Back to Journals » Medical Devices: Evidence and Research » Volume 12
A Comparison Of Conventional Electroencephalography With Amplitude-Integrated EEG In Detection Of Neonatal Seizures
Authors Kadivar M, Moghadam EM, Shervin Badv R, Sangsari R, Saeedy M
Received 6 May 2019
Accepted for publication 10 October 2019
Published 10 December 2019 Volume 2019:12 Pages 489—496
DOI https://doi.org/10.2147/MDER.S214662
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Scott Fraser
Maliheh Kadivar, Elahe Movahedi Moghadam, Reza Shervin Badv, Raziye Sangsari, Maryam Saeedy
Department of Neonatology, Children’s Medical Center, Tehran University of Medical Sciences, Tehran, Iran
Correspondence: Elahe Movahedi Moghadam
Neonatal Health Research Center, Research Institute for Children Health, Shahid Beheshti University of Medical Sciences, Tehran, Iran
Email [email protected]
Introduction: Amplitude-integrated electroencephalogram (aEEG) is widely used in Neonatal Intensive Care Units (NICUs) to monitor neonatal seizures. This method is still not well established compared to conventional electroencephalogram (cEEG), the diagnostic gold standard. However, aEEG can be a good screening tool for the diagnosis of seizures in infants. Our aim in this review study is to evaluate aEEG diagnostic accuracy in comparison with cEEG, for detection of neonatal seizures.
Methods: In this work, we studied the published articles which used EEG and aEEG in the evaluation process of seizures in neonates and compared these techniques to obtain an approach for the detection of neonatal seizures.
Results: Seventeen articles were included. Using aEEG with raw trace to detect individual seizures showed median sensitivity of 78% (range: 68–85) and median specificity of 78% (range: 71–84). The median sensitivity and specificity were 54% (range: 25–95) and 81% (range: 50–100), respectively, in case of using aEEG without raw traces. Brief duration seizures and those occurring away from aEEG leads were less detected.
Conclusion: Studies showed that aEEG has variable sensitivity and specificity. Based on the evidences, aEEG cannot be recommended as the only way for diagnosis and management of seizures in neonates; however, it could complete the diagnosis of seizures in the infant and could be a very good tool for screening seizures.
Keywords: conventional electroencephalography, amplitude-integrated EEG, neonatal seizures
Introduction
Neonatal seizures are the most common neurological manifestations in newborns and often the first sign of neurological dysfunction.1–3 Neonatal seizures usually occur within the first 4 weeks of life in a full-term infant and up to 44 weeks from conception for premature infants. Seizures are more common in neonatal period than other periods of life, particularly in the first 1–2 days to the first week after birth. The incidence of neonatal seizures varies by weight; it is only 2.8 per 1000 for infants with birth weights of 2500 to 3999 g and 57.5 per 1000 in infants with birth weights lower than 1500 g. In Neonatal Intensive Care Units (NICUs), the incidence is as high as 8–15%.1–3
Neonatal seizures may occur because of many different etiologies, such as hypoxic–ischemic encephalopathy which is the most common cause, stroke, intracranial infection, cardiac surgery, extracorporeal membrane oxygenation, etc.4–6
It seems that seizures may affect the maturation and development of the brain in the critical period of life and are associated with a significant incidence of brain injury and long-term neurodevelopmental delay.1–3 They may be short-lived events lasting for a few days only. However, they often imply severe damage or malfunction of the immature brain and they are considered as neurologic emergency conditions which needed urgent diagnosis and management.1–3
Neonatal seizures are usually difficult to recognize as seizure activity in newborns may not be clinically apparent. Clinical observation alone could reduce the successful diagnosis of neonatal seizures because about 80% of the seizures are occult.7 Besides, over-diagnosing of seizure is possible because clinical paroxysmal movements do not correlate with EEG seizure activity which can often be misdiagnosed.8–10 Therefore, electroencephalography (EEG) is an important investigation to accurately identify epileptiform events. Nowadays, two main methods for the detection of neonatal seizures are amplitude-integrated EEG (aEEG) and conventional EEG (cEEG).11–13
In spite of being the diagnostic gold-standard for epileptic seizures, cEEG is of limited availability because of difficult access and the need for neurophysiologists in the clinical centers.14,15 In addition, the results are not available online to help the clinician with patient management.16–18 In contrast, a simple method to gather EEG information (amplified, filtered, and compressed) using a fewer number of electrodes is aEEG, which could detect seizures and provide information on brain electrical activity in real-time. AEEG is increasingly used in the NICUs.19 Several studies have attempted to determine outcomes in babies with neonatal seizures using EEG.20–23
AEEG can be a good screening tool for the diagnosis of seizures in infants. Although it is reported to have less sensitivity and specificity as compared to the cEEG, its sensitivity and specificity make it acceptable to be used as a screening method. Notably, aEEG has an acceptable effect in predicting the neonatal seizure outcome when the background is mildly or severely abnormal.
