Back to Journals » Patient Preference and Adherence » Volume 15
A Co-Design Process to Elaborate Educational Materials to Promote Appropriate Use of Antibiotics for Acute Lower Respiratory Tract Infections in Primary Healthcare in Catalonia (Spain)
Authors Medina-Perucha L ![]() , Gálvez-Hernández P, García-Sangenís A
, Gálvez-Hernández P, García-Sangenís A ![]() , Moragas A
, Moragas A ![]() , Cots JM, Lanau-Roig A, Borrás A, Amo I, Barragán N, Monfá R, Llor C, Berenguera A
, Cots JM, Lanau-Roig A, Borrás A, Amo I, Barragán N, Monfá R, Llor C, Berenguera A ![]()
Received 17 December 2020
Accepted for publication 4 February 2021
Published 8 March 2021 Volume 2021:15 Pages 543—548
DOI https://doi.org/10.2147/PPA.S297581
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Johnny Chen
Laura Medina-Perucha,1 Pablo Gálvez-Hernández,2,3 Ana García-Sangenís,1,4 Ana Moragas,5 Josep María Cots,6 Anna Lanau-Roig,6 Alícia Borrás,2,7 Isabel Amo,2 Nieves Barragán,8 Ramon Monfá,1,4 Carl Llor,1,9 Anna Berenguera1,4,10
1Fundació Institut Universitari per a la recerca a l’Atenció Primària de Salut Jordi Gol i Gurina (IDIAPJGol), Barcelona, Spain; 2Institut Universitari de Pacients (Patients’ University Institut), Universitat Internacional de Catalunya, Barcelona, Spain; 3University of Toronto, IHPME-BFON Collaborative PhD Specialization Program in Health Services and Policy Research, Ontario, Canada; 4Universitat Autònoma de Barcelona, Bellaterra (Cerdanyola del Vallès), Spain; 5Universitat Rovira i Virgili, Jaume I Health Centre, Institut Català de la Salut, Tarragona, Spain; 6La Marina Health Centre, Institut Català de la Salut, Associació d’Infermeria Familiar i Comunitària de Catalunya, Barcelona, Spain; 7Escola Universitària d’Infermeria, Escoles Universitàries Gimbernat, Universitat Autònoma de Barcelona, Sant Cugat del Vallès, Spain; 8Societat Catalana de Medicina Familiar i Comunitària (Camfic), Grupo Programa Comunicación y Salud semFYC. CAP Vallcarca Health Centre, Barcelona, Spain; 9Via Roma Health Centre, Institut Català de la Salut, Barcelona, Spain; 10Departament d’Infermeria, Universitat de Girona, Girona, Spain
Correspondence: Laura Medina-Perucha Gran via de les Corts Catalanes, 587, Attic, Barcelona, 08007, Spain
Tel +34 93 482 4253 ext. 4761
Email [email protected]
Purpose: Co-design processes with patients allow developing health education materials, that are adapted to the population’s knowledge and use of language, to reduce inappropriate antibiotic use.
Patients and Methods: This study presents a co-design process of educational material with patients (over 18 years old) with a previous diagnosis of acute lower respiratory tract infection. The co-design was framed within a qualitative study (Phase I, interviews; Phase II, focus group) conducted in Barcelona between April and September 2019.
Results: Twenty-nine semi-structured interviews were conducted. Six people participated in the focus group. Based on participants’ narratives, educational materials can be useful to support healthcare consultations. Materials should be designed to be accessible in terms of the content and language used.
Conclusion: The co-design of educational materials is essential for health promotion. This study presents an example of how materials can be co-developed with patients. The material elaborated in this study is being used for the ISAAC-CAT project and may be useful for future research, practice in health services and health policy.
Keywords: health education, co-design, acute respiratory infections, antimicrobial resistance, primary healthcare
Plain Language Summary
This study is an example of how educational materials can be designed with patient collaboration. The study is focused on encouraging people to use antibiotics correctly to avoid developing antibiotic resistance. The researchers interviewed 29 patients that had had a respiratory infection in Catalonia (Spain). Six of the patients that were interviewed also participated in a group session where they collaborated with the researchers, on how to design educational material to improve antibiotic use. The materials needed to be easy to understand for the general population, so the language had to be clear and plain. There were also some ideas on how to make the content and formatting of the educational material better. The material that was elaborated will be used in a larger study called ISAAC-CAT. The researchers hope that this study will help in future research and aid healthcare professionals to create public policies.
