Back to Journals » Journal of Experimental Pharmacology » Volume 11
A comparative experimental study of analgesic activity of a novel non-steroidal anti-inflammatory molecule – zaltoprofen, and a standard drug – piroxicam, using murine models
Authors Santenna C ![]() , Kumar S, Balakrishnan S
, Kumar S, Balakrishnan S ![]() , Jhaj R
, Jhaj R ![]() , Ahmed SN
, Ahmed SN ![]()
Received 21 April 2019
Accepted for publication 17 June 2019
Published 2 August 2019 Volume 2019:11 Pages 85—91
DOI https://doi.org/10.2147/JEP.S212988
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Bal Lokeshwar
C Santenna, Sunil Kumar, S Balakrishnan, Ratinder Jhaj, Shah Newaz Ahmed
Department of Pharmacology, All India Institute of Medical Sciences Bhopal, Bhopal, Madhya Pradesh, India
Purpose: Pain is an unpleasant sensation, but a protective mechanism of our body. It is the most common medical complaint requiring a visit to a physician. The new non-steroidal anti-inflammatory drug (NSAID) – zaltoprofen, is a preferential COX-2 inhibitor. It also inhibits bradykinin-induced nociceptive responses by blocking the B2 receptor-mediated pathway in the primary sensory neurons. The present study was conducted to evaluate and compare the anti-nociceptive activity of zaltoprofen with a conventional NSAID – piroxicam, in a mouse model of acute pain using hot plate and tail flick tests.
Materials and methods: Twenty-four adult Swiss albino mice (20–25 g) of either sex were used in this study. Oral zaltoprofen and piroxicam were used as test and standard drugs respectively. Anti-nociceptive activity was evaluated and compared using hot plate and tail flick tests.
Results: In comparison to the control group (vehicle), zaltoprofen showed a significant increase in reaction time at various time periods in the hot plate and tail flick tests. In the hot plate method, zaltoprofen groups (15 and 20 mg/kg) showed a significant elevation in pain threshold in comparison to control group (vehicle) (p<0.001). In the tail flick model also, zaltoprofen groups (15 and 20 mg/kg) showed a significant increase in the reaction time in comparison to control group (vehicle). In both the analgesiometer assays, zaltoprofen was found to be non-inferior compared to a standard drug – piroxicam (positive control).
Conclusion: Our study concludes that zaltoprofen is an effective analgesic agent in various pain models. Our results support that zaltoprofen has therapeutic potential for treating pain disorders and is non-inferior to a standard drug – piroxicam.
Keywords: anti-nociceptive, hot plate, tail flick, zaltoprofen, piroxicam, mouse model
Introduction
Pain is a heterogenous phenomenon that accompanies the inflammatory response of the body to tissue damage. The immune cells at the site of injury actively release chemical mediators that results in vasodilatation, increased vascular permeability, and cellular infiltration.1 The mechanism is conducive to scavenging of necrotic tissue and promotion of tissue healing. Pain also serves as a cue to the organism to withdraw from perceived insult in the external environment. This indicates the existence of a multi-organ system associated with initiation, transmission, and perception of pain. Pain is therefore rightly defined as a:
complex constellation of unpleasant sensory, emotional and cognitive experiences provoked by real or perceived tissue damage and manifested by certain autonomic, psychological, and behavioural reactions.2
The sensory and affective components of pain are modulated by inhibitory and excitatory pathways. Inhibitory neurotransmitters (noradrenaline and serotonin) and drugs (clonidine and dexmedetomidine) act as agonists on α2 adrenoceptors in dorsal horn cells of the spinal cord causing supraspinal analgesia.3 The latest research has shown that non-steroidal anti-inflammatory drugs (NSAIDS) also facilitate noradrenergic activation of α1, α2C and β-adrenoceptors in addition to its peripheral anti-nociceptive action.4