In the present study, we aimed to evaluate the diagnostic accuracy of neonatal seizures using aEEG and compare it with cEEG. For this aim, we investigated original research articles in which the effectiveness of aEEG and cEEG are compared in the diagnosis of neonatal seizures.
Methods
This short review was conducted and reported as the result of evaluating several studies, and finally, a conclusion from all papers was obtained.
Study Design
Seventeen studies that compared aEEG and cEEG in detection of neonatal seizures were reviewed. The participants in these studies were neonates with suspected seizures or were at risk of seizures.
Inclusion And Exclusion Criteria
We included studies in which aEEG and cEEG have been compared according to their effectiveness in diagnosing seizures in term and/or preterm neonates. Only original research articles and clinical trials were included. Neither review articles nor meta-analyses were included. We excluded studies in which there was no simultaneous cEEG and studies that only focused on EEG pattern without addressing the detection of neonatal seizures.
Research Strategy
PubMed and GoogleScholar databases were searched on February 2018 using the following keywords: Infant [Title] AND aEEG [Title] AND seizure [Title/Abstract]. This resulted in 13 papers in the first step. We also checked the lists of references in these papers and included 4 more papers which also fulfilled the criteria.
Results
A summary of the included papers results is demonstrated in Table 1. The sample size of individual studies varied from 12 to 160 and the total sample size was 814. Some of the studies included a mixed group of term and preterm infants. In four studies, aEEG with raw trace was recorded. One study discussed the accuracy of aEEG in diagnosing “patients with seizures” and seven studies reported the precision of aEEG in the detection of “individual seizures”, and five studies reported on both issues while two studies had evaluated aEEG and conception age.
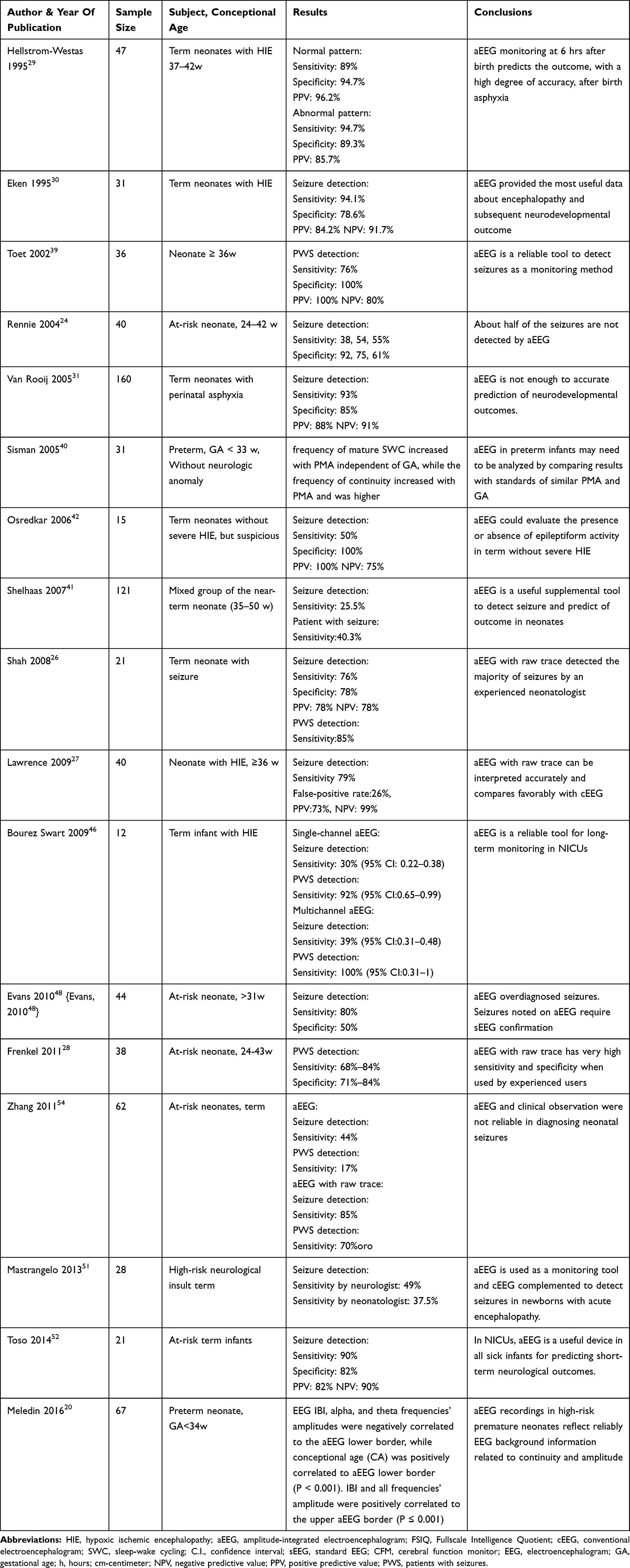 |
Table 1 Important Characteristics Of The Included Studies |
From 40 infants in Rennie et al's (2004) study on 19 infants with and 21 without electrographic seizures, cEEG recordings were compared with a single-channel aEEG from the P3-P4 leads. Sensitivity for “individual seizure” detection was 38% at 6 cm/hr, 54% at 15 cm/hr, and 55% at 30 cm/hr, while specificities were 91%, 75%, and 60%, respectively.24