Introduction
An increase in morbidity and mortality due to antimicrobial resistance is one of the main public health challenges worldwide.1,2 This is the reason why public health programs have been developed around the globe, to design strategies that reduce inappropriate use of antibiotics.3–6 The first aim of the policies planned by the World Health Organization is currently to “increase consciousness and knowledge around antimicrobial resistance through effective communication, education and training”.1 High-quality and effective health communication has become even more crucial in the context of the COVID-19 pandemic.7
The design of materials for health education is one of the key priorities. These materials help to convey precise health information and can be accessed through healthcare services. Thus, they complement the information that patients receive during a healthcare consultation. Given the importance of adapting educational materials to the population to ensure a full understanding of the information, involving patients in the co-design of materials is essential.8,9 However, the population is rarely included as an active agent for co-design research and practice.10 This is a crucial element to promote patient-centered healthcare systems.11,12
This paper presents a co-design process of educational materials to promote an appropriate use of antibiotics for acute lower respiratory tract infections (ALRTIs) in primary healthcare in Spain. This study is part of the ISAAC-CAT project,13 a randomized controlled trial that aims to compare three interventions to reduce antibiotic prescription for ALRTIs in Catalonia (Spain).
Patients and Methods
This paper presents a co-design process, using qualitative research methods, to develop health educational materials to promote appropriate antibiotic use in Catalonia (Spain). The study took place in two phases. In Phase I, twenty-nine patients participated in semi-structured individual interviews that took place between April and July 2019. The interviews lasted between 21 and 84 minutes and were conducted by the authors LMP (N=24) and ABe (N=5). The interviews covered other relevant topics, such as the design and use of educational materials. Other interview findings are published elsewhere.14.In Phase II, a focus group (N=6) was selected and a discussion took place at the [research center] on September 26th 2019, lasting 90 minutes and chaired by LMP and ABe.
Participants were adult patients (over 18 years old) with a diagnosis of at least one ALRTI in the last 12 months. Sampling was selective and purposive. Participants were selected to attain discursive diversity based on the following characteristics: sex, age, ethnicity, date of last ALRTI, number of ALRTIs in the last year and treatments received.15 Thus, participant characteristics were considered throughout recruitment to ensure informants’ variability in their profiles and discourses. Interviewed participants were recruited from four primary healthcare centers, three in Barcelona and one in Tarragona (Catalonia, Spain). The focus group participants were selected from among those who had taken part in the interviews. Then, all interview participants were contacted and invited to take part in the focus group. Six participants agreed and participated in the focus group. A topic guide was used to conduct the interviews, which included other topics including the development and use of educational materials (see Supplementary Material 1). Another topic guide was developed for the focus group, using data from the interviews and different manuals to design health education materials (see Supplementary Material 2).16–18 All interviews and the focus group were audio-recorded with participants’ consent. Data were analyzed using thematic content analysis.15
As for the co-design process, first, interview data were analyzed to design a draft of educational material (Phase I). In the focus group (Phase II), preliminary results were presented to participants, for feedback and co-interpretation of the data. Discussing interview findings with the focus group participants was also useful to design and develop the educational material. Then, participants worked on the co-design of the material. Each participant was given the educational material draft that had been prepared based on the interviews. Participants discussed their views on the drafted material and suggested changes for improvement throughout the session.
The final educational material was based both on the analysis of the interviews and the focus group. This material was finalized with the contributions of the members of the research team and a graphic designer (NG). The designed material cannot be presented in this publication to prevent any interference in the development of the randomized controlled trial of the ISAAC-CAT project where the educational material will be used.13 Instead, examples of changes led by the participants in the material content will be provided.
Results
Interview participants were 29 patients (16 women and 13 men). The average age was 57 (range from 25–89). Almost all participants were White (N=28), while one was Latino. Most had been born in Spain (N=26). Some were working full time (N=12). Six interview participants took part in the focus group (five men and one woman), the average age was 67. Findings are presented separately for the interviews (co-design phase I) and the focus group (co-design phase II).