The global burden of morbidity due to pain is huge. The approximate estimated prevalence of pain is 20% in the adult population.5 Annually, 10% of the world's population is newly diagnosed with chronic pain.5 In the pediatric population, studies have shown that 15%–25% of children and adolescents suffer from recurrent and chronic pain.6 The wide prevalence of pain has a serious impact on the health of people. Globally, pain accounted for 18 crores disability adjusted life years, as per a systematic review of data from 2000–2014.7 On the monetary scale, the cumulative health care and economic cost arising from pain has been found to be more than that of heart disease, cancer, or diabetes.7 The effect of pain on the psychological, social, and economic condition of patients and their families, provides a subtle reason for considering pain as an issue of public health importance.5 Treatment and prevention of pain should therefore be safe, effective, and accessible. A multimodal approach based on an individualized, around-the-clock regimen of NSAIDs, opioids or acetaminophen is recommended to optimize efficacy and minimize the risk of adverse events.8 It involves a stepladder pattern of drug and dose escalation as pain scales up the severity score.9
COX inhibitors are an integral part of most analgesic regimens. COX enzymes exist in two forms, COX-1 and COX-2. COX-1 isoform is constitutive and produces prostanoids essential for physiological processes including protection of gastric mucosa. COX-2 is inducible and synthesizes prostanoids that mediate inflammatory processes like pain, fever, tissue injury, and infection. Classic NSAIDs inhibit both COX-1 and COX-2 isoforms and decrease pain in both acute and chronic pain conditions across the entire spectrum of pain severity.9 However, non-selective inhibition of COX interferes with physiological functions and cause adverse effects like peptic ulcers, platelet dysfunction, helicobacter pylori infection, and nephrotoxicity. On the other hand, COX-2 inhibitors exhibit fewer gastrointestinal and other side effects but have similar anti-inflammatory, anti-pyretic, and analgesic properties.10 In inflammatory states, the expression of COX-2 is accentuated both centrally and peripherally under the influence of proinflammatory cytokine IL-1-b. COX-2 inhibitors modulate nociception through differential activity at both the sites.10 Zaltoprofen, a preferential COX-2 inhibitor, is a potent anti-inflammatory and analgesic propionic acid derivative with novel anti-nociceptive properties. It not only decreases PGE2 production by acting at the COX enzyme, but also inhibits bradykinin and lipoxygenase pathway of nociception.11 The B2 receptor-mediated signaling pathway on the primary sensory neurons is attenuated without actual blocking of bradykinin receptors. It has a greater inhibitory effect on bradykinin-induced nociception than other NSAIDs.12 In addition, the bradykinin-dependent 12-lipoxygenase pathway of pain is also inhibited. The adverse effects of this molecule on gastric and small intestinal mucosa are comparable with other safe NSAIDs.11 The unique mechanism of action of zaltoprofen makes it a promising drug for treatment of painful conditions. So the present study was designed to compare the analgesic efficacy of novel NSAID, zaltoprofen, with standard drug, piroxicam, in a mouse model of acute pain.
Materials and methods
Animals
Adult Swiss albino mice (20–25 g) of either sex were used in this study. All the animals were obtained from Institutional Central Animal House, All India Institute of Medical Sciences (AIIMS) Bhopal, Madhya Pradesh, India. Animals were kept in cages in standard temperature-regulated rooms with air-cooling and 12 hours light and dark cycle and had free access to water and standard laboratory diet. They were allowed to acclimatize to the laboratory conditions and trained to acclimatize to restrainer for a period of 1 week before the experiments were conducted. Food was withdrawn 12 hours prior to drug administration until the completion of the study. The study was approved by the Institutional Animal Ethics Committee (IAEC), AIIMS Bhopal, India and all the experiments were performed as per the Committee for the Purpose of Control and Supervision of Experiments on Animals (CPCSEA) guidelines.
Drugs and reagents
We used piroxicam as positive control in our experiment. Piroxicam is a non-steroidal anti-inflammatory agent with analgesic and anti-pyretic properties comparable to standard NSAIDS in terms of safety and efficacy. It is a standard drug used in animal experiments as a positive control to evaluate and compare the efficacy of newer molecules. The dose of piroxicam used in our experiments in Swiss albino mice corresponded to human equivalent dose for analgesic action.