In Shellhaas et al's (2007) study, six one-year-experienced neonatologists’ interpreted 144 blended strips of single-channel aEEG (19 strips without seizure as control records and 125 strips with seizures from 121 neonates) randomly. The neonatologists reported 22–57% of the “strips with seizure” and 12–38% of “individual seizures”. Using multivariate analyses, the authors concluded that the significant factors in the correct detection of neonatal seizures by aEEG were the seizure duration, aEEG interpretation, amplitude, and frequency.25
In the study of Shah et al (2008), 21 neonates with clinical seizures were studied. In this study, neurologists interpreted the cEEG and neonatologists interpreted two-channel aEEG with the raw trace. Two-channel “aEEG with raw trace” had a specificity of 78% and sensitivity of 76% for seizures detection. The results showed that if an experienced neonatal EEG reader interprets two-channel “aEEG with raw trace”, the majority of electrical seizures could be detected.26
In a randomized controlled trial study, Lawrence et al (2009) tried to evaluate the impact of aEEG monitoring in infants of more than 36 weeks old with the risk of seizures. cEEG and “aEEG with raw trace” were simultaneously recorded from 34 infants with hypoxic–ischemic encephalopathy (HIE). An epileptologist interpreted the cEEG and another reader interpreted the “aEEG with raw trace” independently. “AEEG with raw trace” detected 323/426 (76%) of seizures.27
The study of Frenkel et al (2010) compared two methods of cEEG and aEEG by clinicians with different levels of expertise. A total of 265 paired epochs cEEG/aEEG with raw trace were recorded in 38 infants at risk for seizures. The sensitivity and specificity of “aEEG with raw trace” for the detection of seizures ranged from 68% to 84% and 71% to 84%, respectively.28
Meledin et al (2016) have performed a prospective cohort study with 67 infants less than 34 weeks of gestation. cEEG and aEEG were recorded and assessed separately by a single investigator. A total of 1679 aEEG/EEG pairs of 10-min segments from 189 recordings were analyzed. The authors found a relationship between EEG and aEEG. Accordingly, they suggested that these two methods should be complementary and should be used according to the needs and situations in NICUs.20
The rest of the results of the selected studies has been shown in Table 1.