Phase I: Interviews
Based on participants’ narratives, having access to written materials on ARLTIs could be useful to care for their health. The current access to information was seen as a problem as it is not regulated. For instance, anyone could access a great amount of information on the Internet but there was no control over the quality of the information and how it is portrayed. According to participants, written information should never replace the information given by healthcare professionals.
A few participants mentioned that, even if they thought having written information available was useful, they would most probably not read. Another few explained that they considered having enough information already.
Yes, it would be interesting that they could also give it [written information] to you … well, that there was information, a leaflet or something … […]. Well, everything is on the Internet now, also … well, you also need to filter what you find in the Internet, because it could be that you are already dead for having pneumonia, you know?. (P11, woman, 35 years old)
Participants thought that written information should mainly include treatment guidelines (including non-pharmacological) and preventive measures (including risk factors and transmission routes). Some participants also mentioned the utility of including the etiology of ARLTIs, guidelines to follow when there are comorbidities, drug´ side effects, contraindications and mechanisms of action.
Well so I suppose that related to what each person has, so what is the disease itself, the medication that needs to take, especially warning that it is always the doctor who need to say … but well, normally the medication usually available, and well, these kind of things, and the guidelines to take this medication, because more or less the medication guidelines are always the same, right?. (P18, man, 60 years old)
Participants considered that the materials should be available both in Catalan and Spanish (the two official languages in Catalonia), and use an inclusive and non-judgmental language. Most participants explained that written information had to be available in print, as most people preferred this format (especially the elderly). However, there should also be the option of having this information online so that healthcare professionals could send it via email to those who may prefer it.
Better on paper […] Yes, you can read and re-read and highlighted and even re-read […] Yes, you are used to paper because you retain it and re-read 40 times. And the laziness of scrolling 40 pages on the phone … and also another thing, the phone screens that are used, they do not go well. (P28, man, 89 years old; interview)
Online would be ideal […]. What could be done is to send it always online and the doctor could ask ‘do you want information?’ and then print the leaflet. If you say you don’t want to, then you don’t want to. (P26, woman, 25 years old; interview)
Phase II: Focus Group
Participants discussed the content’s coherence and suitability. Changes were suggested on how the material content was organized. Participants agreed on the fact that educational materials should be based on the patient’s needs and objectives. The importance of appropriate antibiotic use should be highlighted.
Participants identified and suggested eliminating contradictions in the material, such as promoting the use of over-the-counter medication, at the same time that antibiotic use was encouraged to be responsible and based on a prescription. Some participants also mentioned the importance of not using a symptom (eg, cough) as a synonym for a health condition (eg, ARLTI), as this can be misleading. They suggested that language should be accessible and technical terms should be avoided. However, the language had to be formal enough to communicate respect and formality. Some concepts (eg, what a virus is) should be explained to facilitate understanding. Besides, some of the terms used were perceived as being too subjective (eg, continuously or profusely). Participants suggested replacing them with clearer descriptions or terms. Participants also pointed out that the reasons for some health recommendations (eg, avoid covering your mouth with your hands when coughing) should be explained.
The images available in the educational material’s draft were not sensitive or representative to the gender, age and ethnical diversity in the participant’s context, as most images were originally of White men only. Images for the materials should be carefully selected so that they are inclusive of gender, age and ethnical diversity. Other formatting elements, such as font and institutional logos’ size were mentioned. Font-size should be bigger than in the draft, around 14–18 points. Institutional logos should be small to be perceptible without taking too much space. Participants preferred the material in an A4 sheet to a leaflet.
Examples of initial suggestions (on the educational material draft) and changes made based on participants’ suggestions can be found in Table 1.
