riverso P, Bernardi PL, Corsa D, Morra MG, Paganini G, Parigi F. Confronto tra tecniche di ventilazione nell’ARDS. Volume controllato vs volume garantito a regolazione di pressione. [A comparison of ventilation techniques in ARDS. Volume controlled vs pressure regulated volume control]. Minerva Anestesiol. 1998;64(7–8):339–343. Italian [with English abstract]. | ||
Karakurt Z, Yarkin T, Altinöz H, et al. Pressure vs. volume control in COPD patients intubated due to ARF: a case-control study. Tuberk Toraks. 2009;57(2):145–154. | ||
Smith-Blair N, Parker DM, Clancy RL, Pierce JD. Pressure-regulated volume-controlled ventilation. Aust Crit Care. 1999;12(2):60–64. | ||
Kallet RH, Campbell AR, Dicker RA, Katz JA, Mackersie RC. Work of breathing during lung-protective ventilation in patients with acute lung injury and acute respiratory distress syndrome: a comparison between volume and pressure-regulated breathing modes. Respir Care. 2005;50(12):1623–1631. |
 © 2016 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2016 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.