Discussion
In this study, we have extracted and studied 17 papers (including a total of 814 neonates), in which aEEG and cEEG were compared for the detection of seizures in neonates. Seizures in neonates are relatively common and are associated with poor neurodevelopmental outcomes if not diagnosed early and treated properly. Neonatal seizures which lead to increased morbidity and mortality are usually found in NICU. Newborns with seizures are at risk for neonatal death, neurological impairment, developmental delay, and later epilepsy.32
Predicting outcomes can be very difficult in babies with neonatal seizures. In this regard, etiology, clinical profile, EEG background, and neuroimaging have all been considered for prognostication. Neonatal seizures can or cannot have clinical correlates and, therefore, are difficult to be recognized. We analyzed the predictive value of the aEEG background for the neurodevelopmental outcomes.32
Neonatal seizures are still associated with significant mortality and morbidity even in advanced NICUs. Etiologies of neonatal seizures play a primary role in long-term sequelae.33 In Anand et al's study, the mortality outcome of babies with seizures was 17.2%,34 whereas in Nagarajan et al's study, the mortality outcome reached 21%,6 similar to Pisani et al's reports that showed mortality outcome of 19%.35 It was slightly higher than 15% reported from Brazil and Da Silva’s groups or 7% in the study by Tekgul et al.36 The lower mortality in Tekgul’s and Da Silva’s groups may be as a result of babies identification based on clinical seizures.36,37 It is essential to select a test with a very high sensitivity to detect “individual seizures” and to enable the correct identification of seizures as many as possible. In Nagarajan et al's study, babies with neonatal seizures had significant neurodevelopmental consequences: neurodevelopmental impairment in 63%, cerebral palsy in 30%, vision and hearing impairment in 23%, and epilepsy in 33%. Legido et al reported cerebral palsy and developmental delays in about two-thirds of the survivors of babies in which EEG documented seizures38 and severe neurological impairment was reported in Anand’s group (18.5%).34 Probably, the underlying etiology (influencing the background) and the seizures have an additive detrimental effect on prognosis. The occurrence of epilepsy on follow-up has varied from 27% to 56%.39,40 Various causes such as different patient groups, probable etiology identification of seizures by video EEG or clinical, gestational ages and geographical location affect these variations.41,42 Postnatal epilepsy is known as a significant neurological consequence in several studies on the follow-up of babies with neonatal seizures. The incidence of postnatal epilepsy increases when more abnormality is seen in EEG backgrounds.23,39,40,43,44
EEG remains one of the most useful tools for the diagnosis and prognosis of neonatal seizures. A large number of previous studies have shown that EEG is a very good predictor of neurodevelopmental outcomes,1,23,43 while a few studies suggested limited value in predicting outcome.45,46 Severely abnormal EEG background activity was associated with severe injury and neurodevelopmental outcome,47,48 while a mild-to-moderate impairment in EEG background was not a significant prognostic value.47,48
aEEG is a simplified online bedside neurophysiological monitoring tool. The data of aEEG data are processed through EEG signals recorded from one or more channels that reflect the EEG background.47,48
A meta-analysis study conducted by Spitzmiller in 2007 on eight papers, which was performed on asphyxiated full-term infants, showed the sensitivities and specificities of severely abnormal aEEG tracings in prediction of poor outcome (the predicted poor outcome was from 73% to 100%, and a negative likelihood ratio was 0.09 (0.06–0.15 95% CI)). This meta-analysis concluded that aEEG is an excellent screening bedside tool in term hypoxic–ischemic encephalopathic infants to predict a long-term neurodevelopmental outcome.45 In contrast, Osredkar et al reported that the sensitivity of seizure detection of aEEG to standard EEG was 50%, the specificity was 100%, the positive predictive value was 100%, and the negative predictive value was 75%.42 These findings are possibly obtained due to the target groups (ie, infant without severe HIE but at risk for seizure).