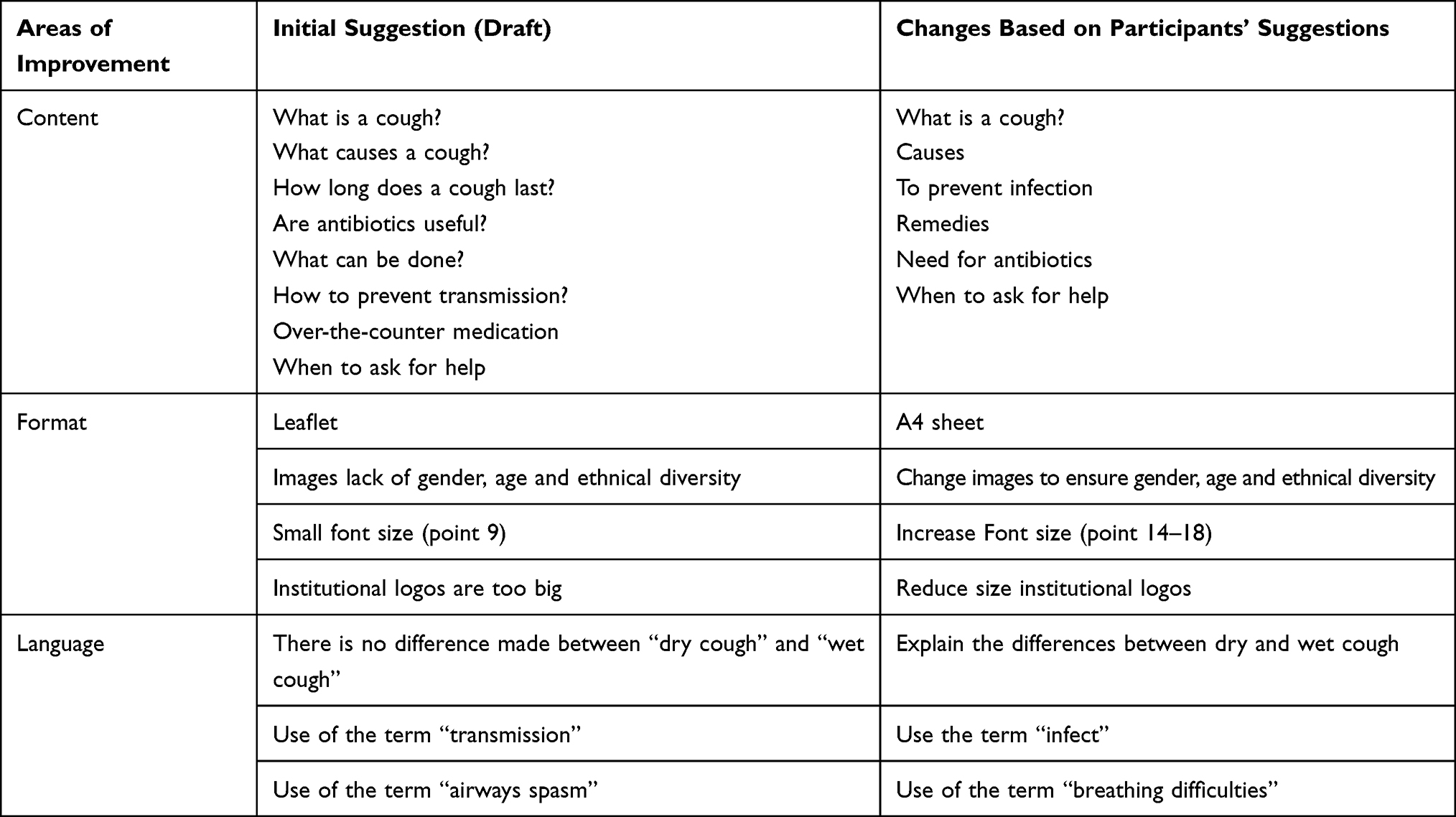 |
Table 1 Examples of Initial Suggestions and Changes Based on Participants’ Suggestions |
Discussion and Conclusions
Communication is an essential element for health promotion.19–21 One of the reasons for its importance is that it promotes the population’s knowledge of their own body and health. Then, communication can become a tool to allow patients to abandon an inherently passive model of patients so that they actively promote and protect their own health.14 This approach means to break with the traditional biomedical model of health, in which the means of healthcare is exclusively owned by healthcare professionals, who represent authorities inside a system that understands and treats people as passive subjects.14,22,23 This is the reason why the co-development of educational materials with patients is key, not only to achieve their function effectively, but to accompany people in a long-term learning process.
Health literacy should also be considered when developing educational materials. This concept is understood as the ability for people to critically evaluate information and make health-related decisions accordingly.24,25 It is an essential element for co-development processes as health literacy has an impact on how people use the healthcare system, communicate and relate with healthcare professionals and practice self-care.24,26 Educational materials for appropriate antibiotic use should ensure health literacy among users. The population’s diversity in education should be considered and people with different characteristics (eg, educational and socioeconomic status levels) should be included in co-development sessions.27,28
In this study, findings suggest that educational materials could be useful to support healthcare consultations. These materials should be accessible, in terms of the content and language used. The educational material will be used for the randomized controlled trial of the ISAAC-CAT project.13 We expect this material to be useful for future research, clinical practice and health policies. And, ultimately, we expect it to contribute to tackling antimicrobial resistance.