Test drug zaltoprofen was purchased from J B Chemicals and Pharmaceuticals Ltd (Mumbai, India) and the standard drug piroxicam from Windlas biotech private limited (Dehradun, India). Zaltoprofen and piroxicam were dissolved in normal saline for oral administration. The animals were divided into four groups (six animals in each group). Group I (vehicle control) mice were administered normal saline 10 mL/kg body weight (NS) orally; Group II (positive control) mice were administered piroxicam 10 mg/kg body weight (PRC10); Group III (Test-I) mice were administered zaltoprofen 15 mg/kg body weight (ZLP15): Group IV (Test II) mice were administered zaltoprofen 20 mg/kg body weight (ZLP20).
Evaluation of analgesic activity
Hot plate and tail flick methods were used to assess analgesic activity of study drugs.
Eddy’s hot plate model and procedure
A modified method of Eddy and Leimbach was used as one of the methods for studying the analgesic effects of the drugs.13 The instrument used in our study was hot plate analgesia meter (IITC Inc. Life Science, CA, USA). It consists of an arrangement of an electrically heated flat platforms from which the animal cannot escape by itself. The temperature of the hot plate can be controlled as per requirement and was maintained at 50°C–55°C for our experiment. Food was withdrawn 12 hours before drug administration and reinstituted after completion of the experiment. The individual mice were placed on the hot plate and were immediately removed as soon as responses like jumping or licking of the paws were seen. A cut-off time of 10 seconds was followed to avoid any thermal injury to the paws. The time taken by the animal to elicit the reflexive pain behavior was taken as the reaction time. The reaction time in seconds was counted at 0, 30, 60, and 90 minutes after the respective treatment.
Tail flick test method and procedure
The second method used in our study was the tail flick test with radiant heat. We used a tail flick digital analgesia meter (Ugo Basile, Gemonio, Italy) for this test. The instrument consists of an arrangement of exposing the middle part of the tail of the restrained mouse to a point source of radiant heat. The animal withdraws its tail in response to the heat applied. The reaction time of this movement is known as tail flick latency. A prolongation of the reaction time is adjudged as an analgesic activity. The instrument automatically records the reaction time and the heat source is simultaneously switched off. A cut-off time of 15 seconds was set as the threshold to avoid damage to the tail of the animal. Animals that showed a mean reaction time of more than 15 seconds were not included in the study. Food was withdrawn 12 hours before drug administration and reinstituted after completion of the experiment. The tail flick latency was recorded prior to drug administration (baseline value) and at 30, 60, and 90 minutes after drug administration.
Statistical analysis
Results are expressed as mean ± SD. Data were analyzed using SPSS version 22.0. Comparison between different groups was done by one-way ANOVA followed by Bonferroni’s test to compare difference between groups at the prespecified time intervals. p-value less than 0.05 (p<0.05) was considered statistically significant.
Results
Hot plate test
Pretreatment with zaltoprofen and standard piroxicam showed significant elevation in pain threshold in comparison to vehicle control as represented in Figure 1 and Table 1. As compared to standard piroxicam 10 mg/kg (PRC10), zaltoprofen at doses of 15 mg/kg (ZLP15) and 20 mg/kg (ZLP20) showed maximum effect at (Figure 2) 30 minutes but PRC10 showed its maximum effects at 60 minutes. By applying Bonferroni's test, it was shown that there was no statistically significant difference between test and standard drugs at 30 and 60 minutes respectively. However, at 90 minutes, PRC10 showed greater mean reaction time than ZLP15, which was statistically significant (p-value<0.05).