In a systematic review article in 2015, Rakshasbhuvankar et al studied 10 papers including 433 neonates and evaluated aEEG and cEEG for seizure detection. Sensitivity and specificity were 76% (range: 71–85) and 85% (range: 39–90), respectively, when aEEG was investigated with raw trace, while sensitivity and specificity were reported low if aEEG was investigated without raw trace (39% and 95%, respectively).5
Chandrasekaran et al (2017) reviewed a total of nine articles (total sampling=529) in a meta-analysis. Sensitivity and specificity of aEEG at 6 hrs of age were 96% (95% CI, 91 to 98) and 39% (95% CI, 32 to 46), respectively. The highest diagnostic odds ratio of an abnormal trace was 48 hrs (66.9 (95% CI 19.7, 227.2)). Adverse neurodevelopmental outcome was associated with persistently abnormal aEEG at 48 hrs or more. Normal 6 hr aEEGs had high negative predictive value, but did not exclude adverse outcomes.49
The median sensitivity for the detection of the neonate with seizures was 80% (range: 76–85, four studies) and it was reasonably good when it was “aEEG with raw trace”. Thus, it could be helpful to identify neonates who might benefit most from doing continuous EEG. aEEG background activity trends are good indicators for prediction of long-term outcome and neurodevelopmental prognosis which was confirmed by many articles.12,15,34,50 Therefore, in the NICUs, the aEEG is appropriately used to evaluate the background activity of the aEEG.
Although it is very easy to implement by the clinicians, shorter seizures are missed due to time compression in the aEEG. Moreover, focal seizures often remain unnoticed due to the limited number of used electrodes. Some of the unique characteristics that make seizures identifiable in neonates, such as spatial evolution, may not be evident on aEEG. Considering the inherent technical limitations, it is illogical to expect aEEG to detect all the seizures. If aEEG is to be used for making treatment decisions, high specificity is also important, because wrong diagnosis and too much treatment could be potentially harmful to the developing brain.51–53 It has been made clear that EEG artifacts (such as electrocardiography (ECG) or high-frequency ventilation) occur frequently despite the filtering process and can influence the aEEG recording significantly.54
Even though cEEG is the gold standard for seizure detection, many neonatologists tend to use aEEG for diagnosis, monitoring, and management of seizures. A recent survey of American neonatologists found that nearly 80% of those who used aEEG used it for deciding to treat seizures.
This review suffers from some limitations including heterogeneity between studies, different times of performing aEEG, post-conceptional age, and underlying diseases. Further projects and research need to be done to obtain a generalizable conclusion about the diagnostic accuracy of aEEG.
Although the gold standard for neonatal seizure detection is conventional video-EEG monitoring, it is expensive, needs expert EEG reading and technologist, the data collection procedure is complex and restricted to be performed everywhere and also it prevents nursing work. These factors have limited their use. The use of aEEG on sick neonates has clinical value in NICUs but does not replace the standard EEG. Finally, it is worth noting that while aEEG can be used as a complementary technique, further research is still required with a focus on improving the sensitivity and specificity of the technique to advance its utility in clinical practice.
Conclusion
Short studies showed that aEEG has variable sensitivity and specificity. By all this information, it is suggested that aEEG is a very good screening tool for detecting neonates who need cEEG in the NICU but is not recommended for primary diagnosis and management of neonates with seizure.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Volpe JJ. Neurology of the Newborn.
2. Rennie JM, Boylan GB, Neonatal seizures and their treatment. Curr Opin Neurol. 2003;16(2):177–181. doi:10.1097/01.wco.0000063768.15877.23
3. Hill A, Neonatal seizures. Pediatrics in Review. 2000;21(4):117–121. doi:10.1542/pir.21-4-117
4. Tadic BV, Kravljanac R, Sretenovic V, Vukomanovic V. Long-term outcome in children with neonatal seizures: A tertiary center experience in cohort of 168 patients. Epilepsy Behav. 2018;84:107–113. doi:10.1016/j.yebeh.2018.05.002
5. Rakshasbhuvankar A, Paul S, Nagarajan L, Ghosh S, Rao S. Amplitude-integrated EEG for detection of neonatal seizures: a systematic review. Seizure. 2015;33:90–98. doi:10.1016/j.seizure.2015.09.014
6. Nagarajan L, Palumbo L, Ghosh S. Neurodevelopmental outcomes in neonates with seizures: a numerical score of background encephalography to help prognosticate. J Child Neurol. 2010;25(8):961–968. doi:10.1177/0883073809355825
7. Sheth RD, Hobbs GR, Mullett M. Neonatal seizures: incidence,onset, and etiology by gestational age. J Perinatol. 1999;19(1):40–43.