Data Sharing Statement
Data will be made available upon reasonable request to the authors, contacting Dr Anna Berenguera at [email protected]. All data will be anonymized to ensure participants’ confidentiality and anonymity.
Ethics Approval and Informed Consent
Ethical approval was granted by the Ethics Committee of the Institut de Recerca en Atenció Primària Jordi Gol i Gurina (IDIAPJGol) (REC P18/227) on 19th of December 2018. All participants were informed about the purpose of the study and gave their verbal and written consent to take part in the study prior to their participation. This study has been conducted in accordance with the Declaration of Helsinki.
Consent for Publication
All participants gave their consent for their anonymized data to be published.
Acknowledgments
We would like to thank all participants that have taken part in this study. We are also grateful to all healthcare professionals who contributed to participant recruitment. We also want to thank them for their contributions to design the final version of the educational material. Lastly, we would like to thank Harriet Phyllis Pinnegar for reviewing and editing the final draft of this article.
Author Contributions
LMP led the data collection, data analysis and interpretation of the findings, the design of the educational material and wrote the manuscript. PGH contributed to the study design and data collection. He critically reviewed this manuscript. AGS and AM collaborated in the design of the study, supported participant recruitment and reviewed this article. They also participated in the educational material’ design. JMC and ALR contributed to the study design, participant recruitment and reviewed the manuscript. Abo and IA contributed to the study design and critically reviewed the manuscript. NB and RM supported the design of educational materials. CL coordinates the ISAAC-CAT project and led the design of the study. He critically reviewed this manuscript. ABe supervised the development of the qualitative study. She participated in the design of the study, data collection, data analysis and interpretation. She also contributed to the design of the educational materials and reviewed this manuscript. All authors made substantial contributions to conception and design, acquisition of data, or analysis and interpretation of data; took part in drafting the article or revising it critically for important intellectual content; agreed to submit to the current journal; gave final approval of the version to be published; and agree to be accountable for all aspects of the work.
Funding
This study is part of the ISAA-CAT Project, funded by the Fundació La Marató de TV3 (Ref. 201820): https://www.ccma.cat/tv3/marato/fundacio/. The funder has not influenced the development of this study.
Disclosure
The authors report no conflicts of interest in this work.
References
1. World Health Organization. Global Action Plan on Antimicrobial Resistance. Geneva:World Health Organization; 2015.
2. Gajdács M. The concept of an ideal antibiotic: implications for drug design. Molecules. 2019;24(5):892. doi:10.3390/molecules24050892
3. Aslam A, Gajdács M, Zin CS, et al. Evidence of the practice of self-medication with antibiotics among the lay public in low- and middle-income countries: a scoping review. Antibiot. 2020;9:9. doi:10.3390/antibiotics9090597
4. Taylor AM, Phillips K, Patel KV, et al. Development of a conceptual framework for understanding shared decision making among african-american Lgbt patients and their clinicians. J Gen Intern Med. 2018;31(6):677–687. doi:10.1007/s11606-016-3616-3
5. Hale AR, Young VL, Grand A, McNulty CAM. Can gaming increase antibiotic awareness in children? A mixed-methods approach. JMIR Serious Games. 2020;34(2):e5. doi:10.1016/j.gaceta.2019.08.010
6. Young VL, Rajapandian V, Eley CV, Hoekstra BA, Lecky DM, McNulty CA. Monitoring web site usage of e-bug: a hygiene and antibiotic awareness resource for children. JMIR Res Protoc. 2019;20(1):e131. doi:10.1186/s13063-019-3727-3
7. Finset A, Bosworth H, Butow P, et al. Effective health communication – a key factor in fighting the COVID-19 pandemic. Patient Educ Couns. 2020;103(5):873–876. doi:10.1016/j.pec.2020.03.027