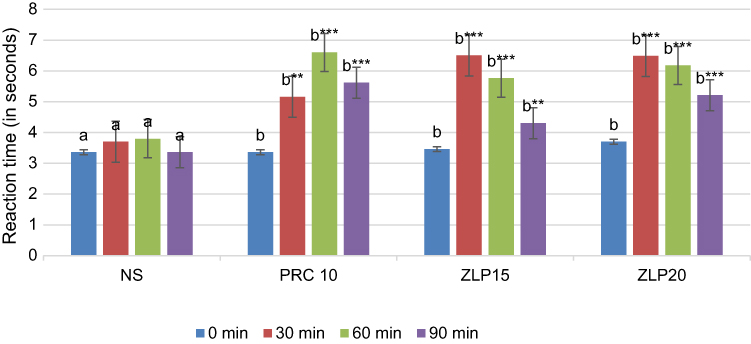 |
Figure 1 Reaction time in seconds (mean value) with different drug dosages in hot plate model of pain in mice.Notes: ** and *** represent p-value <0.01 and 0.001 respectively; a denotes NS control at different time intervals; b denotes test and standard drugs compared to NS. One-way ANOVA with post hoc Bonferroni's test was used for between group differences.Abbreviations: NS, normal saline; PRC10, piroxicam 10 mg/kg; ZLP15, zaltoprofen 15 mg/kg, ZLP20, zaltoprofen 20 mg/kg. |
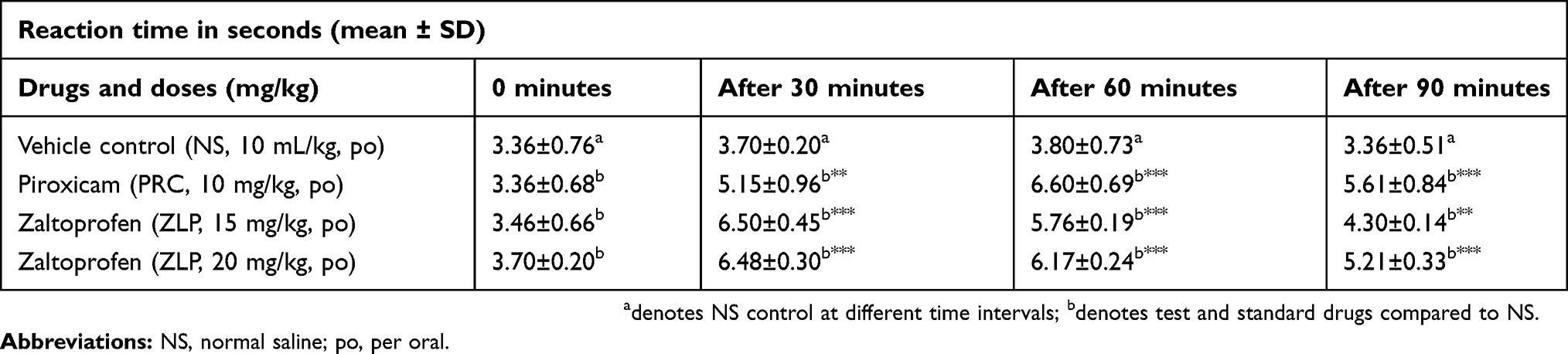 |
Table 1 Reaction time in seconds with different drug dosages in hot plate model of pain in mice |
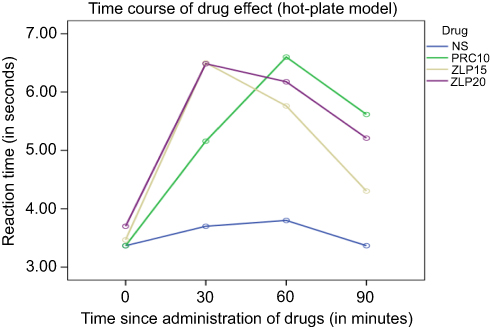 |
Figure 2 Time course of drug effect (Hot-plate model). Abbreviations: NS, normal saline; PRC10, piroxicam 10 mg/kg; ZLP15, zaltoprofen 15 mg/kg; ZLP20, zaltoprofen 20 mg/kg. |
Tail flick test
Pretreatment with zaltoprofen demonstrated significant and dose-dependent anti-nociceptive activity in the tail flick test at doses of 15 and 20 mg/kg at 30, 60, and 90 minutes (P<0.001) as compared to normal saline. Under similar conditions, pretreatment with piroxicam significantly increased latency to radiant heat stimulation 30 minutes after administration and the anti-nociceptive effect was maintained during the entire period of evaluation. By applying Bonferroni's test, it was shown that there was no statistically significant difference between effects of test and standard drugs at 30, 60, and 90 minutes respectively, as represented in Table 2 and Figure 3.