8. Heljic S, Uzicanin S, Catibusic F, Zubcevic S, Predictors of mortality in neonates with seizures; a prospective cohort study. Med Arch. 2016;70(3):182–185. doi:10.5455/medarh.2016.70.182-185
9. Glass HC, Glidden D, Jeremy RJ, Barkovich AJ, Ferriero DM, Miller SP. Clinical neonatal seizures are independently associated with outcome in infants at risk for hypoxic-ischemic brain injury. J Pediatr. 2009;155(3):318–323. doi:10.1016/j.jpeds.2009.03.040
10. Clancy RR, Legido A, Lewis D, Occult neonatal seizures. Epilepsia. 1988;29(3):256–261. doi:10.1111/j.1528-1157.1988.tb03715.x
11. Sanchez Fernandez I, Loddenkemper T. aEEG and cEEG: two complementary techniques to assess seizures and encephalopathy in neonates: editorial on “Amplitude-integrated EEG for detection of neonatal seizures: A systematic review” by Rakshasbhuvankar et al. Seizure. 2015;33:88–89. doi:10.1016/j.seizure.2015.10.010
12. Ben-Ari Y, Holmes GL, Effects of seizures on developmental processes in the immature brain. Lancet Neurol. 2006;5(12):1055–1063. doi:10.1016/S1474-4422(06)70626-3
13. Murray DM, Boylan GB, Ali I, Ryan CA, Murphy BP, Connolly S. Defining the gap between electrographic seizure burden, clinical expression and staff recognition of neonatal seizures. Arch Dis Child Fetal Neonatal Ed. 2008;93(3):F187–F191. doi:10.1136/adc.2005.086314
14. Panayiotopoulos CP. The Epilepsies: Seizures, Syndromes and Management. Chapter 5. Oxfordshire (UK): Blandon Medical publishing;2005.
15. Boylan G, Burgoyne L, Moore C, O’Flaherty B, Rennie J. An international survey of EEG use in the neonatal intensive care unit. Acta Paediatr. 2010;99(8):1150–1155. doi:10.1111/j.1651-2227.2010.01809.x
16. Malone A, Ryan CA, Fitzgerald A, Burgoyne L, Connolly S, Boylan GB. Interobserver agreement in neonatal seizure identification. Epilepsia. 2009;50:2097–2101. doi:10.1111/j.1528-1167.2009.02132.x
17. Abend NS, Wusthoff CJ, Neonatal seizures and status epilepticus. J Clin Neurophysiol. 2012;29(5):441–448. doi:10.1097/WNP.0b013e31826bd90d
18. Thorngate L, Foreman SW, Thomas KA. Quantification of neonatal amplitude-integrated EEG patterns. Early Hum Dev. 2013;89(12):931–937. doi:10.1016/j.earlhumdev.2013.09.018
19. Toet MC, Lemmers PM. Brain monitoring in neonates. Early Hum De. 2009;85(2):77–84. doi:10.1016/j.earlhumdev.2008.11.007
20. Meledin I, Abu Tailakh M, Gilat S, et al. Comparison of amplitude-integrated EEG and conventional EEG in a cohort of premature infants. Clin EEG Neurosci. 2017;48(2):146–154. doi:10.1177/1550059416648044
21. Gucuyener K. Use of Amplitude-integrated electroencephalography in neonates with special emphasis on Hypoxic-ischemic encephalopathy and therapeutic hypothermia. J Clin Neonat. 2016;5(1):18–30. doi:10.4103/2249-4847.173272
22. Shah NA, Wusthoff CJ. How to use: amplitude-integrated EEG (aEEG). Arch Dis Child Educ Pract Ed. 2015;100(2):75–81. doi:10.1136/archdischild-2013-305676
23. Neubauer OD, Paro-Panjan SA, Derganc M, Recording conventional and amplitude-integrated EEG in neonatal intensive care unit. Eur J Paediatr Neurol. 2011;15(5):405–416. doi:10.1016/j.ejpn.2011.03.001
24. Rennie JM, Chorley G, Boylan GB, Pressler R, Nguyen Y, Hooper R, Non-expert use of the cerebral function monitor for neonatal seizure detection. Arch Dis Child Fetal Neonatal Ed. 2004;89(1):F37–F40. doi:10.1136/fn.89.1.f37
25. Shellhaas RA, Soaita AI, Clancy RR. Sensitivity of amplitude-integrated electroencephalography for neonatal seizure detection. Pediatrics. 2007;120(4):770–777. doi:10.1542/peds.2007-0514
26. Shah DK, Mackay MT, Lavery S, et al. Accuracy of bedside electroencephalographic monitoring in comparison with simultaneous continuous conventional electroencephalography for seizure detection in term infants. Pediatrics. 2008;121(6):1146–1154.