8. Barragan N. La comunicación centrada en el paciente. Folia Humanística. 2019. doi:10.30860/0017
9. Hoffmann T, Worrall L. Designing effective written health education materials: considerations for health professionals. Disabil Rehabil. 2004;26(19):1166–1173. doi:10.1080/09638280410001724816
10. Jacques-Aviñó C, Pons-Vigués M, Mcghie JE, et al. Participación pública en los proyectos de investigación: formas de crear conocimiento colectivo en salud. Gac Sanit. 2020;34(2):200–203. doi:10.1016/j.gaceta.2019.08.010
11. Rathert C, Wyrwich MD, Boren SA. Patient-centered care and outcomes: a systematic review of the literature. Med Care Res Rev. 2012;70(4):351–379. doi:10.1177/1077558712465774
12. McMillan SS, Kendall E, Sav A, et al. Patient-centered approaches to health care: a systematic review of randomized controlled trials. Med Care Res Rev. 2013;70(6):567–596. doi:10.1177/1077558713496318
13. Ruiz R, Moragas A, Trapero-Bertran M, et al. Effectiveness and cost-effectiveness of Improving clinicians’ diagnostic and communication Skills on Antibiotic prescribing Appropriateness in patients with acute Cough in primary care in CATalonia (the ISAAC-CAT study): study protocol for a cluster rando. Trials. 2019;20(1):740. doi:10.1186/s13063-019-3727-3
14. Medina-Perucha L, García-Sangenís A, Moragas A, et al. Autonomy, power dynamics and antibiotic use in primary healthcare: a qualitative study. PLoS One. 2020;15(12):e0244432. doi:10.1371/journal.pone.0244432
15. Berenguera A, Fernández de Sanmamed MJ, Pons M, et al. To listen, to observe and to understand. bringing back narrative into the health sciences.
16. Haute Autorité de Santé. Élaboration d’un Document Écrit d’information à l’intention Des Patients et Des Usagers Du Système de Santé. Guide Méthodologique; 2008.
17. National Health Service. Toolkit for Producing Patient Information; 2003.
18. Moumjid N, Morelle M, Carrère M-O, Bachelot T, Mignotte H, Brémond A. Elaborating patient information with patients themselves: lessons from a cancer treatment focus group. Health Expectations. 2003;6(2):128–139. doi:10.1046/j.1369-6513.2003.00218.x
19. Nutbeam D. Health literacy as a public health goal: a challenge for contemporary health education and communication strategies into the 21st century. Health Promot Int. 2000;15(3):259–267. doi:10.1093/heapro/15.3.259
20. Salmon CT, Poorisat T. The rise and development of public health communication. Health Commun. 2019;1–12. doi:10.1080/10410236.2019.1654180
21. Land V, Parry R, Seymour J. Communication practices that encourage and constrain shared decision making in health-care encounters: systematic review of conversation analytic research. Heal Exp Int J Public Particip Heal Care Heal Policy. 2017;20(6):1228–1247. doi:10.1111/hex.12557
22. Haque OS, Waytz A. Dehumanization in Medicine: causes, Solutions, and Functions. Perspect Psychol Sci. 2012;7(2):176–186. doi:10.1177/1745691611429706
23. Foucault M. The Birth of the Clinic. Abingdon: Routledge; 1989.
24. Zarcadoolas C, Pleasant A, Greer DS. Understanding health literacy: an expanded model. Health Promot Int. 2005;20(2):195–203. doi:10.1093/heapro/dah609
25. Salm F, Ernsting C, Kuhlmey A, Kanzler M, Gastmeier P, Gellert P. Antibiotic use, knowledge and health literacy among the general population in Berlin, Germany and its surrounding rural areas. PLoS One. 2018;13(2):e0193336–e0193336. doi:10.1371/journal.pone.0193336
26. Paasche-Orlow MK, Wolf MS. The causal pathways linking health literacy to health outcomes. Am J Health Behav. 2007;31(Suppl 1):S19–S26. doi:10.5993/AJHB.31.s1.4
27. McNulty CAM, Lecky DM, Hawking MKD, Roberts C, Quigley A, Butler CC. How much information about antibiotics do people recall after consulting in primary care? Fam Pract. 2016;33(4):395–400. doi:10.1093/fampra/cmw022
28. McNulty CAM, Boyle P, Nichols T, Clappison P, Davey P. Don’t wear me out--the public’s knowledge of and attitudes to antibiotic use. J Antimicrob Chemother. 2007;59(4):727–738. doi:10.1093/jac/dkl558
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.