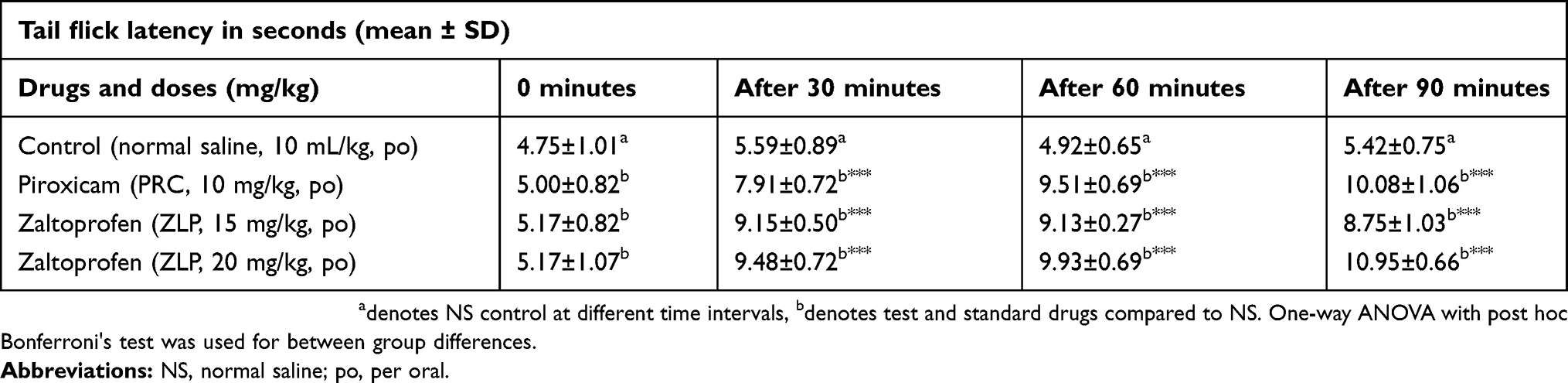 |
Table 2 Tail flick latency with different drug dosages in tail flick model of pain in mice |
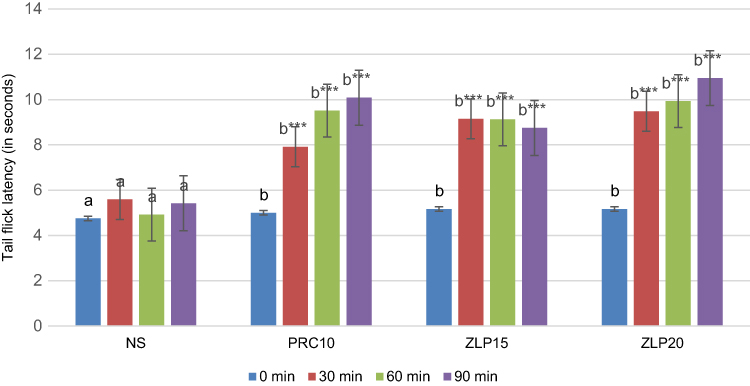 |
Figure 3 Tail flick latency with different drug dosages in tail flick model of pain in mice.Notes: *** represents p-values < 0.001; a denotes NS control at different time intervals, b denotes test and standard drugs compared to NS. One-way ANOVA with post hoc Bonferroni's test was used for between group differences.Abbreviations: NS, normal saline; PRC10, piroxicam 10 mg/kg; ZLP15, zaltoprofen 15 mg/kg; ZLP20, zaltoprofen 20 mg/kg. |
Discussion
Hot plate and tail flick methods are used in animal models of pain based on polysynaptic reflexes initiated at the spinal level and modulated from supraspinal centers. Cortical and brainstem control of these reflexes is strengthened by training and acclimatization.13 These reflexes are generated due to the application of heat, cold, mechanical, and electrical stimulus.14 Thermal and radiant heat are used in hot plate and tail flick models respectively. With the hot plate, pain reflex behavior is noted as jumping and licking of paws, whereas with tail flick, the same is indicated by withdrawal of tail from the ray of incident radiant heat. The behavior and type of pain usually depends on the affected part of tissue such as skin, muscle, joint, viscera, etc15,16 and the mechanism of injury such as thermal, mechanical, inflammatory, neuropathic.14,17 Both are acute models of pain and both types of stimuli induce pain by heat-mediated damage of tissues and inflammation leading to release of peripheral mediators.18 Owing to underlying anatomical and physiological similarities between the two species, human disease can be accurately replicated in murine models for testing of drugs. The tail flick model of acute pain involves spinal and bulbospinal pathways while the hot plate method involves additional supraspinal modulation. Despite having poor face and construct validity, the models can be used in predicting efficacy of both opioid and non-opioid (at higher dose) analgesics in humans.19,20
In our study, zaltoprofen at two different doses of 15 and 20 mg/kg (ZLP15 and ZLP20) significantly increased the threshold of pain at all time intervals in both the models (hot plate and tail flick) of acute pain as compared to normal saline (vehicle) group (Figures 1–4; Tables 1 and 2). In the hot plate model of acute pain, the maximum effect of zaltoprofen (both at 15 mg/kg and 20 mg/kg) was observed at 30 minutes as compared to standard piroxicam (10 mg/kg), which showed its maximum effect at 60 minutes (Figure 1; Tables 1). This indicates that zaltoprofen had a quicker onset of action as compared to piroxicam in this part of the experiment. However, there was no statistically significant difference between the maximum effects of the two drugs at 30 and 60 minutes, respectively. At 90 minutes, PRC10 showed