27. Lawrence R, Mathur A, Zempel J, Inder T, A pilot study of continuous limited-channel aEEG in term infants with encephalopathy. J Pediatr. 2009;154(6):835–841. doi:10.1016/j.jpeds.2009.01.002
28. Frenkel N, Friger M, Meledin I, et al. Neonatal seizure recognition–comparative study of continuous-amplitude integrated EEG versus short conventional EEG recordings. Clin Neurophysiol. 2011;122(6):1091–1097.
29. Hellstrom-Westas L, Rosen I, Svenningsen NW. Predictive value of early continuous amplitude integrated EEG recordings on outcome after sever birth asphyxia in full term infants. Arch Dis Child Fetal Neonatal Ed. 1995;72(1):F34–F38. doi:10.1136/fn.72.1.f34
30. Eken P, Toet M, Groenendaal F, de Vries L. Predictive value of early neuroimaging, pulsed Doppler and neurophysiology in full term infants with hypoxic-ischaemic encephalopathy. Arch. Dis. Childhood. Fetal Neonatal Ed. 1995;73:75–80. doi:10.1136/fn.73.2.F75
31. van Rooij L, Toet M, Osredkar D, van Huffelen AC, Groenendaal F, de Vries L. Recovery of amplitude integrated electroencephalographic background patterns within 24 hrs of perinatal asphyxia. Arch. Dis. Childhood. Fetal Neonatal Ed. 2005;90:245–251. doi:10.1136/adc.2004.064964
32. Karpiński Ł, Mazela J. Amplitude-integrated electroencephalography use in preterm infants: current knowledge and applications. NeoReviews. 2015;16(9):e526–e534. doi:10.1542/neo.16-9-e526
33. Ter Horst HJ, Sommer C, Bergman KA, Fock JM, van Weerden TW, Bos AF. Prognostic significance of amplitude-integrated EEG during the first 72 hrs after birth in severely asphyxiated neonates. Pediatr Res. 2004;55(6):1026–1033. doi:10.1203/01.pdr.0000127019.52562.8c
34. Anand V, Nair P. Neonatal seizures: predictors of adverse outcome. J. Pediatr. Neurosci. 2014;9:97–99. doi:10.4103/1817-1745.139261
35. Pisani F, Cerminara C, Fusco C, Sisti L. Neonatal status epilepticus vs recurrent neonatal seizures: clinical findings and outcome. Neurology. 2007;69:2177–2185. doi:10.1212/01.wnl.0000295674.34193.9e
36. Tekgul H, Gauvreau K, Soul J, et al. The current etiologic profile and neurodevelopmental outcome of seizures in term newborn infants. Pediatrics. 2006;117:1270–1280. doi:10.1542/peds.2005-1178
37. Da Silva G, Nunes L, Da Costa J. Risk factors for developing epilepsy after neonatal seizures. Pediatr. Neurol. 2004;30:271–277. doi:10.1016/j.pediatrneurol.2003.09.015
38. Legido A, Clancy R, Berman P. Neurologic outcome after electroencephalographically proven neonatal seizures. Pediatrics. 1991;88:583–596.