greater mean reaction time than ZLP15 which was statistically significant (p-value<0.05). Higher dose zaltoprofen (ZLP20) showed a peak effect at 30 minutes (like ZLP15) but continued to show equally efficacious analgesia compared to PRC10 until 90 minutes (Figure 2). Therefore, in the hot plate model, both ZLP15 and ZLP20 had earlier peak action than PRC10 (although statistically not significant), but only ZLP20 had a similar duration of action as compared to PRC10. In the tail flick model of acute pain, all three drug groups, PRC10, ZLP15, and ZLP20, showed significantly increased pain threshold in a dose-dependent manner (Figure 3; Table 2) at all time intervals as compared to the control (vehicle) group. The mean tail flick latency continued to increase for PRC10 and ZLP20 until 90 minutes, while ZLP15 started showing decline in efficacy after 30 minutes (Figure 4). However, there was no statistically significant difference in mean tail flick latency between the three drug groups at the prefixed time points of 0, 30, 60, and 90 minutes. Therefore, in the tail flick method, the three drug dosages were observed to be equally efficacious in analgesic effect during the experimental time period of 90 minutes. When the results of the two analgesiometric assays (hot plate and tail flick) in our study were compared, it was evident that the same drug groups (PRC10, ZLP15, ZLP20) showed variation in the time course of drug effect based on the type of analgesiometer. The variations in the onset and peak of the two drugs in the two types of analgesiometer (hot plate and tail flick) are shown in Figures 2 and 4, respectively. The peak response of zaltoprofen (15 mg/kg) was seen at the same time (at 30 minutes) in both the assays, but the peak responses of PRC10 and ZLT20 were seen at different times in the two assays. It has been indicated in previous studies that the anti-nociceptive action of NSAIDs might involve central neural mechanisms in addition to the peripheral analgesia induced by COX inhibition. It is also known that there is significantly greater supraspinal modulation of pain perception in the hot plate method compared to the tail flick method. While the pharmacokinetics of a drug can be assumed to be constant in standard test conditions, it is the pharmacodynamic differences of the same drug in different analgesiometer assays, arising out of processing and modulation of the nociceptive input by the spinal cord, that can explain the variation in time course of drug effect. This corroborates the fact that analgesic action of NSAIDs also involve central mechanisms.21 Despite the gaps in knowledge of the mechanism of pain and pain relief that exist at present, our study points out that zaltoprofen can be utilized as an effective alternative to standard analgesic in treatment of painful conditions. In a randomized, comparative, multicentric, double blind, double-dummy, Phase III clinical study conducted