39. Toet MC, van der Meij W, de Vries LS, Uiterwaal CS, van Huffelen KC, Comparison between simultaneously recorded amplitude integrated electroencephalogram (cerebral function monitor) and standard electroencephalogram in neonates. Pediatrics. 2002;109(5):772–779. doi:10.1542/peds.109.5.772
40. Sisman J, Campbell D, Brion L. Amplitude-integrated EEG in preterm infants: maturation of background pattern and amplitude voltage with postmenstrual age and gestational age. J. Perinatol. 2005;25:391–396. doi:10.1038/sj.jp.7211291
41. Tao JD, Mathur AM. Using amplitude-integrated EEG in neonatal intensive care. J Perinatol. 2010;30(Suppl):S73–S81. doi:10.1038/jp.2010.93
42. Osredkar D, Derganc M, Paro-Panjan D, Neubauer D. Amplitude-integrated electroencephalography in full-term newborns without severe hypoxic-ischemic encephalopathy: case series. Croat. Med. J. 2006;47:285–291.
43. Hagmann CF, Robertson NJ, Azzopardi D. Artifacts on electroencephalograms may influence the amplitude-integrated EEG classification: a qualitative analysis in neonatal encephalopathy. Pediatrics. 2006;118(6):2552–2554. doi:10.1542/peds.2006-2519
44. Eken P, Toet MC, Groenendaal F, de Vries LS, Predictive value of early neuroimaging, pulsed doppler and neurophysiology in full term infants with hypoxic-ischaemic encephalopathy. Arch Dis Child Fetal Neonatal Ed. 1995;73(2):F75–F80. doi:10.1136/fn.73.2.f75
45. Spitzmiller RE, Phillips T, Meinzen-Derr J, Hoath SB. Amplitude-integrated EEG is useful in predicting neurodevelopmental outcome in full-term infants with hypoxic-ischemic encephalopathy: a meta-analysis. J Child Neurol. 2007;22(9):1069–1078. doi:10.1177/0883073807306258
46. Bourez-Swart M, van Rooij L, Rizzo C, et al. Detection of subclinical electroencephalographic seizure patterns with multichannel amplitude-integrated EEG in full-term neonates. Clin. Neurophysiol. 2009;120:1916–1922. doi:10.1016/j.clinph.2009.08.015
47. Song J, Xu F, Wang L, et al. Early amplitude-integrated electroencephalography predicts brain injury and neurological outcome in very preterm infants. Sci Rep. 2015;5:13810. doi:10.1038/srep13810
48. Evans E, Koh S, Lerner J, Sankar R, Garg M. Accuracy of amplitude integrated EEG in a neonatal cohort. Arch. Dis. Childhood. Fetal Neonatal Ed. 2010;95:169–173. doi:10.1136/adc.2009.165969
49. Chandrasekaran M, Chaban B, Montaldo P, Thayyil S. Predictive value of amplitude-integrated EEG (aEEG) after rescue hypothermic neuroprotection for hypoxic ischemic encephalopathy: a meta-analysis. J. Perinatol. 2017;37:684–689. doi:10.1038/jp.2017.14
50. Kang S, Kadam S. Neonatal seizures: impact on neurodevelopmental outcomes. Front. Pediatr. 2015;3:101. doi:10.3389/fped.2015.00101
51. Mastrangelo M, Fiocchi I, Fontana P, et al. Acute neonatal encephalopathy and seizures recurrence: a combined aEEG/EEG study. Seizure. 2013;22:703–707. doi:10.1016/j.seizure.2013.05.006
52. Toso P, González AJ, Pérez ME, et al. Clinical utility of early amplitude integrated EEG in monitoring term newborns at risk of neurological injury. J. Pediatr. (Rio. J). 2014;90:143–148. doi:10.1016/j.jped.2013.07.004
53. Bari A, Pathan H, Kokiwar P. Incidence and outcome of neonatal seizures at a tertiary care hospital. Int J Contemp Pediatr. 2017;4:2165–2169. doi:10.18203/2349-3291.ijcp20174750
54. Zhang L, Zhou Y, Chang L, XP L. Diagnostic value of amplitude-integrated electroencephalogram in neonatal seizures. Neurosci. Bull. 2011;27:251–257. doi:10.1007/s12264-011-1413-x
 © 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.