in patients with primary knee osteoarthritis, comparing zaltoprofen with diclofenac, it was concluded that the efficacy and safety of zaltoprofen is clinically non-inferior to that of diclofenac.22 In another observational, prospective study, zaltoprofen in combination with topical anesthetic gel was found to be superior to anesthetic gel alone in controlling cystoscopy-related pain.23 Recently, a study published in Cancer Medicine concluded that zaltoprofen could be a promising drug against the malignant phenotypes in chondrosarcomas via activation of PPAR γ and inhibition of MMP2 activity.24
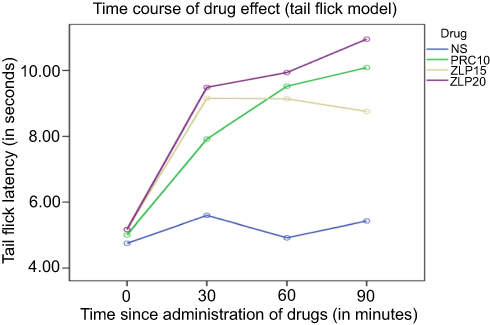 |
Figure 4 Time course of drug effect (Tail flick model). Abbreviations: NS, Normal saline; PRC10, piroxicam 10 mg/kg; ZLP15, Zaltoprofen 15 mg/kg, ZLP20, Zaltoprofen 20 mg/kg. |
Conclusion
Zaltoprofen is an effective analgesic agent in mouse models of acute pain. Its efficacy was non-inferior to standard NSAID, piroxicam, in the conducted experiment. The analgesic properties of this drug can be attributed to inhibition of inflammatory mediators at the site of injury and modulation of the supraspinal pain mechanism. Although more preclinical and clinical studies are required to establish its long-term efficacy and safety, it has immense therapeutic potential of being used as an effective analgesic. Since the doses employed in our study correspond to adult human dose, it is considered that zaltoprofen, which has a novel mechanism of anti-nociception and has already been approved for human use, can be effectively utilized for management of acute somatic pain in clinical conditions.
Acknowledgments
The authors are highly thankful to the staff of the Animal House of All India Institute of Medical Sciences Bhopal for their help and cooperation.
Sources of support
There was no external agency as financer. All materials and equipment were obtained from the institutional facility. Chemicals were procured from standard sources as per institutional rules.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Institute of Medicine (US) Committee on Pain, Disability, and Chronic Illness Behavior; Osterweis M, Kleinman A, Mechanic D, Editors. Pain and Disability: Clinical, Behavioral, and Public Policy Perspectives. Washington (DC): National Academies Press (US); 1987.Vol. 7. The Anatomy and Physiology of Pain. Available from: https://www.ncbi.nlm.nih.gov/books/NBK219252/.
2. Dubin AE, Patapoutian A. Nociceptors: the sensors of the pain pathway. J Clin Invest. 2010;120(11):3760–3772. doi:10.1172/JCI42843
3. Neil MJ. Clonidine: clinical pharmacology and therapeutic use in pain management. Curr Clin Pharmacol. 2011;6(4):280–287.
4. Bannister K. What do monoamines do in pain modulation? Curr Opin Support Palliat Care. 2016;10(2):143–148. doi:10.1097/SPC.0000000000000207
5. Goldberg DS, McGee SJ. Pain as a global public health priority. BMC Public Health. 2011;11:770. doi:10.1186/1471-2458-11-770
6. Mazur A, Radziewicz Winnicki I, Szczepański T. Pain management in children. Ann Agric Environ Med. 2013;20(1):28–34.
7. Henschke N, Kamper SJ, Maher CG. The epidemiology and economic consequences of pain. Mayo Clin Proc. 2015;90(1):139–147. doi:10.1016/j.mayocp.2014.09.010
8. Wardhan R, Chelly J. Recent advances in acute pain management: understanding the mechanisms of acute pain, the prescription of opioids, and the role of multimodal pain therapy. F1000Research. 2017;6. doi:10.12688/f1000research.10493.2
9. Cisewski DH, Motov SM. Essential pharmacologic options for acute pain management in the emergency setting. Turk J Emerg Med. 2019;19(1):1–11. doi:10.1016/j.tjem.2018.11.003
10. Kaye AD, Baluch A, Kaye AJ, Gebhard R, Ralf G, Lubarsky D. Pharmacology of cyclooxygenase-2 inhibitors and preemptive analgesia in acute pain management. Curr Opin Anaesthesiol. 2008;21(4):439–445. doi:10.1097/ACO.0b013e3283007e8d
11. Li L, Ma P, Cao Y, Tao L, Tao Y. Single-dose and multiple-dose pharmacokinetics of zaltoprofen after oral administration in healthy Chinese volunteers. J Biomed Res. 2011;25(1):56–62. doi:10.1016/S1674-8301(11)60007-9
12. Tang H-B, Inoue A, Oshita K, Hirate K, Nakata Y. Zaltoprofen inhibits bradykinin-induced responses by blocking the activation of second messenger signaling cascades in rat dorsal root ganglion cells. Neuropharmacology. 2005;48(7):1035–1042. doi:10.1016/j.neuropharm.2005.01.011
13. Gregory N, Harris A, Robinson C, Dougherty P, Fuchs P, Sluka K. An overview of animal models of pain: disease models and outcome measures. J Pain Off J Am Pain Soc. 2013;14:11. doi:10.1016/j.jpain.2013.06.008
14. Schmidt BL, Hamamoto DT, Simone DA, Wilcox GL. Mechanism of cancer pain. Mol Interv. 2010;10(3):164–178. doi:10.1124/mi.10.3.7
15. Ness TJ, Gebhart GF. Visceral pain: a review of experimental studies. Pain. 1990;41(2):167–234.
16. Sluka KA. Stimulation of deep somatic tissue with capsaicin produces long-lasting mechanical allodynia and heat hypoalgesia that depends on early activation of the cAMP pathway. J Neurosci Off J Soc Neurosci. 2002;22(13):5687–5693. doi:10.1523/JNEUROSCI.22-13-05687.2002
17. DeSantana JM, Sluka KA. Central mechanisms in the maintenance of chronic widespread noninflammatory muscle pain. Curr Pain Headache Rep. 2008;12(5):338–343.
18. Xu J, Brennan TJ. The pathophysiology of acute pain: animal models. Curr Opin Anaesthesiol. 2011;24(5):508–514. doi:10.1097/ACO.0b013e32834a50d8
19. Whiteside GT, Adedoyin A, Leventhal L. Predictive validity of animal pain models? A comparison of the pharmacokinetic-pharmacodynamic relationship for pain drugs in rats and humans. Neuropharmacology. 2008;54(5):767–775. doi:10.1016/j.neuropharm.2008.01.001
20. Berge OG. Predictive validity of behavioural animal models for chronic pain. Br J Pharmacol. 2011;164(4):1195–1206. doi:10.1111/j.1476-5381.2011.01300.x
21. Miranda HF, Lopez J, Sierralta F, Correa A, Pinardi G. NSAID antinociception measured in a chemical and a thermal assay in mice. Pain Res Manag. 2001;6(4):190–196. doi:10.1155/2001/701427
22. Pareek A, Gupta AK, Chandurkar NB, et al. Zaltoprofen, a noninferior alternative to diclofenac for the treatment of primary knee osteoarthritis – a comparative evaluation of efficacy and safety in a 4-week, multicentric, randomized, double-blind, double-dummy trial. Expert Opin Pharmacother. 2011;12(7):1007–1015. doi:10.1517/14656566.2011.566867
23. Komiya A, Endo T, Kobayashi M, et al. Oral analgesia by non‐steroidal anti‐inflammatory drug zaltoprofen to manage cystoscopy‐related pain: a prospective study. Inter Jour of Uro. 2009;16(11):874–880. doi:10.1111/j.1442-2042.2009.02384.x
24. Higuchi T, Takeuchi A, Munesue S, et al. Anti-tumor effects of a nonsteroidal anti-inflammatory drug zaltoprofen on chondrosarcoma via activating peroxisome proliferator-activated receptor gamma and suppressing matrix metalloproteinase-2 expression. Cancer Med. 2018;7(5):1944–1954. doi:10.1002/cam4.1580
 © 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.